 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Expanded indication issue]
[Expanded indication issue]
There is no consensus on the definition of EI (expanded indication). There are two major issues related with the definition of EI; (1) the terminology of differentiated/undifferentiated cancer, and (2) whether undifferentiated cancers can be included in the EI.
According to the WHO classification, gastric cancers are histologically classified as (1) papillary adenocarcinoma, (2) tubular adenocarcinoma (including well differentiated, moderately differentiated and poorly differentiated adenocarcinomas), (3) signet ring cell carcinoma, and other rare subtypes.
In Japan, however, there is a tradition that all gastric cancers are divided into differentiated and undifferentiated gastric cancers (Sugano 1982). Literatures from Japan used this terminology (‘differentiated’ vs ‘undifferentiated’) to describe the indication of endoscopic resection for gastric cancer. This made a great confusion in Korea, where the term ‘differentiated carcinoma’ is not routinely used. Instead, Korean physicians considered that ‘differentiated carcinoma’ in Japan is similar to ‘well-differentiated and moderately differentiated adenocarcinoma’ in Korea. However, there is no direct comparison between them. We don’t know exactly whether ‘differentiated carcinoma’ in Japan is exactly the same with ‘well-differentiated and moderately differentiated adenocarcinoma’in Korea. This problem makes the direct comparison of the data between the two countries difficult.
Most commonly used definition of EI is differentiated cancer with no lymphovascular involvement and (1) mucosal cancers without ulcerative findings, regardless of tumor size; (2) mucosal cancers with ulcerative findings ≤ 30 mm; or (3) minute (< 500 micrometer from the muscularis mucosae) submucosal invasive cancers ≤30 mm. (Reference: Endoscopic and oncologic outcomes after endoscopic resection for early gastric cancer: 1370 cases of absolute and extended indications). In the original review by Soetikno et al,11 gastric cancers were divided into intestinal and diffuse. Only EGCs with intestinal type histology were included in the EI. EGCs with diffuse type histology were not considered as candidates for endoscopic mucosal resection. In some recent Japanese clinical studies, however, small undifferentiated type cancers were also considered as one of EI. ( http://www.ncbi.nlm.nih.gov/pubmed/24520251). It is also true for some reviews by Japanese authors (Gotoda GIE 2008;67;805-807).
In Korea, the situation is very confusing. Some Korean doctors think that poorly differentiated adenocarcinoma or signet ring cell carcinoma cannot be considered as EI. Other Korean doctors think that undifferentiated cancers can be included in EI like Japan. Until now, most Korean endoscopy studies about EI do not included poorly differentiated adenocarcinoma or signet ring cell carcinoma. ESD for poorly differentiated adenocarcinoma and signet ring cell carcinoma have been handled as a separate issue. Jee et al. from Seoul National University Bundang Hospital 20 reported that there were lymph node metastasis in 2.8% (5 patients) of surgically treated EGC within EI of ER. However, 4 out of 5 cases with lymph node positive EGC were poorly differentiated adenocarcinoma or signet ring cell carcinoma. As you can see in this interesting report, some Korean doctors think poorly differentiated adenocarcinoma or signet ring cell carcinoma may be included in the EI. In a recent clinical guideline on the treatment of gastric cancer in Korea, small undifferentiated mucosal cancer is considered as EI of ER. To prevent further confusion, it is urgent to make clear definition of EI in Korea.
![]() [Symposium 기획의도 상세화 방안]
[Symposium 기획의도 상세화 방안]
학술단체에서 주관하는 심포지엄에서 강의 내용의 구성은 누구의 권한일까요?
저는 신문이나 잡지의 편집자가 어떤 역할을 하는지 곰곰히 생각해 봅니다. 아무래도 구체적인 내용은 필자가 구성하지만, 전체적인 흐름은 편집자의 역할일 것입니다. 학회 심포지엄도 강의의 내용은 강사가 구성하지만 전체적인 방향성은 학회에서, 특히 학술위원회에서 정해야 할 것 같습니다.
과거에는 학회의 학술위원회에서 심포지엄 세션 토픽과 강의 제목을 정한 후 연자에게 강의 의뢰를 하였습니다. 그러면 강사는 강의 제목과 심포지엄 토픽을 잘 보고 적절히 강의 내용을 구성하였습니다. 대부분 강의는 무난하게 진행되지만, 학술위원회에서 강의를 의뢰한 방향성과 영 다른 강의도 없지 않습니다.
