 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [식도열공탈장. Hiatal hernia. 허니아. 헤르니아] - 終
[식도열공탈장. Hiatal hernia. 허니아. 헤르니아] - 終

2017-5-19 one point lesson
Cameron ulcer와 hiatal hernia. PDF 3.7M - Case Reviews in Gastroenterology
1. Classification 분류
3. Reflux esophagitis with/without hiatal hernia
4. Hiatal hernia. It's not LA-C
5. Hiatal hernia with CLE. It's not LA-D
6. Mallory-Weiss tear: location of the MW tear and relationship with hiatal hernia
![]() 1. 분류
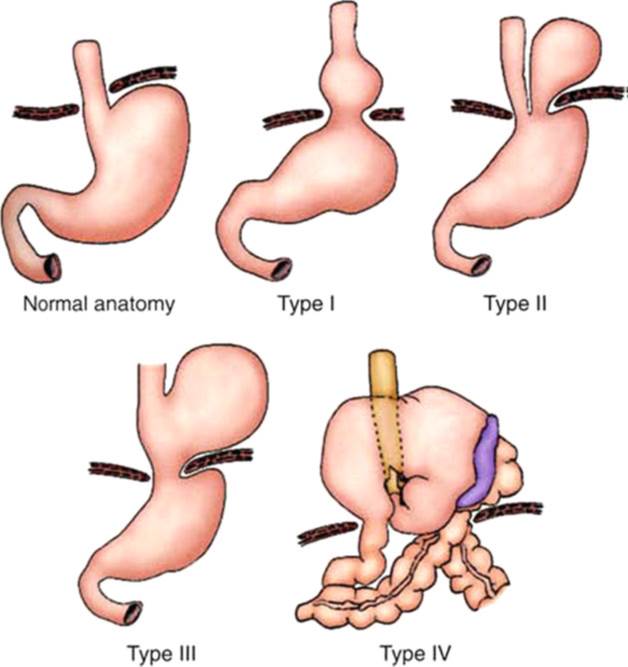
1. 분류
1) Type 1 (sliding hiatal hernia)
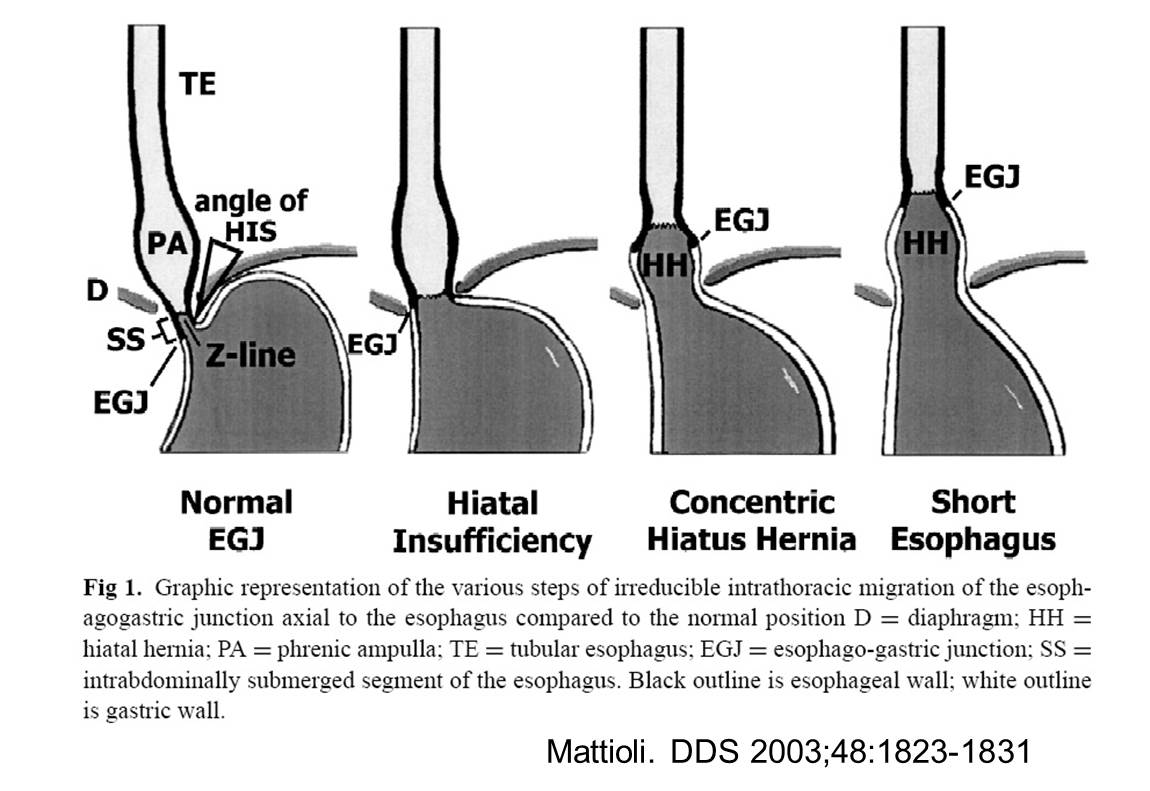
식도열공 주위에서 식도를 횡격막에 부착시켜 주는 횡격막식도 인대(phrenoesophageal ligament)가 헐거워져서 하부식도와 위식도접합부, 위의 상부 일부가 흉강 내로 미끄러져 들어가는 형태의 탈장으로, 활주열공탈장(sliding hiatal hernia)이라고 부릅니다. 전체 식도열공탈장의 95%를 차지합니다. 대부분 탈장 자체로는 증상이 없고, 주로 gastric juice의 역류에 의해 이차적으로 증상이 일어납니다. 식도열공탈장은 역류성 식도염을 일으키는 주요 원인의 하나입니다. 1형 식도열공탈장 없이도 TLESR (transient LES relaxation)등에 의하여 위식도역류질환이 발생하기도 하지만 LA-C나 LA-D와 같은 심한 역류성 식도염의 경우는 대부분 식도열공탈장이 동반되어 있습니다. 1형 식도열공탈장은 대부분 후천성이며, 보통 40대 이후에 발생하게 되고, 비만, 무거운 것을 드는 운동, 임신, 위식도역류나 식도점막의 산화에 의해 유발되는 식도의 종주근육의 긴장성 수축이 악화 인자로 생각됩니다.
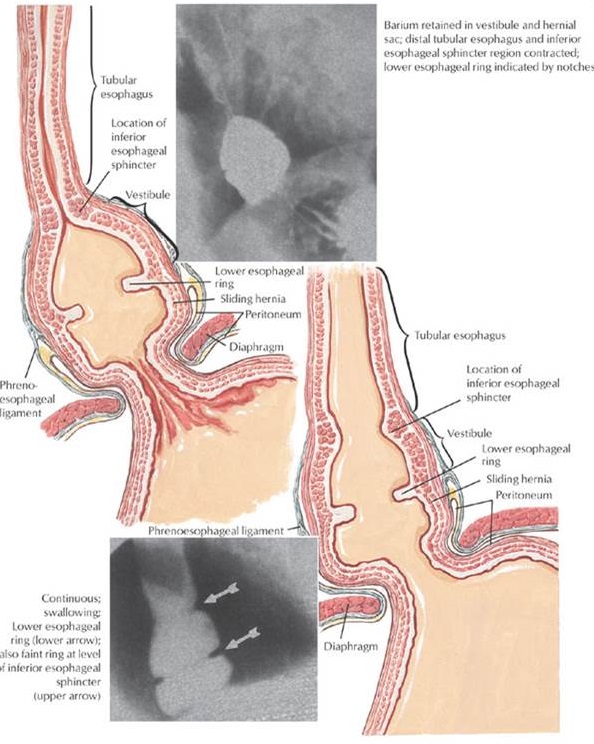
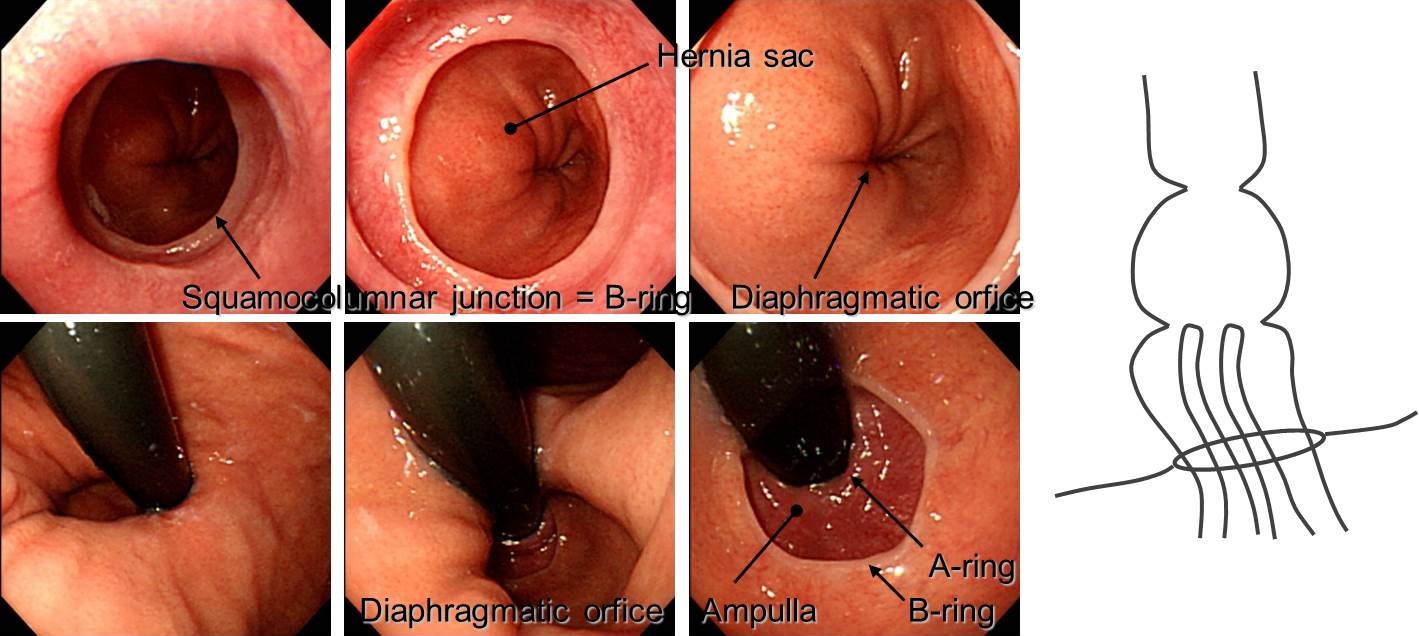
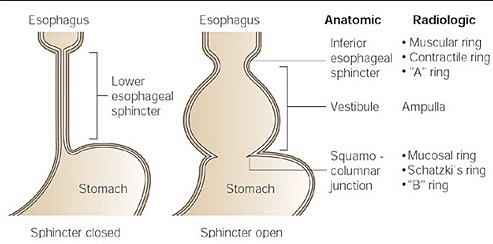
Sliding hiatal hernia가 있으면 LES 하단의 squamous columnar junction 부위가 web 비슷하게 inward indentation을 보이는데 이를 mucosal ring 혹은 B ring이라고 부르며, 이 부위가 fixed되어 좁아지면 Shatzki ring이라고 합니다. LES 상단이 약간 뭉퉁하게 수축되어 보이는데 이를 muscular ring 혹은 A ring이라고 부릅니다. 실제로 이 부위가 anatomical하게 좁아지지는 않습니다. 내시경을 할 때 내시경 삽입부를 약간 조이고 있는 듯하게 보일 뿐입니다. Sliding hiatal hernia가 있을 때 musclar ring과 mucosal ring의 사이(그러니까 LES 부위와 일치합니다)가 배흘림기둥처럼 약간 바깥으로 불룩한데 이 부위를 ampulla 혹은 vestibule이라고 부릅니다. Sliding hiatal hernia가 있을 때 mucosal ring (= squamocolumnar junction = EG junction) 아래부터 diaphragmatic orfice 사이도 배흘림기둥처럼 약간 바깥으로 불룩한데 이 부위를 hernia sac이라고 부릅니다.
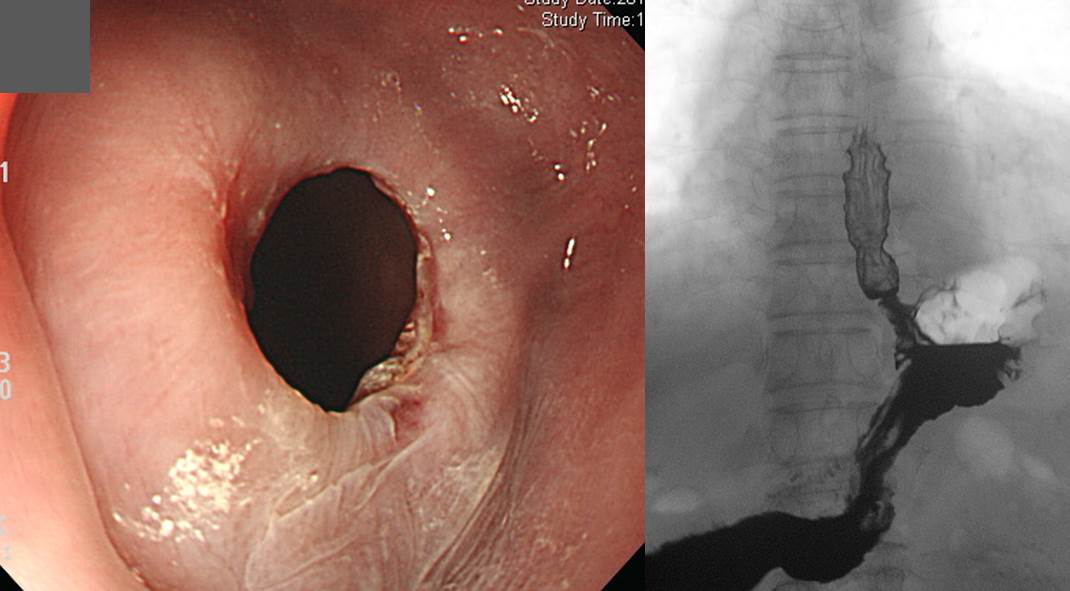
Hiatal hernia with triangle-shape mucosal break
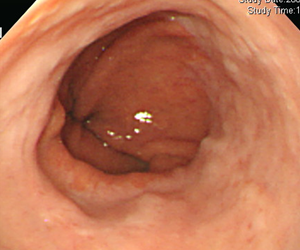
Sliding hiatal hernia가 있으면서 mucosal ring이 좁아지면서 stricture가 발생한 예입니다.
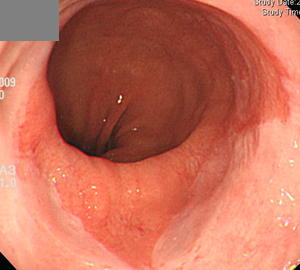
Sliding hiatal hernia이면서 mucosal ring이 조금 indentation된 경한 예
* 참고: Type 1 Hiatal hernia 내시경 소견 연습
그림을 클릭하세요.
2) Type 2 (식도주위탈장, para-esophageal hernia)
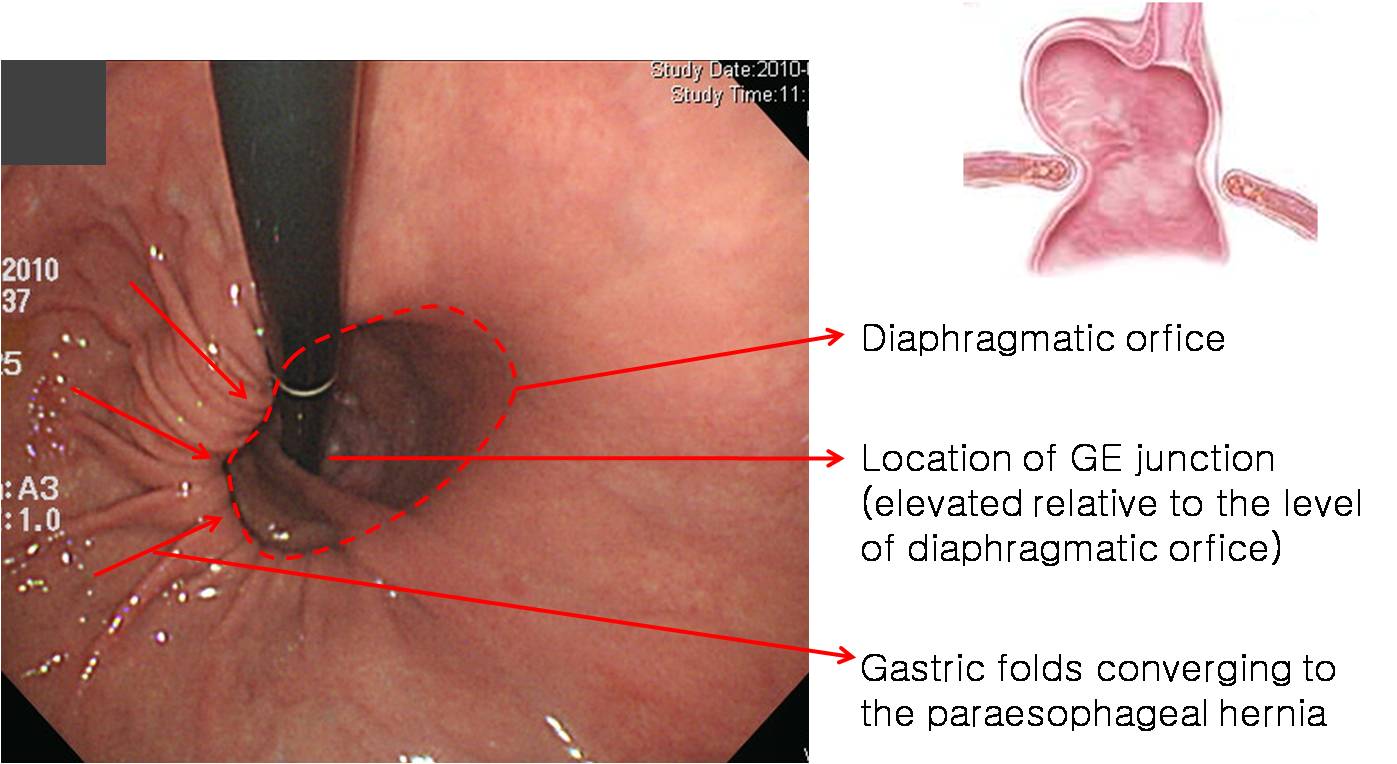
횡격막식도 인대의 손상은 없고, 열공 자체가 늘어나서 그 틈으로 위의 일부(특히 위분문부)가 흉강으로 빠져 들어가는 형식의 탈장을 말합니다. Gastroesophageal junction이 diaphragmatic orfice와 같은 level, 즉 정상 높이에 위치하고 있습니다. 병리에서는 rolling type이라고도 부릅니다. 매우 드문 형태입니다. 책에서는 hiatal hernia의 2% 정도라고 합니다만 사실 저는 거의 본 적이 없습니다. 우리가 흔히 paraesophageal hernia라고 말하는 것은 대부분 type 3입니다. 아래는 인터넷 사진입니다.
한 애독자께서 보내주신 type 2 para-esophageal hernia 증례 사진입니다.
SCJ이 hiatal opening 바로 위에 위치하고 있습니다. Sliding hernia 요소가 거의 없습니다.
EG junction에서 1-2cm 떨어진 fundus의 대만 쪽에 작은 구멍이 있고 이를 향하여 위 주름이 빨려들어가고 있는 모습니다.
근접 사진
Diaphragm 상방 심장 뒤쪽으로 air shadow가 보입니다.
3) Type 3 (mixed paraesophageal hiatal hernia)
Type 3은 type 1 부분과 type 2 부분이 섞인 것입니다. 횡격막식도인대의 손상으로 위식도 접합부가 밀려 올라가면서 열공 자체가 커지고 이를 통하여 위 분문부가 흉강 안으로 빠져 들어간 형태입니다. 정확한 이름은 mixed type hiatal hernia인데, 그냥 paraesophageal hernia라고 부르는 경우가 많습니다. 진정한 의미의 paraesophageal hernia는 거의 없고 대부분 mixed type이기 때문입니다. 저는 mixed paraesophageal hernia라고 부르고 있습니다.
Olympus 내시경
Pentax 내시경
Fujifilm 내시경
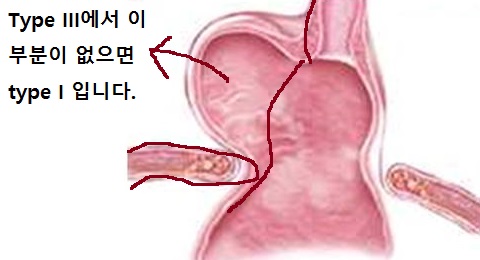
Type 2 부분, 즉 횡격막 위로 올라간 fundus 부분이 없다고 생각하면 type 1입니다. 아래 그림 참고하세요.
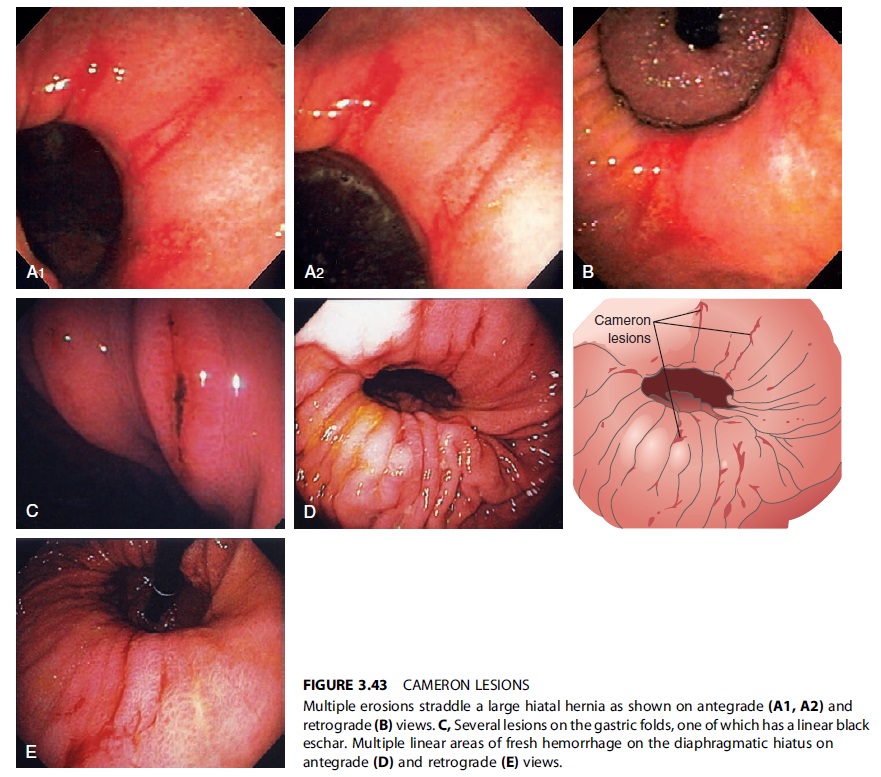
Mixed paraesophageal hernia에서는 hiatal opening level에서 ulcer가 발생할 수 있습니다. Cameron ulcer라고 부릅니다. 아마도 hiatal opening을 경계가 胃가 위아래로 움직이면서 기계적인 자극을 받는 것이 한 요인일 것으로 생각합니다.

