![]() [Description exercise 5]
[Description exercise 5]
![]() Case 29
Case 29
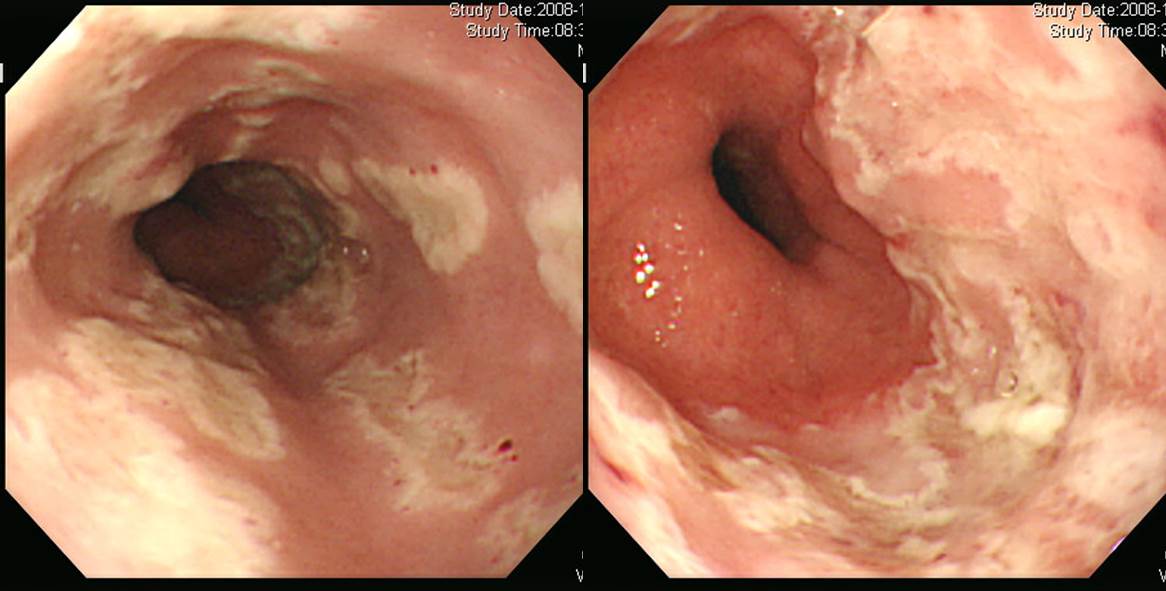
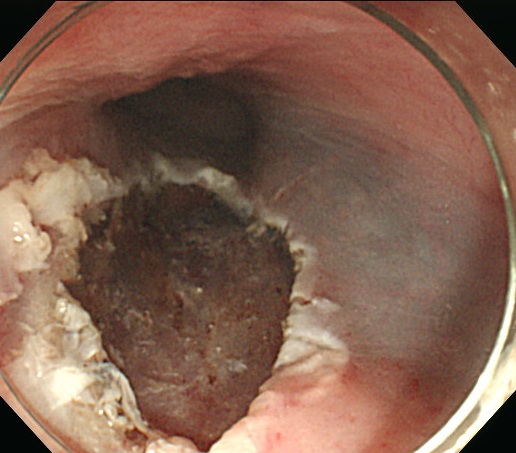
Findings: In the mid to distal esophagus, there are multiple discrete oval to linear shallow ulcers with raised margins. The edges are discrete and the base is flat and covered with white exudate.
Impression: Viral esophagitis (herpetic esophagitis)
[Comments]
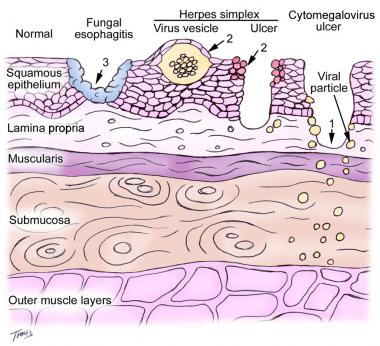
Typical findings of herpetic esophagitis
(1) The endoscopic appearance is characterized by diffuse friability; ulceration; and exudates, mostly in the distal esophagus.