최근에는 심포지엄 세션별로 간단한 기획의도를 붙이는 것이 유행입니다. 그러나 이러한 기획의도는 강사를 위한 것이라기보다는 청중을 위한 것이었습니다. 강사는 여전히 제목을 보고 뭘 요구하는지 상상하는 수 밖에 없는 상태입니다.
저는 학술위원회에서 강사들에게 아주 구체적인 기획의도를 알려드리면 어떨까 생각해 보았습니다. 마침 심포지엄 토픽이 작아 강사들의 강의 내용이 겹칠 위험이 큰 경우를 만났습니다. 장문의 기획의도를 보내드려보았습니다.
심포지엄 - Updates on Neuroendocrine Tumor
기획의도: Gastric neuroendocrine tumor의 진단과 치료에 대하여 심도있게 논의하는 시간을 마련하였습니다.
강사 1 교수님께: 비록 병리과에서는 여러 번 강의되고 논의된 주제라는 점을 잘 알고 있지만, 소화기내과 의사들은 아직도 neuroendocrine tumor의 개념과 분류에 대한 질문을 많이 가지고 있습니다. 임원 위원 워크샵이므로 너무 기초적인 것은 강의에 넣지 않으셔도 좋은데요… 저희의 궁금증에 대한 답변을 강의에 포함시켜 주시면 감사하겠습니다. (a) 최근 진단에 사용되는 병리학적 분류는 어떤 것입니까? 이러한 병리학적 진단을 내리는 과정에서 chromogranin등 면역형광marker 혹은 serum marker는 어떻게 이용되고 있습니까? (b) 병리학적으로 type 1/2와 type 3를 나눌 수 있는 clue는 없습니까? Serum gastrin level이 중요하다고 생각하십니까? 아니면 background gastric mucosa의 atrophy가 중요하다고 생각하시는지요? (c) Enterochromaffin-like cell이 어떠한 것인지요? Neuroendocrine hyperplasia 혹은 dysplasia가 무엇인지, 병리학적 진단은 어떻게 내리는 것인지, NE tumor와의 구분은 어떻게 되는지, 임상적 의의는 무엇인지 궁금합니다. 아울러 micronodular hyperplasia, adenomatoid hyperplasia 등의 개념이 실제로 이용되고 있는지요? (d) Behavior code라는 것이 정확히 어떤 의미를 가지는 것입니까? Behavior code를 가지고 D code 혹은 C code를 나누는 기준이 될 수 있을까요? 2008년 발표하신 coding에 대한 병리학자들의 survey결과가 의미하는 바가 무엇입니까? 선생님은 5 mm 정도의 type I gastric neuroendocrine tumor가 C로 coding되어야 한다고 생각하십니까? 아니면 D로 coding되어야 한다고 생각하십니까? (e) Gastric neuroendocrine tumor와 colorectal neuroendocrine tumor의 차이점은 무엇입니까? (f) 2012년 Cancer Res Treat에 발표된 국내 gastroenteropancreatic neuroendocrine tumor에 대한 조사결과도 간단히 소개해 주시면 좋겠습니다.
강사 2 교수님께: 직장 carcinoid가 많은 것으로 알고 있습니다. 이에 대한 평이한 수준의 강의를 해 주시면 되는데 이슈가 되는 포인트만 잘 짚어주시면 되겠습니다. 저희가 관심이 있고 궁금한 것은 다음과 같습니다. (a) 내시경 치료와 TEM등 수술적 치료의 선택기준은 무엇입니까? (b) 내시경 치료나 수술적 치료 후 lymph node metastasis의 risk 때문에 개복수술 혹은 복강경 수술을 권하는 기준은 무엇입니까? (c) 실제 우리나라에서 rectal carcinoid 치료 후 systemic recur를 보인 증례는 얼마나 있습니까? (d) 모든 선생님께 질문드립니다. C code 혹은 D code를 부여하는 선생님의 방식을 소개해 주시기 바랍니다.