위 환자에게 PPI 장기 투약한 후 Cameron ulcer가 호전된 모습
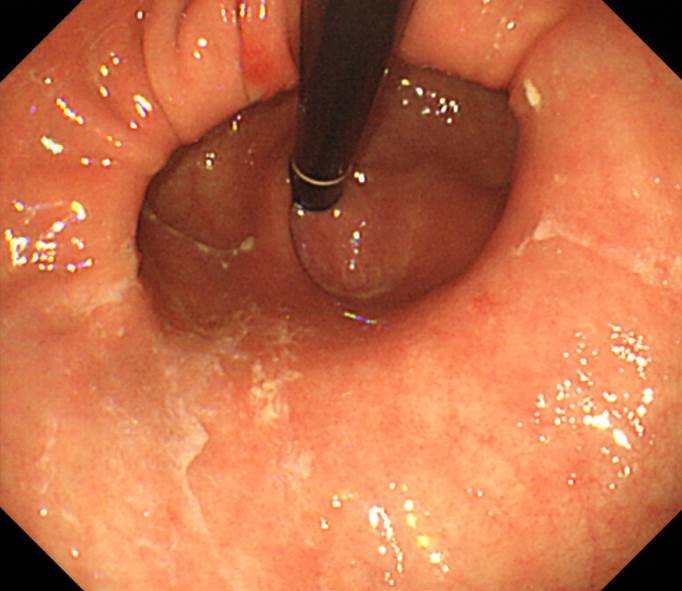
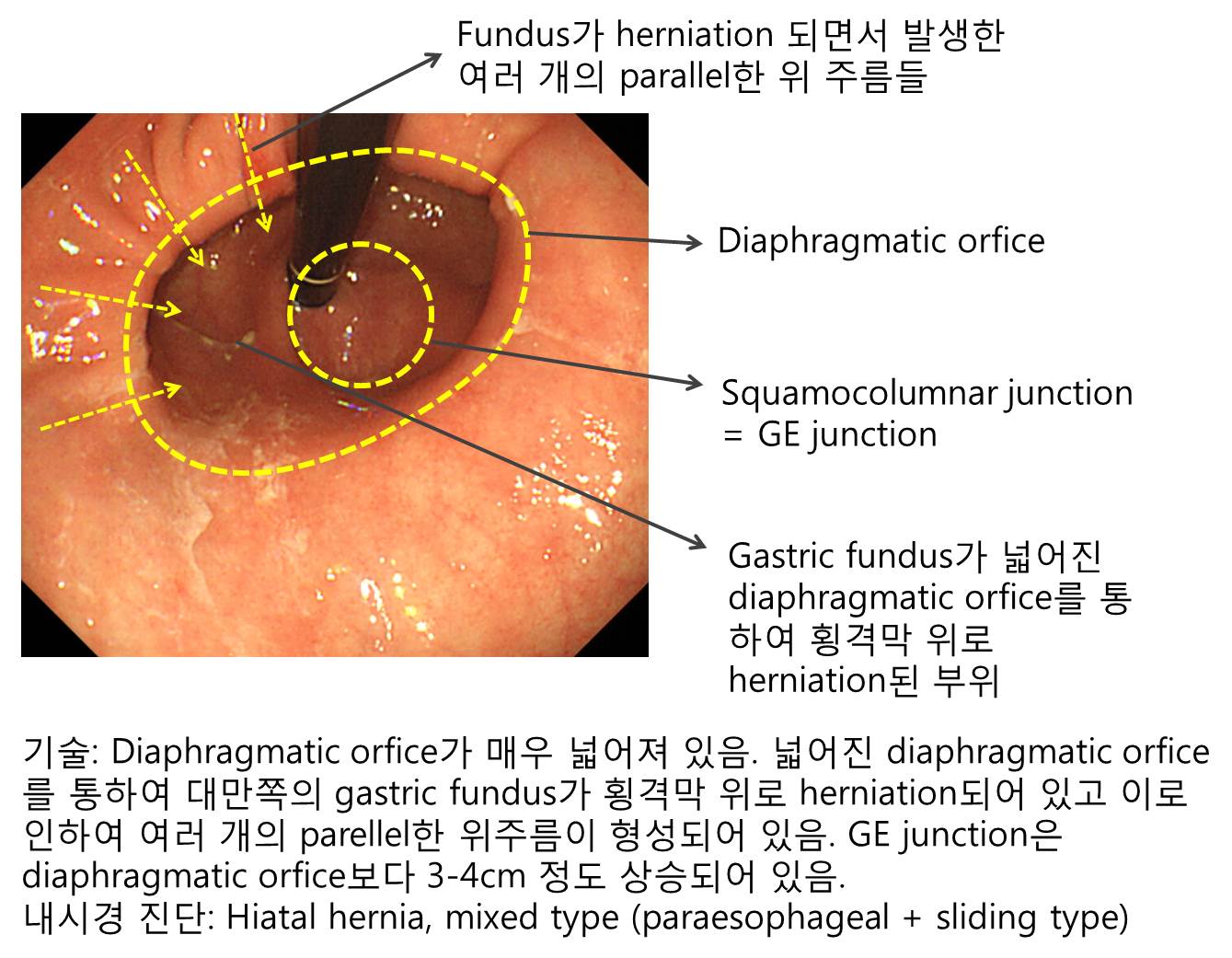
전형적인 mixed paraesophageal hernia 증례들과 함께, Cameron ulcer가 있었던 경우, Marfan 환자에서 발견된 경우, herniation된 부위에 위암이 있었던 경우 등을 소개합니다. 자세히 기술하는 연습을 해 보세요.
한 전공의 선생님께서 기술한 내용을 소개합니다. 멋진 description이라고 생각했습니다.
"식도 중하부에 전체적으로 1mm size 미만의 multiple scattered whitish spot 이 관찰됨. GE junction 이 diaphragmatic orifice 위쪽으로 올라와 있음. Retroflexion view 에서 4cm 크기의 diaphragmatic opening 이 관찰되며 옆쪽에는 gastric fold 가 high body GC에서 hernia sac 안쪽으로 이어지고 있음. Imp ) Esophageal candidiasis Gr 1, mixed type hiatal hernia"
Paraesophageal hernia와 sliding hiatal hernia가 함께 있는 mixed type hiatal hernia입니다. Diaphragmatic opening 아래 위체상부 소만에 Cameron ulcer가 있습니다. 출혈의 원인입니다.
Marfan 증후군 환자 paraesophageal hiatal hernia (mixsed type)
위 Marfan 증후군 환자의 6 년 전 내시경 사진
Mixed type hiatal hernia + Cameron cancer (상세 설명: EndoTODAY 위암 625)
* 전형적인 증례의 serial한 내시경 소견: Mixed paraesophageal hiatal hernia
4) Type 4
어떤 책을 보면 hiatal hernia type을 1, 2, 3, 4로 나누기도 합니다. 위가 몽땅 횡경막 위로 올라간 경우를 type 4로 보면 됩니다. 보통 type 3가 매우 심해지면 type 4처럼 됩니다.
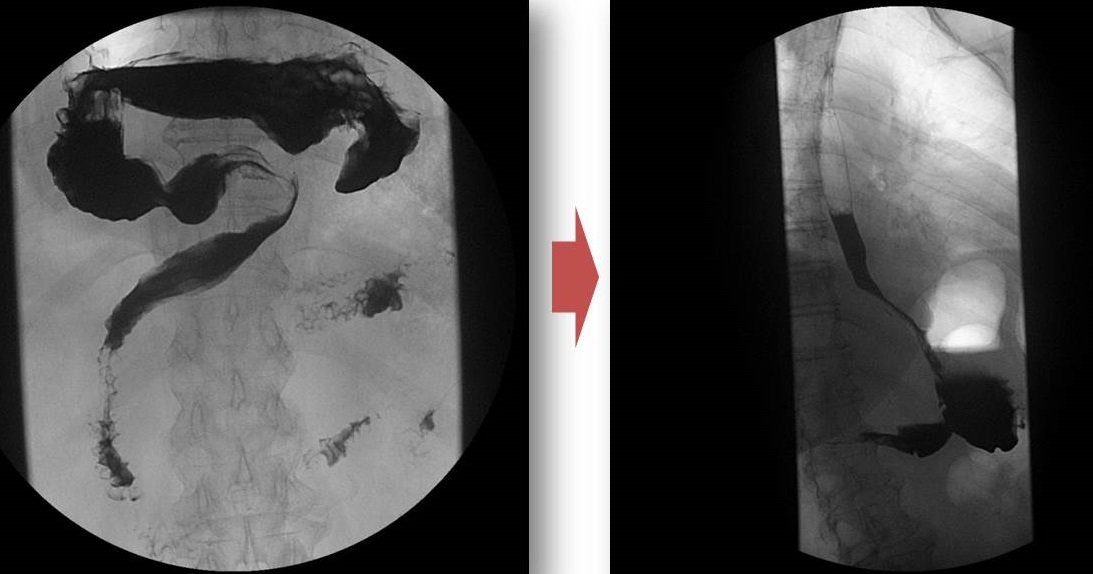
Recurrent bleeding으로 내원하신 여성입니다. Hiatal hernia가 심하고 Cameron ulcer로 인한 출혈이 발생한 경우였습니다. 수술적 치료를 권했으나 환자가 약물치료를 원하여 상당 기간 PPI를 사용하였습니다. 그럼에도 불구하고 출혈이 반복되었습니다. 처음에는 심한 sliding hernia 상태였으나 시간이 지나고 구토, 복통, 출혈로 환자가 수술을 결심하게 될 무렵에는 위 전부가 횡격막 위로 올라온 type 4 hiatal hernia가 된 상태였습니다.
심한 sliding hiatal hernia with Cameron ulcer bleeding 상태
수술하기 직전. 위 전체가 횡경막 상방으로 이동된 type 4 hiatal hernia 상태
Laparoscopic hernia reduction and partial fundoplication이라는 수술을 하였고 깔끔히 좋아졌습니다.
또 다른 환자입니다. 보행시 호흡곤란을 일으킬 정도의 hiatal hernia였습니다. 15년 사이에 천천히 진행된 모양입니다. Surgical correction이 필요한 type IV입니다.
아래 CRG에 기고한 증례를 살펴보시기 바랍니다.
![]() 2. Sliding hiatal hernia
2. Sliding hiatal hernia
Sliding hiatal hernia의 발생은 주로 phrenoesophageal ligament의 늘어짐과 관련되어 있습니다 (Pathogenesis 참조).
Phrenoesophageal ligament의 늘어짐과 함께 하부 식도는 curved 됩니다.
Hiatal hernia가 오래되어 fixed 되기 전까지 phrenoesophageal ligament는 늘어나 있으나 식도가 짧아지지는 않아서 어느 정도의 reducibility를 보입니다. 공기를 넣기 전과 넣은 후가 다르고, 호흡에 따라 다르고, 내시경 넣을 때와 나올 때가 다른 이유입니다.
Sliding hiatal hernia의 내시경 소견을 이해하기 위하여 알아야 할 해부학적 용어는 A-ring (muscular ring), B-ring (mucosal ring = Schatzki ring), ampulla, hernia sac 등입니다.
Sliding hiatal hernia는 2 cm 이상으로 정의되고 있으나 그보다 짧은 경우는 short segment hiatal hernia라고 부르기도 합니다. GERD와 관련되어 있기 때문입니다.
Sliding hiatal hernia가 오래되면 B ring (mucosal reing) 부위가 좁아집니다. 협착이 심해지면 확장술이 필요합니다.
Sliding hiatal hernia 증례를 모아보았습니다.
Hiatal hernia 내시경 연습입니다. 그림을 click해 보십시오.
12시 방향에서 아주 작은 sentinel polyp이 보입니다.
역류성 식도염 LA-C로 의뢰된 분입니다. 그러나 hiatal hernia 였습니다. Hiatal hernia가 있으면 squamocolumnar junction이 약간 불규칙해지거나 지저분해 보이는 수가 있습니다. 이를 mucosal break로 오인하면 안 되겠지요.
역류성 식도염 LA-D로 의뢰된 분입니다. 그러나 hiatal hernia 였습니다. Columnar metaplasia가 동반되었습니다. 조직검사에서 Goblet cell metaplasia가 없었으므로 CLE (columnar-lined esophagud)에 해당합니다. 지금까지 제게 LA-C나 LA-D로 의뢰된 상당수의 환자는 hiatal hernia였습니다. 내시경 과잉진단이 그만큼 많다는 뜻입니다.
[Is it hiatal hernia or web?] Esophageal web이라는 내시경진단으로 의뢰된 분입니다. 과연 이 환자에서 esophageal web이 적당한 용어일까요? 분명히 sliding type의 hiatal hernia가 있고 squamocolumnar junction(SCJ)이 거의 360도에 걸쳐 inward foldding이 되어 보입니다. 특히 12시부터 4시 방향까지가 현저합니다. 공기를 뺀 상태에서 관찰하면 12시부터 4시까지는 inward folding되어 보이지만 다른 부위는 정상적인 SCJ으로 관찰됩니다. Sliding hiatal hernia를 가진 환자에서 위에 공기를 많이 넣고 환자의 호흡을 조절하는 방식으로 SCJ이 upward elevation 되게 하면 많은 환자에서 SCJ이 inward folding을 보입니다. Hernia가 심하여 이 부분이 folding된 상태로 고정되고 좁아지면 Schatzki ring이라고 부릅니다. 그러나 이 증례에서는 inward folding이 고정된 부위가 원주의 1/3정도에 지나지 않고 obstruction 소견도 전혀 없습니다. 이런 경우까지 web이라고 부르기는 어렵지 않을까요? 단지 SCJ의 일부가 반복적인 mucosal break와 healing으로 인하여 다소 단축된 것 아닌가 생각됩니다. GERD 증상이 있으면 치료하고 없으면 무시하면 그만이겠습니다.
![]() 3. Reflux esophagitis with/without hiatal hernia
3. Reflux esophagitis with/without hiatal hernia
Hiatal hernia 없는 역류성 식도염 환자도 많습니다. 그렇지만 심한 역류성 식도염 환자들은 대부분 hiatal hernia를 가지고 있습니다.
Hiatal hernia가 없는 역류성 식도염
Hiatal hernia가 있는 역류성 식도염
Hiatal hernia에 대하여 2 cm 기준을 고집하면 상황이 복잡해집니다. 그냥 단순히 눈으로 봐서 hiatal hernia가 있는지 판단하면 상황이 단순해집니다.
![]() 4. Hiatal hernia. It's not LA-C
4. Hiatal hernia. It's not LA-C
역류성 식도염 LA-C로 의뢰된 분입니다. 그러나 hiatal hernia 였습니다.
Hiatal hernia가 있으면 squamocolumnar junction이 약간 불규칙해지거나 지저분해 보이는 수가 있습니다. 이를 mucosal break로 오인하면 안 되겠지요.
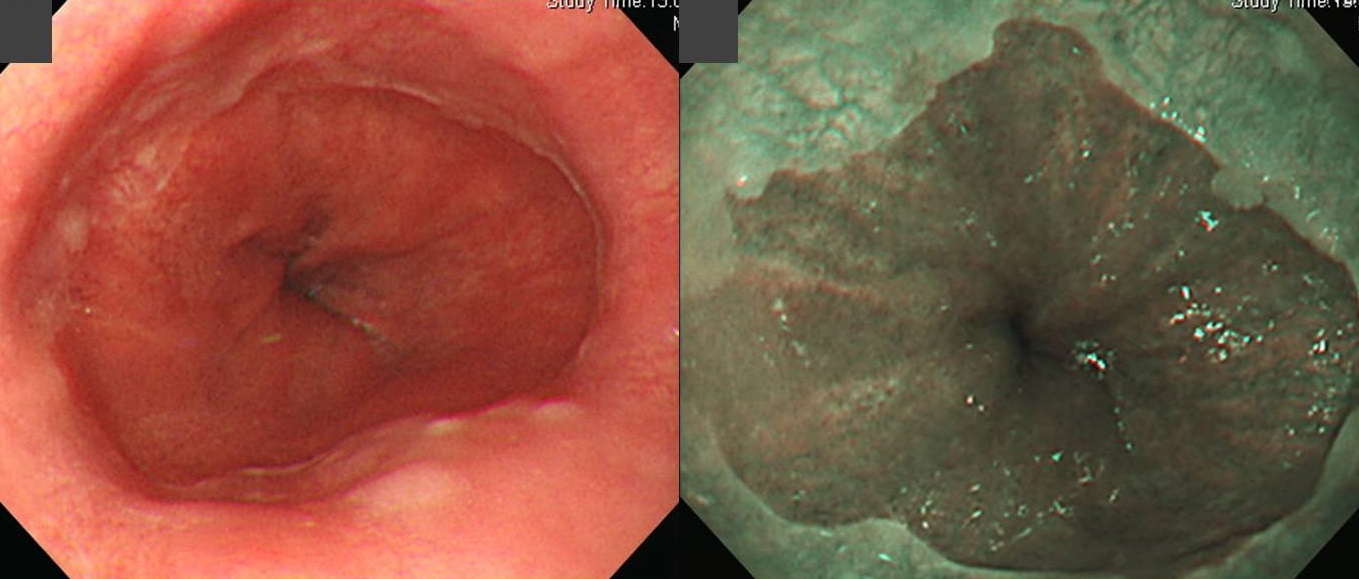
![]() 5. Hiatal hernia with CLE. It's not LA-D
5. Hiatal hernia with CLE. It's not LA-D
역류성 식도염 LA-D로 의뢰된 분입니다. 그러나 hiatal hernia 였습니다. Columnar metaplasia가 동반되었습니다. 조직검사에서 Goblet cell metaplasia가 없었으므로 CLE (columnar-lined esophagud)에 해당합니다.
지금까지 제게 LA-C나 LA-D로 의뢰된 상당수의 환자는 hiatal hernia였습니다. 내시경 과잉진단이 그만큼 많다는 뜻입니다.
![]() 6. Mallory-Weiss tear: location of the MW tear and relationship with hiatal hernia
6. Mallory-Weiss tear: location of the MW tear and relationship with hiatal hernia
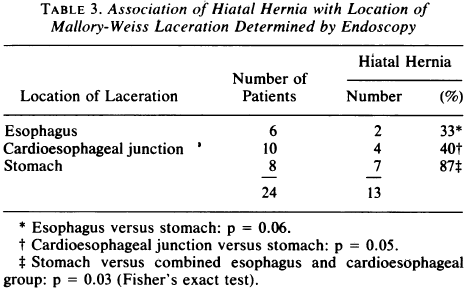
MW tear의 위치와 hiatal hernia는 약간의 관련성이 있다. 이에 대한 최근 자료는 드물기 때문에 1980년 MGH에서 발표한 논문의 table을 capture하였다.
필자의 경험과는 달리 30여년전 MGH에서는 식도와 위에 걸친 경우가 가장 많았고 식도에만 위치한 예도 적지 않았던 모양이다. 흥미로운 것은 stomach에 위치한 MW의 대부분이 hiatal hernia가 있던 환자에서 발생하였다는 것이다.
정확한 자료는 없지만 필자는 이렇게 생각한다. Hiatal hernia가 뚜렷한 환자에서 MW tear는 stomach에 발생하기 쉽다는 점은 동의한다. 그러나 hiatal hernia가 뚜렷하지 않더라도 대부분의 MW tear는 stomach에서 시작한 것이 아닐까?
위에서 시작하여 식도쪽으로 약간 progression한 예가 아닐까?
![]() 7. 강의 - 정의
7. 강의 - 정의
In my opinion, the definition of the hiatal hernia is not defined yet. This is a screenshot from a patient information website of the Mayo Clinic. Yes, it is right. Hiatal hernia is a condition when the upper part of the stomach bulges through the diaphragm into the chest cavity. But, there are two important questions here. How much part of the stomach needs to be bulged? How would you evaluate the length of herniation? With what method?
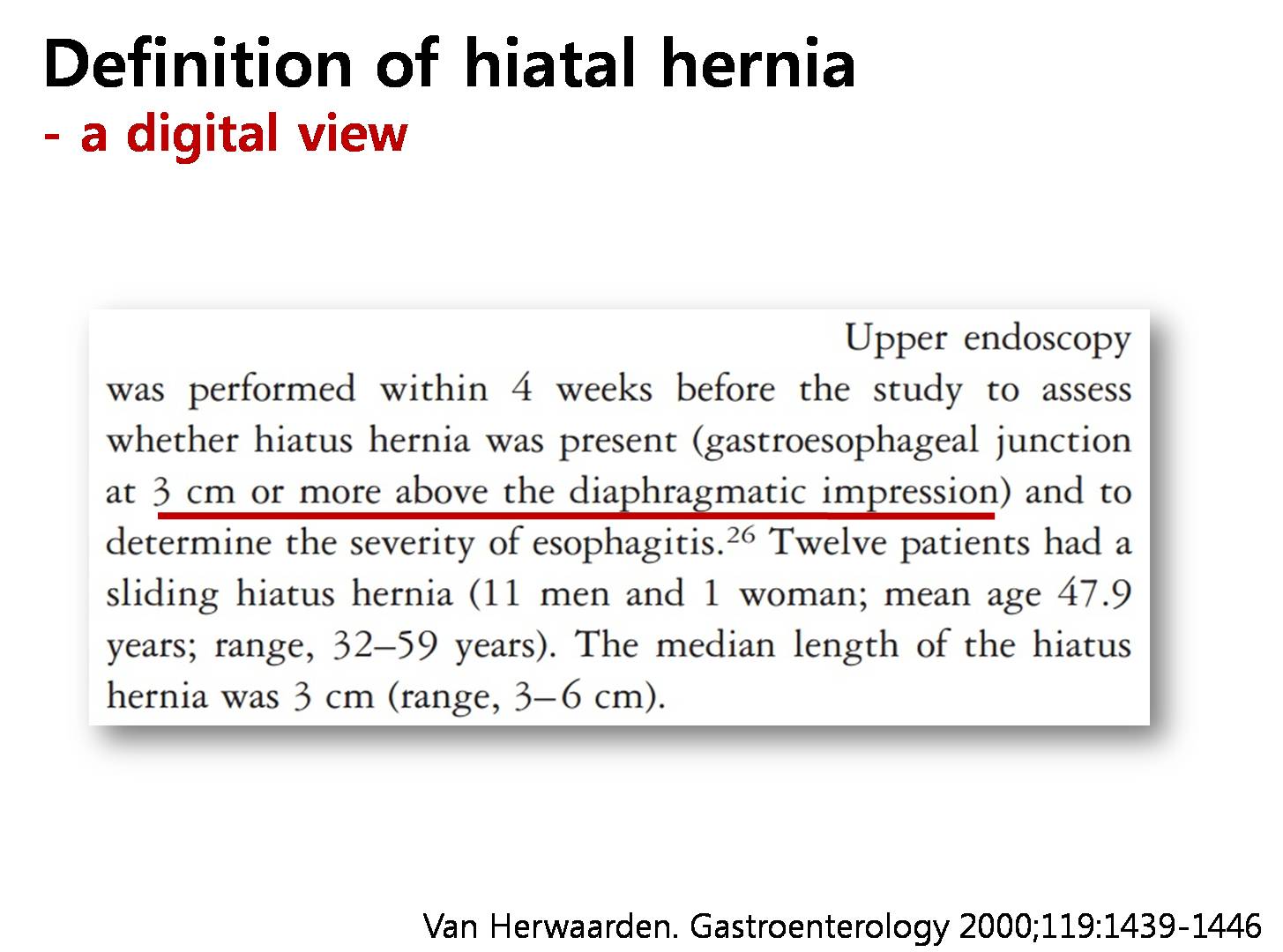
In this study, the definition of hiatal hernia was bulging of 3 cm or more above the diaphragmatic impression.