(2) Classically, the earliest esophageal lesions are rounded 1- to 3-mm vesicles in the mid to distal esophagus, the centers of which slough to form discrete circumscribed ulcers with raised edges.
(3) These lesions can also be appreciated radiographically.
![]() Case 30 - Upper esophagus
Case 30 - Upper esophagus
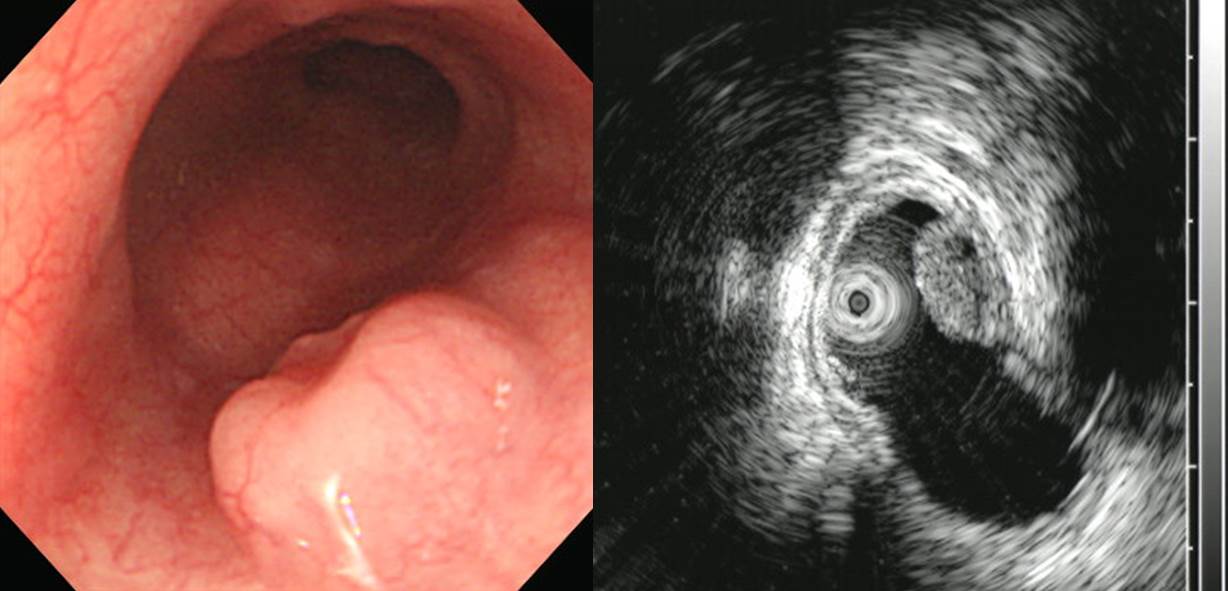
Findings: In the upper esophagus, a 1cm-sized elevated lesion with slight central depression was found. The overlying mucosa is normal. On EUS, it is a mixed hyperechoic lesion originating from the second layer.
Impression: Esophageal SET (granular cell tumor, more likely)
[Comment]
Granular cell tumor is the most likely impression, but the final pathology was large cell neuroendocrine carcinoma. Both of them are neuroendocrine origin.
