Previous | Home | EndoTODAY | List | Next
![]() [Myeloid sarcoma = granulocytic sarcoma]
[Myeloid sarcoma = granulocytic sarcoma]
Myeloid sarcoma (= granulocytic sarcoma)는 골수에 병발하지 않고 extramedullary mass 형태로 나타나는 leukemia입니다. 넓은 의미에서 myeloid leukemia의 일종이라고 할 수 있습니다. 골수에서 병발하지 않는 환자들도 시간이 지나면서 골수에서 leukemia가 발생하는 경우가 있다고 합니다.
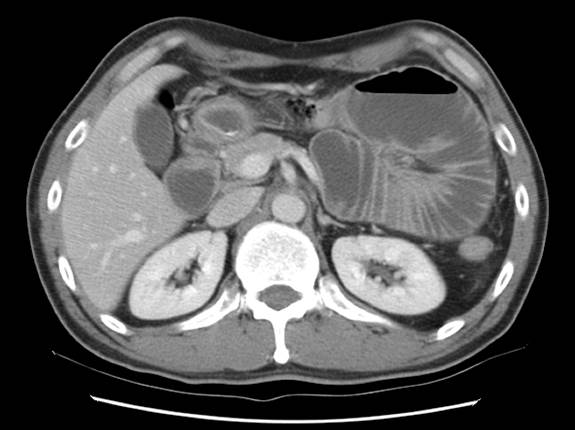
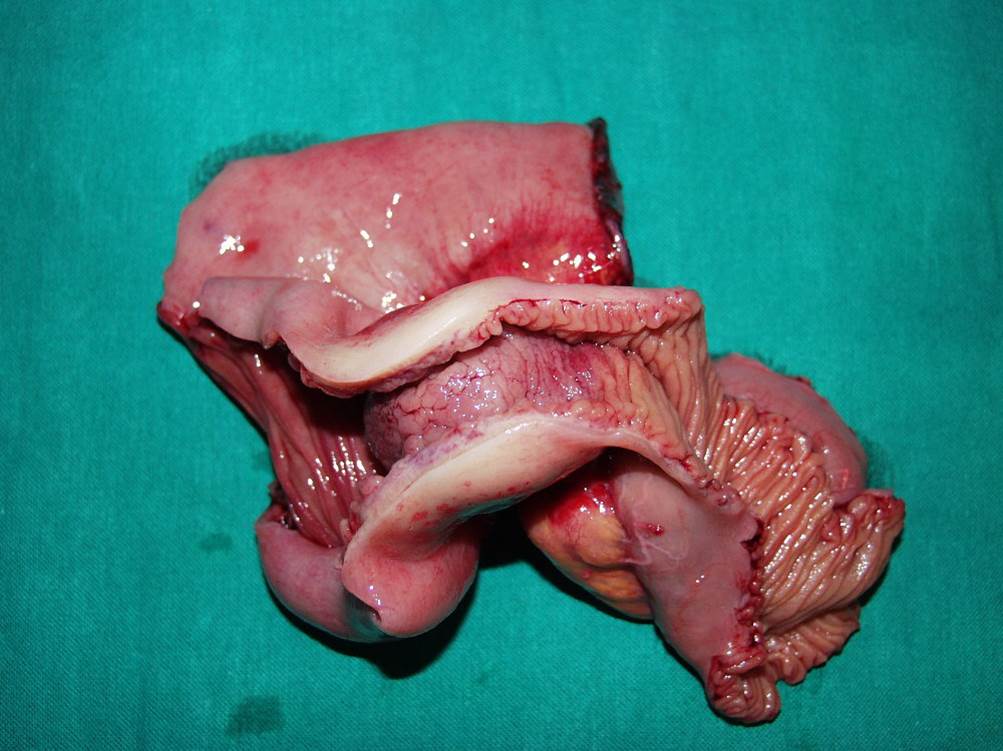
![]() [증례 1. 소장 myeloid sarcoma - 40세 남성. 복통과 체중감소]
[증례 1. 소장 myeloid sarcoma - 40세 남성. 복통과 체중감소]
![]() [증례 2. 10여년 전 MDS로 PBSCT 받은 환자(여자 55세)의 위 종양 조직검사에서 myeloid sarcoma]
[증례 2. 10여년 전 MDS로 PBSCT 받은 환자(여자 55세)의 위 종양 조직검사에서 myeloid sarcoma]
Biopsy : Consistent with MYELOID SARCOMA
CD 34 : Positive in tumor cells
C-KIT (CD 117) : Focal positive in tumor cells
CD 99(MIC-2,EWING'S SARCOMA) : Focal weak positive in tumor cells
Vimentin : Positive in tumor cells
CD 45 RB (LCA) : Positive in tumor cells
CD 56 : Focal weak positive in tumor cells
CD 123, IL-3 : Focal weak positive in tumor cells
Cytokeratin (AE1/AE3) : Focal weak positive in tumor cells
CD 4, (Leu-3a) : Focal weak positive in tumor cells
Myeloperoxidase : Negative in tumor cells
Lysozyme : Negative in tumor cells
CD 138, Syndecan-1 : Negative in tumor cells
MUM-1(IRF-4) : Negative in tumor cells
Synaptophysin : Negative in tumor cells
Tdt : Negative in tumor cells
CD 3, T-CELL : Negative in tumor cells
CD 20, L26 : Negative in tumor cells
Ki-67 : Positive in ~50% of tumor cells
Kappa ISH : Negative in tumor cells
Lambda ISH : Negative in tumor cells
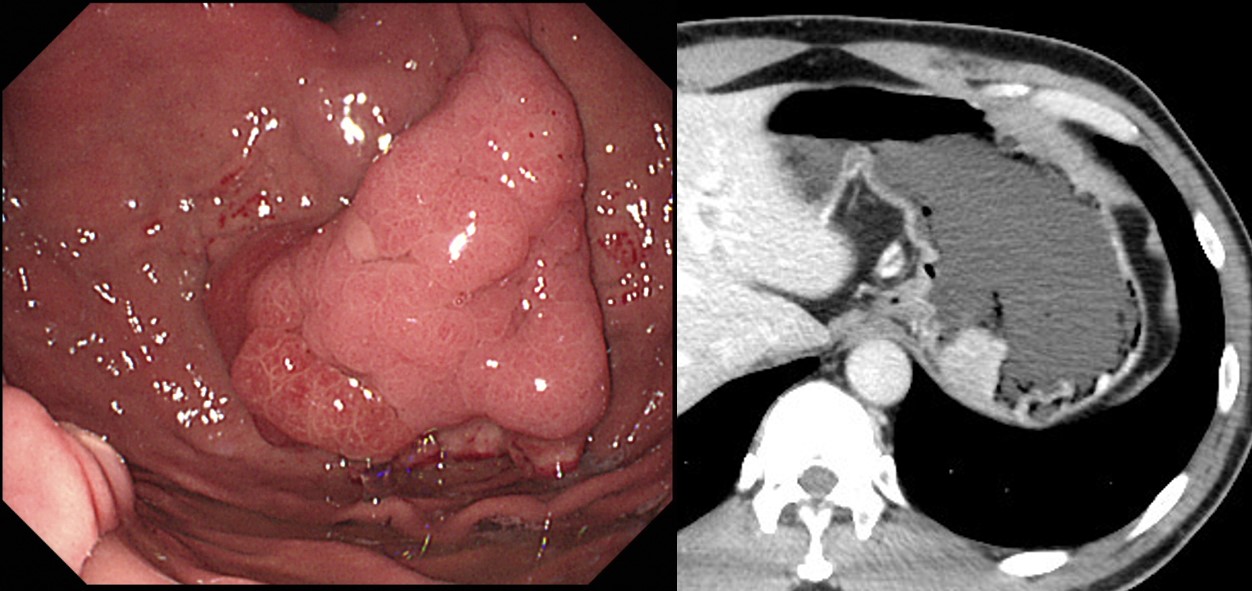
![]() [증례 3] Gastric myeloid sarcoma without acute myeloblastic leukemia World J Gastroenterol. 2015 Feb 21; 21(7): 2242-2248.
[증례 3] Gastric myeloid sarcoma without acute myeloblastic leukemia World J Gastroenterol. 2015 Feb 21; 21(7): 2242-2248.
Endoscopic examination revealed numerous hyperplastic nodules in the stomach