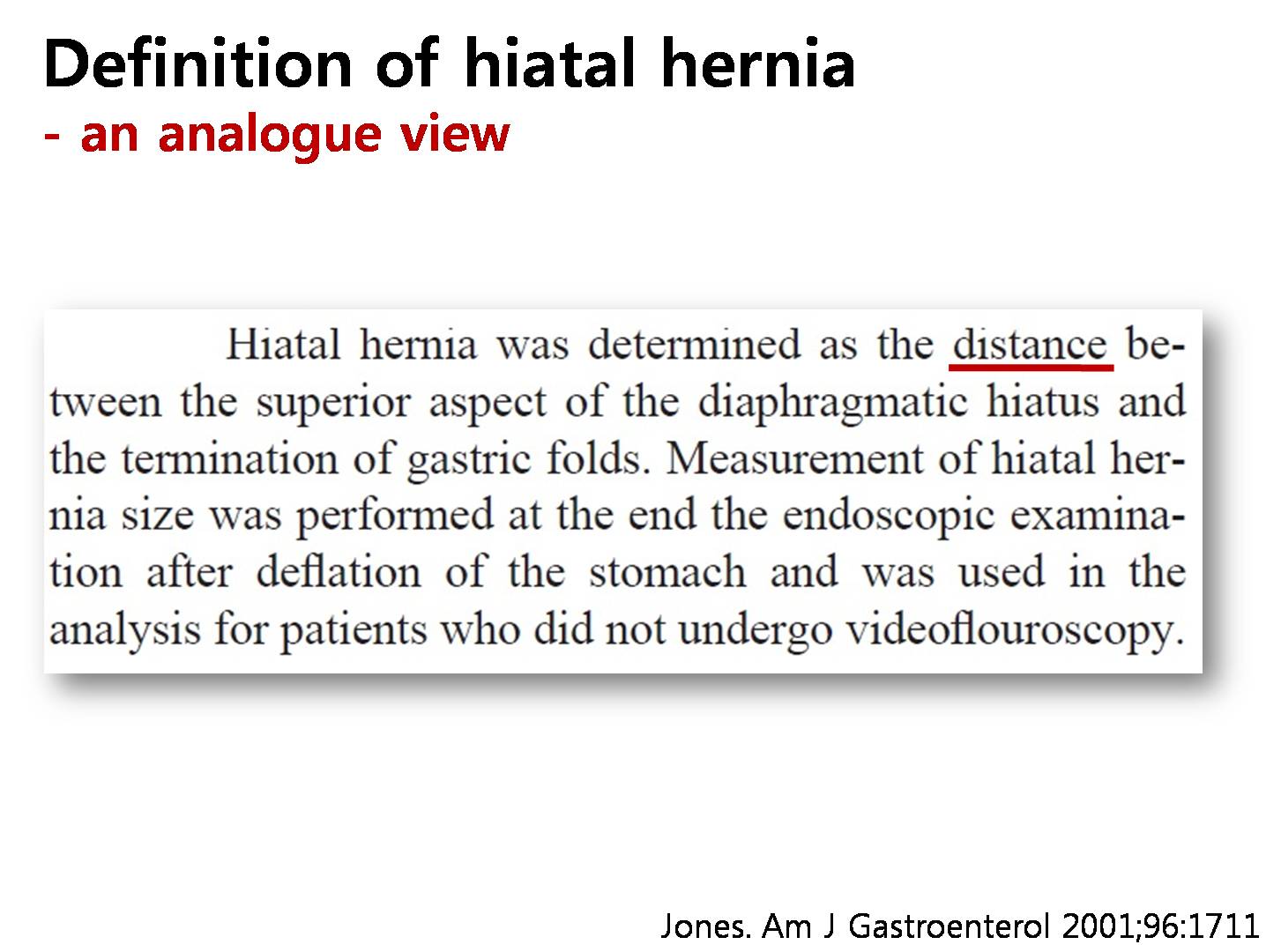
In another study, there was no definite criteria in terms of the length. Just the distance was measured like 1 cm, 2 cm, etc.
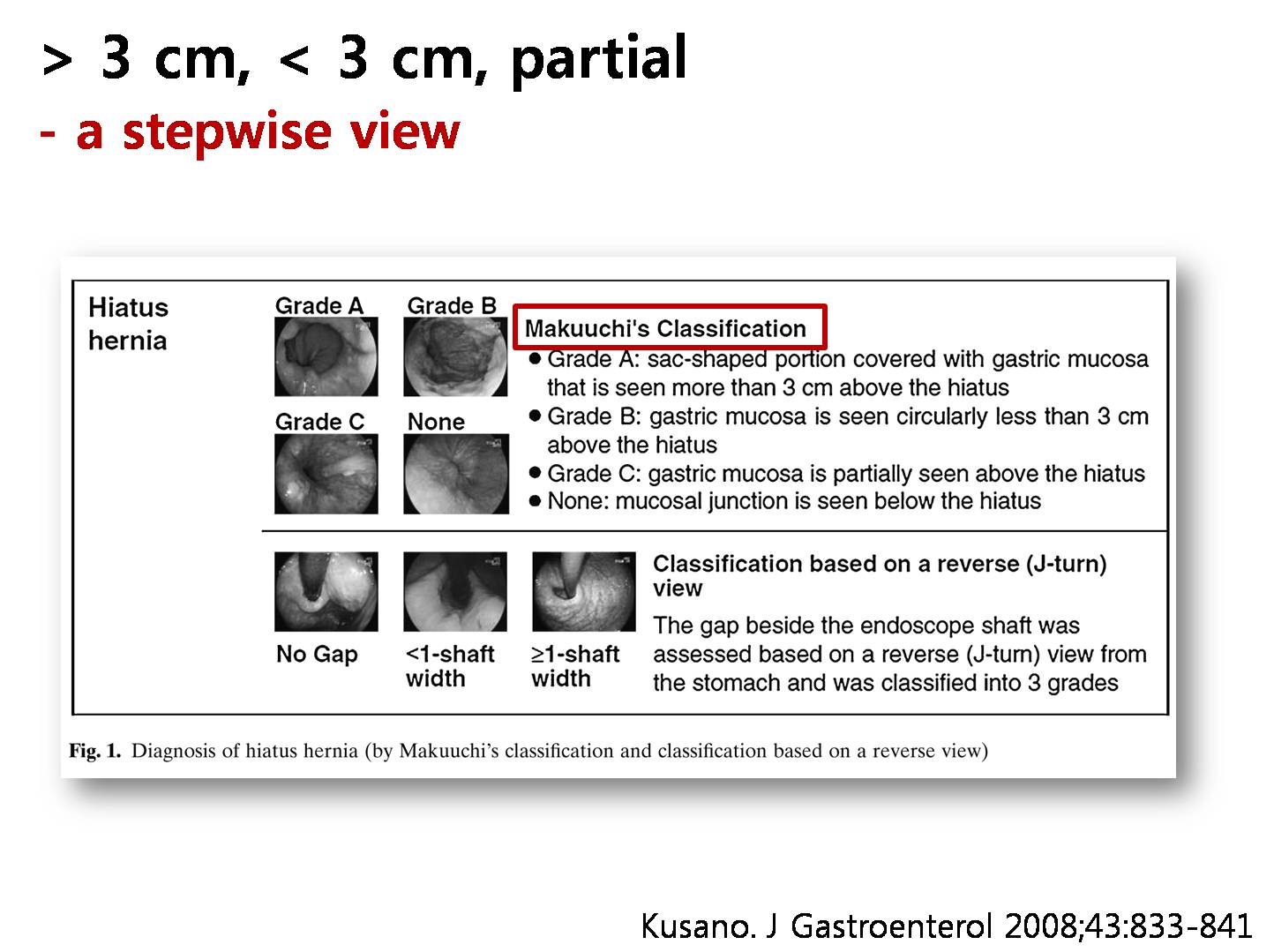
This is a unique classification system in Japan called Makuuchi’s classification. In this system, hiatal hernia is graded into A, B, and C. Group C is usually not considered as hiatal hernia by most physicians outside Japan.
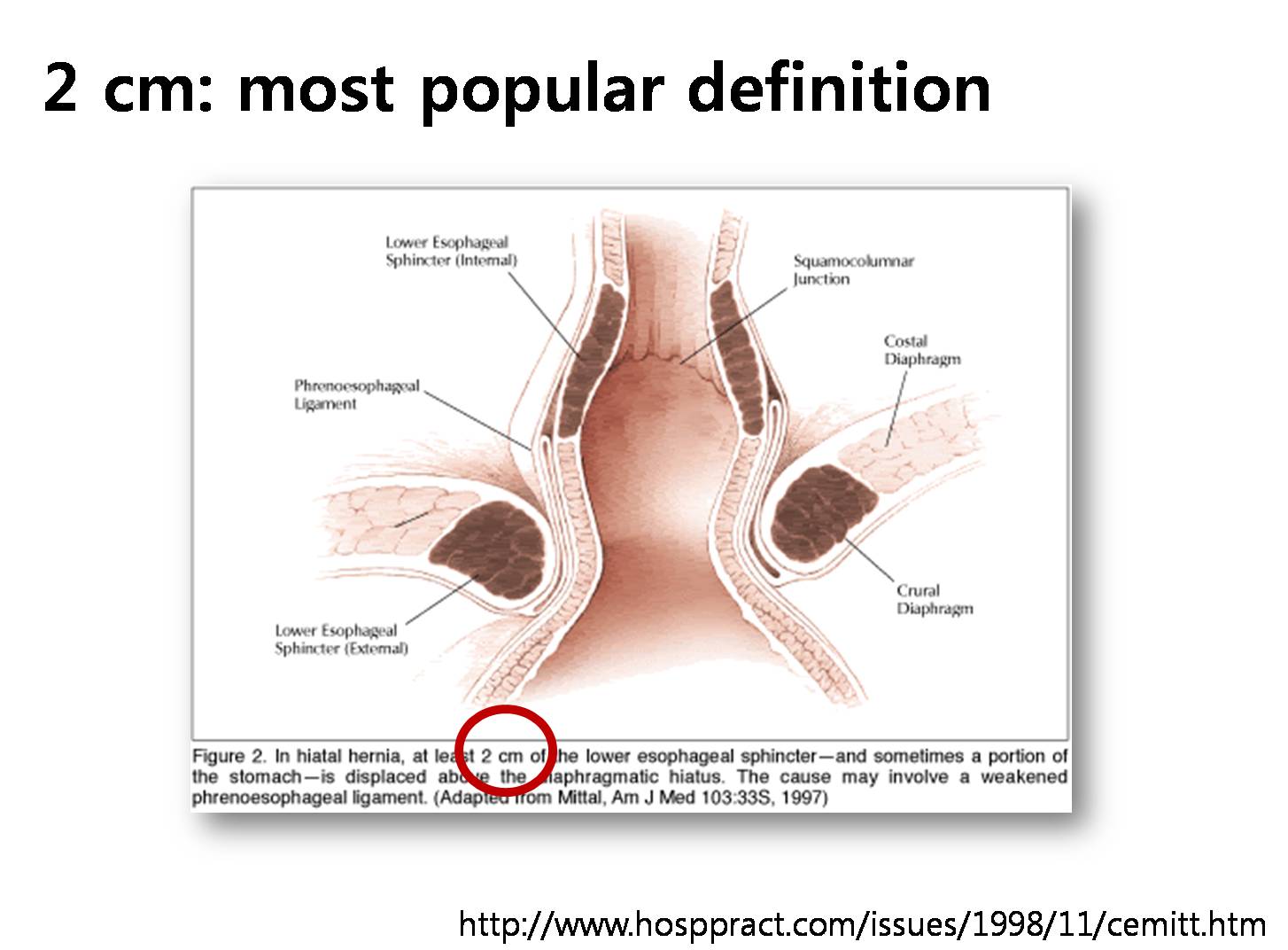
In Korea, upward bulging of at least 2 cm is considered necessary for the diagnosis of hiatal hernia.
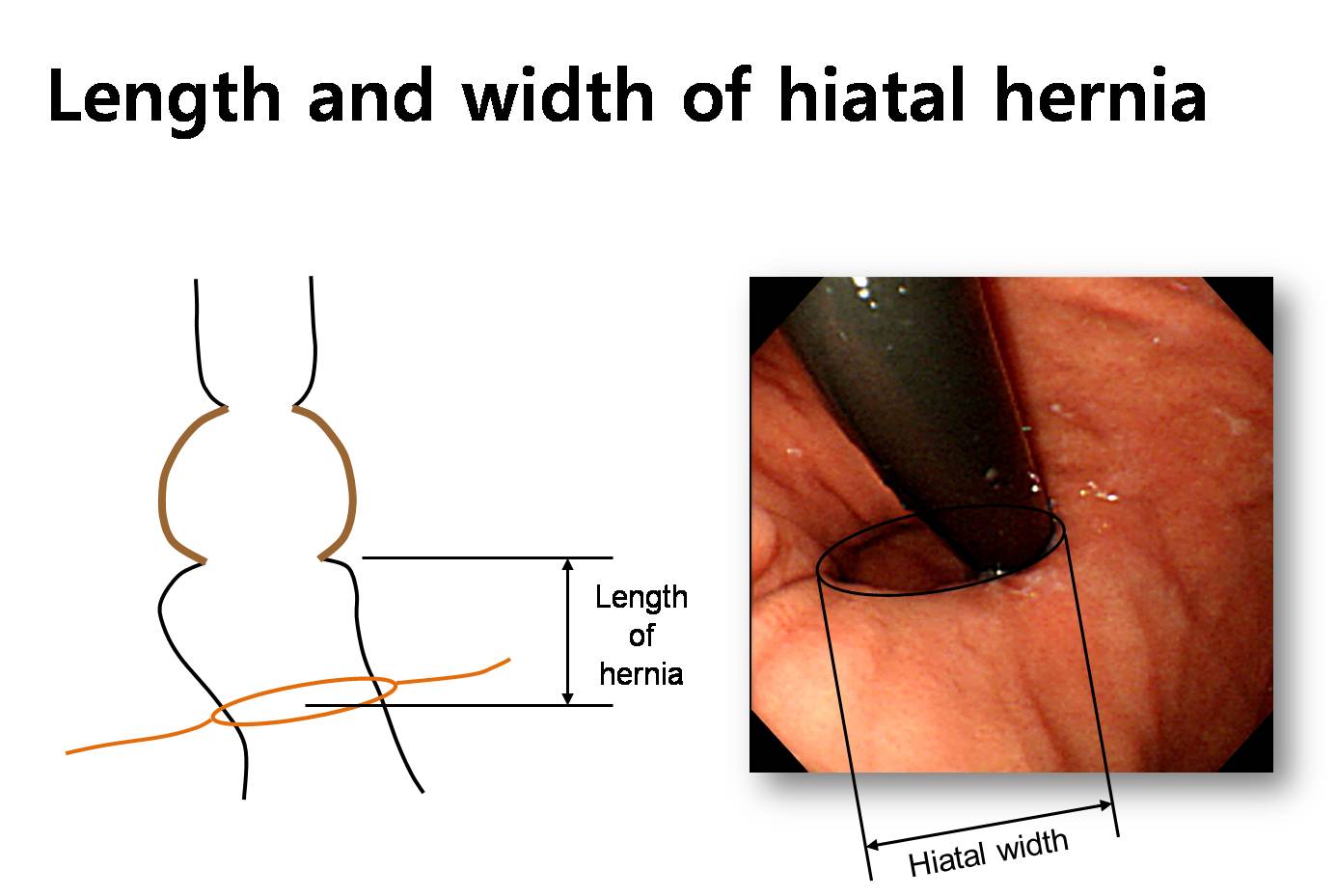
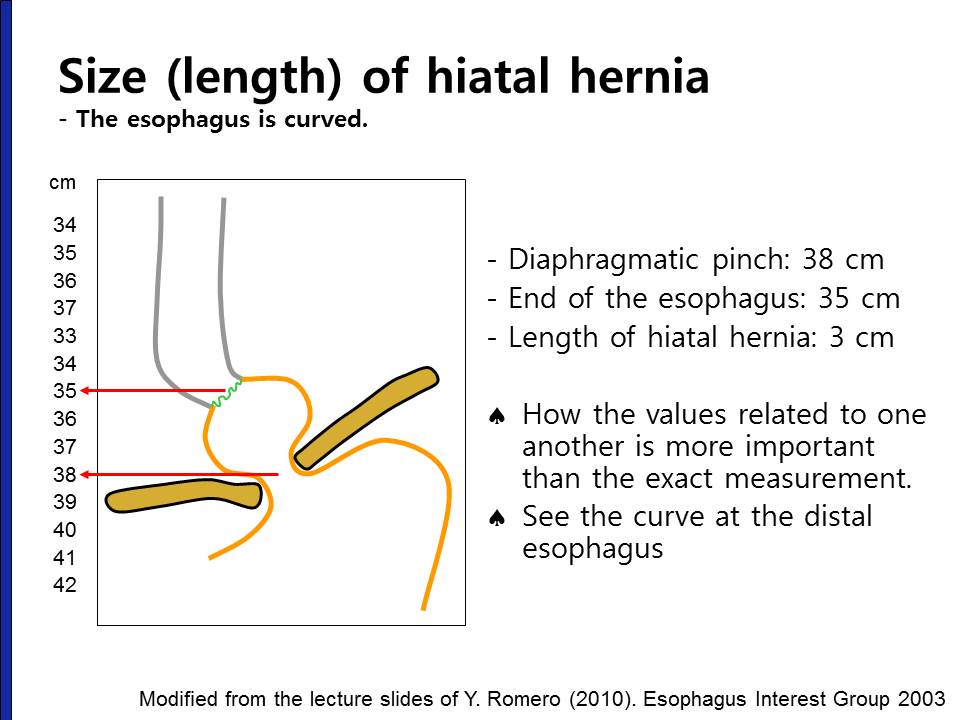
The size of a hiatal hernia can be measured not only vertically, but also horizontally. Sometimes, we call it hiatal width.
With any definition of hiatal hernia, there are some challenges for endoscopists. Upright position is necessary to exactly measure the vertical length. But endoscopy in upright position is impossible. The esophagus may be curved. And we also consider the influence from air inflation and respiration. Paraesophageal hernia is also very confusing. And finally, short segment hiatal hernia less than 2 cm may have some clinical importance.
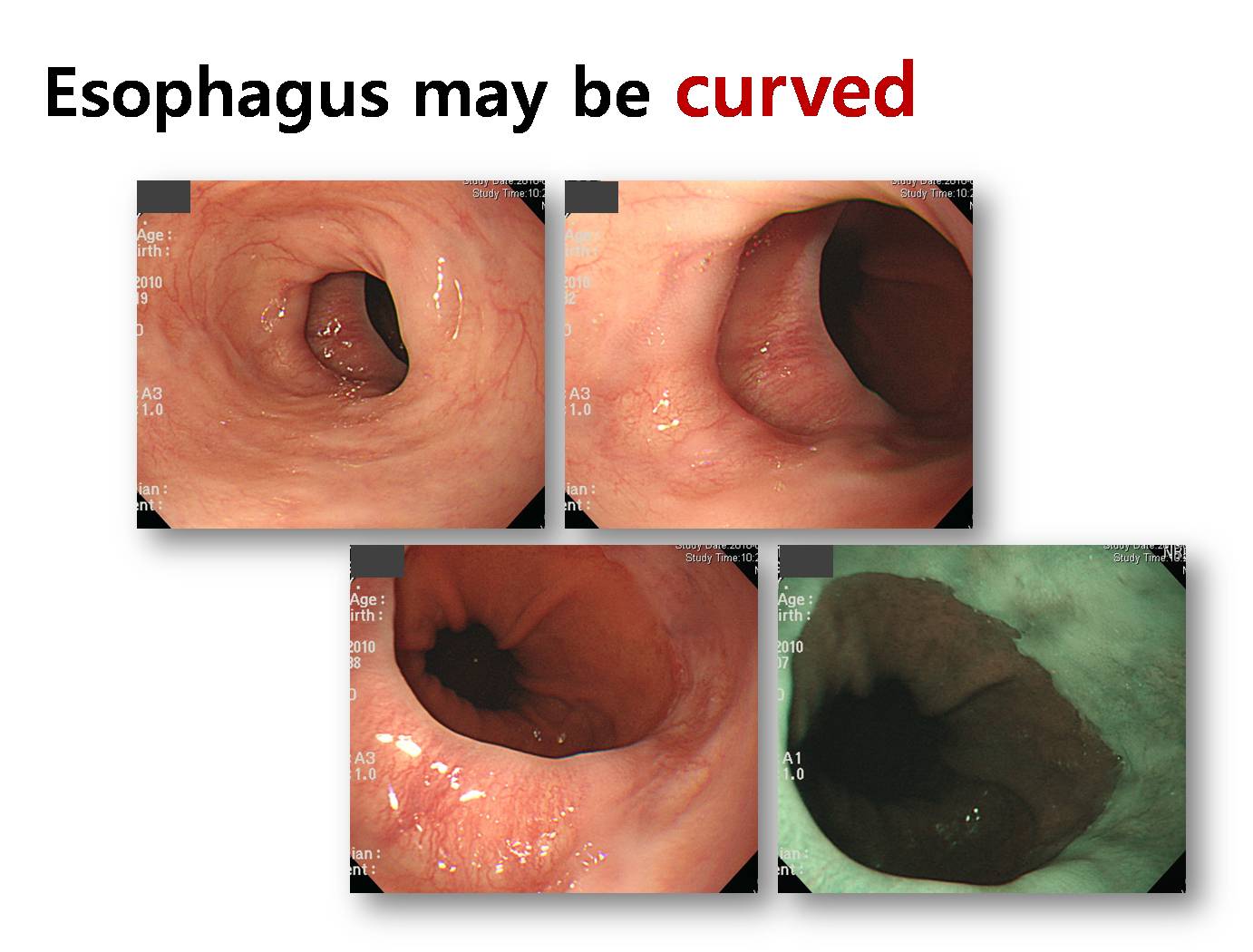
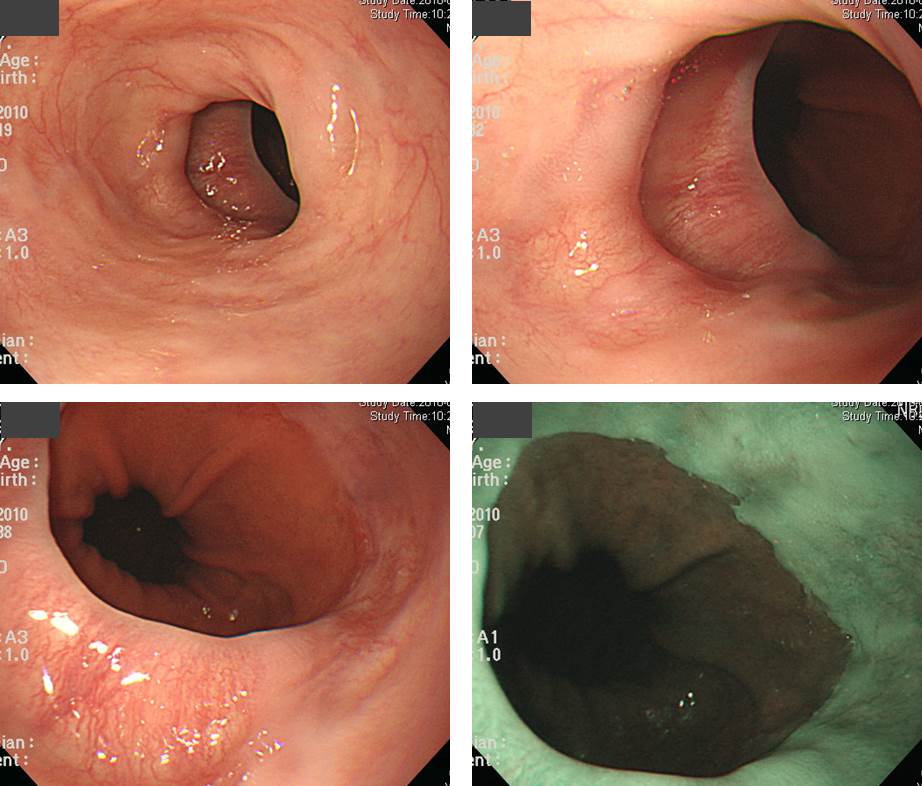
As you can see in these pictures, distal esophagus is quite often curved especially in the elderly population.