강사 3 교수님께; 임원 위원 워크샵이므로 너무 평이한 내용보다는 궁금증 위주로 강의해 주시면 감사하겠습니다. 강사 4 선생님과 강의 내용이 너무 겹치지 않기를 바랍니다. 두 분이 서로 사전에 소통해주시면 감사하겠습니다. 다음 내용이 포함되었으면 좋겠습니다. (a) Gastric neuroendocrine tumor의 내시경 소견을 이번 기회에 정리해 주시기 바랍니다. 특히 multiple gastric neuroendocrine tumor의 경우에 어떻게 하시는지요. (b) Gastric neuroendocrine tumor의 진단에서 serum marker의 역할은 무엇입니까? (c) Rindi type을 구분함에 있어서 serum gastrin 만을 고려하지는지요. 아니면 내시경 육안소견의 atrophy를 함께 고려하시는지요? 혹시 조직검사를 시행하여 atrophy 여부를 확인하고 계십니까? (d) Gastric neuroendocrine tumor의 진단과 치료에서 Helicobacter pylori는 어떠한 의미가 있다고 생각하시는지요? (e) 내시경 치료의 증례와 tip을 소개해 주시기 바랍니다. (f) 모든 선생님께 질문드립니다. C code 혹은 D code를 부여하는 선생님의 방식을 소개해 주시기 바랍니다. (g) Type I multiple gastric neuroendocrine tumor에 대하여 치료 없이 경과관찰하는 전략에 대한 선생님의 의견도 부탁합니다. 이 부분은 강사 4 선생님께도 부탁할 것입니다. 상세히 다뤄주시면 감사하겠습니다.
강사 4 교수님께: Gastric neuroendocrine tumor에 대하여 준비해 주시면서 식도 혹은 십이지장에 대해서도 살짝 언급해 주시면 감사하겠습니다. 강사 3 선생님과 강의 내용이 너무 겹치지 않기를 바랍니다. 이에 대하여 두분이 서로 사전에 소통해주시면 감사하겠습니다. (a) Rindi classification에서 gastrin이 100이하이면 type III입니다. 종양은 작은데 type III로 나오는 경우 어떻게 할 것인지 궁금합니다. 내시경 치료가 가능할지요? 아니면 Rindi의 방식대로 aggressive하다고 보고 적극적인 치료를 해야 하는 것인지요? (b) Surgical resection의 경우 보다 aggressive한 치료가 좋다고 생각하시는지 아니면 wedge resection등의 less invasive한 치료도 충분하다고 보시는지요? (c) Neuroendocrine carcinoma로 나온 증례를 보여주시면서 이에 대한 설명을 해 주시면 감사하겠습니다. (d) 식도의 neuroendocrine tumor에 대한 언급을 부탁합니다. (e) 십이지장 neuroendocrine tumor에 대한 언급을 부탁합니다. 내시경 치료시 천공의 위험은 얼마나 되는 것입니까? (f) 모든 선생님께 질문드립니다. C code 혹은 D code를 부여하는 선생님의 방식을 소개해 주시기 바랍니다. (g) Type I multiple gastric neuroendocrine tumor에 대하여 치료 없이 경과관찰하는 전략에 대한 선생님의 의견도 부탁합니다. 이 부분은 강사 3 선생님께도 부탁할 것입니다. 상세히 다루어 주시면 감사하겠습니다.
대한상부위장관헬리코박터학회 동계워크샵 (PDF, 3.6 M) 준비과정에서 위와 같은 방식으로 강사들에게 상세한 기획의도를 전달하였습니다. 고맙게도 강사님들께서 기획의도를 충실히 고려하여 강의를 해 주셨습니다. 서로간의 겹치는 부분이 최소화된 상태에서 논점이 명확히 정리되었습니다. 좋은 방식이라고 자체평가를 하였습니다.
![]() [2014-4-14. 애독자 의견] 교수님, 안녕하세요? 엔도투데이 감사히 잘 받아읽고 있는 애독자입니다. 얼마전 한 학술모임에서 느낀 점입니다. 교수님께서 지적하신 기획의도라는 관점에서 일부강의에서 상당히 마음이 불편했습니다. '사전에 조율이 없었나? 도대체 뭘 확인하고 싶은거지?'라는 생각이 들었습니다. 강의가 끝나고 질문이 가이드라인 정도는 슬라이드에 넣었어야 하는거 아니냐, 강의슬라이드 구성은 어떻고, 다른나라 데이터는 결과가 그렇지 않다는 등...... 누가 누구를 지적할 상황이 아니였습니다.
