Previous | Home | EndoTODAY | List | Next
![]() [Colonoscopy with cap & injection for polypectomy] - 終
[Colonoscopy with cap & injection for polypectomy] - 終
아래는 오래 전 논의입니다. 2025년 현재 대장내시경 시 투명 cap을 사용하는 것은 보편적으로 받아들여지고 있습니다.
[2013-9-16. 애독자 질문] 저는 내과 수련 후 공부의 생활을 하며 내시경을 배우고 따로 fellow 과정을 거치지 않은 상태로 local 에서 위, 대장 내시경을 하고 있습니다. 처음 배우는 과정부터 cap (long cap, 직경 1cm정도)을 사용하는 대장내시경을 익히게 되었고, 현재까지도 cap을 사용하여 검사하고 있습니다. 이런 방식에만 익숙해지다 보니 cap없는 검사를 시도하지 않았고, 할 수도 없는 상황이 되었습니다. 일반적인 방식과 다르다 보니 그에 따른 불편감 및 불안감이 있습다. Cap 사용 검사에 대해 선생님은 어떻게 생각하시는지요?
또 한가지는 snare를 이용한 용종절제술을 배우는 과정에서 대부분 saline 및 epinephrine을 이용한 injection을 시행하지 않고 바로 snare polypectomy를 해왔습니다. 그게 전부인 줄 알았는데 연수강좌 등을 통해서 또는 소화기내과 fellow를 하는 친구들을 통해 물어보면 당연히 injection을 이용한 lifting 후 snare polypectomy를 시행하는 것 같습니다. 제 스승님은 굳이 그렇게 하지 않아도 천공 등의 위험성에 큰 차이는 없는 것 같다고 하시는데... 선생님께서는 이 부분에 대해 어떻게 생각하시는지요?
![]() [2013-9-16. 전문가 (S대 교수) 답변]
[2013-9-16. 전문가 (S대 교수) 답변]
질문을 읽고 "배운다는 것이 참 중요하구나"라는 것을 느꼈습니다. 저는 반대로 캡을 안 씌우는 대장 내시경을 배웠고, 용종 절제술에는 submucosal injection을 안하면 반드시 구멍나는 줄 알았습니다. 이후에 캡을 씌우고 하는 것이 구석구석 보는 데 도움이 된다는 것도 알 수 있었고 (ASGE에서 용종 발견에 도움이 된다는 리포트가 있습니다) 치료내시경에서는 반드시 씌우고 들어가는 편입니다. 개인적 의견으로는 캡을 씌우고 하는 방법은 단점보다 장점이 많은 것 같습니다. 굳이 다른 방법으로 바꿀 필요는 없을 것 같습니다.
용종제거술의 submucosal injection 역시 근처 대형병원에서도 그리 열심히 시행하지 않는 것으로 알고 있습니다. 저와 같은 트레이닝을 받았던 분께서 보시고는 ‘야 여기 구멍이 좀 나겠구나’ 했었는데... 실은 그렇지 않다는 것입니다. 물론 이러한 사실이 객관적으로 입증된 것은 아닙니다. 합병증이란 구멍 뿐 아니라, post polyectomy coagulation syndrome, 출혈 등도 있을 수 있기 때문에 자세한 검증이 필요하지 않을까 생각합니다. 참고로 분당서울대 및 다른 병원에서 다음과 같은 논문이 있었습니다. 따라서, 적어도 좀 크거나 납작한 놈들은 submucosal injection 하는 것이 좋을 것 같습니다.
참고문헌 1 (분당서울대병원): Submucosal saline-epinephrine injection in colon polypectomy: appropriate indication
BACKGROUND/AIMS: Opinions vary among endoscopists concerning the indications for submucosal saline-epinephrine injection for the prevention of postpolypectomy complications after colonic snare polypectomy. This study was performed to determine the appropriate indications for submucosal saline-epinephrine injection.
METHODOLOGY: Clinical characteristics and complications (hemorrhage and perforation) in polypectomies were retrospectively evaluated. Postpolypectomy complications were analyzed in terms of demographic characteristics (age, gender), polyp characteristics (size, configuration, location, and histopathology), and the administration of submucosal saline-epinephrine injection.