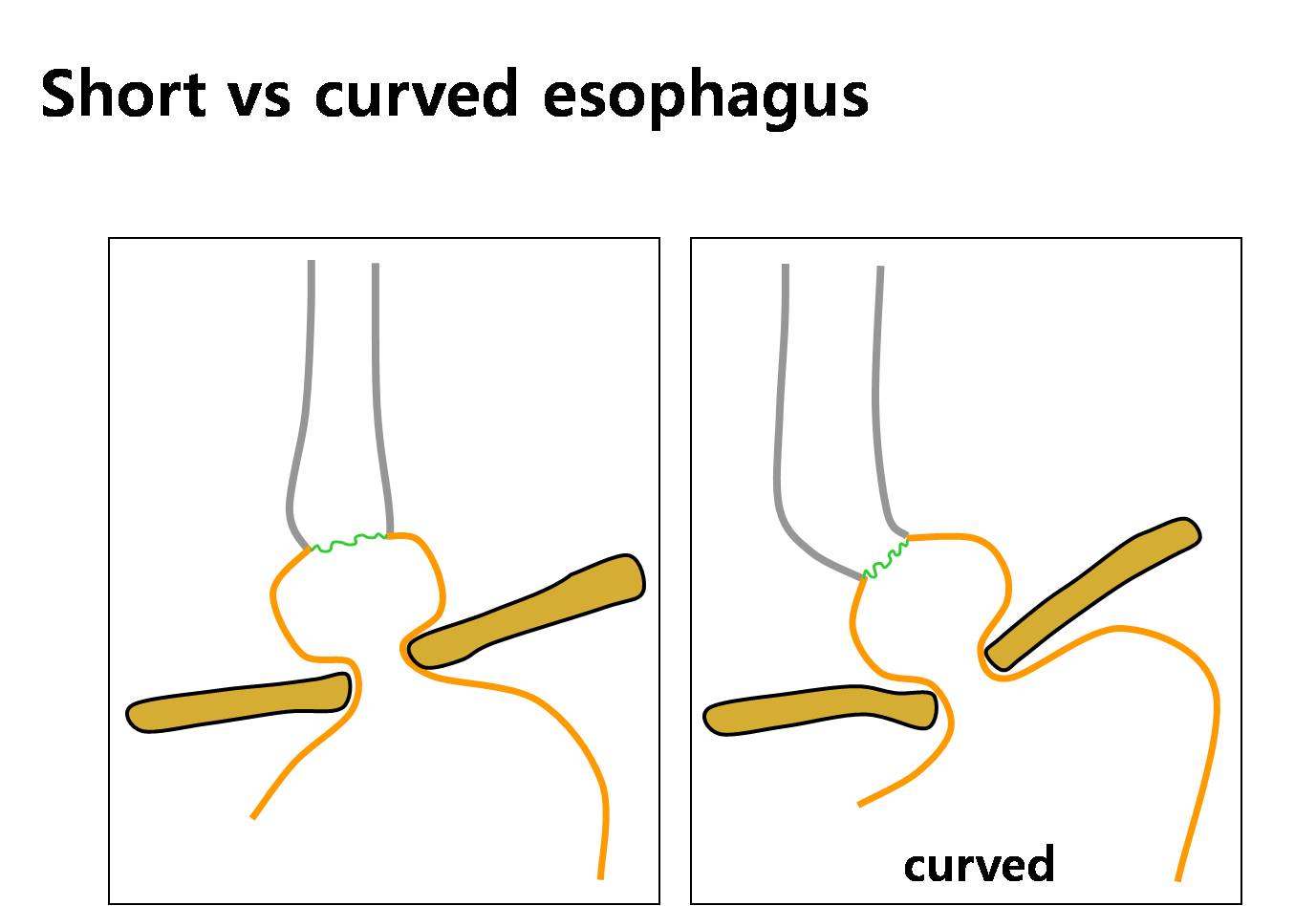
When the esophagus is straight, it is relatively easy to measure the length of the hiatal hernia. However, when the distal esophagus is severely curved, measuring the vertical length is sometimes difficult.
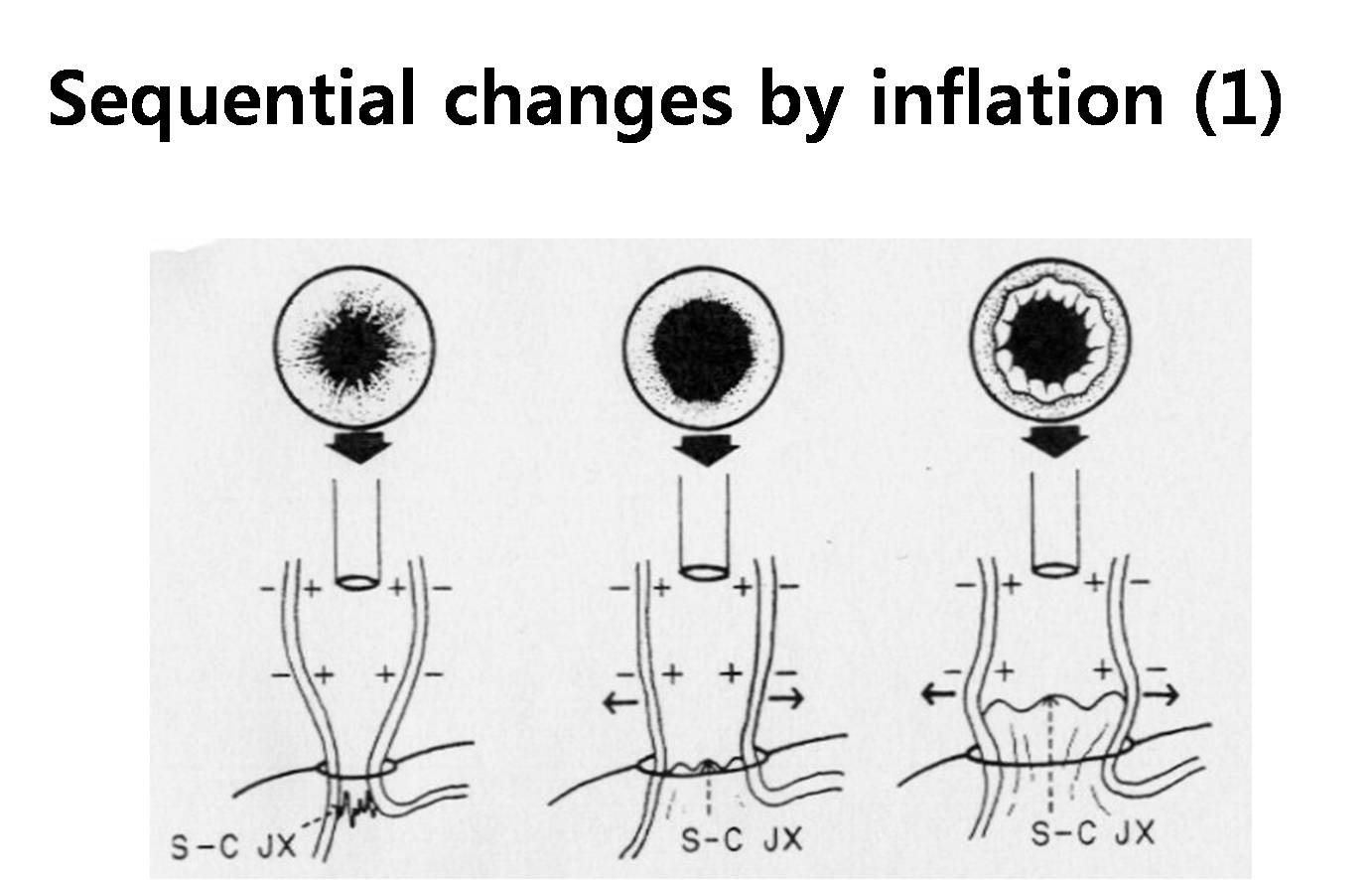
With air inflation, the distal esophagus looks quite differently.

When you push a lot of air, distal esophagus can be changed like the right-side cartoon.
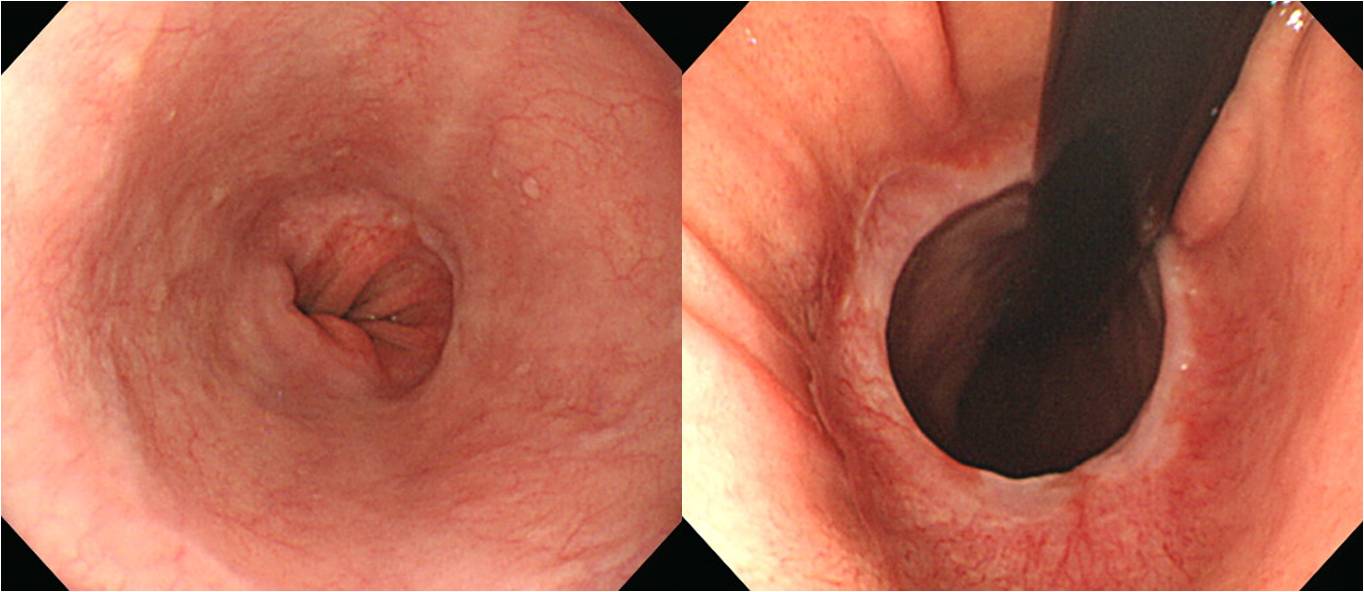
This is an example. Distal esophagus in the straight view and in the retroflection view is quite different. It is mainly due to air inflation.
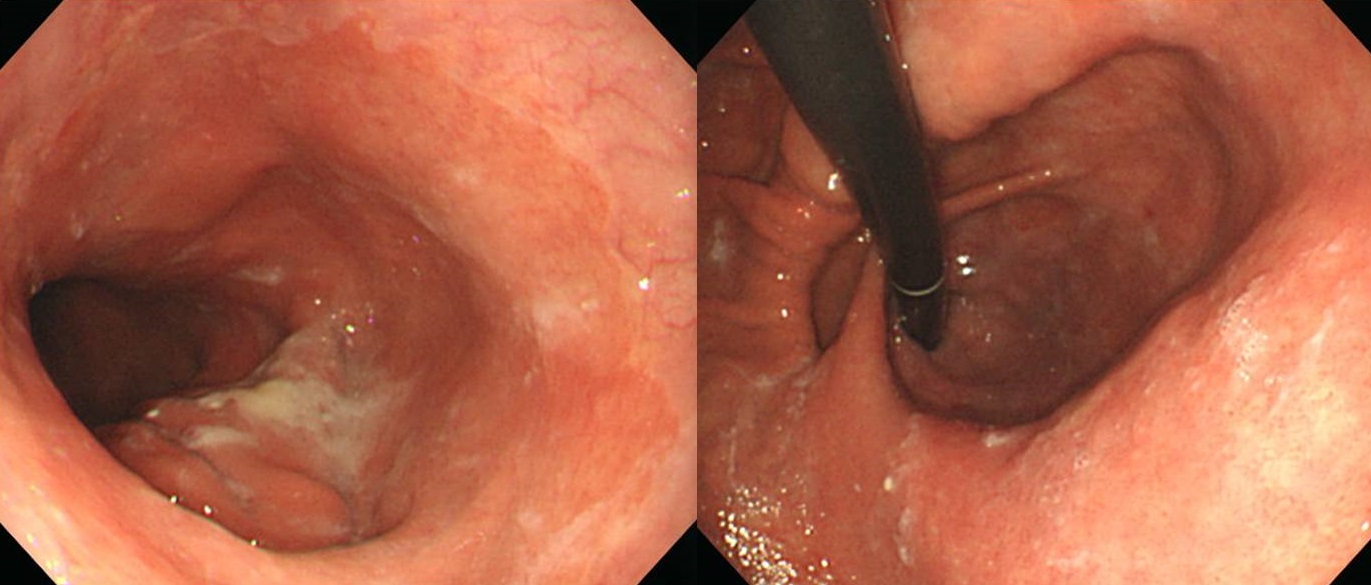
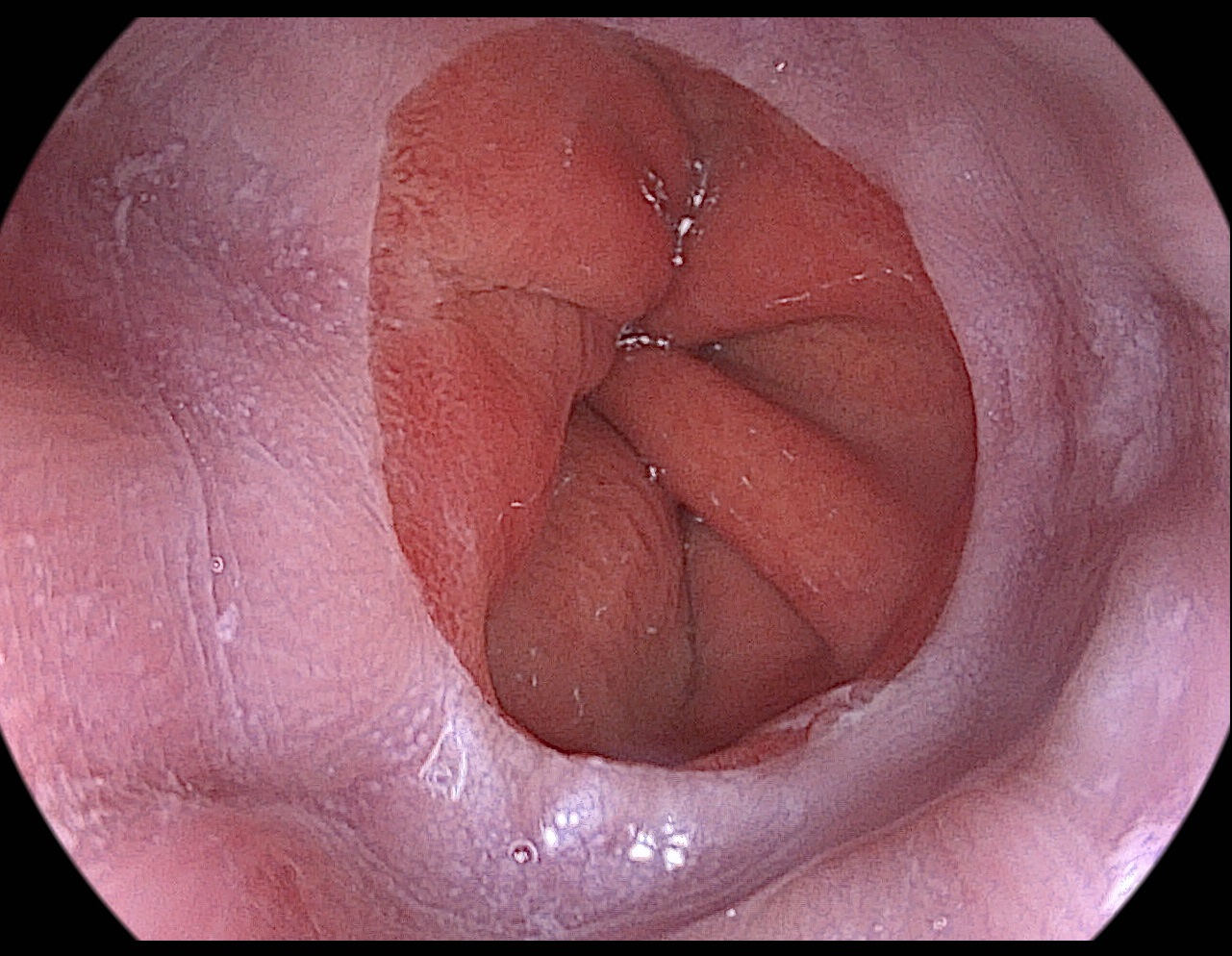
When sliding hiatal hernia is mixed with paraesopharaesophageal hernia, the landmarks for measuring the vertical length become unclear.
What’s your opinion about these pictures? Do you think there is a hernia or not?
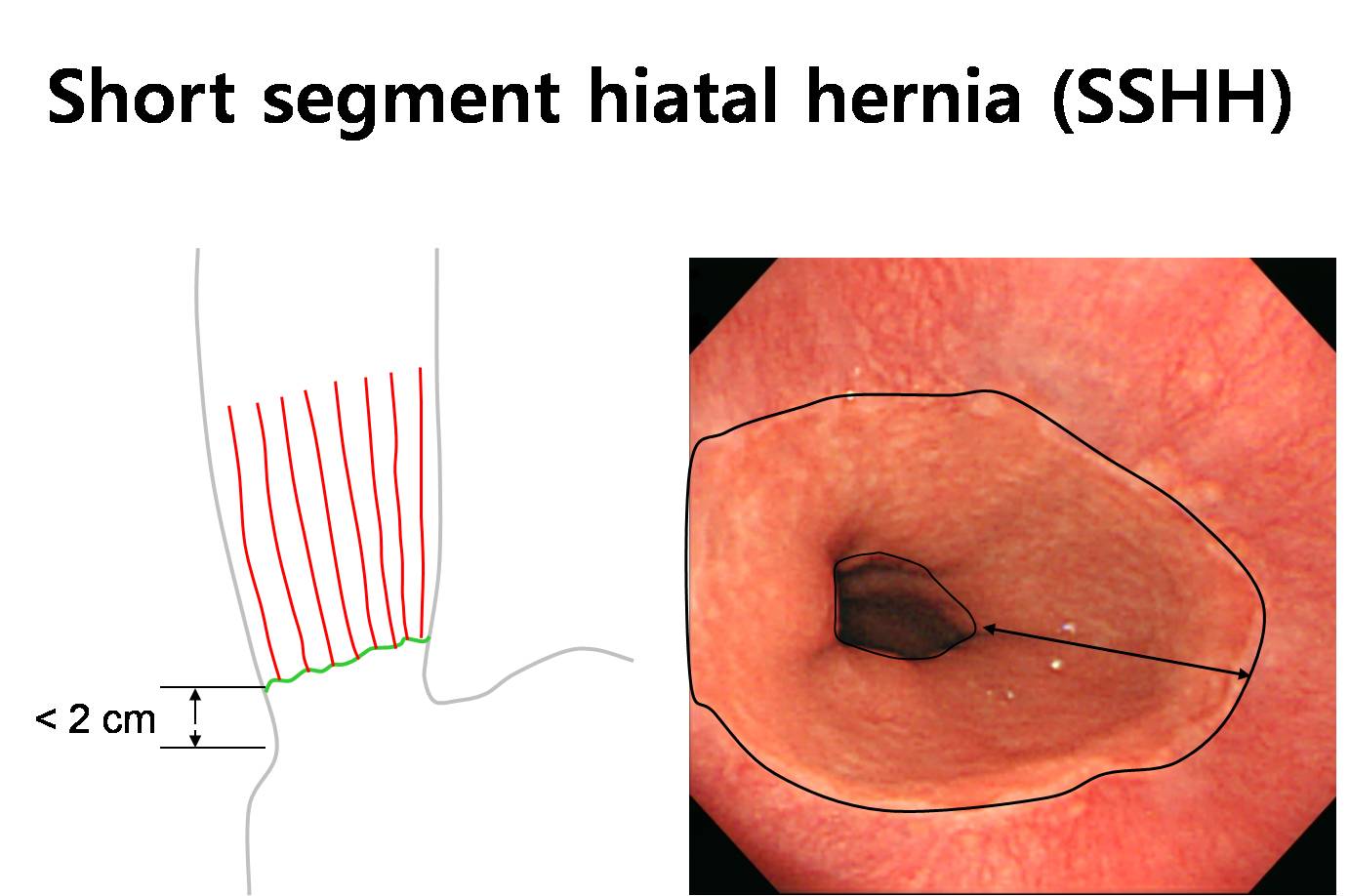

A simple small hiatal hernia measuring less than 2 cm is sometimes called as short segment hiatal hernia.
