Previous | Home | EndoTODAY | List | Next
![]() [SMC experience]
[SMC experience]
다소 오래된 자료입니다만 저도 gastric tube cancer 자료를 발표한 바 있습니다 (Kim. Hepatogastroenterology 2008). 수술 후 추적관찰기간이 짧았기 때문에 Niigata 대학처럼 누적발생률을 구하기는 어려웠습니다. 다만 식도암 수술 환자 728명 중 11명(1.1%)에서 발견한 gastric tube cancer에 대한 이야기였습니다. 식도암에서 위암까지의 간격은 8 - 85 개월(median : 37)이었습니다.
Hepatogastroenterology 2008
BACKGROUND/AIMS: With the improvement of the outcome after esophagectomy for esophageal cancer, patients with metachronous gastric cancer (MGC) in the reconstructed thoracic stomach have been observed in clinical practice. This study is a report of experiences with MGC with an emphasis on clinical pictures and treatment results. METHODOLOGY: Medical records were reviewed of 728 patients who underwent surgery for esophageal cancer at Samsung Medical Center between 1994 and 2004. MGC was defined as follows; (1) diagnosed more than 6 months after esophagectomy, (2) squamous cell carcinoma in histology of the surgically resected esophagus, (3) adenocarcinoma in histology of the stomach biopsy or surgical specimen. The clinicopathologic characteristics of MGC were evaluated. RESULTS: Eight patients (1.1%) of 728 patients were diagnosed with MGC. All patients were male and had a history of active smoking and drinking. The median age at the time of diagnosis of MGC was 67.8 years old (range: 62-76). Three patients (37.5%) were asymptomatic. Two patients (25%) complained of epigastric pain and 3 patients (37.5%) complained of obstructive symptoms including regurgitation, aspiration, dysphagia, and vomiting. The median interval between diagnosis of MGC and esophagectomy was 37 months (range: 8-85). Three MGCs (37.5%) were detected by endoscopic examination but not by computed tomography (CT). Three patients (37.5%) received surgery and were alive without recurrence for 12, 18 and 63 months respectively. One patient (12.5%) received radiation therapy and was alive for 69 months. Four patients (50%) received no treatment because of follow-up loss in 2 patients (25%) and death within days of MGC diagnosis in 2 patients (25%). CONCLUSIONS: Favorable outcomes can be obtained by active treatment in patients with MGC after esophagectomy. Regular endoscopic follow-up is important for early detection and more effective treatment of MGC, especially in areas where the incidence of gastric cancer is high.
중하부 식도암의 대표적인 수술적 치료방법법은 Ivor-Lewis operation입니다. 중하부식도를 절제한 후 위를 당겨서 남아있는 식도와 연결하는 술식입니다. Screening endoscopy가 보편화되면서 조기에 발견되는 식도암 환자가 증가하고 있습니다. 특히 식도암 수술 후 장기 생존하는 환자가 많아지면서 gastric tube cancer가 문제가 되고 있습니다. 다행스럽게 조기에 발견되면 내시경 절제술을 시행할 수 있겠지만 진행된 상태에서 발견되면 수술을 피할 수 없습니다. 이때의 수술은 colonic interposition일 수 밖에 없으며 상당한 morbidity와 mortality가 동반될 수 밖에 없다고 생각됩니다.
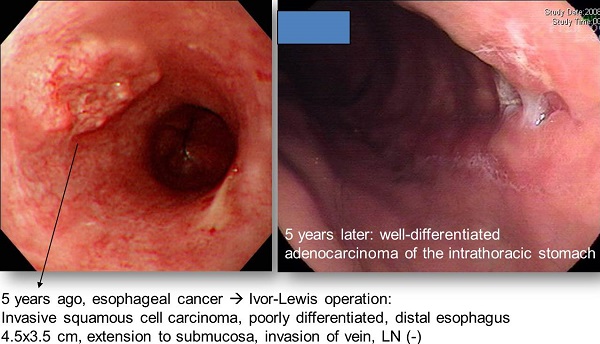
아래 증례는 식도암 수술 후 5년만에 발견된 intra-thoracic stomach의 암입니다. 식도암 수술 후 보다 비교적 이른 시기에 위암이 발견된 예도 없지 않습니다. 식도암 진단시 위도 자세히 관찰할 필요가 있습니다.
[2013-4-17 경향신문] 전략적 모호성 또는 철학의 부재 - 민감한 현안에 모호한 자세를 취하는 것을 마냥 탓할 수만은 없다. 이른바 '전략적 모호성'은 국제정치 무대에서나 이분법적 선택을 요구하는 상황에서 현명한 전략일 수 있다. 박 대통령이 공약 현실화에 방점을 두고 보수와 진보, 지지층과 반대층을 아우르기 위해 이런 전략을 쓰고 있다고 해석할 수도 있다. 하지만 전략적 모호성이 만병통치약은 아니다. 남용될 경우 정치불신을 키우고, 지도자에게는 치명상으로 돌아올 수 있다. 박 대통령의 자산인 신뢰에 금이 갈 수도 있다는 얘기다. 전략적 모호성이 수반하는 불확실성과 혼란의 사회적 비용도 결코 적지 않다. 일련의 모호성이 전략적 차원이라면 그나마 다행이지만, 철학과 실천의지의 부재에 기인한 것이라면 심각한 문제다.
[Home]