RESULTS: Total 1039 polypectomies were performed in 563 patients (age 59.8 +/- 10.1 years), and submucosal saline-epinephrine injection was performed in 679 polypectomies. Twenty seven episodes (2.6%) of hemorrhage and 3 cases (0.2%) of perforation occurred. Malignant adenoma, a rectal polyp, and procedure without submucosal saline-epinephrine injection increased the risk of hemorrhage with odds ratios of 10.48, 4.71, and 3.44, respectively. Furthermore, submucosal saline-epinephrine injection significantly reduced the risk of hemorrhage in sessile polyps and those > 8 mm in size and with odds ratio of 16.41 regardless of location or histopathology. The occurrence of postpolypectomy perforation was not associated with any clinical characteristics and method.
CONCLUSIONS: Submucosal saline-epinephrine injection should be performed for sessile polyps and those > 8 mm in size, and might be performed optionally in other cases to prevent postpolypectomy hemorrhage.
참고문헌 2 (타이완 논문): Is submucosal epinephrine injection necessary before polypectomy? A prospective, comparative study.
BACKGROUND/AIMS: Polyps of the gastrointestinal tract are usually removed due to their link to bleeding, obstruction and malignancy. However, complications may occur following polypectomy. The aim of this study was to assess whether submucosal epinephrine injection before polypectomy could reduce the incidence of bleeding and perforation.
METHODOLOGY: Between June 1997 and November 1999, patients with sessile polyps of the gastrointestinal tract found in our endoscopic unit were randomized to receive submucosal epinephrine injection (epinephrine group) or no injection (control group) before polypectomy. In the epinephrine group, epinephrine (1:10,000) was injected surrounding the stalk of the polyp until the mucosa was blanched and bulged. The patients were observed for complications in the following month.
RESULTS: A total of 120 patients with 151 sessile polyps were enrolled in this study. In the epinephrine group, 75 polyps (n = 68) were randomized to receive epinephrine injection before polypectomy. In the control group, 76 polyps (n = 61) underwent polypectomy without epinephrine injection. In both groups, there was no significant difference in clinical features including the sizes of the polyps and their stalks, the location of polyps and the pathological diagnosis. There were a total of nine episodes of post-polypectomy hemorrhage, two in the epinephrine group and seven in the control group (2/75 vs. 7/76) (P = 0.07). One case in the epinephrine group experienced delayed bleeding (4 days later). Immediate hemorrhage occurred less in the epinephrine group than that in the control group (1/75 vs. 7/76, P = 0.03). There was one case of perforation in each group.
CONCLUSIONS: Epinephrine injection prior to polypectomy is effective in preventing immediate bleeding
![]() [2013-9-16. 전문가 (C대 교수) 답변]
[2013-9-16. 전문가 (C대 교수) 답변]
1. 대장내시경 때 cap을 계속 사용하는 문제
- 다른 개원의선생님들도 그런 분이 있어 큰 문제 없을 것 같습니다.
- 대장 용종 발견도 잘 할 수 있다는 강점도 있고,, (한 문헌에 의하면) 길 찾기도 쉬워 빨리 한다는 얘기를 들은 적이 있습니다.
- 저는 개인적으로 캡을 사용하지 않고 있고, 산부인과 수술을 받았던 분 등 OP Hx가 있는 환자에게 제한적으로 사용하고 있습니다.
- 계속 사용해도 큰 문제는 없을 것 같지만, 사용하길 원치 않으신다면, 검사가 쉬워 보이는 분들 (체형을 보면 대충 짐작이 가능하시죠? 수술 병력 없는 마르지 않은 적당한 체격의 남자) 에게 캡 없이 검사를 해 보시면 차츰 차츰 캡 없이도 충분히 할 수 있을 것 같습니다. 물론, 수술 병력이 있거나 어려워 보이는 케이스는 캡을 계속 사용하시는 것도 문제 없겠습니다.