1. Name of Procedure: ESD
2. Site of Tumor: Esophagus
3. Diagnosis: Large cell neuroendocrine carcinoma
4. WHO classification(2010): Neuroendocrine carcinoma
5. Multiplicity: Single
6. Size: 0.9x0.8 cm
7. Extent: Mucosa and submucosa
8. Grading: Mitotic Count: >20/10 HPF. Ki-67 labeling index: G3>20%
9. Immunohistochemical Stains - Synaptophysin : Positive, Chromogranin A: Positive, CD56: Positive, Ki-67: Positive (60%), PHH-3: Positive (198/10 HPFs)
10. Lymphovascular invasion: Present
11. Perineural invasion: Not identified
12. Resection Margins: Involved by tumor with cautery artifacts
![]() Case 31
Case 31
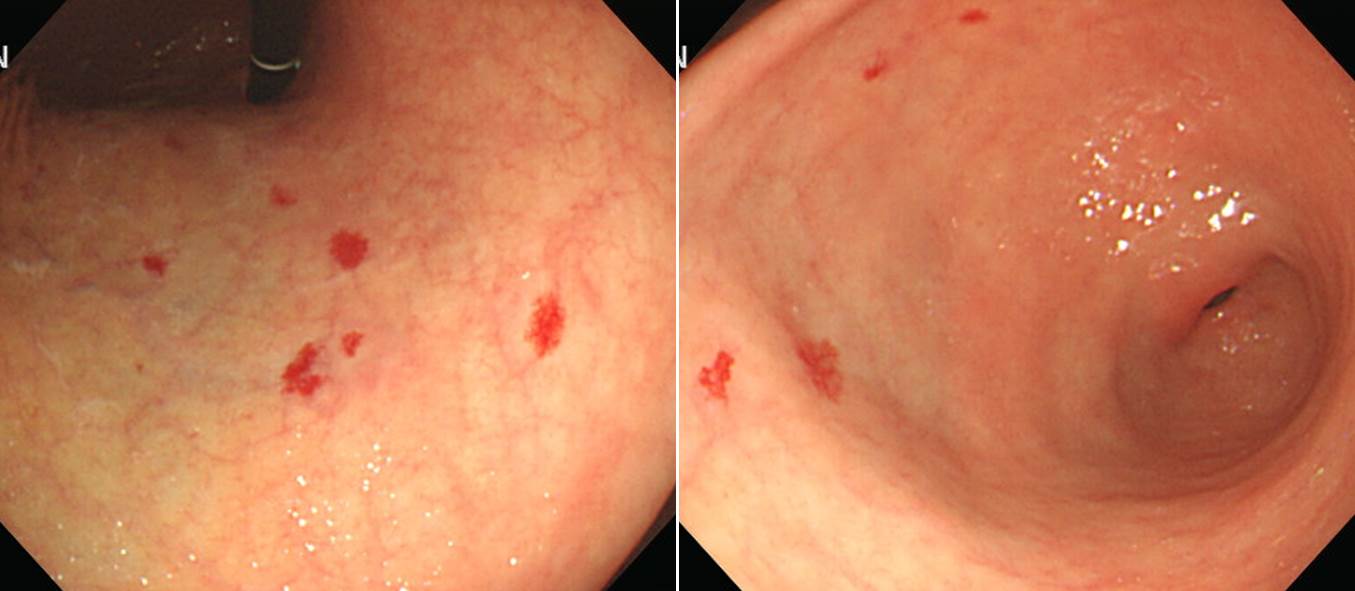
Impression: In the lower body and antrum along lesser curvatur, there area multiple flat hyperemic lesions (= red macules) with vascular patterns in close up.
