![]() [Description exercise 6] - 終
[Description exercise 6] - 終
![]() Case 36
Case 36
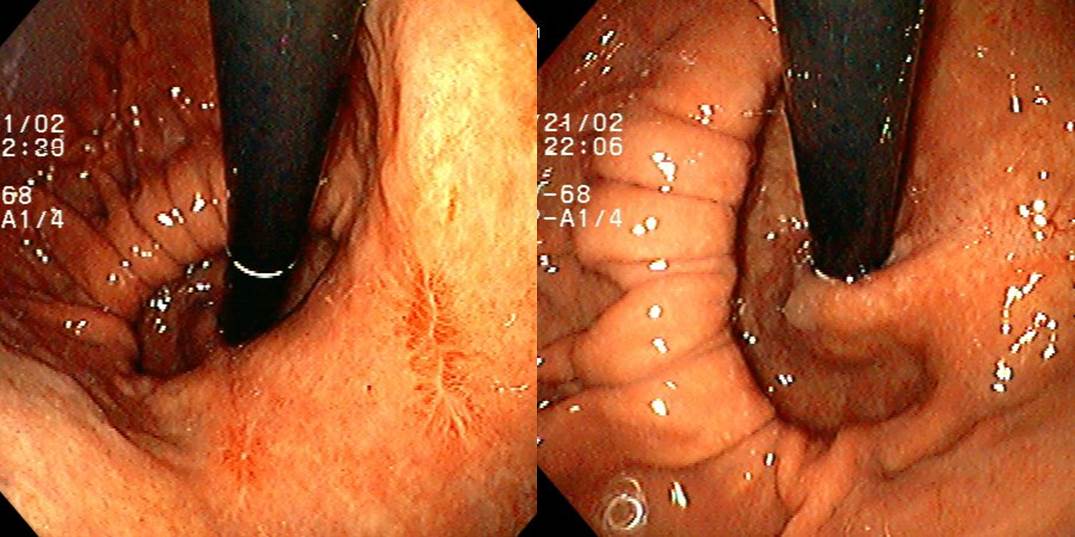
Findings: Hiatal opening is widely opned. Part of the fundus was herniated through the hiatal opening into the thoracic space. SC junction is also elevated from the hiatal opening. At the 4 o'clock aspect of the cardia lesser curvature side, there ia a 1cm sized linear scar with erythema.