2. EMR 과 Snare polypectomy 에 대해: 저도 개인적으로 EMR(Saline injection 후에 snaring) 로 하고 있습니다. 물론 현재 용종 하나 절제했을 때 수가는 못 받고 있지만요...두 방법에 대한 study가 없어서 보험에 적용을 못받고 있다고 알고 있습니다. 작은 용종에 대해서는 큰 차이가 없다고 생각합니다. 그러나, 어느 정도 크기가 있는 (예를 들면, 1cm 이상, 근거는 없습니다.) 용종 절제술에 대해서는 얘기가 다르다고 생각합니다. 용종절제술 할 때 EMR로 saline injection 을 한 후 suction 을 한 상태에서 snaring을 정상점막까지 해야 lateral margin이 혹시 남을 수도 있는 부분을 방지할 수 있습니다. 물론, ESD와 마찬가지로 saline injection이 잘 되면 천공등의 합병증을 줄일 수 있다고 생각합니다. Saline으로 점막하 주입하는 것이 육안적 완전절제를 도와준다는 것입니다. 천공등의 합병증도 방지할 수 있습니다. 결론적으로, 큰 크기에 대해선 EMR method가 완전절제을 할 수 있고, 천공의 합병증도 줄일 수 있다고 생각합니다.
![]() [2013-9-16. 전문가 (K대 교수) 답변]
[2013-9-16. 전문가 (K대 교수) 답변]
Cap을 이용한 대장내시경이 더 유리하며 권장해야 한다고 생각합니다. 직장에서의 J턴을 통한 관찰이 어려운 경우에만, cap을 빼고 재삽입을 하여 관찰하면 될 것 같고 그 정도의 수고는 감수할 수 있을 것 같습니다. Cap을 사용하는 데 따르는 추가적인 비용을 산정할 수 없고, 매 환자마다 cap을 바꾸고 세척/소독이 필요하다는 점을 제외하면 cap없이 대장내시경을 하는 경우에 비하여 용종의 발견율도 유리하고, 이어서 시행하는 용종절제술에도 보다 유리한 점이 많습니다. 저는 cap을 지속해서 사용하기를 권장합니다.
Cap사용을 꺼리는 이유가 궁금합니다. 간혹 장정결이 잘 되지 않아 cap내 이물질로 인해 방해를 받는 경우가 있지만 이 경우 장정결을 추가해서 대장내시경을 하는 것이 높은 수준의 대장내시경을 위해 필요한 과정이므로 추가로 장정결을 환자/보호자에게 설명하는 것이 바람직할 것입니다. Cap을 사용하면서 느끼는 불편감이 있으시겠지만, cap을 사용하지 않더라도 불편감이 있습니다.
두번째 질문에 대하여 대장내시경하 내시경치료에는 올가미로 점막하 용액 주입이 없이 시행하는 용종절제술과 점막하 용액을 주입하여 시행하는 점막절제술이 있고, 최근에는 내시경하 점막하박리술/점막하종양절제술 등이 있습니다. 종양의 모양/크기/위치에 따라 적절한 방법을 사용하여 종양을 제거하면 되겠습니다. 모든 술기에 따른 장/단점을 이해하고 많은 경험을 쌓은 후 적절한 적응증에 맞추어 적용하면 됩니다. 반드시 점막절제술을 시행하여야만 하는 것은 아닙니다.
그러나, 점막절제술이 용종절제술에 비하여 지혈용액과 점막하층에 쿠션을 만들어 주어 출혈이나 천공의 빈도가 다소 낮은 것 같습니다. 종양(용종)의 모양이 유경성(목을 가진 경우)에는 용종절제술이 보다 유리하고, 무경성중에서도 편평형( Yamada type I, Type Is)이나 lateral spreading tumor 의 경우에는 점막절제술을 시행하여야 할 것 같습니다. 다시 말하지만, 종양의 모양/크기/위치에 따라 내시경적 절제술의 방법을 선택하는 것이 바람직하겠으며, 근무하는 병원의 규모/외과의의 협진 정도 등을 고려하여 추가로 다른 시술이 필요하신 경우 충분한 교육과 연습을 하신 후에 시술에 임할 것을 권합니다. 자칫 섯부르게 환자에게 시술을 하는 것은 좋지 않다고 생각합니다. 또 자신의 실력 이상의 종양에 대하여 절제술을 어설프게 하기보다는 상급기관으로 전원하여 안전하고 확실한 치료가 될 수 있게 하는 것이 올바른 선택이라고 생각합니다.