[2014-4-14. 애독자 의견] 교수님, 안녕하세요? 엔도투데이 감사히 잘 받아읽고 있는 애독자입니다. 얼마전 한 학술모임에서 느낀 점입니다. 교수님께서 지적하신 기획의도라는 관점에서 일부강의에서 상당히 마음이 불편했습니다. '사전에 조율이 없었나? 도대체 뭘 확인하고 싶은거지?'라는 생각이 들었습니다. 강의가 끝나고 질문이 가이드라인 정도는 슬라이드에 넣었어야 하는거 아니냐, 강의슬라이드 구성은 어떻고, 다른나라 데이터는 결과가 그렇지 않다는 등...... 누가 누구를 지적할 상황이 아니였습니다.
새벽부터 집에서 나와 학회 강의를 듣고 있던 저는 그런 질문이 오고가니 참 힘이 빠지더군요. 당황스럽기도 했구요. 제목만 보고 강의내용의 방향을 알기 어려운 경우도 있습니다. 더구나 동시강의가 진행되는 학회의 경우는 더더욱 기획의도를 읽어보고 학회에서 어떤 강의를 들을지 결정하게 됩니다.
학회발표는 연자가 학회의 테스트를 받는 자리가 아니라고 생각합니다. 청중이 돈(때론 무료이기도 하지만)과 시간을 들여 전문가의 강의를 듣고 또한 전문가들의 발전적인 활발한 의견교환이 이루어지는 장이 되었으면 합니다. 교수님의 기획의도에 대한 의견에 공감합니다. 늘 감사합니다.
![]() [2014-4-15. 이준행 답변] 좋은 의견입니다. 저도 그 학술모임의 말씀하신 세션에 청중으로 앉아 있었습니다. 저도 조그마한 학회의 학술위원장으로 일하고 있으므로 안타까운 마음으로 지켜보았습니다. 선생님의 말씀에 동의합니다. 준비가 부족해 보였습니다.
[2014-4-15. 이준행 답변] 좋은 의견입니다. 저도 그 학술모임의 말씀하신 세션에 청중으로 앉아 있었습니다. 저도 조그마한 학회의 학술위원장으로 일하고 있으므로 안타까운 마음으로 지켜보았습니다. 선생님의 말씀에 동의합니다. 준비가 부족해 보였습니다.
저는 세미나, 심포지엄의 강의 내용과 presentation 품질을 높이는 방안을 늘 고민합니다. 일전의 심포지엄 기획의도 상세화방안에서 말씀드렸듯이 현재의 잠정적 결론은 '학술위원장은 감독이 되어야 한다'는 것입니다. 영화감독, 드라마 연출과 비슷한 역할을 해야 한다는 것이지요. 강사에게 제목만 던져주고, 강의시간 20분의 내용과 진행을 알아서 하라는 것으로는 부족하다는 문제의식을 가지고 있습니다.
그런데 이게 쉽지 않습니다. 강의 제목만을 알려주면서 강의를 의뢰하는 관례때문입니다. 제가 드물게 해외에서 강의하는 경우에도 그쪽에서 강의제목만 보내옵니다. 구체적으로 어떻게 강의를 구성해 달라고 요청하지는 않습니다. 대부분의 국내 학회도 같은 전통을 가지고 있습니다. 제목만 알려 주는 것이지요. 그러면 어떤 학회의 어떤 모임인지, 내 세션의 큰 제목은 무엇인지, 다른 강사의 제목은 무엇인지 잘 보고 상상력을 동원하여 나의 강의 내용을 구성하는 수 밖에 없습니다. 사실 기획의도라는 것이 우리나라 소화기학회나 유관학회에 도입된 것도 제가 학술위원으로 일할 때 제안한 방식입니다. 현재는 형식적으로 운영되고 있어서 아쉽기는 합니다만...