Impression: paraesophageal hernia (mixed type), BGU scar (Cameron ulcer scar)
[EndoTODAY comment]
* Reference: EndoTODAY hiatal hernia
![]() Case 37
Case 37
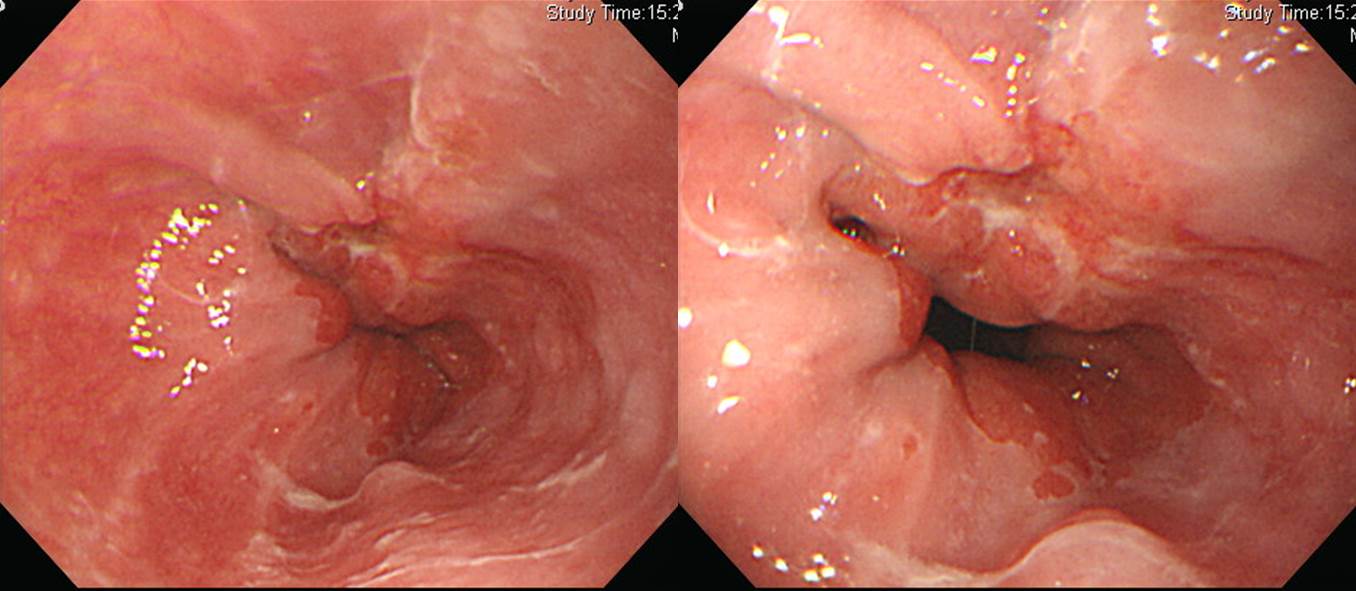
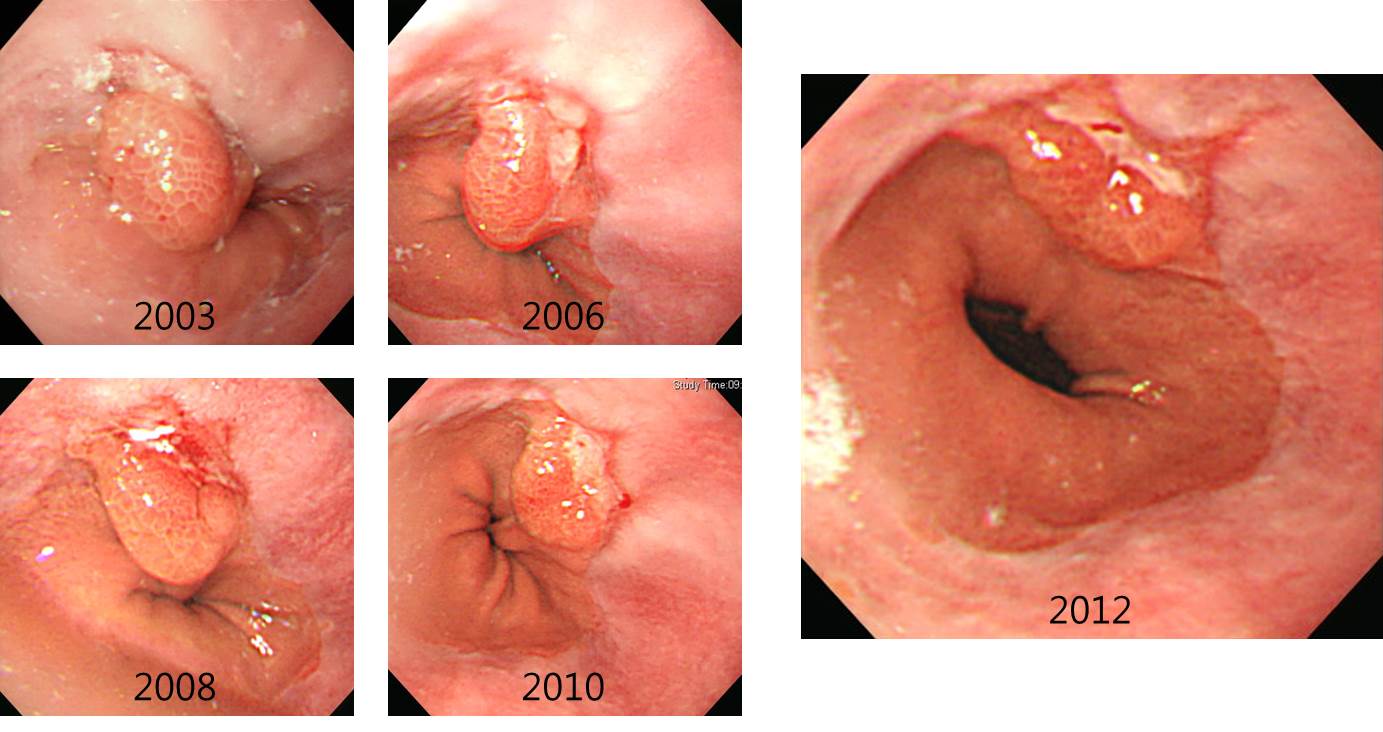
Findings: At the 12-3 o'clock aspect, there is a geographic depression with slight elevation at the distal aspect.