![]() [2013-9-16. 전문가 (Y대 교수) 답변]
[2013-9-16. 전문가 (Y대 교수) 답변]
1. 대장내시경에서의 cap 사용: (1) Cap 을 장착하고 대장내시경을 시행하면 insertion time 을 단축시킬 수 있다는 보고들이 많이 있고, (2) Cap으로 인해 polyp 을 더 많이 찾을 수 있다는 일부 주장도 있지만, adenoma detection rate 를 높이지는 못한다는 주장도 있어서 이에 대해서는 논란이 있으며, (3) Cap 을 장착하고 대장내시경을 함으로 인해서 합병증이 높아진다는 근거도 없습니다. 따라서 Cap 을 장착하고 대장내시경을 하는 것에 잘못이 있다고 생각되지 않습니다. 하지만 1 cm 정도의 long cap의 경우에는, 제 경험 상 아무리 transparent cap 이라고 하더라도 플라스틱 cap 부위를 통해 비추어 보는 시야가 뿌옇게 보여서, 시야가 좋지 못하기 때문에 polyp 관찰에 오히려 약간 방해가 될 소지도 있다고 생각됩니다. 따라서 cap 의 길이를 조금씩 짧은 cap (예를 들면 4mm cap) 으로 바꾸어서 colonoscopy 시행하는 훈련을 한다면 좋을 듯 합니다. 그러면 추후 짧은 cap 또는 cap 없이 하는 대장내시경에 점차 적응을 할 수 있지 않을까 합니다.
2. Colon polypectomy시의 submucosal injection
1) Submucosal injection에 대해서는 장연구학회 가이드라인에서 언급하고 있는 바는 polypectomy 후 immediate bleeding을 줄일 수는 있지만 delayed bleeding에는 차이가 없다고 언급하고 있고, 천공율을 줄일 수 있다는 근거도 부족합니다
2) 대표적으로 신촌세브란스의 경우가 submucosal injection 없이 polypectomy 를 많이 하는 편인데 (대체로 1cm 이상에서만 injection 시행), 천공이나 출혈이 문제가 되는 경우는 많지 않습니다.
3) 개인적 의견은, 5mm 정도의 작은 용종은 injection 없이 polypecotmy 시행하여도 상관 없다고 생각됩니다.
4) 크기가 큰 용종일수록 snare 로 포획하는 점막의 면적이 넓어지게 되면서, 절제를 위한 electrical current burden이 증가하므로, post-polypectomy electrocoagulation syndrome 및 perforation risk 가 상승하기 때문에 크기가 조금 큰 용종에서는 당연히 submucosal injection 을 하는 것이 좋다고 생각합니다만, 몇 mm 크기부터 하는 것이 좋을지는 개인적 성향이라고 생각합니다. 저는 개인적으로 7-8 mm 정도 용종 부터는 submucosal injection을 시행한 후 용종절제술을 하고 있습니다.
![]() [2013-9-16. 전문가 (S대 교수) 답변]
[2013-9-16. 전문가 (S대 교수) 답변]
1. cap (long cap, 직경 1cm정도) assisted colonoscopy:
1) 궁금한 것이 어떤 종류의 cap사용하는 것입니다. long cap은 제게는 익숙하지 않은데 과거에 많이 사용하던 hard cap을 말하는 것인지요?
우선 저는 개인적으로 치료내시경에서 사용은 물론 진단 내시경에서도 cap의 긍적적인 면에 찬성합니다. 대장내시경에서 cap을 사용은 것은 초기에는 fold를 젖혀 뒤의 숨겨진 작은 polyp의 진단함으로 진단율을 상승시킬 수 있다는 가정으로, 최근에는 삽입을 수월하게 할 수 있다는 장점으로 많이 사용이 증가 하고 있습니다.
일부 cap을 사용하용에 희의를 보이는 내시경의사는 1개당 2만 4천원인가 하는 cap을 사용해야 하므로 경제적 이유 (물론 환자에게 fee를 물릴수는 없지만), 시야가 오히려 협소해지고 fecal material이 내시경에 걸려서 진단율이 떨어진다라는 것들을 문제시 하는 것으로 알고 있는 것으로 생각됩니다.
