Previous | Home | EndoTODAY | List | Next
![]() 대장내시경 검사시간에 대한 이틀 전 EndoTODAY에 대하여 S 대학 C 교수님께서 촌평을 보내오셨습니다. "간단하게 생각합시다. 웬만하면 6 분 이상 봅시다."
대장내시경 검사시간에 대한 이틀 전 EndoTODAY에 대하여 S 대학 C 교수님께서 촌평을 보내오셨습니다. "간단하게 생각합시다. 웬만하면 6 분 이상 봅시다."
![]() [Endoscope insertion]
[Endoscope insertion]
[애독자 질문] 도저히 해결되지 않는 문제가 있어서 여쭈어봅니다. 처음에는 이상동으로 진입을 하니 환자들의 구역질이 심하였습니다. 그러다 여러 선배들의 도움으로 정중앙에서 하는 것이 편하다는 것을 알게 되어 그렇게 하고 있습니다. 문제는 그렇게 하고 나니 환자들 사래가 걸리는 일이 많아졌습니다. 이상동으로 들어갈때는 구역질 및 통증으로 처음에는 힘들지만 EGJ 넘어가면 환자들이 진정이 되는 반면, 사래는 일단 생기면 이건 2-3분동안 계속 기침을 하는 것이 여간 신경쓰이는 것이 아닙니다. 빈도도 10명 중의 1-2명 정도는 사래가 걸리는 것 같습니다. 다른 분들께 여쭈어보니 skill 부족이라고 하는데, 사래를 줄이기 위한 skill로는 어떠한 것이 있는지 여쭈어 보고 싶습니다.
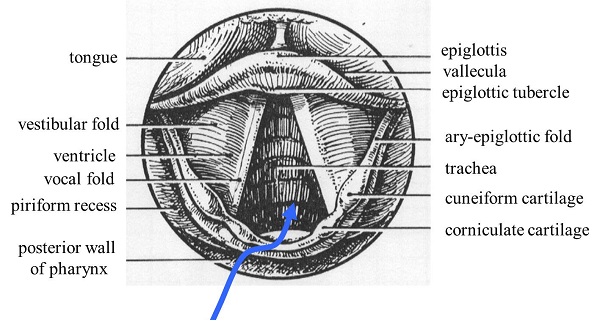
[이준행 답변] Inserting endoscope (내시경 삽입법)을 참고하시기 바랍니다. 특히 이상동보다 중앙쪽으로 잘 들어간다는 것은 아래 내용과 관련된 것입니다. Pyriform sinus로 넣는다고 생각하면 내시경 끝이 자꾸 바깥쪽을 향하게 됩니다. Pyriform sinus를 통하여 중앙으로 들어간다는 느낌이 좋습니다.
화면 좌측 pyriform sinus에 내시경이 도달하면 내시경 끝이 가운데를 향하도록 조작하면서 조심스럽게 밀어 넣습니다. Pyriform sinus로 진입하는 각도가 바깥 쪽을 향하는 경우가 많기 때문에 가운데로 넣는다는 느낌을 잊지 말아야 합니다. Knob를 이용할 수도 있지만, 그보다는 내시경을 시계방향으로 돌리면서 좌측 손을 올려주면 자연스럽게 가운데를 향하여 들어가게 됩니다.

사래를 줄이기 위한 skill에는 정답이 없습니다. 잘 하는 수 밖에...... 문제는 사람마다 다르다는 것입니다. 기본 술기는 inserting endoscope (내시경 삽입법)를 보시고 그 이상은 선생을 찾아가십시요. 내시경의 섬세한 술기를 글로 알려드릴 방법을 저는 알지 못합니다. 내시경 술기를 글로 가르치는 것은 '라디오 발레 강의'와 비슷합니다. 발을 꼿꼿이 세우고, 허리에 힘을 빼고, 양 팔을 95도 정도 올리고, 1초에 3번 반 속도로, 반시계 방향으로 4초 동안, 새벽 햇살을 받으면서 기지개를 펴는 백조와 같은 느낌으로, 부드럽게 그러나 약간 도도한 느낌으로 돌아 보십시요. 잘 될까요?