Impression: GE junction cancer
[EndoTODAY comment]
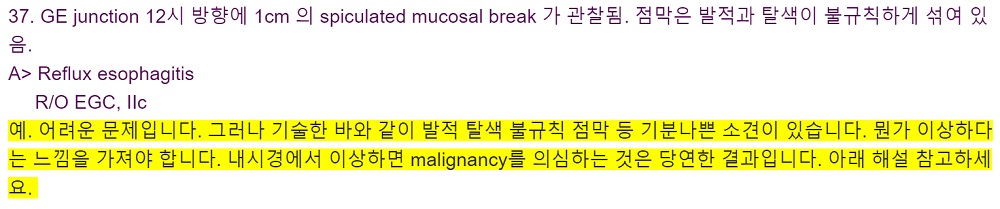
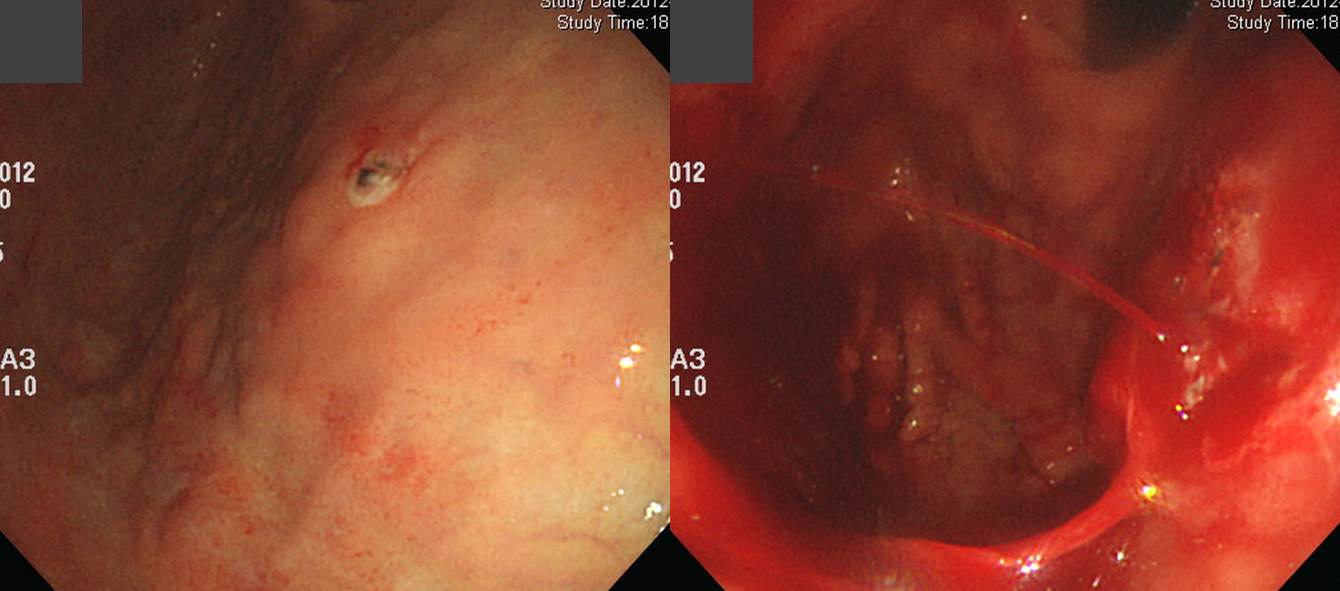
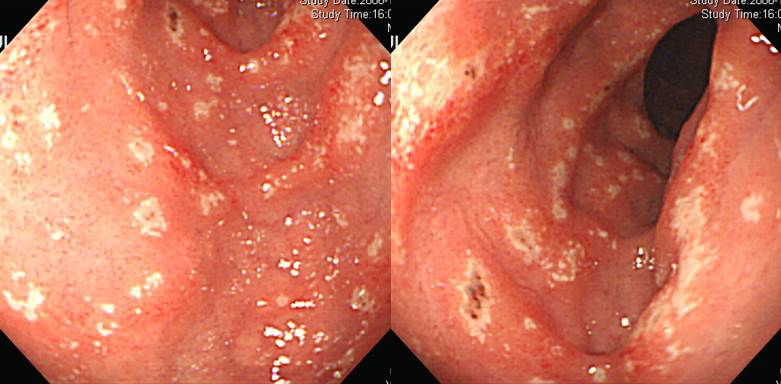
Differential diagnosis between reflux esophagitis and EE junction cancer is sometimes difficult. If there is some kind of irregularity in the depressed area, the possibility of malignancy should be considered and biopsy is necessary. Surgery was done in this case.