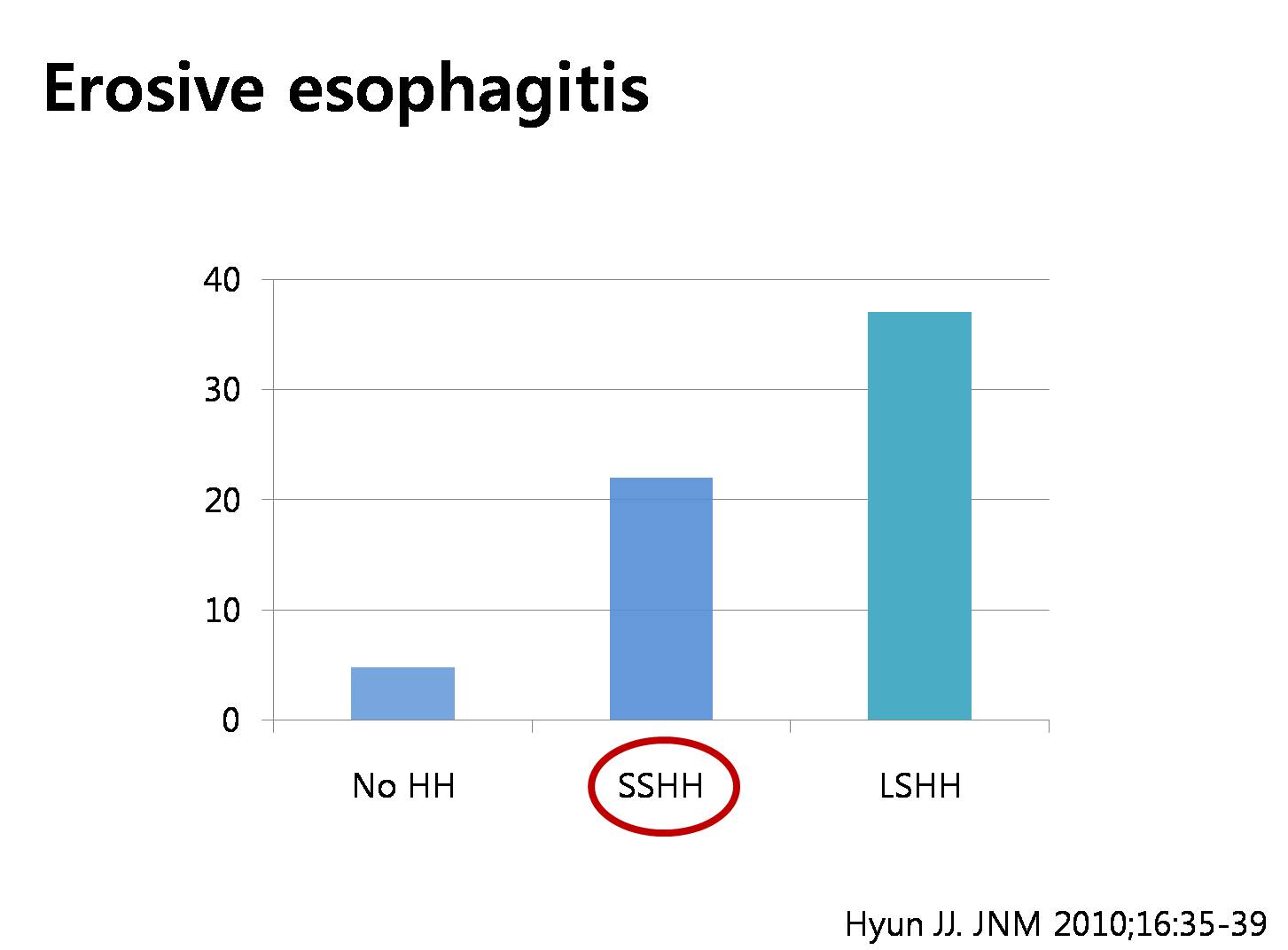
In a recent study, the incidence of erosive esophagitis in patients with short segment hiatal hernia was higher than the normal control and lower than the patients with hiatal hernia more than 2 cm. So, there may be some clinical meaning for hiatal hernia less than 2 cm.
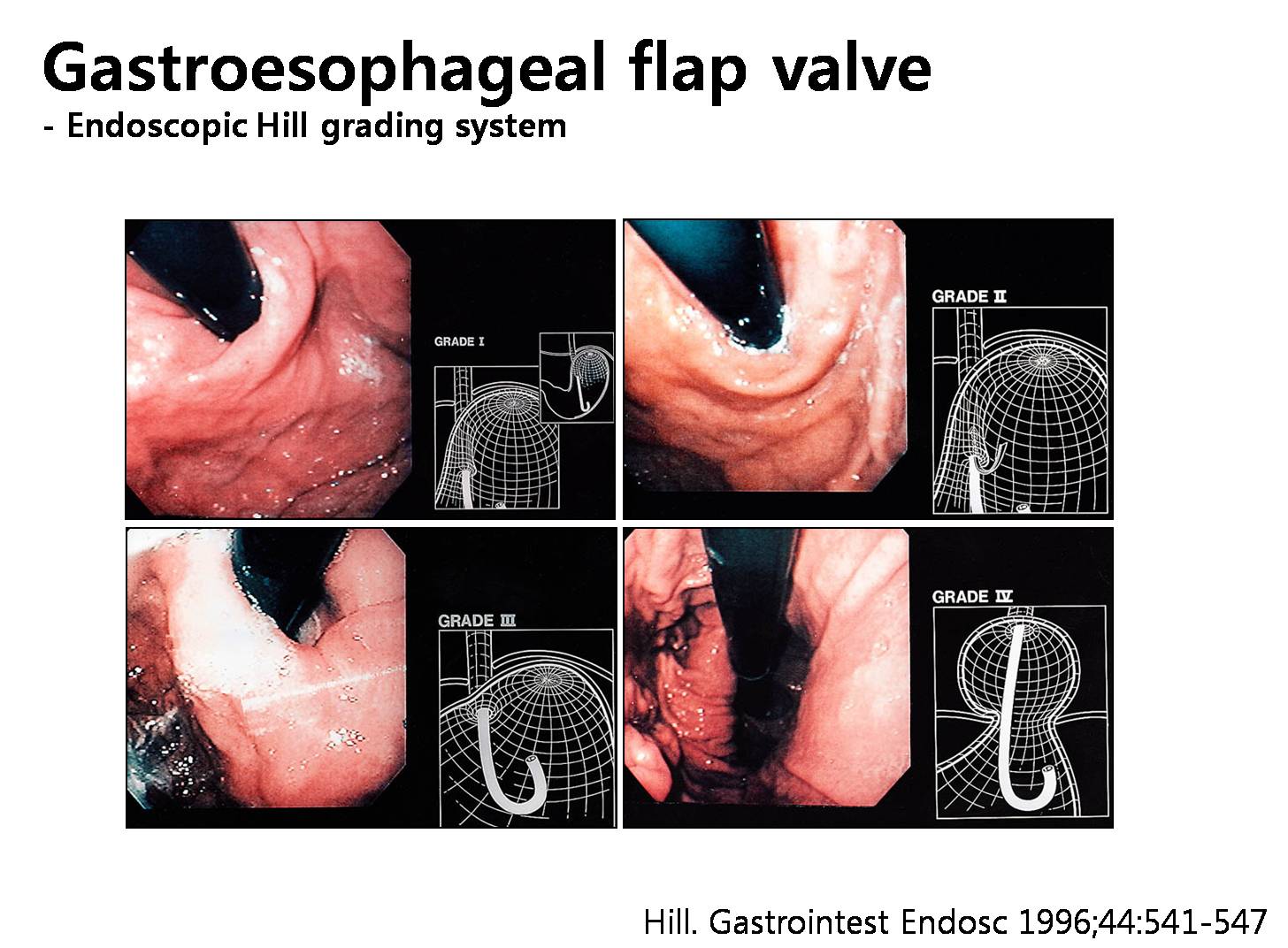
This is a famous Hill grading system for gastroesophageal flap valve. Grade 4 is hiatal hernia but grade 2 and 3 is just weak gastroesophageal flap valve.
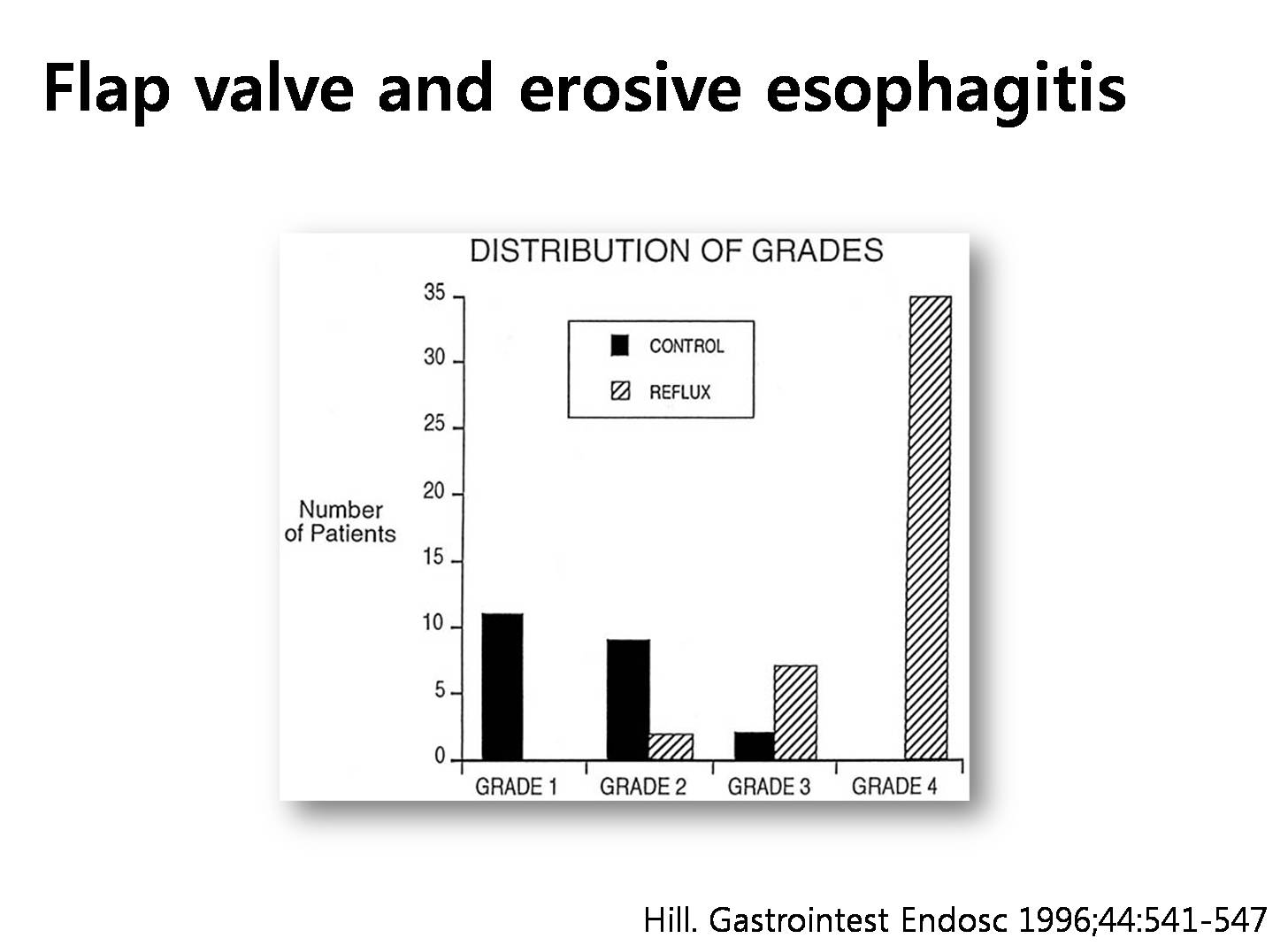
In the doctor Hill’s original study, the appearance of the flap valve was a better predictor of the presence or absence of reflux than LES pressure. We can conclude that there should be something between normal and fixed hiatal hernia.
![]() 8. 강의 - Pathogenesis
8. 강의 - Pathogenesis

During swallowing, the esophageal body shortens, which is caused by contraction of the longitudinal muscles. This results in a proximal movement of the LES and a small portion of the proximal stomach into the thoracic cavity through the diaphragmatic hiatus. After swallowing, all structures return to their original anatomical positions because of the elasticity of the phreno-esophageal ligaments.
A study in opossums showed that acid exposition to the esophagus induces esophageal shortening. Acid gastro-esophageal reflux itself might induce, maintain or even increase a sliding hiatus hernia.
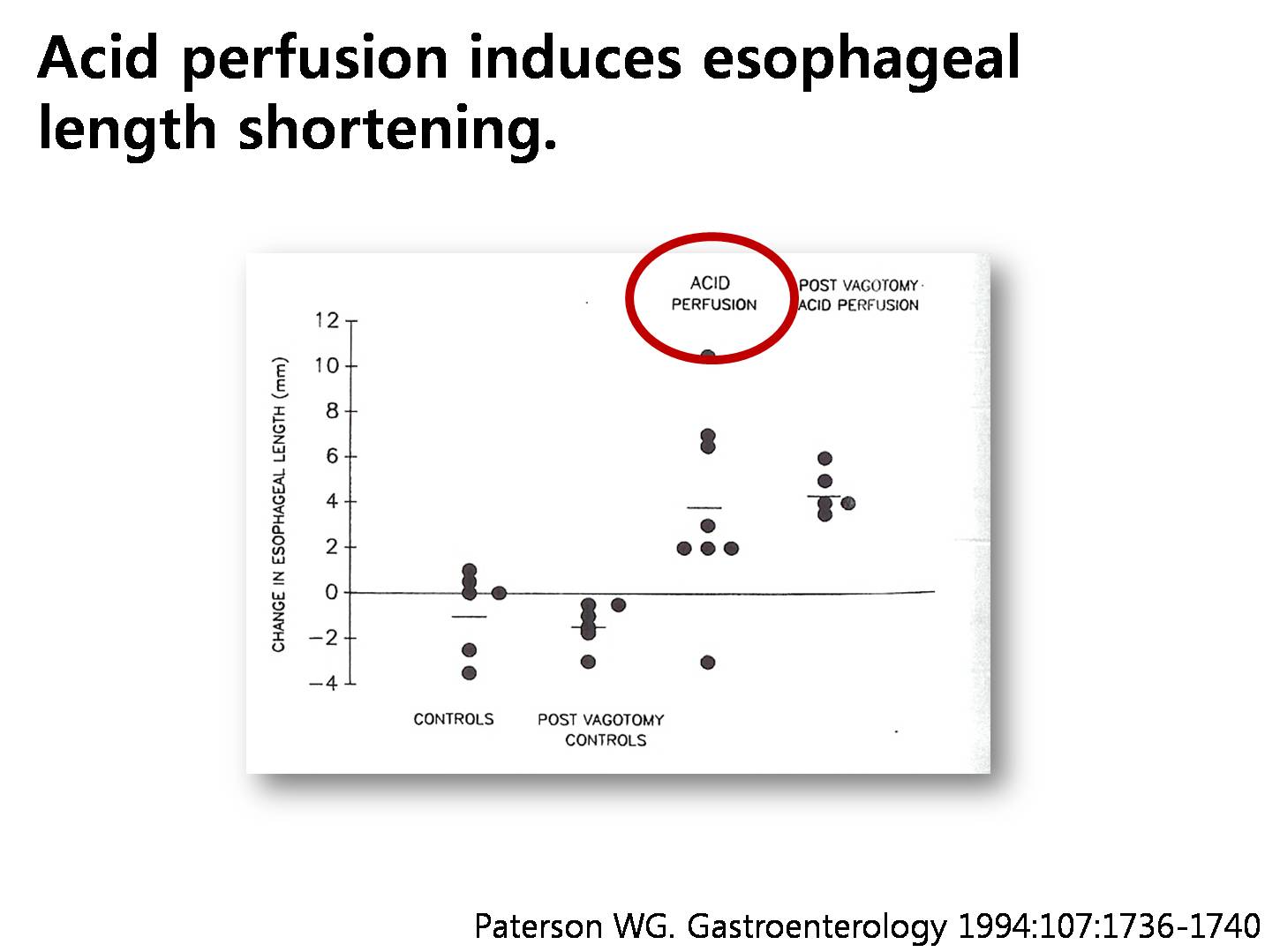
This figure clears shows that acid perfusion induces esophageal length shortening, which can lead to the development of hiatal hernia.

Another possible mechanism is the degeneration of the phrenoesophageal ligament.
![]() 9. 강의 - Hiatal hernia as a dynamic entity.
9. 강의 - Hiatal hernia as a dynamic entity.

All hiatal hernias are not the same. In the barium esophagography, the shape of the gastroesophageal junction is quite variable in terms of hiatal hernia.
Previously, doctor Sloan defined the reducing hiatus hernia as a hernia occurring only during mid-swallows, but reducing between swallows. It represents a stage in the development of fixed hiatal hernia.
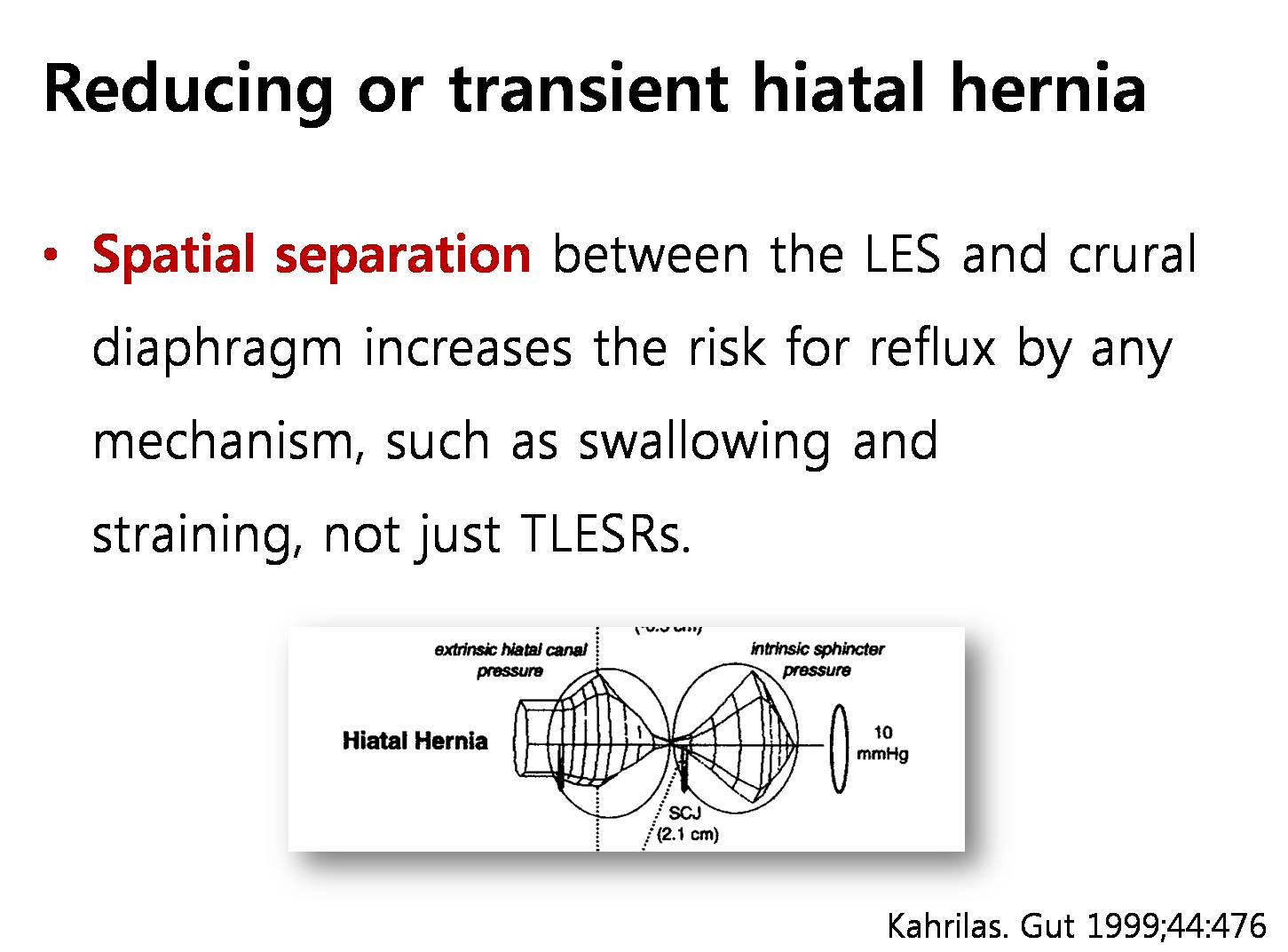
What is the effect of reducing or transient hiatal hernia? It is the spatial separation. Spatial separation between LES and crural diaphragm increases the risk for reflux by any mechanism, such as swallowing and straining, not just TLESRs
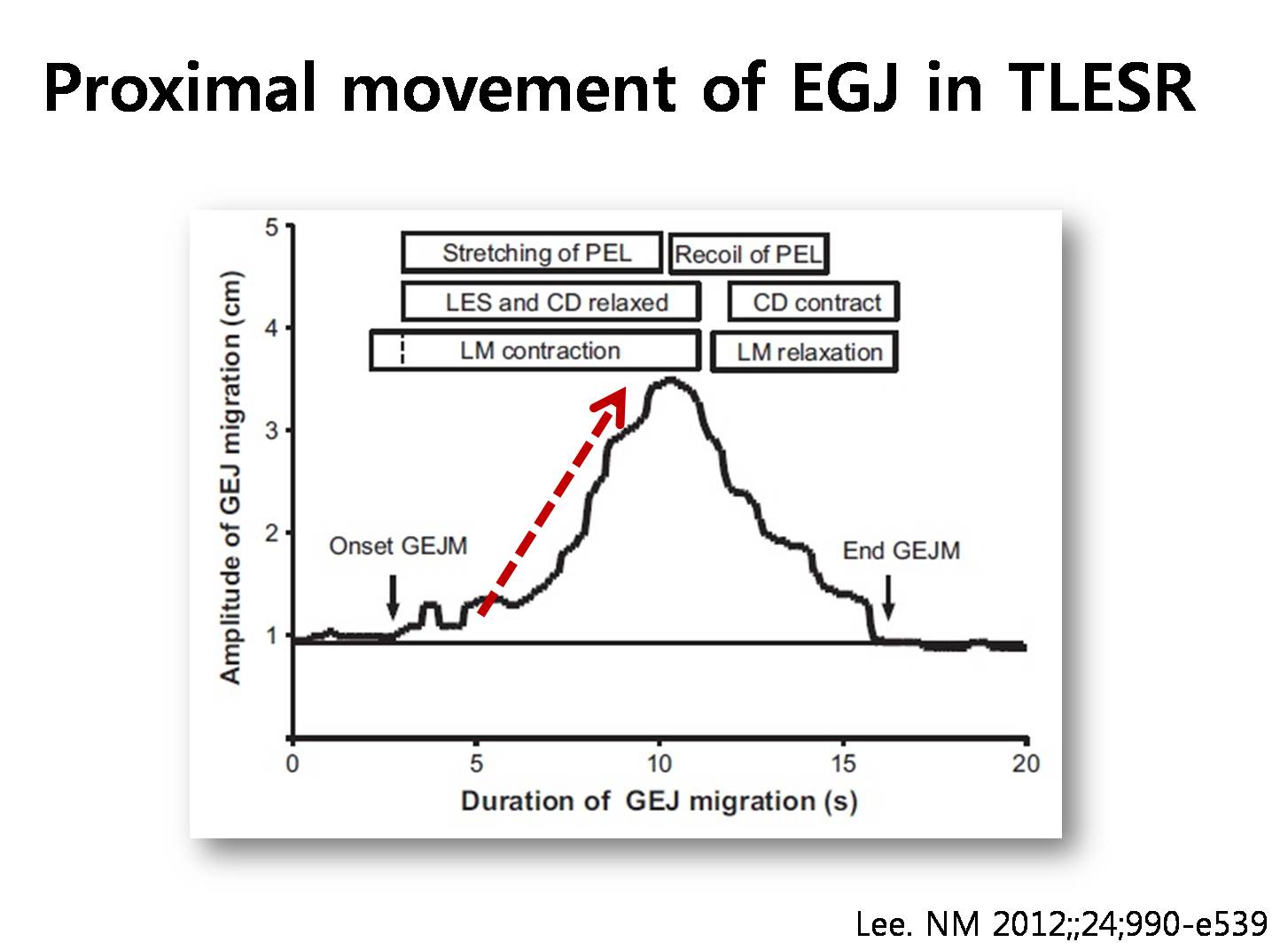
Transient LES relaxation also can induce transient hiatal hernia, because upward migration of gastroesophageal junction is occurring during the transient LES relaxation.