Impression: Angiodysplasias
[Comment]
Pathogenesis of angiodysplasia (Boley et el. Am J Gastroenterol 1977;72:650)
Angiodysplasia with typical halo
Sometimes, angiodysplasia can be very wide. Biopsy results: submucosal tortuous blood vessels and mucosal congestion strongly suggestive of angiodysplasia
Chronic anemia due to multiple angiodysplasia
Small bowel angiodysplasia (capsule endoscopy)
Small bowel angiodysplasia (capsule endoscopy)
![]() Case 32
Case 32
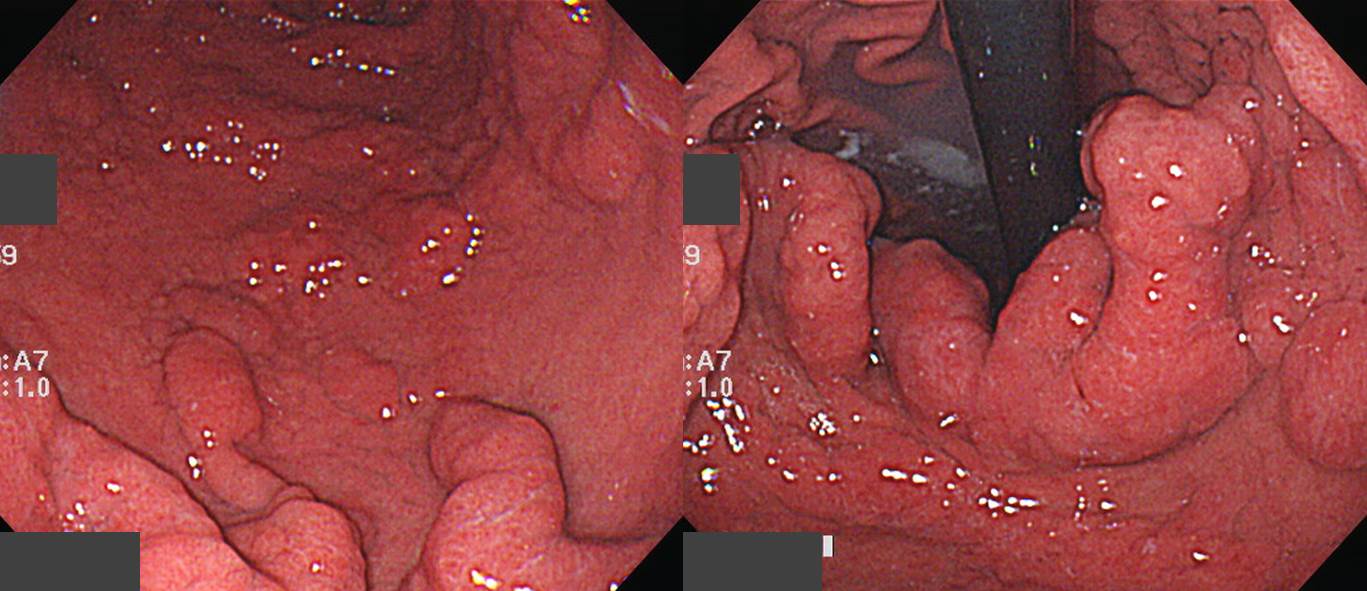
Findings: Gastric folds in the lower body is diffusely thickened and tortuous.
Impression: Hypertrophic gastritis
![]() Case 33
Case 33
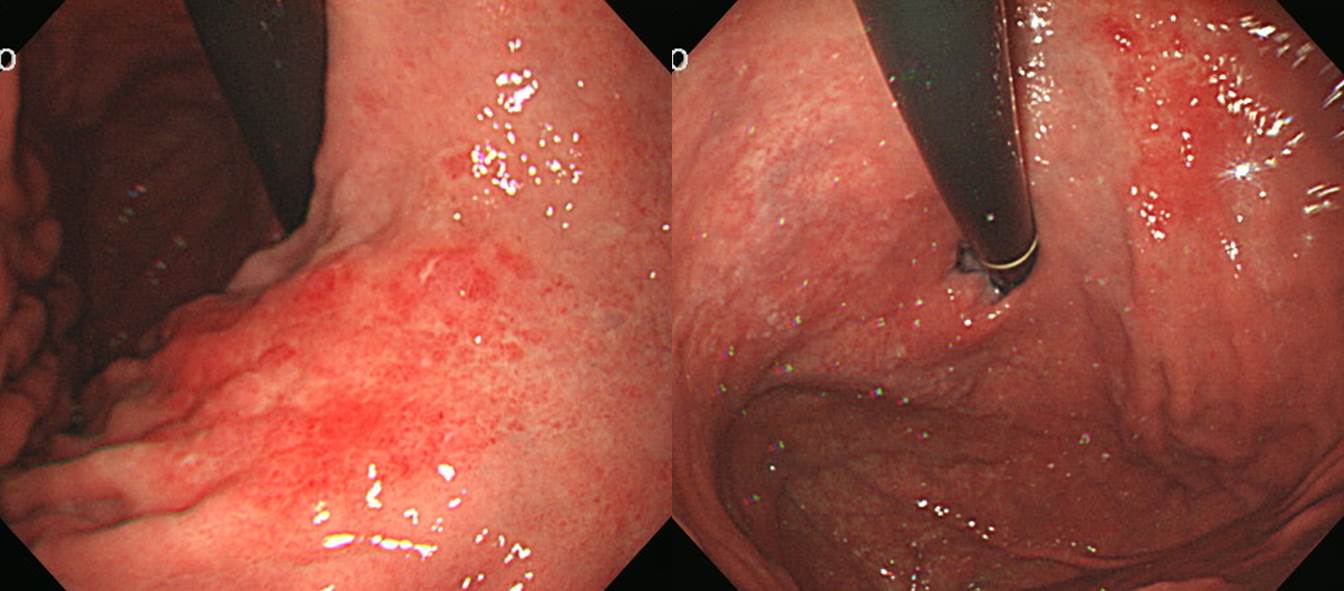
Findings: In the mid to lower body along anteroLC side, a 5cm-sized flat discolorated area with irregular, nodular, hyperremic, uneven surface.