요즘 저는 이렇게 생각합니다. 학술모임의 성격에 따라 나눠야 할 것 같습니다. 연구와 교육을 나누는 것이지요. 연구자들이 새로운 것에 대하여 치열하게 논의하는 자리에서는 제목만 주면 충분할 것 같습니다. 정기 학술대회의 invited speaker session이 그렇습니다. 전적으로 강사의 재량에 의존하는 것이지요. 그러나 보통 회원을 대상으로 한 교육 목적의 심포지엄/세미나에서는 강의 제목뿐만 아니라 강의 내용, 수준, 기타 자세한 detail까지 학술위원회에서 검토할 필요가 있습니다. 어떤 학회에서는 강사들이 미리 모여 강의내용을 논의하고, Powerpoint 중간원고를 함께 보면서 예행연습을 하고, 겹치는 것은 빼고 줄이는 것은 보충하기도 합니다. 심지어는 심포지엄 전체의 Powerpoint format까지 통일하여 잘 연출된 하나의 작품으로 만드는 곳도 있습니다 (응급의학과가 그렇습니다). 똑같이 따라할 필요는 없겠지만 이런 저런 학회의 다양한 예를 참고하여 우리 소화기학계도 변신을 도모해야 합니다. 아이디어를 내야 합니다. 좀 더 다양한 시도가 필요합니다.
저는 최근 외부 전문가(병리과 교수님)를 모시고 진행하는 세미나를 기획하고 있습니다. 어떻게 하면 소화기내과 의사들에게 도움되는 강의내용을 이끌어 낼까 고민하다가 장문의 강의 요청을 보내는 방법을 시도했습니다. "자료를 준비하면서 아래를 참고해 주시면 매우 좋을 것 같습니다"라는 말과 함께 제가 이해하는 내용과 궁금한 점을 써 보냈습니다. 무례는 아닌가 살짝 걱정되기도 했지만, 그 병리과 선생님께는 과거에도 비슷한 방식으로 강의요청을 한 적이 있기 때문에 저의 의도를 이해하여 주실 것 같았습니다. 아직도 더 좋은 방법은 없는지 고민하고 있습니다.
제가 병리과 선생님께 강의 내용을 구성하면서 참고해 달라고 보낸 내용입니다. 장문의 강의요청서라고 보시면 됩니다.
1. 우리나라 소화기 병리의사들이 undifferentiated carcinoma라는 용어를 사용하는 방법 - 정확히 WHO 기준에 따르고 있습니다.
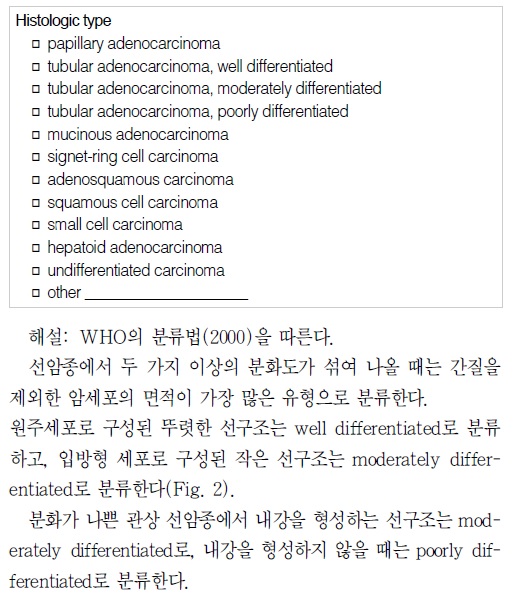
2014년 현재까지 우리나라 위암병리판독의 기준으로 간주되는 2005년 대한병리학회 소화기병리학연구회의 위암 병리보고서 기재사항 표준화 (PDF 0.3M)에는 (1) 위암의 histologic type은 2000년 WHO 분류를 따름, (2) 두 가지 이상의 분화도가 섞여 나올 때는 간질을 제외한 암세포의 면적이 가장 많은 유형으로 분류함, (3) 선구조나 편평상피 분화가 없는 경우에는 undifferentiated carcinoma로 분류함을 명확히 밝히고 있습니다 (아래 그림 참조).

유명한 일본위암분류(1998)에 따르면 일본에서 외과의사들이 이해하는 위암의 조직학적 분류는 아래 그림과 같습니다. "The histological classification should be based on the prominant pattern of tumor"라고 언급하고 있습니다. 여기서 "prominant"는 우리나라 위암 병리보고서 기재사항 표준화(2005)에서 언급한 "암세포의 면적이 가장 많은 유형"과 비슷한 의미로 생각됩니다.