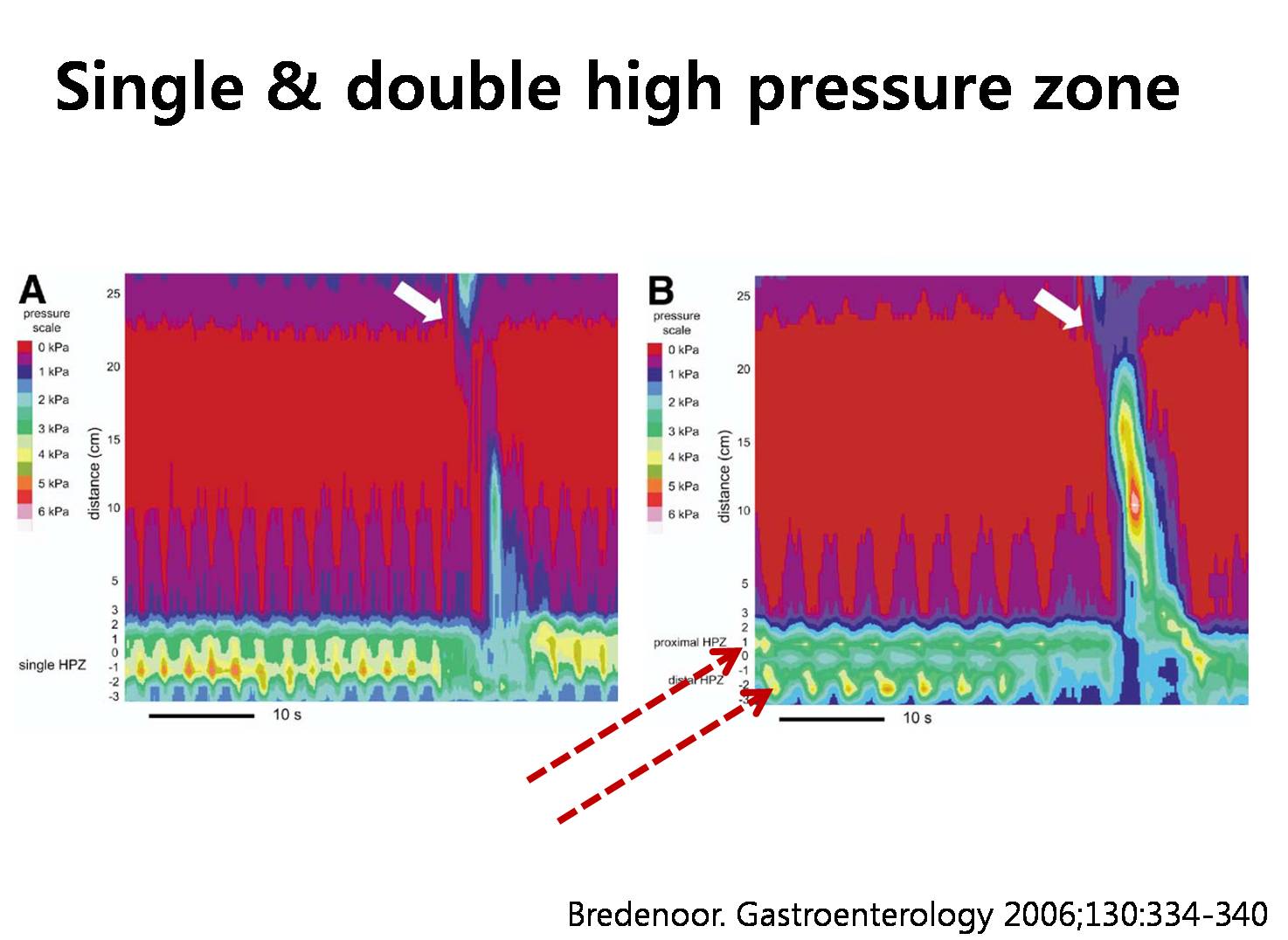
In the high-resolution manometry figure of the right-hand side, the arrows indicate the transient separation of high pressure zone, the meaning of which is exactly the same as the transient hiatal hernia.
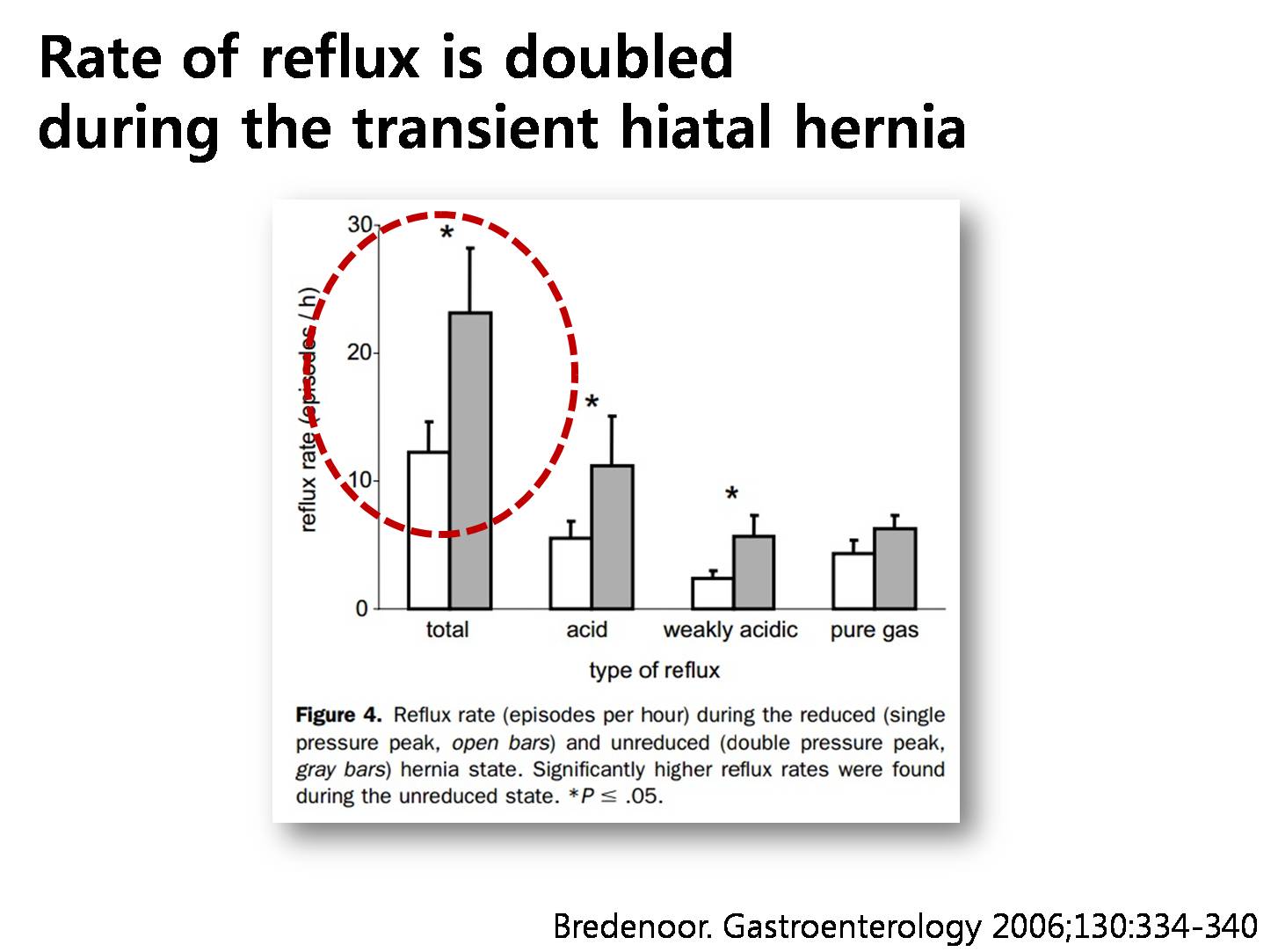
The rate of reflux is doubled during the transient hiatal hernia than the reduced state, and most of them was acid or weakly acidic reflux.
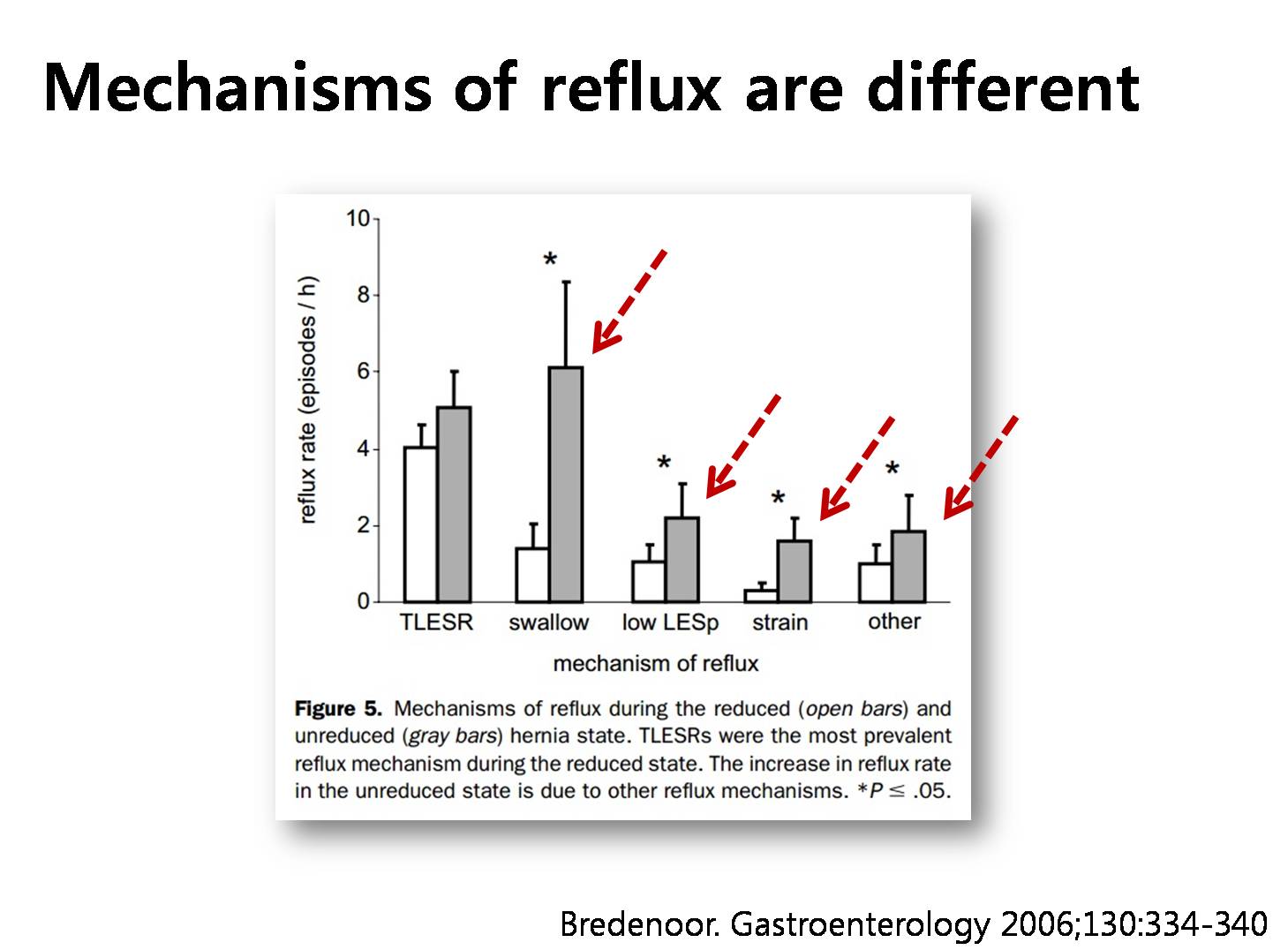
Moreover, the mechanisms of reflux are different in the transient hiatal hernia state. Mechanisms other than transient LES relaxation were much more common in the transient hiatal hernia state.

Now, we can say that anatomy and function is closely related.
![]() 10. 강의 - Relationship between hiatal hernia and the development of GERD symptoms.
10. 강의 - Relationship between hiatal hernia and the development of GERD symptoms.
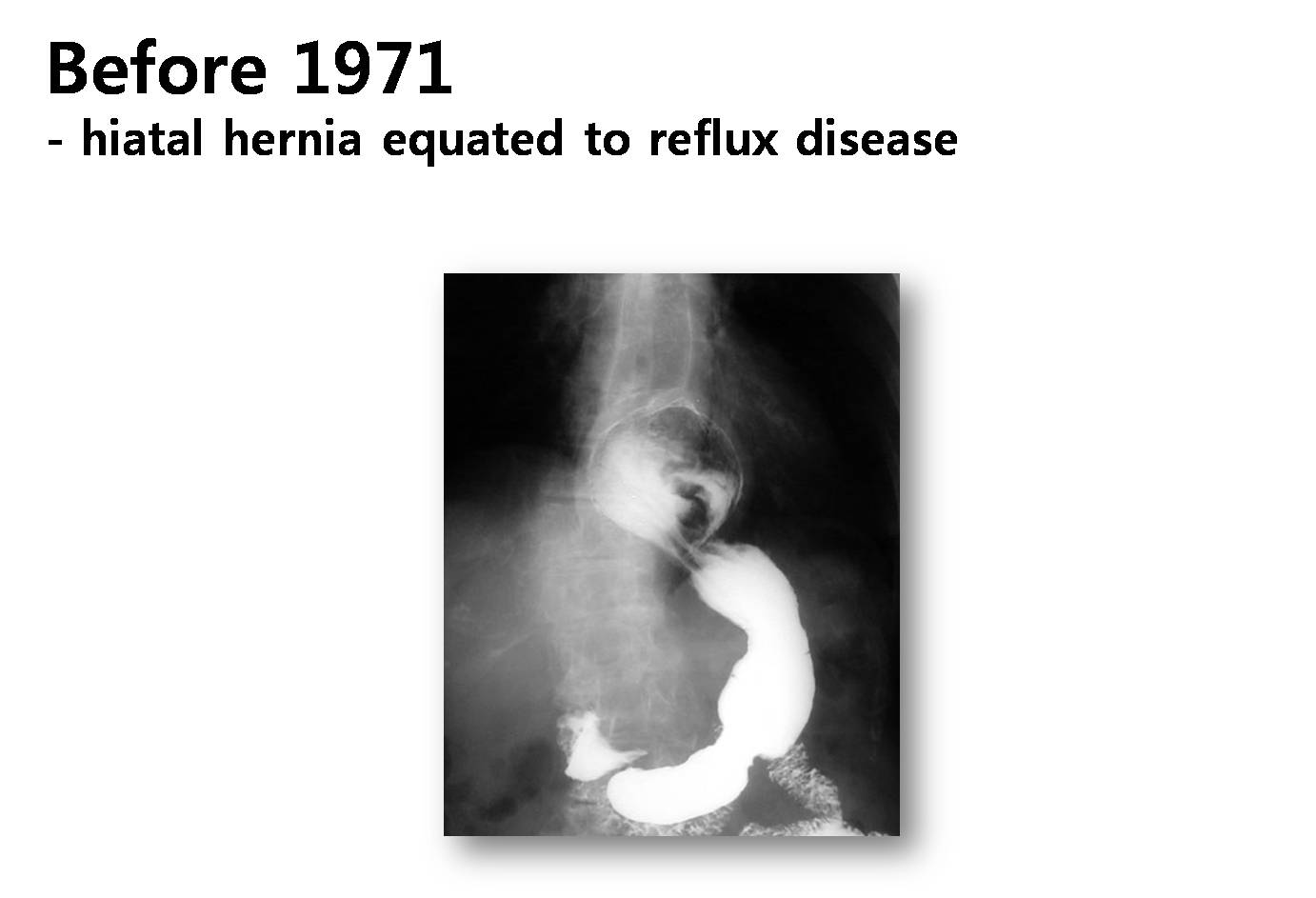
Before 1971, hiatal hernia was a hallmark of gastroesophageal reflux disease. However, after 1971, the meaning of hiatal hernia was shrunk. It became regarded as epiphenomenon. What happened in 1971?

In cases with severe hiatal hernia, prominent mucosal breaks are usually seen.
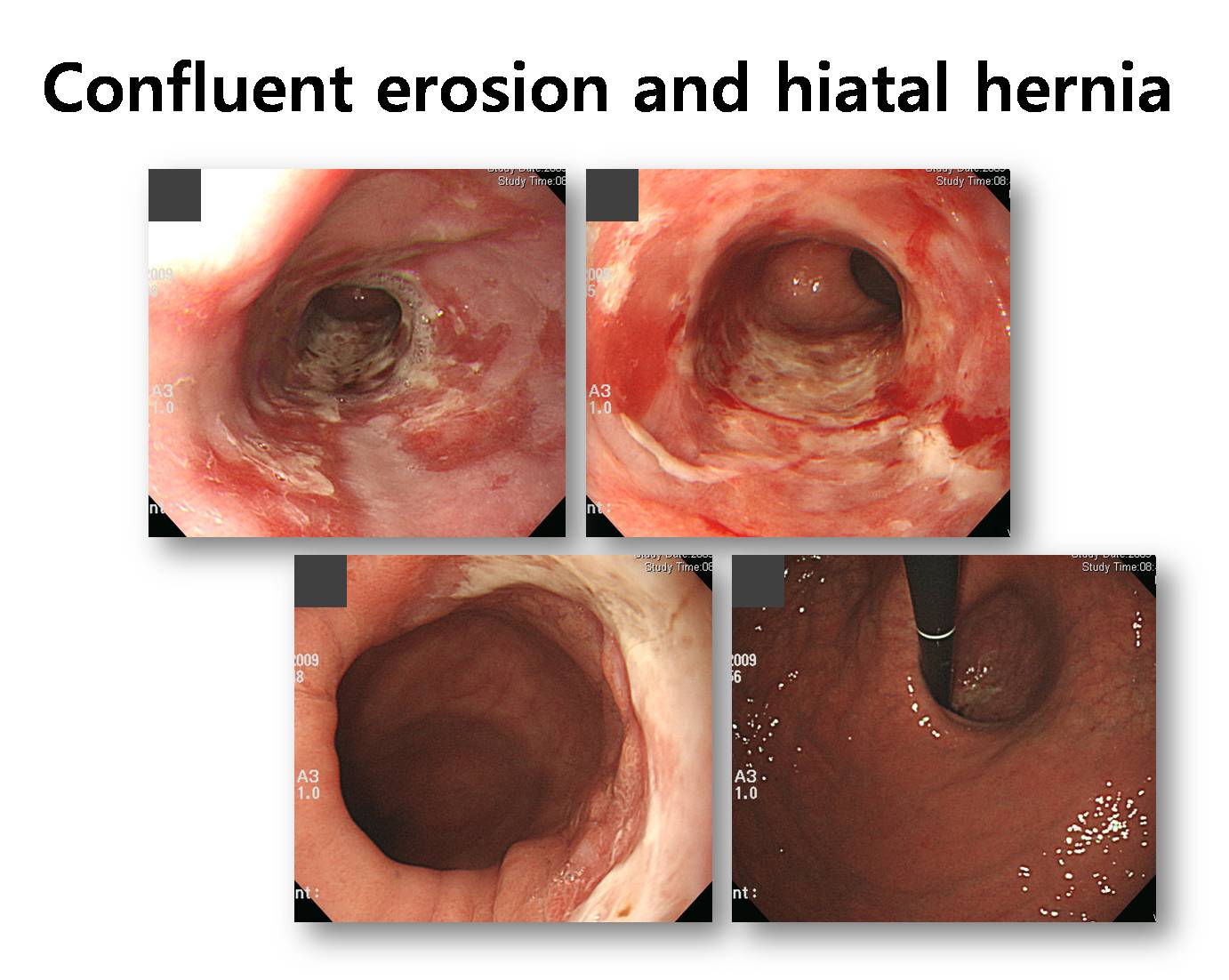
This is another case of hiatal hernia with severe confluent mucosal breaks. It is LA group D reflux esophagitis.

In 1971, Dr Cohen published a famous report in New England Journal of Medicine. He showed that the mean LES pressure was not different between patients with hiatal hernia and the control. In patients with GERD, the LES pressure was not different by the presence of hiatal hernia. After this clear finding, the meaning of hiatal hernia was under-valued. I think the wrong conclusion of this study came from limitations of the study methodology of that time.