Esophagus and upper stomach, Ivor Lewis operation:
Invasive squamous cell carcinoma, moderately differentiated, gastroesophageal junction:
1) tumor size: 2x1.5 cm
2) extension to perimuscular adventitia
3) extension to stomach
4) endolymphatic tumor emboli: present
5) perineural invasion: not identified
6) negative resection margins (proximal, 7.5 cm; distal, 5.5 cm)
7) metastasis to one out of 33 regional lymph nodesIn comparison, following case was reflux esophagitis with a sentinel polyp.
* Reference: EndoTODAY GE junction cancer
![]() Case 38 (history of massive hematemesis)
Case 38 (history of massive hematemesis)
Findings: There is a small ulcer with an exposed vessel in the middle. In the middle of the examination, sudden massive blood pumping developed.
Impression: Pumping bleeding from Dieulafoy lesion (or ulcer), Forrest classification Ia
[EndoTODAY comment]
Treatment of the Dieulafoy ulcer bleeding can be done with band ligation, clipping, and electrocauterization.
The patient was on clopidogrel due to heart failure. Dieulafoy ulcer bleeding was controlled by electrocauterization after injection.
![]() Case 39 - History of recurrent upper GI bleeding for a couple of weeks
Case 39 - History of recurrent upper GI bleeding for a couple of weeks
Findings: On the duodenal bulb and the second portion, there were multiple 2-5 mm sized multiple erosions. Each erosions have irregular margin, but descrete and covered with whitish exudate and hematin.
Impression: Erosive duodenitis (Zollinger- Ellison syndrome, most likely)
[EndoTODAY comment]
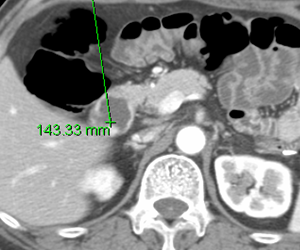
This patient had a mass in the pancreas body with hepatic metastasis. Gastrin was more than 1000 pg/ml.
Followings are another case of Zollinger Ellison syndrome.