가까운 대학병원 내시경실을 찾아가 경험 많은 교수님께 직접 배우시기를 권합니다. 배우러 오겠다는데 막는 사람 없습니다 (만약 그런 사람이 있다면 욕하십시요. 많이 욕하십시요. 저는 아직까지 한번도 그런 사람을 본 적이 없습니다). 배우러 오는 사람이 없어서 문제지, 선생이 없어서 문제는 아닙니다. 기본 술기는 도제교육밖에 없습니다. 학회에서 배울 수 없습니다. 내시경 세미나에서 배울 수 없습니다. 기본을 익히고 난 이후에 학회도 있고 세미나도 있습니다. 목구멍 넘기기는 도제교육밖에 없습니다. 2-3일 휴가를 내시고, 아침 일찍 내시경실로 찾아가기를 강력히 추천합니다.
![]() 사대주의의 여파가 사라지지 않고 있습니다. 해외 유명 저널에 실린 논문때문에 좋은 대학의 교수로 임용되는 관행이 계속되는 한 논문 사기는 없어지지 않을 것 같습니다. 언제까지 이런 기사를 읽어야 하는 것일까? 영어 논문 1개 보다는 그 사람의 평소 행실, 동료 사이의 reputation 등이 더 중요한 것 아닐까요? JCI 논문에 연연하는 것은 사대주의의 잔재가 남아있기 때문입니다. 우리나라 사람이 쓴 우리말 논문이 떳떳하게 인정받는 시대는 올까요? 요원하다고 봅니다. 저는 계속 우리말 논문을 쓸 것입니다.
사대주의의 여파가 사라지지 않고 있습니다. 해외 유명 저널에 실린 논문때문에 좋은 대학의 교수로 임용되는 관행이 계속되는 한 논문 사기는 없어지지 않을 것 같습니다. 언제까지 이런 기사를 읽어야 하는 것일까? 영어 논문 1개 보다는 그 사람의 평소 행실, 동료 사이의 reputation 등이 더 중요한 것 아닐까요? JCI 논문에 연연하는 것은 사대주의의 잔재가 남아있기 때문입니다. 우리나라 사람이 쓴 우리말 논문이 떳떳하게 인정받는 시대는 올까요? 요원하다고 봅니다. 저는 계속 우리말 논문을 쓸 것입니다.
[2013-11-8. KBS] 한국 과학자 저명 논문 2편 조작 논란 파문
<앵커 멘트> 한국인 과학자들이 세계적인 학술지에 실린 논문 조작의혹에 휩싸였습니다. 당시 연구의 총 책임자였던 한국과학자들의 지도교수가 직접 논문의 오류를 인정하고 논문을 철회했습니다.
<리포트> 지난 2009년 과학전문지 '사이언스'에 실린 논문입니다. 한국인 연구원 2명이 제1저자로 벼에 특정 단백질을 주입하면 병원균에 대한 면역 반응을 일으킨다는 내용입니다. 벼의 병충해를 예방할 수 있는 획기적인 논문으로 인정받아 관련 논문이 2011년 플로스 원이라는 학술지에도 실렸습니다. 저자 2명은 이 업적 등을 인정받아 2010년과 지난해 국내 대학교수로 임용됐습니다. 그런데 최근, 이 연구의 지도교수였던 미국 캘리포니아 데이비스대학 로널드 교수가 이 논문 2편을 철회했습니다. 실험을 반복해도 면역과 관련된 논문의 결과가 나오지 않았고 다른 균주를 사용해 실험해봤지만 벼에 영향을 주지 못했다는 겁니다. 생명과학계에서는 실험이 재현되지 않는다면 논문 조작이라고 보고 있습니다.
<인터뷰> 황은성(서울시립대 산학협력단장) : "실수에 의해서 일어날 수 있고 또 하나는 누군가가 의도를 갖고 일어날 수 있는데 " 해당 교수들은 과정의 오류는 인정했지만 조작 의혹은 부인했습니다.
<녹취> A교수(제1저자) : "다른 연구원이 그 균주를 만들었어요. 이제 걔가 만들어서 연구실 사람들한테 쓰라고 나눠준 거죠." 교수들이 재직하고 있는 대학들은 논문 조작 여부를 조사해 임용취소 여부를 결정하기로 했습니다.황우석 사태로 추락했던 한국 과학자들에 대한 신뢰가 다시 한번 위기를 맞고 있습니다.
![]() 왜 의사들은 아파도 쉬지 않고 일을 할까요? Ofri는 이렇게 말하고 있습니다. "Somewhere, deep down, I needed to convince myself that we doctors were a different species from our patients."