Clinical behavior and therapeutic response are not influenced by age, sex, anatomic site, presentation, histotype, phenotype or cytogenetic findings. For MS treatment, chemotherapy had been found more effective than radiation therapy or surgical resection for improving disease-free intervals or disease-free survival
![]() [Reference]
[Reference]
Myeloid Sarcoma: Current Approach and Therapeutic Options Ther Adv Hematol. 2011 Oct; 2(5): 309-316.
Myeloid sarcoma (MS), also known as chloroma (owing to its green color attributed to the enzyme myeloperoxidase), is a pathologic diagnosis for an extramedullary proliferation of blasts of one or more of the myeloid lineages that disrupt the normal architecture of the tissue in which it is found. It has also been addressed as granulocytic sarcoma, myeloblastoma and extramedullary myeloid cell tumor. MS is included as one of the major subgroups of myeloid neoplasms and acute leukemia in the WHO classification and is most often found either concurrently or following a previously recognized AML. It may also occur as an isolated leukemic tumor or precede the appearance of blood or bone marrow (BM) disease. Less often, MS may occur in association with a myeloproliferative neoplasm (MPN) or myelodysplastic disorder (MDS). In published series, MS is often included with extramedullary disease (EMD); however, these two phenomena may not share the same outcome and may need to be treated differently.
The current recommended treatment regimen in patients presenting with isolated MS or MS presenting concomitantly with AML is conventional AML-type chemotherapeutic protocols. A comprehensive overview of AML treatment is beyond the scope of this review and can be viewed in recently published review papers. This recommendation is based on the observation of a higher rate of progression to AML in isolated MS patients receiving localized treatment (88-100%) compared with patients given systemic chemotherapy (42%)
[Home]