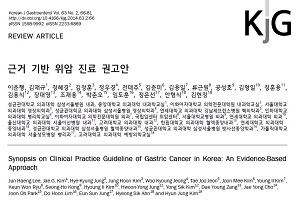
우리나라에서 최초로 시도된 다학제 위암진료권고안(제가 간사로 참여하였습니다)에서는 (1) 선구조를 만드는 면적이 95% 초과하면 고분화형, (2) 선구조를 만드는 면적이 50-95%면 중분화형, (3) 선구조를 만드는 면적이 49%이하면 저분화형으로 언급하고 있습니다.
Histological classification of gastric adenocarcinoma for epidemiological research: concordance between pathologists. Shibata et al. Cancer Epidemiol Biomarkers Prev 2001
Diagnosis of gastric epithelial neoplasia: Dilemma for Korean pathologists. Kim JM et al. World J Gastroenterol 2011 (PDF)Two pathologists, each blinded to the other's assessment, reviewed H&E-stained slides of gastric tumor... Concordance for tumor grade was 87%, with a kappa coefficient of 0.72 (95% confidence interval, 0.57-0.87).
Korean pathologists experience much difficulty making a diagnosis because we are influenced by Japanese pathologists as well as Western medicine. Japan is geographically close to Korea, and academic exchanges are active. Additionally, Korean doctors are familiar with Western style medical terminology. As a result, the terminology, definitions, and diagnostic criteria for gastric intraepithelial neoplasia are very heterogeneous in Korea.
Differences between biopsy- or specimen-related Lauren and World Health Organization classification in gastric cancer. Flucke, et al. World J Surg 2002
Out of 48 tumors with preoperative diagnosis of an intestinal type, 10 tumors (20.8%) exhibited a diffuse growth pattern in the gastrectomy specimens; and 16% of the cases showed a disagreement of the pre- and postoperative histopathological type according to the WHO classification.
Expression of E-cadherin, beta-catenin, CD44s and CD44v6 in gastric adenocarcinoma: relationship with lymph node metastasis. Joo et al. Anticancer Res 2003
Expressions of CD44s and CD44v6 play an important role in tumor progression; especially, CD44v6 expression may be a useful predictor of lymph node metastasis, while the expressions of E-cadherin and beta-catenin complex are more probably related to tumor morphology than to tumor progression.