따라서, hard cap은 시야를 협소하게 만들기 때문에 좋지 않다고 생각하며(최근 olympus hard cap은 국내에서는 판매되지 않는 것으로 알고 있습니다), 흔히 구할 수 있는 판매하는 cap을 사용하는 것은 지속적인 사용하데에도 전 문제가 전혀 없다고 생각됩니다. 또한, cap을 사용하셔서 걱정이 되신다면 더욱더 천천히 회수하시고 6분 이상의 관찰 시간을 지키심이...좋겠습니다. )
2. CPP시 submucosal injection
흔히 injection을 안 하는 것을 polypectomy 방법이라고 하고, injection을 하는 것을 endosocpic submucosal resection (EMR)방법이라고 하기도 하지요. 아마도 injection없이 CPP하는 방법에 익숙하시다면, 말씀하신 것처럼 천공과 출혈과 같은 위험성은 injeciton에 안해도 크게 증가하 않을 것으로 생각됩니다. 또한, 출현 천공 자체가 매우 드문 합병증이기도 하구요. 저희가 0%가 될수 있도록 노력해야 하는 것이 아닐까 싶습니다. 기존 연구를 보면 injection을 하면 immediate and acute bleeding 과 같은 합병증이 낮은 것으로 되어 있습니다.
하지만, 제가 SM injection 을 모든 CPP에 권유하는 것은 합병증 예방 외에도 폴립의 완전절제를 위해서 입니다. SM injection 후 절제를 하는 것은 병변의 margin을 충분히 잡아 완전 절제가 높을 것이라고 확신합니다. 실제 injection 없이 절제하는 방법은 sessile polyp을 snare로 잡기가 쉽지 않으며 주변 정상 점막도 조금 함께 잡아 resecton margin free로 절제하려는 시도를 하기가 어렵기 때문임을 잘 아실 것입니다.
Sessile polyp의 잔존 조직은 interval cancer의 주요 요인임을 잘 알려져 있고, 내시경의사마다 CPP의 완전 절제율이 다름은 CARE study등을 통해 잘 알려져 있습니다.
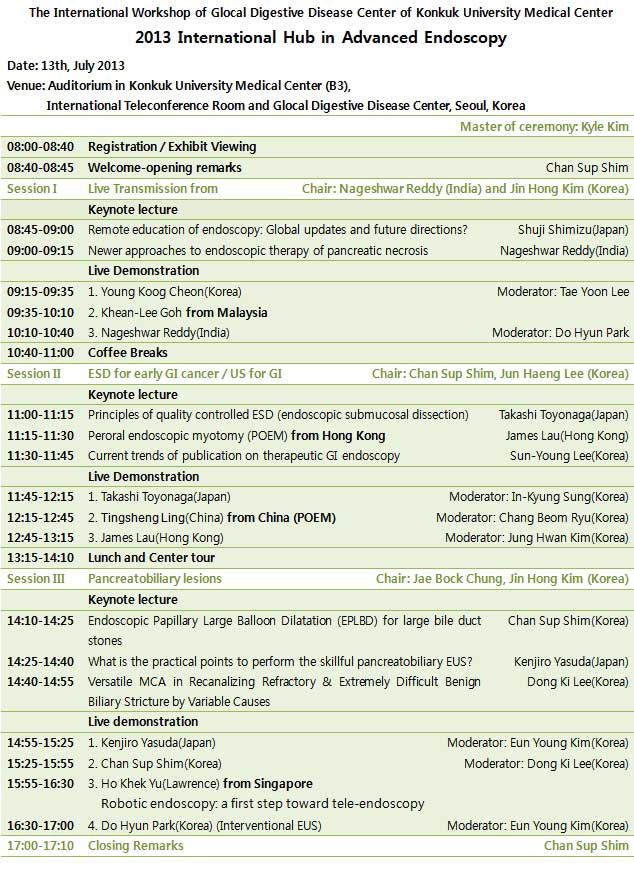
![]() [The International Workshop of Glocal Digestive Disease Center of Konkuk University Medical Center] - 2013 International Hub in Advanced Endoscopy
[The International Workshop of Glocal Digestive Disease Center of Konkuk University Medical Center] - 2013 International Hub in Advanced Endoscopy
Opening remarks by Professor Chan Sup Shim
Teleconference with Professor Khean-Lee Goh and his colleques in Malaysia
Live demonstration by Professor Nageshwar Reddy (India) at the Endoscopy Room of Konkuk University Hospital
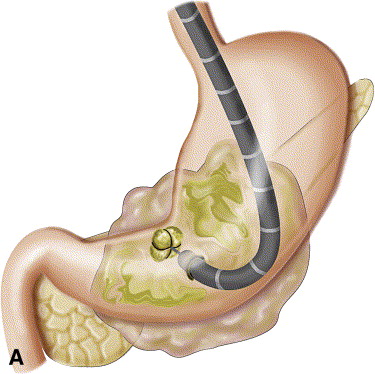
![]() Endoscopic transgastric pancreatic necrosectomy (Professor Nageshwar Reddy, India)
Endoscopic transgastric pancreatic necrosectomy (Professor Nageshwar Reddy, India)
Reddy 교수는 pancreas necrosis의 벽이 잘 maturation되면 위의 후벽을 통하여 pancreatic necrosectomy를 시행할 수 있음을 보여주었습니다. 교수님는 2012년 3월 JAMA에 수술과 endoscopic necrosectomy를 비교한 randomized study 결과도 소개하셨습니다 (Endoscopic Transgastric vs Surgical Necrosectomy for Infected Necrotizing Pancreatitis). JAMA 논문에서 소개된 시술방법 설명 그림와 결과 table을 아래에 옮깁니다.
