크게 보시려면 그림을 클릭하세요.
[20111127. Bleeding peptic ulcer (9): 2010 consensus recommendation]
2010년 Ann Internal Med에 실린 consensus recommendation을 소개한다.
크게 보시려면 그림을 클릭하세요.
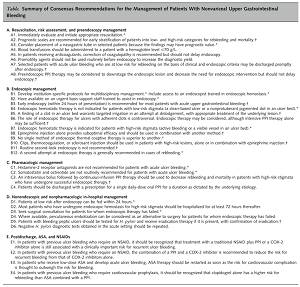
위 table 중 내시경치료에 대한 부분만을 옮긴다. 우리말은 필자의 comment임.
B1. Develop institution-specific protocols for multidisciplinary management. Include access to an endoscopist trained in endoscopic hemostasis.
B2. Have available on an urgent basis support staff trained to assist in endoscopy.
B3. Early endoscopy (within 24 hours of presentation) is recommended for most patients with acute upper gastrointestinal bleeding. - 대부분의 환자(most patients)라는 점에 주의하자. 환자 상태가 안 좋으면 무리해서 서둘러 내시경을 할 필요는 없다. Vital을 잡고 환자의 전신 상태를 돌보는 것이 최우선이다.
B4. Endoscopic hemostatic therapy is not indicated for patients with low-risk stigmata (a clean-based ulcer or a nonprotuberant pigmented dot in an ulcer bed).
B5. A finding of a clot in an ulcer bed warrants targeted irrigation in an attempt at dislodgement, with appropriate treatment of the underlying lesion. - 일단 clot은 제거하는 것이 표준이다. 그러나 상황에 따라 달라질 수 있다. 재출혈률은 20% 전후이다.
B6. The role of endoscopic therapy for ulcers with adherent clots is controversial. Endoscopic therapy may be considered, although intensive PPI therapy alonemay be sufficient. - 과거보다 PPI를 일찍 시작하는 경향이다.
B7. Endoscopic hemostatic therapy is indicated for patients with high-risk stigmata (active bleeding or a visible vessel in an ulcer bed).
B8. Epinephrine injection alone provides suboptimal efficacy and should be used in combination with another method. - 이 부분이 가장 중요한 point라고 생각된다. Epinephrine injection은 반드시 보다 definitive한 치료와 함께 이루어져야 한다. 이런 관점에서 필자는 clip을 좋아한다 (clip은 보험급여가 되지 않는다. 말도 안되는 일이지만 현실이 그렇다). Electrocauterization도 나쁘지 않다.
B9. No single method of endoscopic thermal coaptive therapy is superior to another.
B10. Clips, thermocoagulation, or sclerosant injection should be used in patients with high-risk lesions, alone or in combination with epinephrine injection.
B11. Routine second-look endoscopy is not recommended. - Second-look endoscopy를 늘상 실행하는 관례는 하루 빨리 없어져야 한다. 근거도 없고, 환자도 싫어하고, 비용만 올라간다. 입원기간도 길어진다. 한 마디로 필요없다.
B12. A second attempt at endoscopic therapy is generally recommended in cases of rebleeding. - 재출혈이 없는 환자에서 또 다시 무리하여 preemptive hemostasis를 하지는 말아야 한다. 긁어 부스럼된다.
![]() [References]
[References]
1) 상부위장관 출혈의 치료: 소화성궤양 출혈을 중심으로 (강기주, 이준행) 대한내과학회지 2010
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.