Poorly differentiated component in gastric pinch biopsies predicts submucosal invasion. Lee SM. Diagn Pathol 2014
Poorly differentiated component and papillary architecture are significant histopathologic predictors of SM invasion in pretreatment gastric biopsies of lesions considered for endoscopic therapy.
This is my conceptual model of histological differentiation of early gastric cancer. There are two dominant types of histology. One is differentiated type, and the other is undifferentiated type. However, there are a lot of cases in the middle. We don’t know exactly how many patients are included in this mixed area.
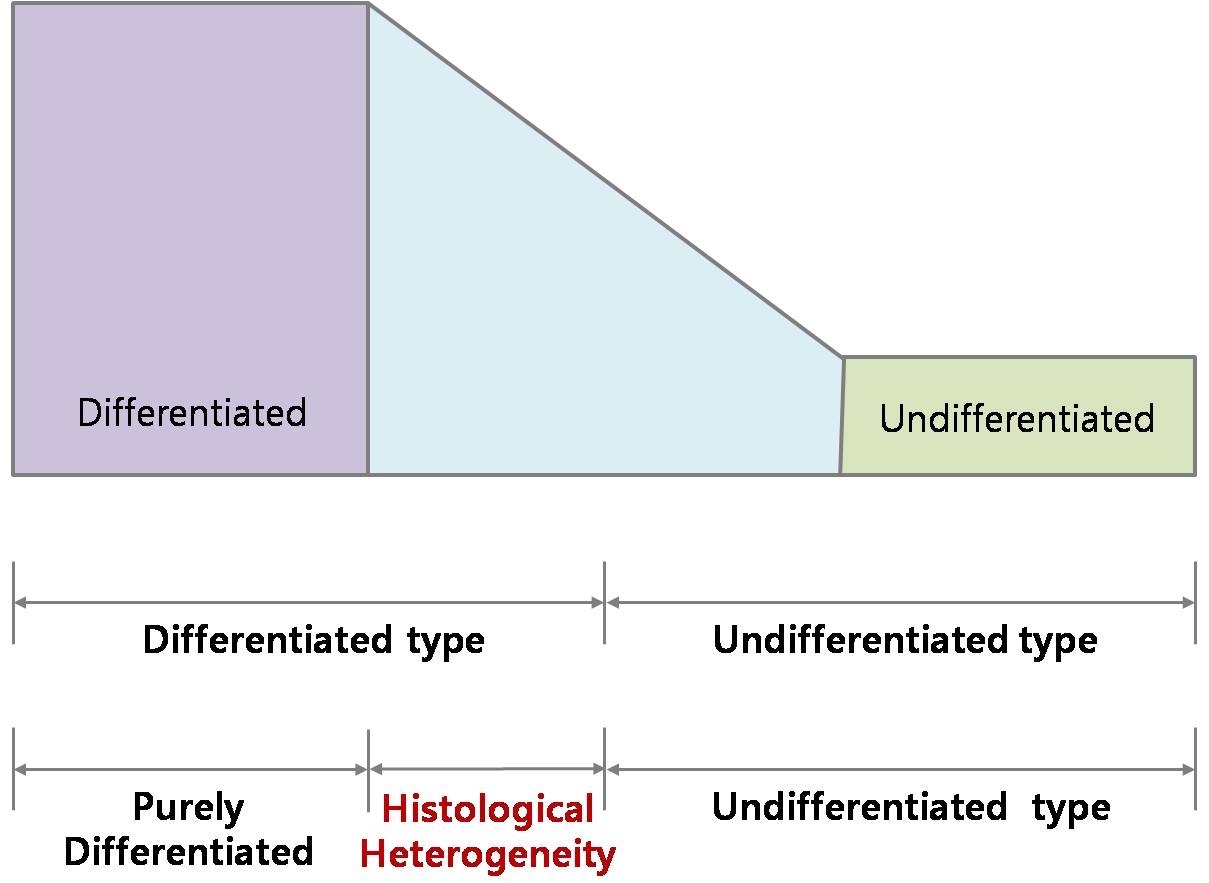
Usually, the histological grouping is made by the major area of histological differentiation. For example, if 70 percent of area shows undifferentiated histology, we call it undifferentiated type of early gastric cancer like the blue arrow. If 80 percent of area shows undifferentiated histology, we call it differentiated type of early gastric cancer like the red arrow. The concept of histological heterogeneity comes from this area. EGC cases mixed with undifferentiated component less than 50 percent of area can be called as histological heterogeneity. And we evaluated cases in this unique group of patients.
1) 우리나라, 일본, WHO의 위암 분화도 판정 기준은 개념상 (definition에서) 차이가 있습니까?
2) 우리나라 병리의사들의 위암 분화도 판정 기준은 개념상 통일되어 있습니까? 실제로는 어떻습니까?
3) 일본 병리의사들의 위암 분화도 판정 기준은 개념상 통일되어 있습니까? 실제로는 어떻습니까?
4) 내시경 조직검사에 대한 위암 분화도 판정의 interobserver variation과 intraobserver variation은 어느 정도입니까?
5) 수술 조직에 대한 위암 분화도 판정의 interobserver variation과 intraobserver variation은 어느 정도입니까?
6) EMR/ESD 조직에 대한 위암 분화도 판정의 interobserver variation과 intraobserver variation은 어느 정도입니까?
7) 위암 조직검사 분화도와 내시경치료 혹은 수술 후 검체에서 분화도가 달라지는 경우는 어느 정도입니까? 특히 W/D 혹은 M/D에서 P/D 혹은 signet ring cell carcinoma로 바뀌는 경우는 어느 정도입니까? 그 반대는 어느 정도 입니까?
8) 우리나라의 다학제 위암진료권고안에서 언급된 "조직형의 분류가 어려운 경우 면역조직화학염색 또는 조직화학염색을 시행하여 도움을 받을 수 있는 경우"는 어느 정도입니까? Tubular adenocarcinoma에서도 그러한 경우는 어느 정도 있습니까?
9) Histological heterogeneity란 어떤 개념입니까? 이것이 조직검사와 치료 후 최종병리결과의 분화도 차이에 미치는 영향은 어떠합니까?
![]()