Impression: EGC IIb
[Comment]
The lesion was bigger than endoscopic estimation.
Stomach, total gastrectomy:
Early gastric carcinoma
1. Location : middle third, Center at body and anterior wall
2. Gross type : EGC type IIb
3. Histologic type : signet-ring cell carcinoma
4. Histologic type by Lauren : diffuse
5. Size : 10 x 7 cm
6. Depth of invasion : invades submucosa (sm3) (pT1b)
7. Resection margin: free from carcinoma
8. Lymph node metastasis : no metastasis in 52 regional lymph nodes (pN0)
9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. Peritoneal cytology : negative
![]() Case 34
Case 34
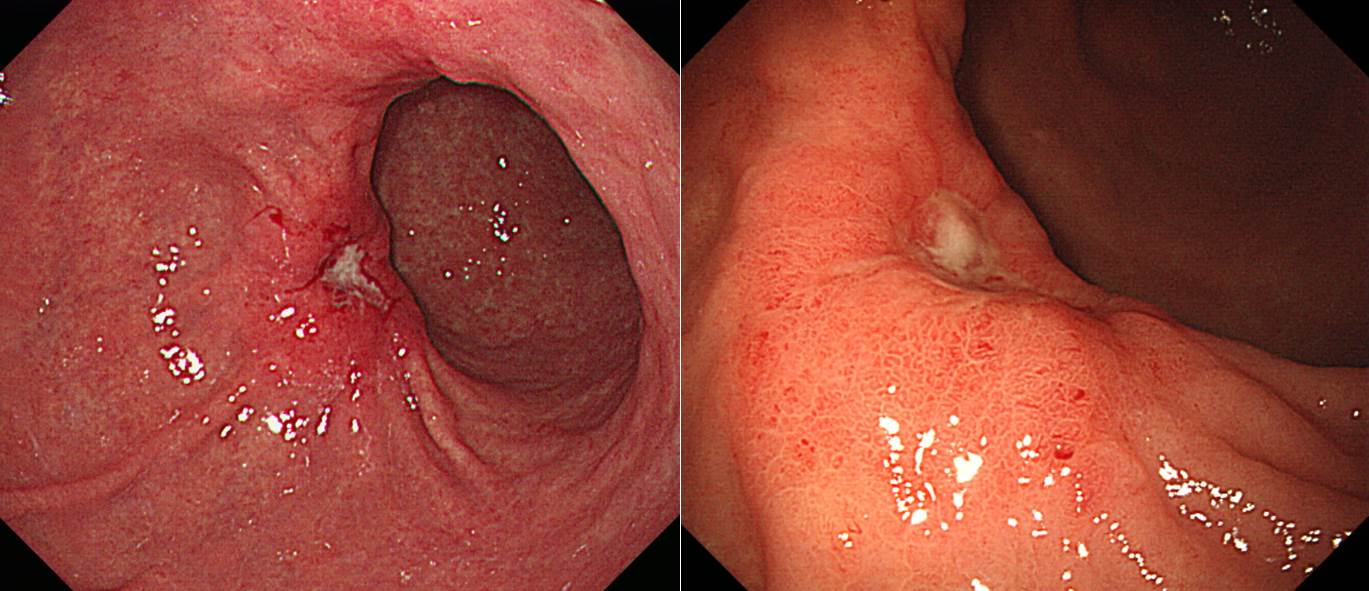
Findings: In the mid-antrum along anterior wall, a 4cm-sized mass with small central ulceration is found. Muliple converging folds are seen.
