 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Micrometastasis - an important concern for ESD beyond absolute indication]
[Micrometastasis - an important concern for ESD beyond absolute indication]
Endoscopic resection (ER) is the established treatment for early gastric cancer (EGC) in selected patients with negligible risk of lymph node metastasis (“absolute indication”). Based on the clinical observations and the large pathological databases, expanding indications of endoscopic resection beyond absolute indication has been tried in Japan and Korea. However, there are controversies about the safety of treating EGC beyond absolute indication. One example is concern for micrometastasis.
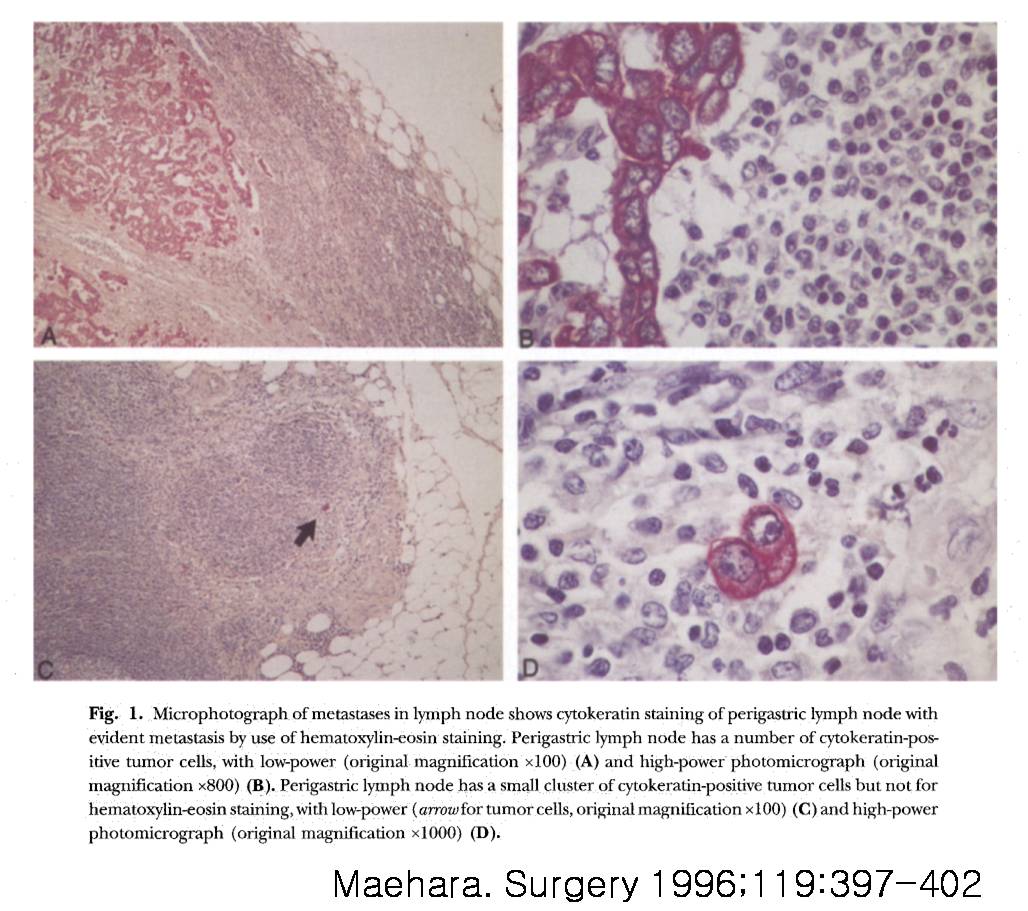
LN micrometastasis has been focused on in various malignant neoplasms. LN micrometastasis is basically defined as the presence of a single or small clusters of gastric tumor cells identified by immunohistochemistry (IHC) in pN0 lymph nodes determined by hematoxylin-eosin (HE) staining.
The incidence of LN micrometastasis ranges from 10% to 36% in patients with pN0 gastric cancer. However, it is controversial whether LN micrometastasis has clinical significance in patients with gastric cancer at present.
In a study of 300 gastric cancer patients with pT1N0 tumor, Morgagni et al.,reported that there were no significant differences in the 10-year overall survival rates among patients with or without LN micrometastasis. In contrast, Cao et al., in a study of 160 gastric cancer patients with pT1N0 tumors, reported that LN micrometastasis was one of the independent prognostic factors in pN0 EGC patients.
There is one important point that we need to consider. I agree that the clinical significance of microstasis is still uncertain in patients who received subtotal gastrectomy AND lymph node dissection already. In ESD patients WITHOUT lymph node dissection, the clinical significance of micrometastasis may be different (actually much dangerous). The risk of micrometastasis in the non-treated lymph node must be higher than the risk of micrometastasis in the dissected lymph node.
In this context, we need to be careful to expand indication of endoscopic resection for EGC based on the surgical database consisting of LN assessments by conventional HE staining.
![]()