 Reflux esophagitis
Reflux esophagitis
[20101120. JNM Facebook GERD club case (1) posted on Dec 7, 2010]
Let me introduce myself. I am Jun Haeng Lee working at Samsung Cancer Center, one of the major comprehensive cancer centers in Korea. My main interest is gastroesophageal reflux disease and early gastric cancer.
I have a plan to organize a discussion using the JNM Facebook site. Hopefully, I would make a short case presentation with a few pictures once in a week. Every comment and opinion would be welcomed.
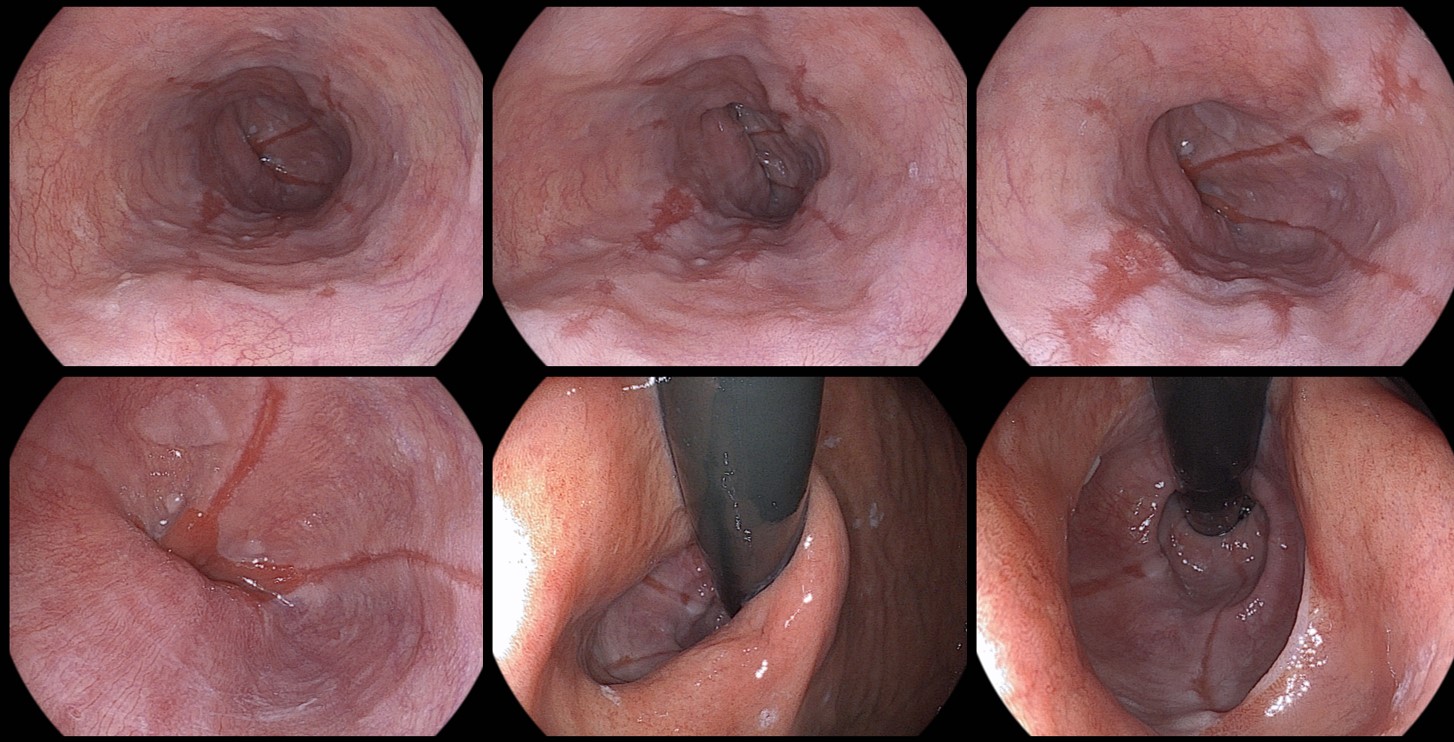
This is my first case. A middle aged man visited my clinic with a complaint of typical heartburn. You can see the endoscopic findings in the two pictures below. What's your endoscopic diagnosis? Please choose one answer and give some comments.
1. Normal
2. Erosive esophagitis
3. Hiatal hernia
4. Short segment hiatal hernia
5. Minimal change lesion
6. Others
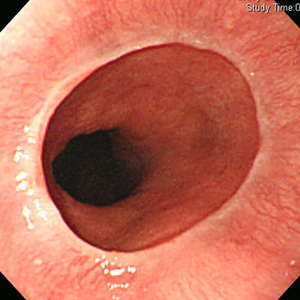
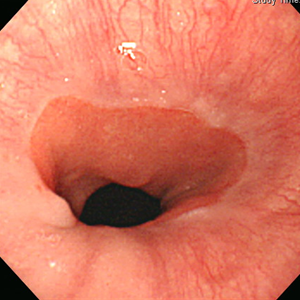
My comment: My personal answer is #4. The classic length criteria of hiatal hernia is 2 cm or more, but I think it is too arbitary. When I measured the vertical length of this hiatal hernia, it was less than 2 cm. Dr. Bak of Korea University called it a short segment hiatal hernia (SSHH). The term of SSHH is not supported by many researchers, but most physicians already know that something may be wrong even if the length is less than 2 cm. In my opinion, SSHH can be used as a clue for the diagnosis of GERD.
Best comment from members of ANMA by Dr. Hirota Miwa: This is a case of hiatal hernia. Some physician would claim this is an erosive esophagitis or minimal change with very small irregularity of the EC junction, but we should not mind such a small changes. There is no apprent mucosal breaks. Please note that endscopic findings of reflux esophagitis change very quickly. Therfore it is of no meaning to discuss very small endoscopic findings.
[위식도역류질환 공개강좌 동영상]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.