* References: EndoTODAY H-S purpura
![]() Case 40
Case 40
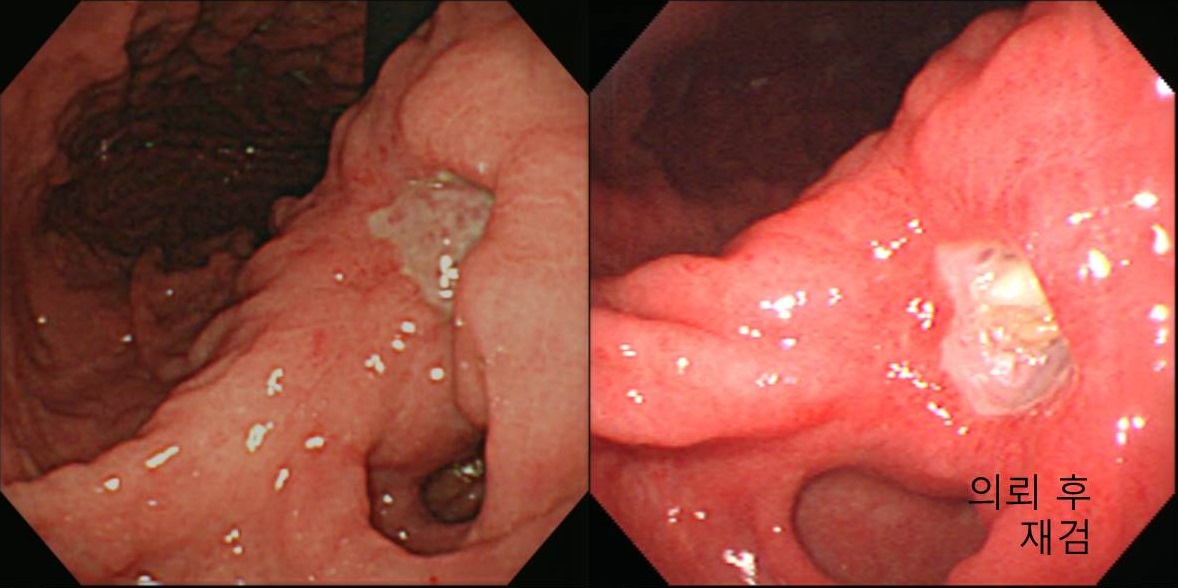
Impression: benign gastric ulcer, A2 (r/o recurrent ulcer)
[EndoTODAY comment]
Second ulcer can develop on the ulcer scar. In that case, the stage of the ulcer crator and the stage of the surrounding can be different.
![]() Case 41
Case 41
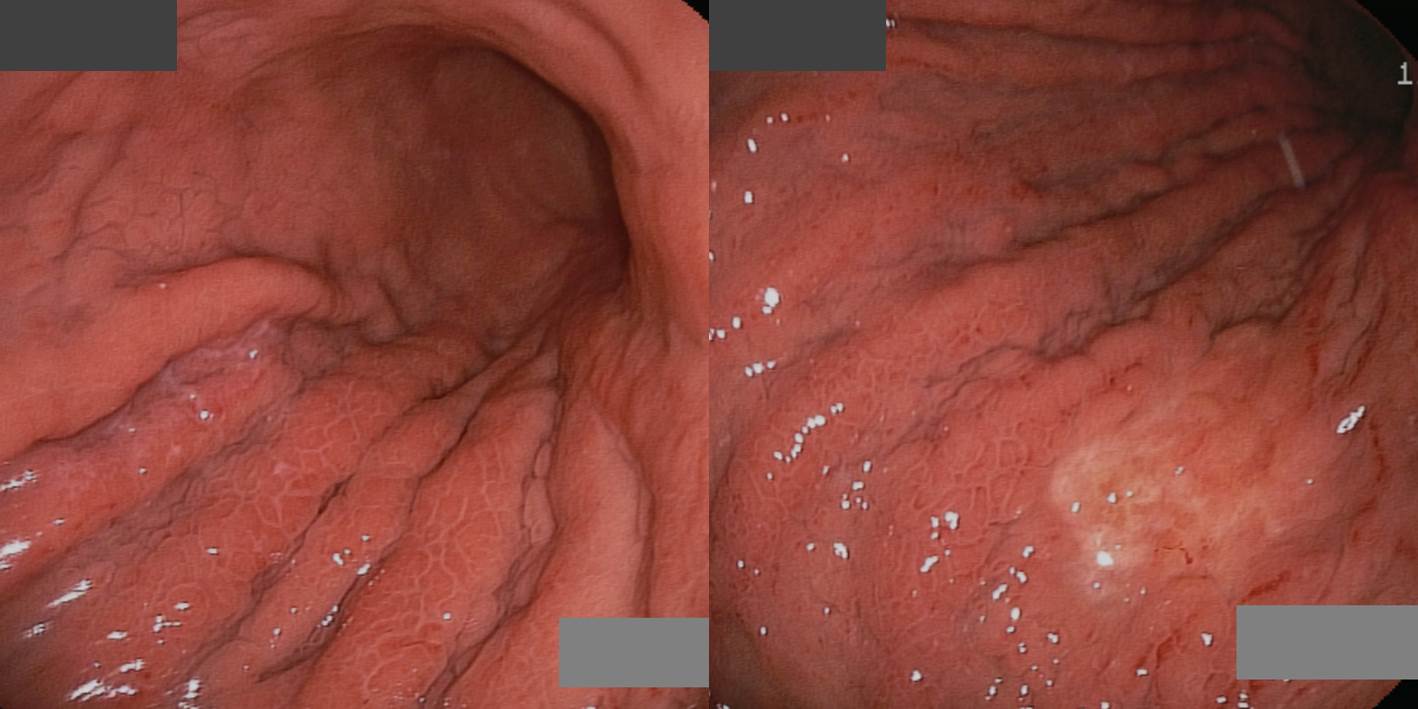
Findings: Diffuse gastric folds thickening from the fundus to the lower body. The surface of the thickened folds shows mozaic pattern. There is a small ill-defined depressed lesion (3-4 cm) on the postero-GC side of the high body.