왜 의사들은 아파도 쉬지 않고 일을 할까요? Ofri는 이렇게 말하고 있습니다. "Somewhere, deep down, I needed to convince myself that we doctors were a different species from our patients."
[2013-11-17. New York Times] Why Doctors Don’t Take Sick Days

THE bottle of Maalox sat perched on the triage desk in the emergency room. It was mint flavor, or maybe lemon ? I don’t recall exactly ? but it shimmered temptingly. I had just finished with a new admission, and my stomach had been groaning ominously for hours. It was after midnight, the whole night was still ahead of me, and I was getting desperate. I scribbled the last of my medication orders and snagged the Maalox bottle, popping the top and chugging two revolting capfuls on my way to the elevator.
As I rode upstairs, I could feel the intestinal protestations growing. There was going to be an apocalyptic resolution to this. The elevator opened and I burst into the restroom, just in time to disgorge the Maalox and everything else into the toilet, conscientiously keeping my white coat and stethoscope clear of the fray.
I staggered into the call room and flopped onto the couch. My fellow resident listened to my tale of gastrointestinal woe and did what any residency buddy would do: he slid an 18-gauge IV into my antecubital vein and strung up a bag of IV saline. I spent the pre-dawn hours prostrate on the couch doing phone work ? renewing medications, answering calls from nurses, ordering labs ? while my colleagues did the foot work on the wards and in the emergency room. Together we kept everything running.
After morning rounds, I caught a few hours of sleep at home, showered, and then reported back to the hospital at 10 p.m. for my next shift.
What I didn’t do was call in sick.
It has long been known that doctors make the worst patients. From day one in medical training, the unspoken message is that calling in sick is for wimps. Much of this is logistics. The staff has to scramble to reschedule patients ? many of whom have been waiting weeks or months for their appointments. Patients who need medical attention that day are crammed into someone else’s schedule or sent to the emergency room. Your already overworked colleagues are saddled with extra work, and patients usually get the short end of the stick.
So most doctors ignore their symptoms and resist taking the day off unless they are sick enough to be hospitalized in the next bed over.
This, of course, is ridiculous behavior on the part of medical professionals who would never recommend such nonsense to their patients. Medical workers with respiratory infections are contagious. Caregivers with gastrointestinal infections ? as I had ? can easily infect their patients.
A 2005 outbreak of the norovirus stomach bug in a nursing home highlighted the role of medical personnel in spreading communicable disease. The most disturbing aspect of the case was that medical staff members continued to come to work while ill, well into the outbreak, despite strenuous and public exhortations to stay home. This may have prolonged the outbreak and led to more patients’ falling ill.
A survey of British doctors back in the ’90s found that 87 percent of G.P.’s said they would not call in sick for a severe cold (compared to 32 percent of office workers who were asked the same question). In Norway, a 2001 survey revealed that 80 percent of doctors had reported to work while sick with illnesses for which they would have advised their own patients to stay home. Two-thirds of these illnesses were considered contagious.
What explains this toxic brew of denial, ignorance and bravado? Part of it is a professional but often exaggerated sense of responsibility to colleagues and patients. Even if you are sick enough to have an IV running in your arm, you keep doing your job.
But another part is how we see ourselves. Illness is what we do, not who we are. We define ourselves by vanquishing illness, not succumbing to it.
As much as we empathize with our patients, part of protecting our inner core may require drawing an unconscious demarcation between “us” and “them.” I can recall, as a resident, the palpable relief of leaving the hospital at the end of a long night, something I generally thought about in physical terms ? getting out of grubby scrubs, the promise of a hot shower and edible food. But it was more than that: There was also the awkward relief of leaving behind the graphic reminder of what could befall my own body. Somewhere, deep down, I needed to convince myself that we doctors were a different species from our patients.
I thought of all this recently, after my daughter woke with a fever, and I had to stay home from the hospital at the last minute. I realized it was my first “sick day” in about 25 years. I was grateful that my colleagues stepped in, but it was a frenetic scramble that inconvenienced everyone, especially my patients.
I wish there were a simple process to make it easier for doctors to call in sick so that it’s not an operational crisis every time. But it isn’t possible to have a pool of substitute doctors the way we have substitute teachers.
What we can do, however, is examine the existential qualms that doctors have about illness. From the beginning of medical school it is important to advance the idea that illness is a part of all of us ? doctors and patients alike; that there is very little that separates us from our patients, other than the circumstance of the moment; and, for goodness’ sake, that we need to call in sick when we are sick.