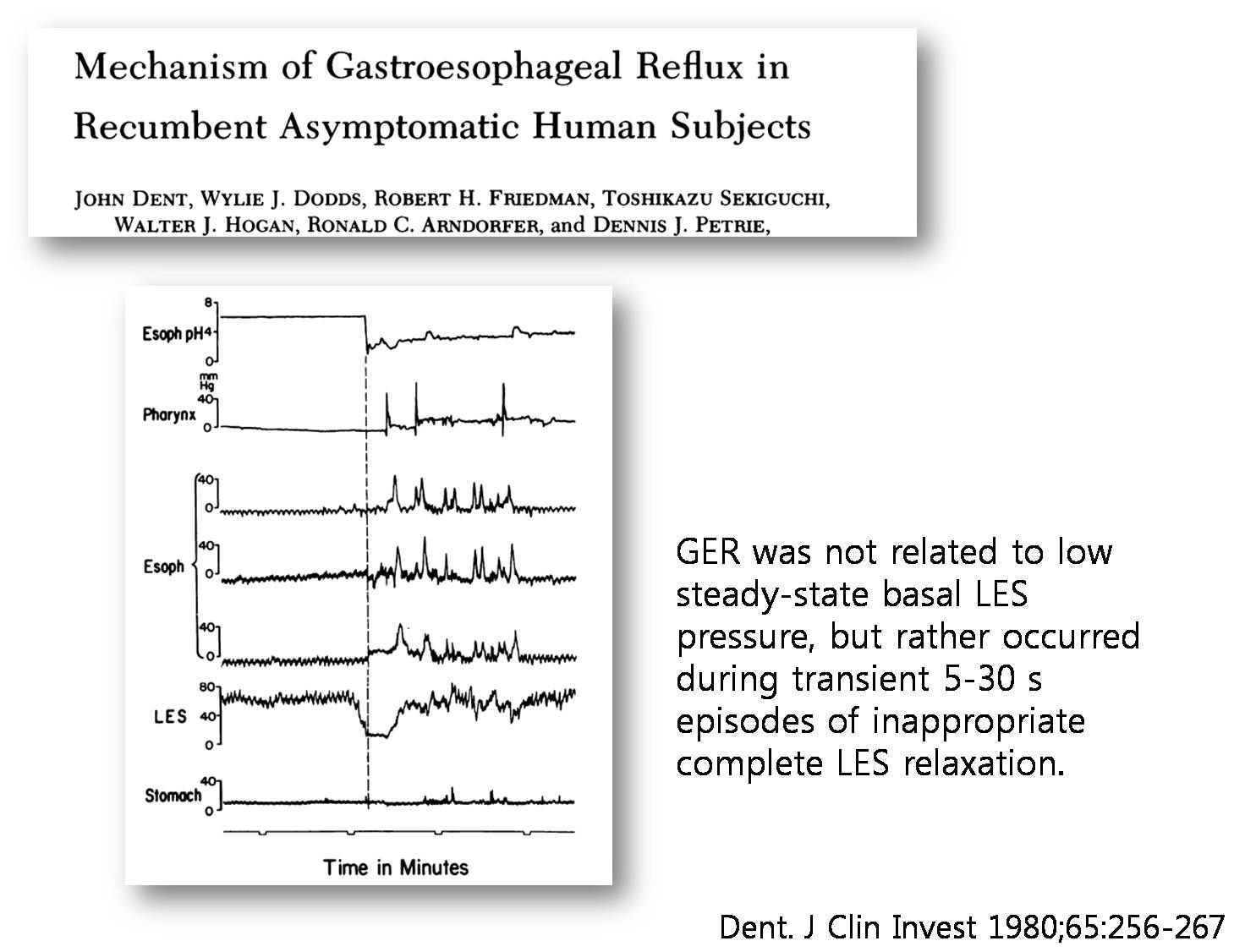
As you know, in 1980, Dr Dent found an important phenomenon. LES relaxation usually occurs after swallowing some food. However, after a meal, LES relaxations occur without swallowing. This is called transient LES relaxation.
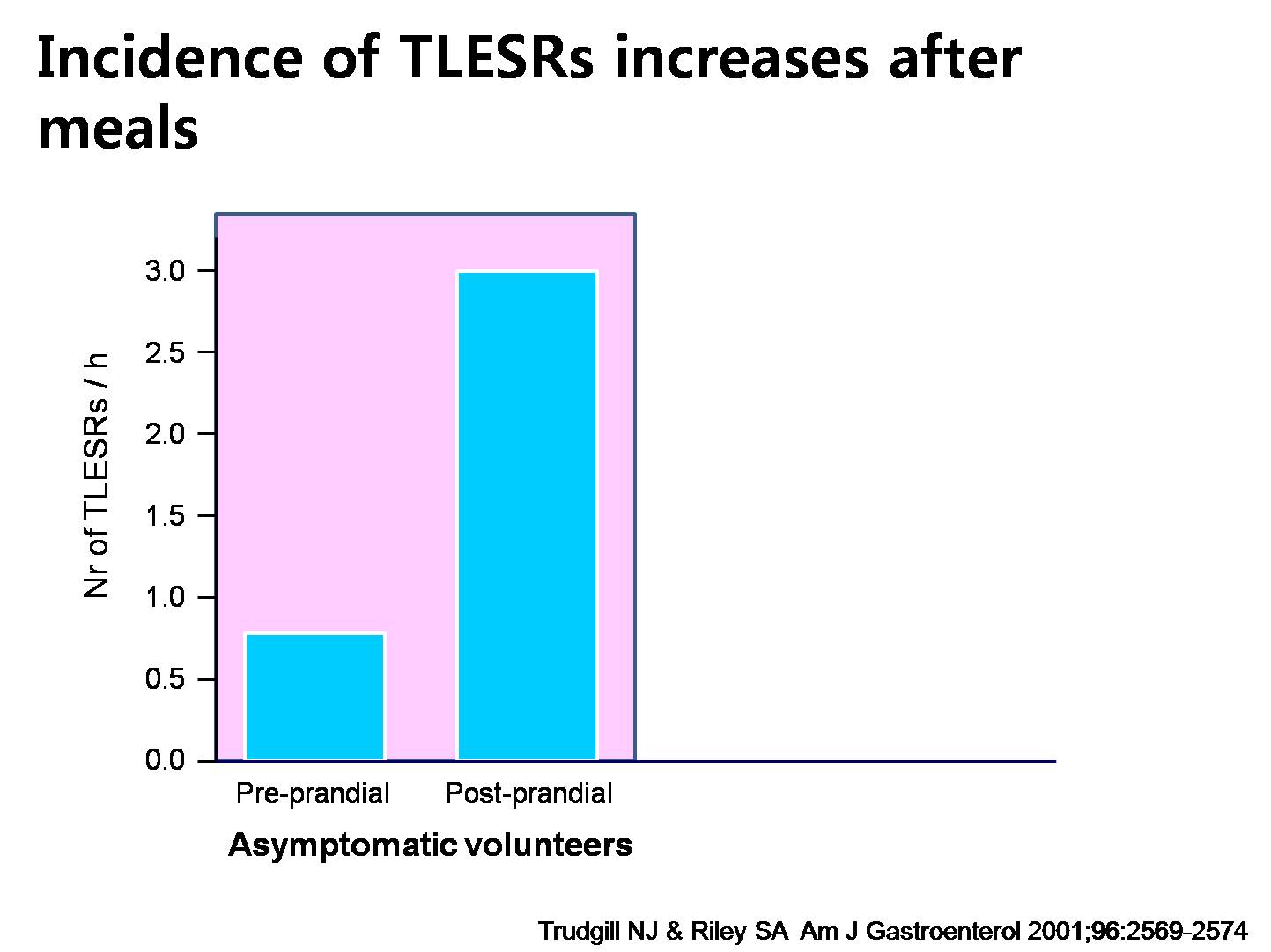
This study showed 3 important characteristics of TLESR. First, they occur more often after a meal.

Second, TLESR do not occur more frequently in GERD patients than control.
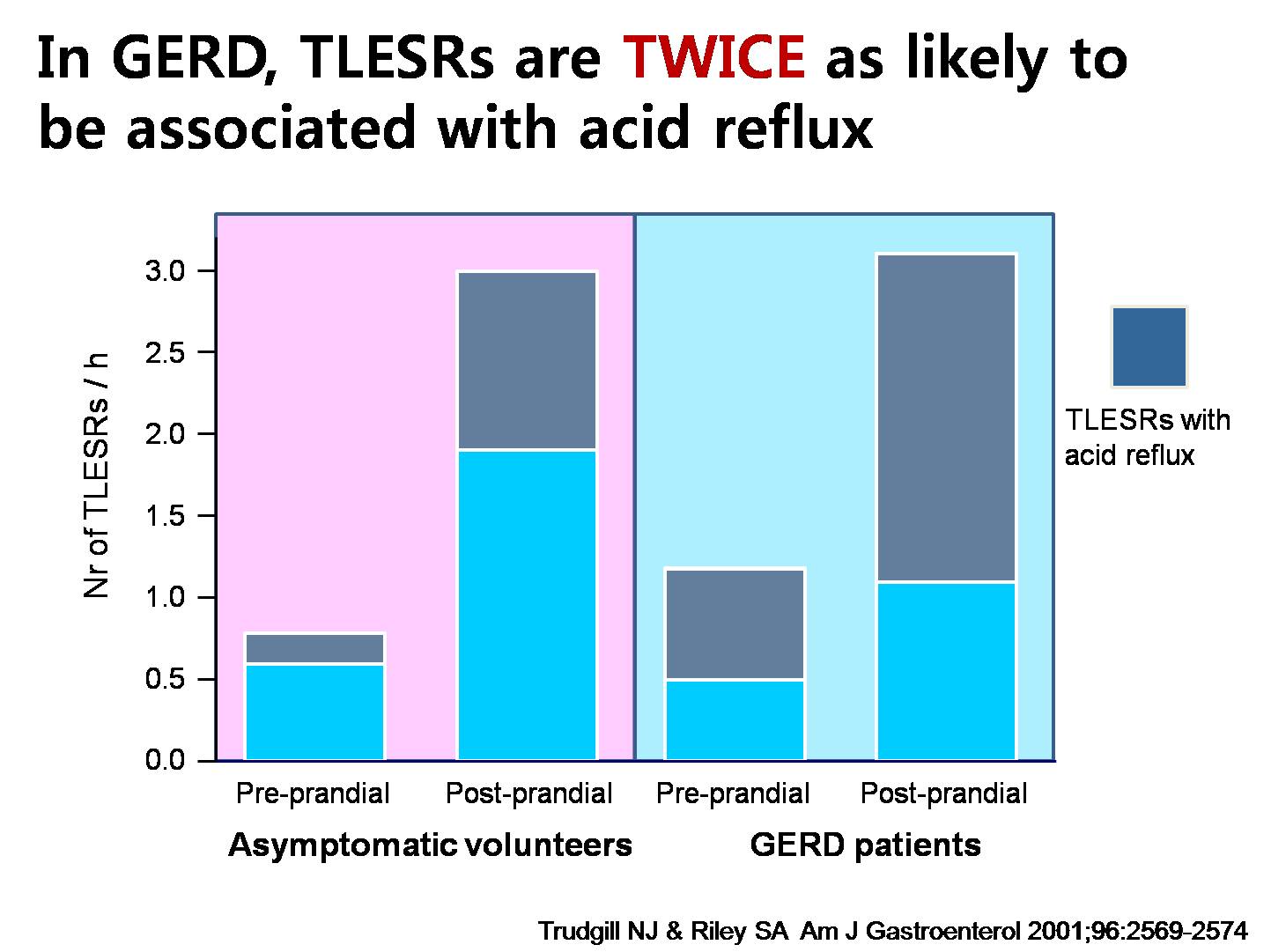
Finally, in GERD, TLESRs are twice as likely to be associated with acid reflux. It suggests that the meaning of TLESR is different between GERD patients and control. There must be another factor other than TLESR in the development of GERD symptoms. As you can guess, it is the hiatal hernia.
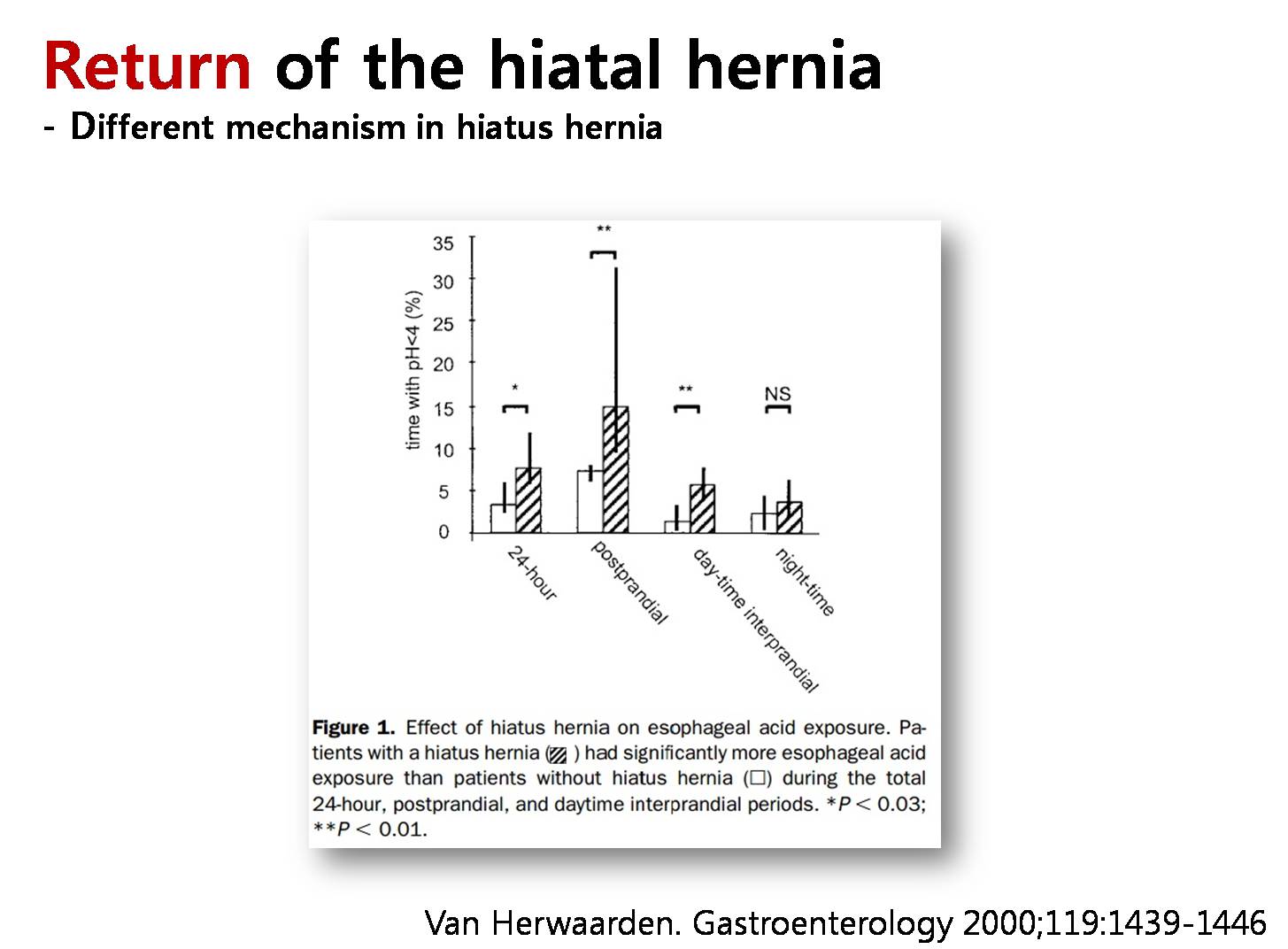
This slide shows the mechanism acid reflux in GERD patients without hiatal hernia. The increase in reflux episodes in patients with a hiatal hernia is mainly explained by the observation that, in addition to TLESRs, other mechanisms come into play. Indeed, half of the reflux episodes in patients with GERD with a hiatal hernia occur during swallowing or straining. We can say that hiatal hernia is important.
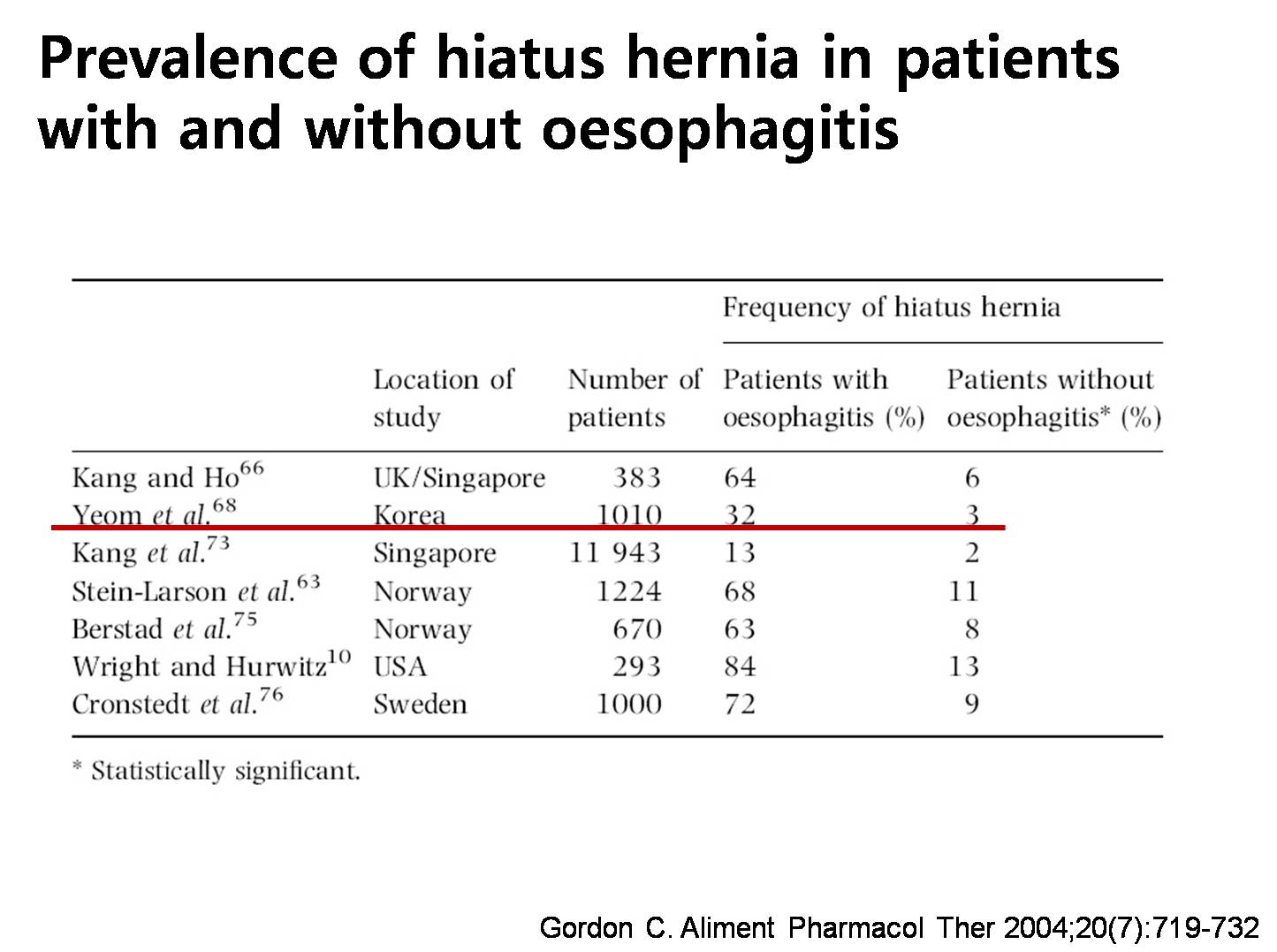
In a Korean study by Dr. Yoem from Yonsei University, the frequency of hiatal hernia in patients with reflux esophagitis was 32 %, which is much higher than 3 % in the control. So hiatal hernia must be very important in the pathogenesis of reflux esophagitis.
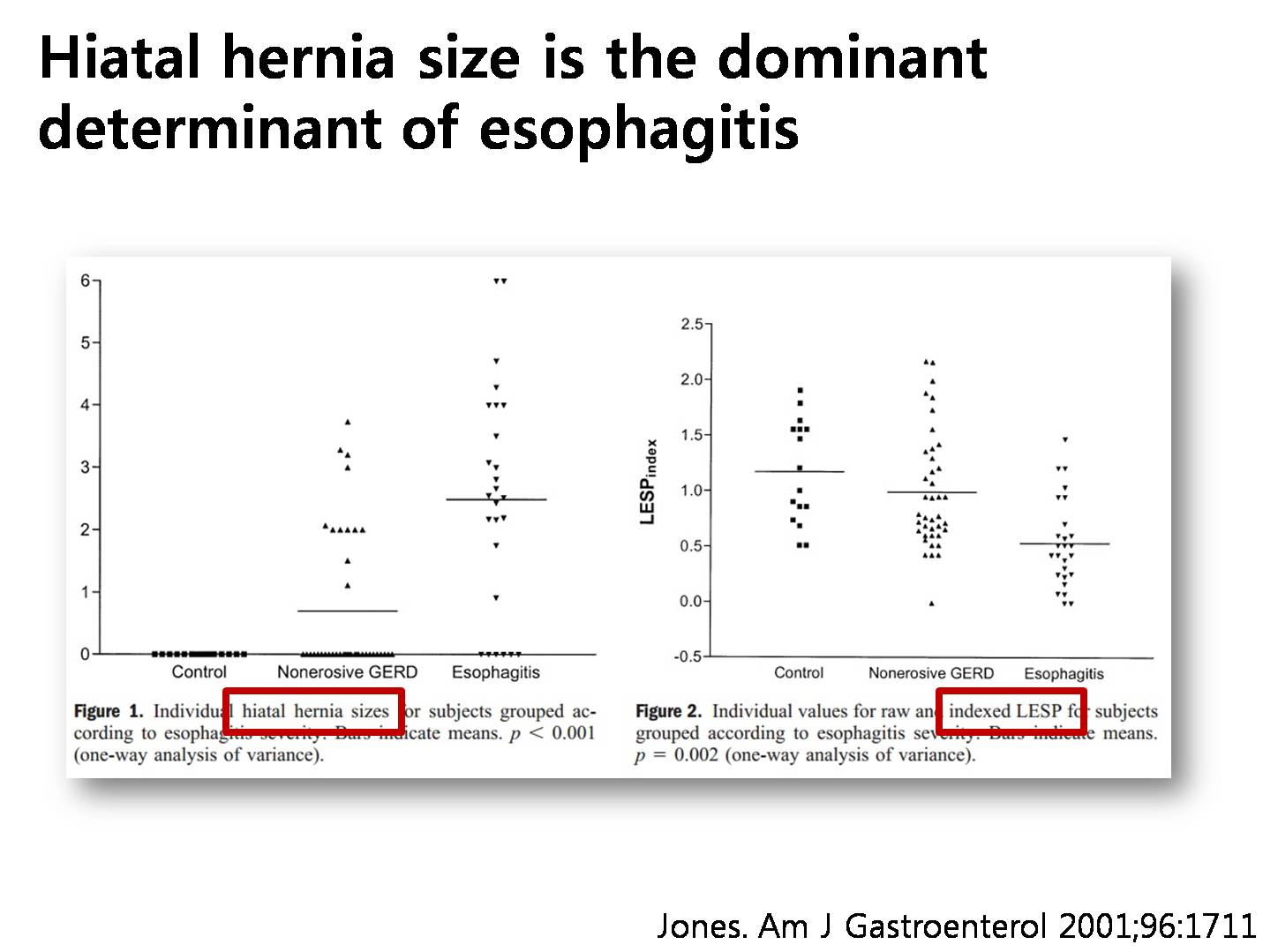
In this beautiful study, doctor Jones identified that the size of the hiatal hernia and lower esophageal sphincter pressure were significant predictors of erosive esophagitis. Actually, hiatal hernia size is the dominant determinant of esophagitis.