Impression: AGC, Borrmann type IV
[EndoTODAY comment]
I strongly recommend the following video lecture.

subnote 2023-8-17.
![]() 증례 42
증례 42
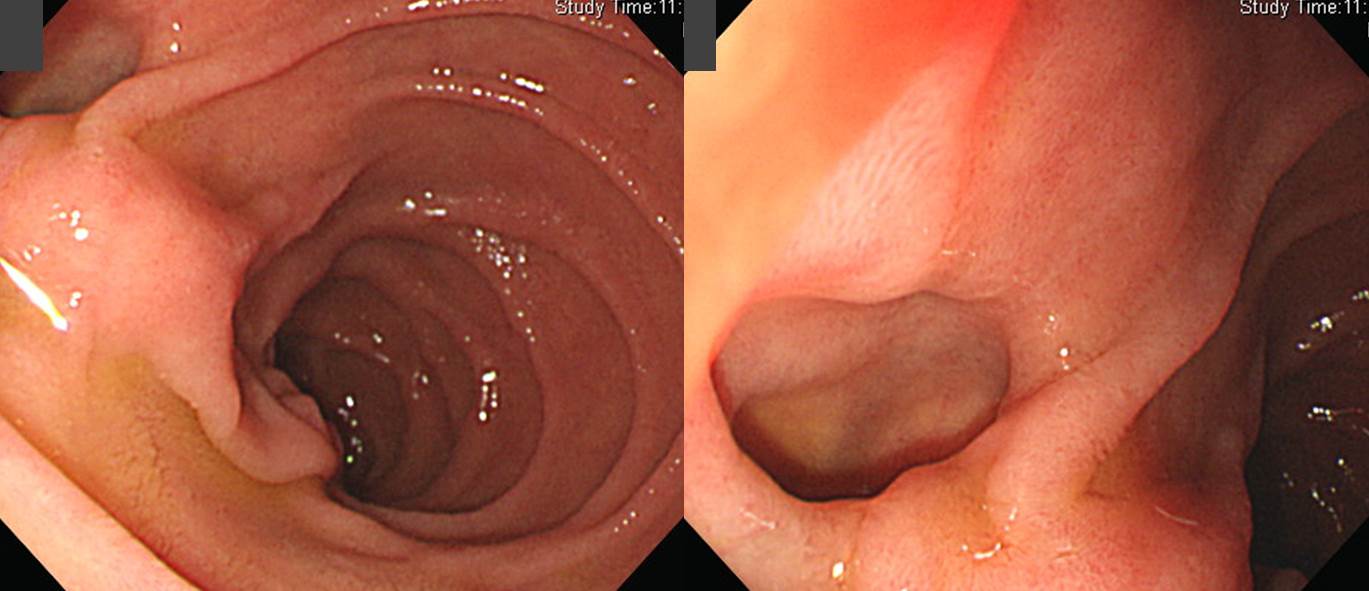
Findings: There is a small outpouching opeining on the inner side of the second part of the duodenum.
Diagnosis: Duodenal diverticulum
[EndoTODAY comments]

2020-4-25. 순천만내시경세미나 동영상 강의 (in Korean)
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.