Impression: AGC, B-III
[Comments]
Stomach, subtotal gastrectomy: Advanced gastric carcinoma
1. Location : middle third, Center at body and anterior wall
2. Gross type : Borrmann type 3
3. Histologic type : signet-ring cell carcinoma
4. Histologic type by Lauren : diffuse
5. Size : 6.5x4.5 cm
6. Depth of invasion : penetrates subserosal connective tissue (pT3)
7. Resection margin: free from carcinoma, safety margin: proximal 2.5 cm, distal 3.5 cm
8. Lymph node metastasis : metastasis to 4 out of 67 regional lymph nodes (pN2), (perinodal extension: present)
9. Lymphatic invasion : present
10. Venous invasion : not identified
11. Perineural invasion : present
12. Peritoneal cytology : negative
13. AJCC stage by 7th edition: pT3 N2
![]() Case 35 - Colon, stomach and duodenum
Case 35 - Colon, stomach and duodenum

Findings: In the cecum and proximal, transverse, descending colon, there are numerous small Is polyps. In the gastric fundus, multiple sessile or semipeduculated polyps are seen. In the second portion of the duodenum, multiple pale sessile polyps are seen.
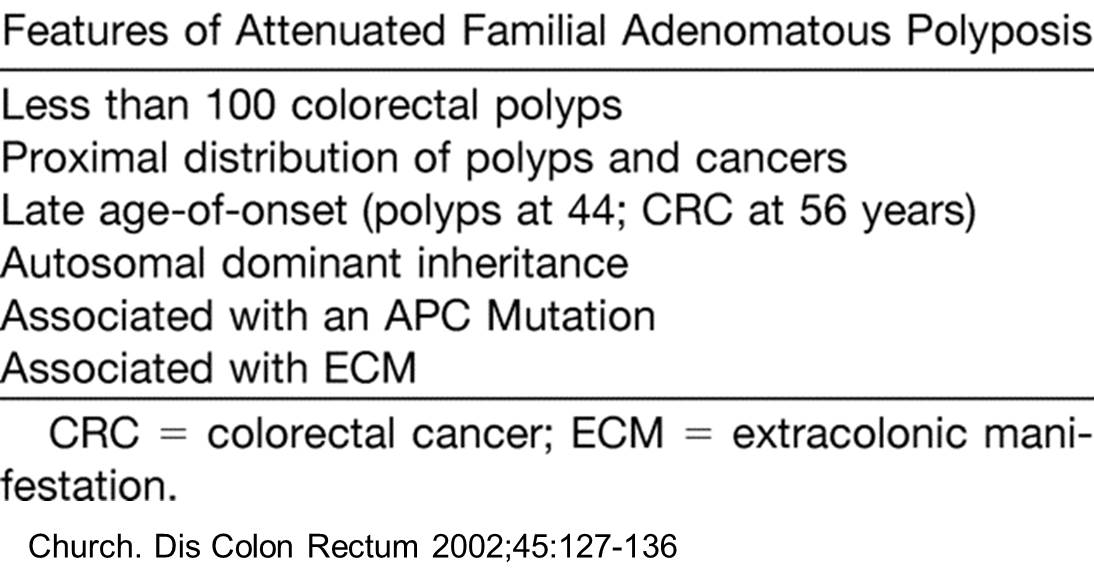
Impression: (1) FAP with colonic polyposis, gastric fundic gland polyposis and multiple small flat duodenal adenomas, (2) R/O Cowden syndrome, less likely
[Comments]
This is typical case of FAP.

© EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.