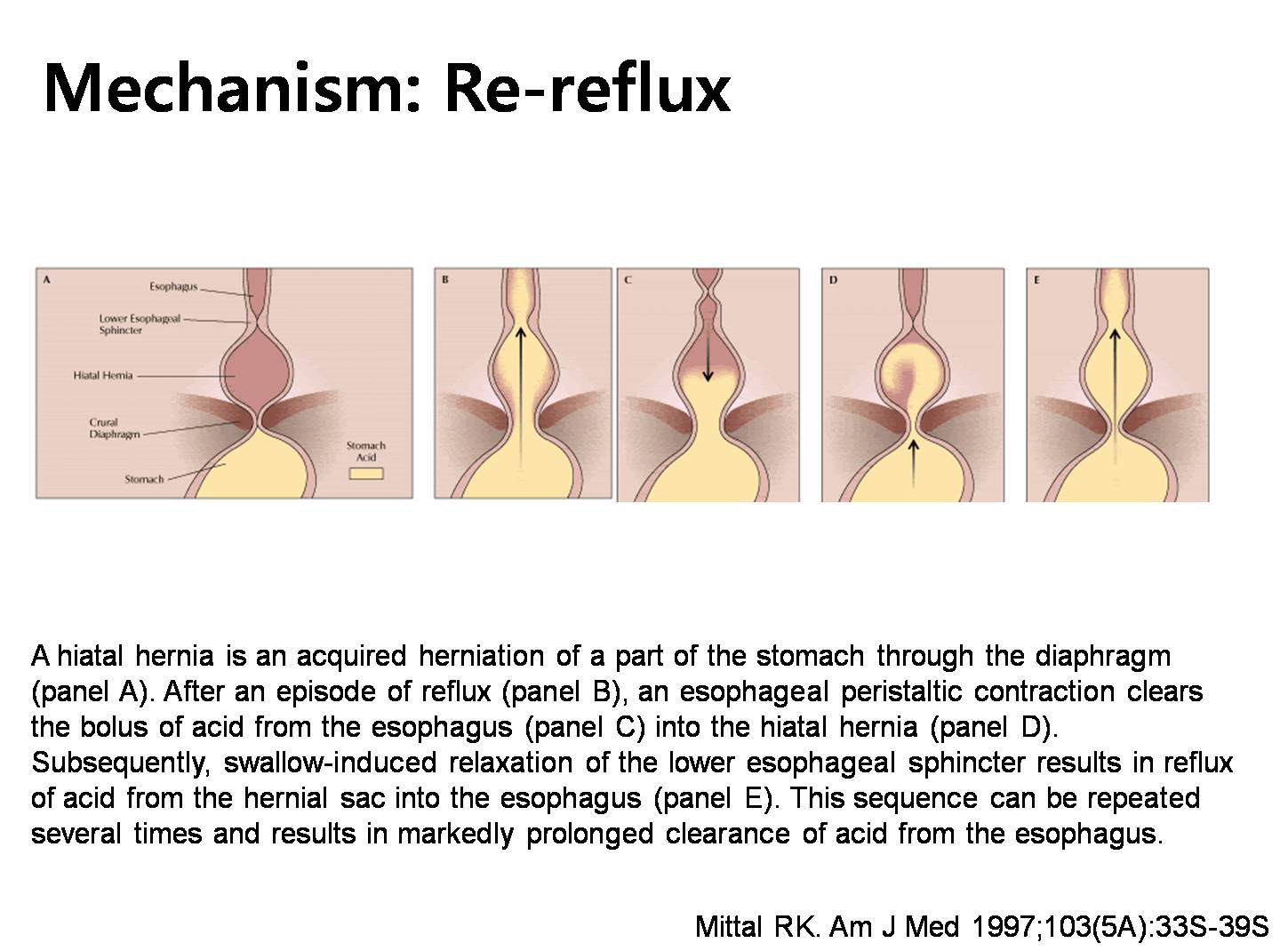
Hiatal hernia is closely related to the reflux symptoms. I previously explained it in terms of the pressure barrier. Are there any other mechanisms? Doctor Mittal once mentioned re-reflux of the acid in the hernia sac. The hiatal sac may function as a reservoir from which acidic fluid can re-reflux into the esophagus after swallowing or during periods of low sphincter pressure.
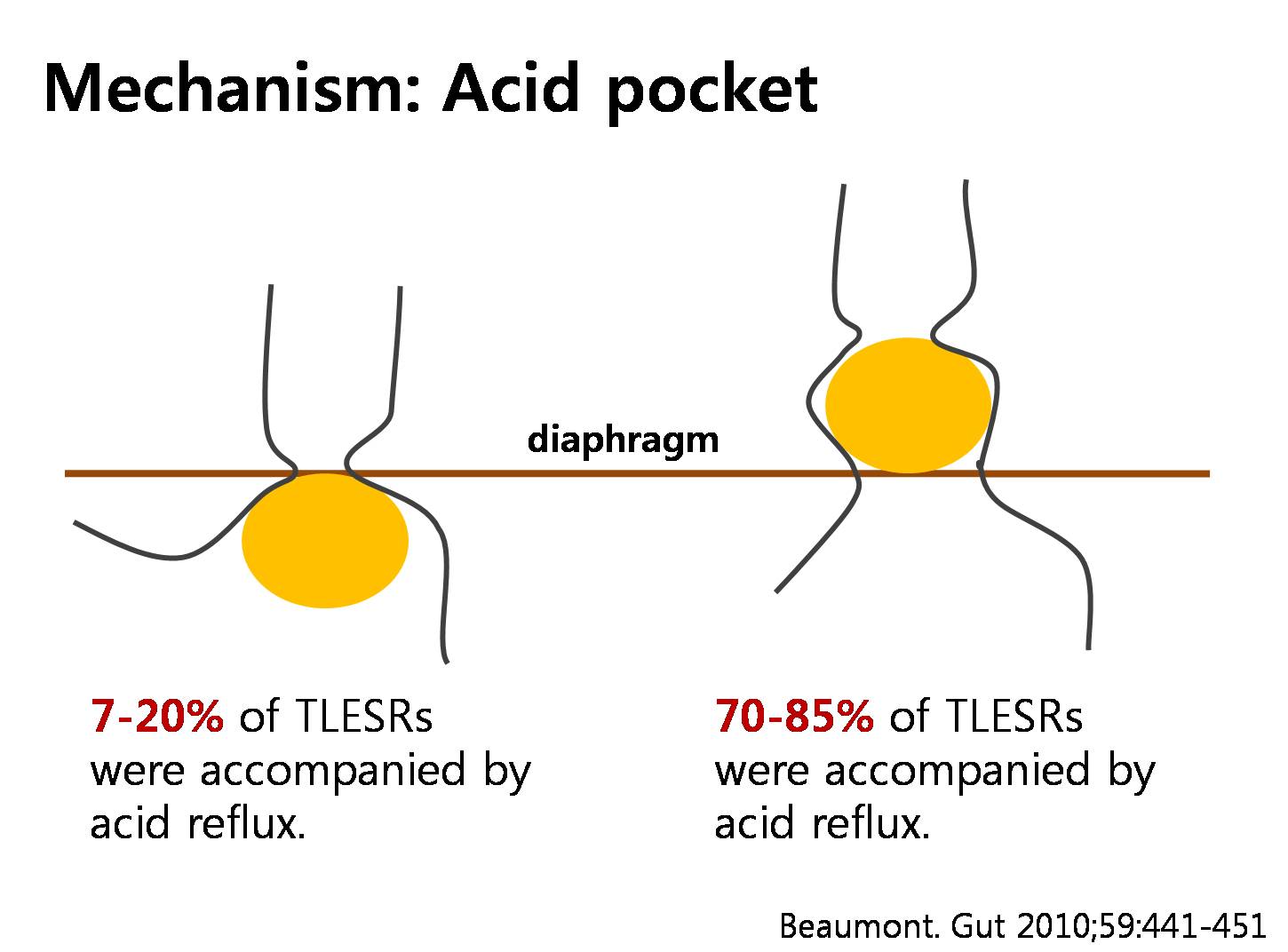
Recently, the recent concept of acid pocket also can explain the relationship between hiatal hernia and the development of the reflux symptoms.
* 참고: EndoTODAY 산주머니 (acid pocket)
![]() 11. Diaphragmatic eventration
11. Diaphragmatic eventration
The term ‘diaphragmatic eventration’ is used in common practice to describe a condition of relaxation of the diaphragmatic dome. It may present at birth as a congenital condition due to a defect of diaphragmatic development or in a later stage of life as an acquired condition (‘acquired diaphragmatic paralysis’ or ‘acquired diaphragmatic elevation’). (참고자료)
40대 후반 여성
- 식도: Squamocolumnar junction이 upper incisro 36cm 부위에 있음. 통상적인 경우보다 4-5cm 정도 상방임
- 위: SCJ 직하방부터 화면의 2 시 방향으로 위 lumen이 보임. 통상적으로 관찰되는 SCJ 직하방의 9시 방향에서 보이는 fundus가 보이지 않음. 따라서 SCJ 직하방부터 fundus, 위체부로 이어지는 양상임. Antrum으로 들어가는 길이 매우 길고 휘어 있음. Pyloric ring 근처까지 접근하였으나 내시경 scope가 긴 loop을 형성하면서 duodenum에 들어갈 길이가 모자람. 공기를 빼고 loop를 풀기 위하여 여러번 시도하였으나 공기를 빼면 시야가 확보되지 않고 공기를 넣으면 loop 때문에 pyloric ring을 통과할 수 없었음. 위점막 병소는 없음.
- 십이지장: 관찰할 수 없음
- 결론 및 진단: Diaphragm eventration 환자이나 식도와 위의 점막병소는 없음. 십이지장은 들어갈 수 없었음
[2016-6-10. 애독자 편지]
위대(大) 하신 분들이나, 수술(주로 wedge resection)이나 과거 궤양으로 인하여 내시경이 shortening 이 힘들거나, 유문부에서 진입이 잘 안되는 경우에는 cap을 씌우고 들어가면 공기를 전혀 송기하지 않고 들어갔던 적이 있습니다.
[2016-6-12. 애독자 편지]
저의 경우에는 전정부에 이를 때 쯤 루푸가 심하게 형성되어 진입이 힘들것으로 판단되면, 공기를 최대한 흡기해서 내강의 방향만 보일 정도로 흡기하면서, 체상부 까지 내시경을 무르고 대장내시경 같이 배꼽 좌측이나 배꼽 근처를 압박하고 압박된 손을 지렛대로 진입 하면서부터 실패하지 않았던 것 같습니다.
![]() 12. Hiatal hernia 단상 - Hiatal hernia 무시하지 맙시다.
12. Hiatal hernia 단상 - Hiatal hernia 무시하지 맙시다.
Hiatal hernia는 중요하지 않습니다. Hiatal hernia는 중요합니다. 어느 쪽이 맞을까요?
Hiatal hernia는 중요하지 않다고 생각하는 사람이 많습니다. 중요한 것은 GERD 환자의 증상이지 내시경 소견이 아니라는 점에서 증상하고 관련성이 뚜렷하지 않은 hiatal hernia의 존재는 무시당하는 것이 현실입니다. 그러나 이는 hiatal hernia에 대한 합당한 대접이 아니라고 생각합니다.
(1) LA-C나 LA-D와 같은 심한 confluent erosive esophagitis는 대부분 현저한 hiatal hernia와 동반됩니다. (2) NERD 환자의 상당수도 hiatal hernia와 관련이 있습니다. (3) 중증의 Barrett esophagus는 대부분 hiatal hernia와 관련이 있습니다. (4) Paraesophageal hernia와 동반된 반복출혈을 보이는 환자도 있습니다. Hiatal hernia가 출혈의 원인임을 모른다면 진단이 되지 않겠지요. 사실 그런 환자가 많습니다. 그런데도 무시되고 있습니다. 황당한 일이 아닐 수 없습니다.
단지 표준화가 어렵고 inter-observer variation이 심하다는 이유로 hiatal hernia라는 중요한 entity가 완전히 무시되는 상황입니다. 서구식 사고입니다. 표준화가 되지 않으면 중요한 것도 무시하는 것이 서구인의 사고 방식입니다. 중요한지 안 중요한지 명확하지 않아도 일단 보이는 것은 나름대로 기술하고 의미를 찾아보자는 것이 옳지 않을까요. 우리는 지나치게 서구 방식만 따르다 보니 스스로 장님이 되어 보이는 것도 기술하지 못하는 경우를 만든 것입니다. Hiatal hernia 공부를 권합니다.
![]() 13. [2017-2-19. 중앙 선데이] 위식도 역류 증상엔 식도곁탈장 의심을
13. [2017-2-19. 중앙 선데이] 위식도 역류 증상엔 식도곁탈장 의심을
어떤 일간지 일요일판에 paraesophageal hernia에 대한 기사가 실렸습니다. 그런데 흥미롭게도 기사를 쓰신 분이 가톨릭대 서울성모병원 위장관외과 교수 이한홍 선생님입니다. '객원 의학전문기자'라는 타이틀을 가지고 계셨습니다. Paraesophageal hernia를 '식도곁탈장'이라는 용어로 설명하시면서 수술적 치료를 소개하셨습니다. 내과적 치료가 너무 가볍게 다뤄진 점이 없지는 않았지만... 여하튼 기사를 옮깁니다.

최근 들어 소화불량이 심해진 정모(76·여)씨는 식사 때마다 음식을 삼키기가 힘들어 곤혹스럽다. 처음엔 체한 줄 알고 음식을 먹지 않다가 좀 나은 것 같으면 다시 먹곤 했다. 그런데 소화불량은 나아지질 않고 한 번 생기면 3~4일은 계속 식사를 하기 힘들었다. 증상이 계속 반복되다 보니 체중도 줄었다. 그러다 음식을 삼키기 힘들어 이틀 정도 금식했더니 어지럽고 토하는 증상까지 생겨 급히 응급실을 찾았다. 복부CT 검사 결과 복강(배 안)에 있어야 할 위의 대부분이 흉강(가슴 안)으로 딸려 들어가 있는 것으로 나타났다. 식도곁탈장이란 진단을 받은 정씨는 혈액 검사에서 식이 부족으로 인한 철 결핍성 빈혈도 발견됐다. 정씨는 복강경을 이용해 탈장된 부위를 원상태로 되돌리는 식도곁탈장 수복술과 식도 하부조임근을 보완하는 위기저부 주름술을 받았다. 수술을 받은 뒤 정씨는 별다른 합병증 없이 퇴원해 식사하는 데 문제가 없을 만큼 회복했다.
식도곁탈장은 위식도 역류 증상을 일으키는 주요 질환의 하나다. 위식도 역류는 위산이나 위 속의 내용물이 식도로 역류하는 증상을 말한다. 여러 가지 이유로 위식도 경계 부위의 구조가 파괴되면 흉강과 복강을 구분하는 횡격막(가로막)의 각근육(脚筋肉) 사이가 벌어지면서 틈새가 생긴다. 각근육은 횡격막 가운데 구멍을 이루는 근육이다. 식도곁탈장은 벌어진 공간을 통해 복강 내 장기 중 주로 위가 식도 옆 흉강으로 딸려 들어가는 현상을 말한다. 초기에는 증상이 없는 경우도 많다. 하지만 탈장의 정도가 심해지면 소화불량이나 위산 역류 같은 증상이 나타나고, 딸려들어가는 복강 내 장기의 양이 많아지면서 구토 같은 심한 증상이 생긴다. 흉강으로 탈장하는 공간이 증가하면 호흡 곤란도 생길 수 있지만 흔하지는 않다.
식도곁탈장이 생기는 원인은 지속적인 과식 등으로 위 용적이 팽창하면서 위식도 경계 부위의 구조가 파괴되고 횡격막부위(각근육)가 벌어지는 것이 대표적이다. 호흡을 하면서 흉부와 복부는 압력차가 일어나는데, 벌어진 횡격막 부위로 위가 딸려 올라가면서 식도곁탈장이 시작된다. 횡격막 근육의 노화도 원인이 될 수 있다. 그래서 식도곁탈장은 대부분 노년기에 생긴다. 간혹 자주 과식하고 과다 체중이면 젊은 연령이라도 생길 수 있다. 소화불량이 계속되고 위산 역류가 있으면서 간헐적인 구토가 있고 구토한 뒤 증상이 나아진다면 식도곁탈장을 의심해야 한다. 만성적이면서 간헐적으로 발생하는 식도곁탈장은 심한 증상은 없더라도 음식을 많이 섭취하기 어렵기 때문에 식이 섭취부족으로 철 결핍성 빈혈 등도 나타날 수 있다.
김모(63·남)씨는 위식도 역류 증상이 계속돼 집 근처 병원에서 내시경 검사를 받았다. 식도곁탈장으로 진단을 받았지만 탈장의 크기가 작고 역류 말고는 다른 증상이 없었다. 약물치료를 권유받아 양성자 펌프억제제를 복용했더니 증상이 나아져 계속 약물치료를 받았다. 하지만 한 번이라도 약 먹는 것을 건너뛰면 역류 증상이 어김없이 나타나 일상생활이 힘들었다. 약물 복용량도 점차 증가하게 되자 김씨는 수술을 받기로 결심했다. 복강경으로 식도곁탈장 수복술과 위기저부 주름술을 받은 김씨는 수술 이후 역류 증상이 없어지고 약물 치료도 중단했다. 식도곁탈장은 내시경검사·위조영제검사·CT검사 등의 결과를 확인해 진단한다. 증상이 심할 경우 간단한 흉부 촬영으로 흉부의 장 내 공기 음영 상태를 보고 진단하기도 한다. 하지만 치료를 진행하려면 탈장의 정도나 탈장낭 내 복부 장기 등을 확인하기 위해 흉부 촬영 외 다른 검사 결과도 참고해야 한다. CT검사는 제공하는 정보가 많아 수술 전 계획을 세우기에 가장 유용하다.
증상이 미미하거나 나타나는 빈도가 뜸 할 때는 주의 깊게 관찰하기도 하지만 증상이 악화되고 잦아지면 즉시 치료를 시작하는 게 좋다. 약물 치료는 위산 역류 증상만 일시적으로 완화시킬 수 있지만 식도곁탈장은 복부 장기의 해부학적 구조가 변화된 것이기 때문에 근본적으로 치료되지는 않는다. 해부학적 구조를 원상 복구시키고 재발을 방지하려면 수술을 받아야 한다.
최근에는 흉터가 거의 남지 않는 복강경 수술을 주로 하는 편이다. 수술은 복강으로 수술 기구를 넣어 흉강으로 올라간 장기를 복강으로 되돌려놓고 복강 장기가 흉강으로 올라가면서 생긴 탈장낭을 제거하는 과정으로 진행한다. 이후 벌어진 횡격막 부위를 좁혀주고 재발과 위산 역류를 방지하는 목적으로 위기저부 주름술을 시행한다. 수술 직후 정상화된 복부 장기의 위치를 조영제 검사 등으로 확인하고 식사를 하게 된다. 대개 수술을 받고 나서 3일 뒤 퇴원한다. 1년에 한 번 정도 추적 검사로 내시경이나 CT검사를 하기도 하지만 증상이 재발되지 않았다면 반드시 할 필요는 없다. 간혹 고령이라 수술을 망설이는 경우가 있는데 소화기관을 절제하는 수술이 아니고 복강경 수술이라 고령 환자에게도 비교적 안전한 수술법이다. 수술 후 금식과 입원 기간이 길지 않아 증상이 심하다면 수술을 받는 편이 건강에 도움이 된다.
![]() [FAQ]
[FAQ]
[2016-8-30. 애독자 질문]
Paraesophageal hernia 같은데 정확히 기술하기가 어려웠습니다. 그리고 type 분류는 어떻게 하는 것이 좋을까요?
[2016-8-30. 이준행 답변]
Type 2 식도주위탈장(paraesophageal hernia)은 횡격막식도 인대의 손상은 없고, 열공 자체가 늘어나서 그 틈으로 위의 일부(특히 위분문부)가 흉강으로 빠져 들어가는 형식의 탈장을 말합니다. Gastroesophageal junction이 diaphragmatic orfice와 같은 level, 즉 정상 높이에 위치하고 있습니다. 매우 드문 형태입니다. 책에서는 hiatal hernia의 2% 정도라고 합니다만 사실 저는 거의 본 적이 없습니다.
전형적인 type 2 paraesophageal hernia
우리가 흔히 paraesophageal hernia라고 말하는 것은 대부분 type 3입니다. 보내주신 증례도 type 3 hernia입니다.
상세한 기술은 아래 그림을 참고하세요.
[2017-6-8. 애독자 질문]
EG junction에 대한 이해가 부족하여 질문드립니다. 식도 말단부위 해부학을 찾아보니 구글에서 다음과 같은 그림을 찾았습니다.

LES가 식도 distal 부위 횡축에 길게 선상으로 걸쳐있으며 그 범위안에 A,B,C 링이 있는데 A링은 구체적으로 muscularis ring(=inf.esophageal sphincter), B링은 mucosal ring(=SC junction), C링은 diaphragmatic orifice로 이해하면 될까요?
구체적으로 EG junction이 어느 부위인지 그리고 SC jungtion 관계는 어떻게되는지 혼란스럽습니다.
[2017-6-8. 이준행 답변 질문]
보내주신 그림 중 첫번째 그림은 참고할만 하지만, 두번째 그림은 매우 엉터리입니다. 잊어버리시기 바랍니다. 차라리 제가 그린 그림을 보시면 좋겠습니다.
LES는 식도 circular muscle이 하부식도에서 3cm 길이 정도 두꺼워진 것입니다. 정상적인 경우 LES 말단과, squamocolumnar junction과 EG junction은 거의 일치합니다.
C ring은 잘 쓰는 말이 아닌데요... 선생님이 보내주신 첫번째 그림을 보니 diaphragmatic orfice를 지칭하는 것 같습니다. "LES가 식도 distal 부위 횡축에 길게 선상으로 걸쳐있으며 그 범위안에 A,B,C 링이 있는데" 부분은 질문하신 선생님께서 완전히 잘 못 알고 계신 것이니 잊어버리세요. LES는 A ring과 B ring 사이이고 C ring과는 전혀 무관합니다.
보다 상세한 내용은 제가 YouTube에 올린 강의 동영상을 참고하시기 바랍니다. 17:00 부터 27:30 사이입니다.
[2020-8-18. 애독자 질문]
위내시경 시 fundus가 매우 길게 or 깊게 보인 경우 hernia나 병변 가능성이 있겠습니까?
[2020-8-18. 이준행 답변]
일단 EG junction (tubular esophagus와 saccular stomach의 경계)을 잘 살피십시오. 특히 squamocolumnar junction과 hiatal opening의 위치관계를 검토하면 sliding type의 hiatal hernia가 있는지 알 수 있습니다.
그 다음 hiatal opening이 넓은지 좁은지 모고 이것이 넓으면서 이 곳으로 위의 일부가 parallel한 주름을 만들면서 언덕을 넘어가는 모습이 보이면 paraesophageal hernia가 있는 것입니다.
이러한 소견 없이 그냥 fundus가 길고 깊어 보이면 normal variant일 가능성이 더 높습니다. 키가 큰 사람이 있고 작은 사람이 있는 것처럼 위도 긴 사람이 있습니다. 과거에는 위가 길고 처져 있으면 위하수라고 불렀는데요... 요즘은 의미없는 소견이라고 생각하여 위하수라는 진단명은 사용하지 않고 있습니다.
![]() [References]
[References]
1) EndoTODAY Aacid pocket 산주머니
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.


{kind=link}