Figure 1. Video-Assisted Retroperitoneal Debridement and Endoscopic Transgastric Necrosectomy - A, Cross-sectional view depicting an enlarged, partially necrotic pancreas with a peripancreatic collection containing fluid and necrosis. The preferred access route for video-assisted debridement is within the left retroperitoneal space to reach the necrotic collection between the left kidney and descending colon. A laparoscope is inserted, and long grasping forceps are used to debride the necrosis. B, The access route for natural orifice transluminal endoscopic surgery is through the posterior wall of the stomach. The necrotic collection most often bulges into the stomach facilitating endoscopic transgastric necrosectomy. After balloon dilatation of the puncture site in the stomach wall, the endoscope is introduced into the retroperitoneal space and loose necrotic material is removed.
Results: We randomized 22 patients, 2 of whom did not undergo necrosectomy following percutaneous catheter drainage and could not be analyzed for the primary end point. Endoscopic transgastric necrosectomy reduced the postprocedural IL-6 levels compared with surgical necrosectomy (P = .004). The composite clinical end point occurred less often after endoscopic necrosectomy (20% vs 80%; risk difference [RD], 0.60; 95% CI, 0.16-0.80; P = .03). Endoscopic necrosectomy did not cause new-onset multiple organ failure (0% vs 50%, RD, 0.50; 95% CI, 0.12-0.76; P = .03) and reduced the number of pancreatic fistulas (10% vs 70%; RD, 0.60; 95% CI, 0.17-0.81; P = .02).
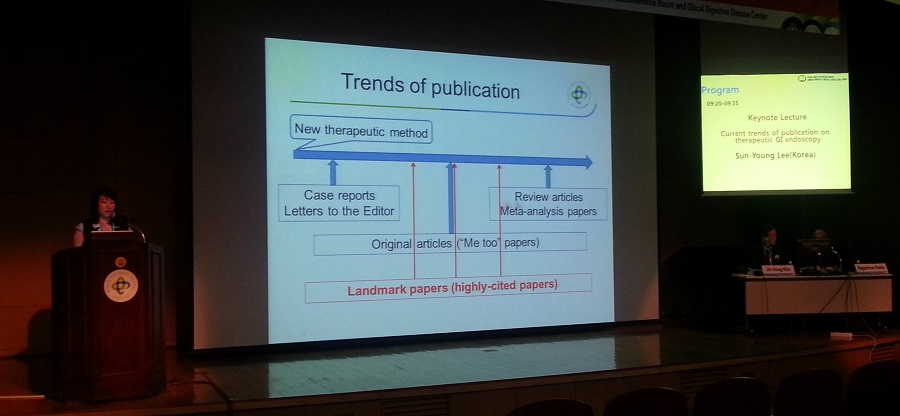
![]() Current trends of publication in therapeutic GI endoscopy (Professor Sun-Young Lee, Konkuk University, Seoul, Korea)
Current trends of publication in therapeutic GI endoscopy (Professor Sun-Young Lee, Konkuk University, Seoul, Korea)
이선영 교수님에 의하면 2000년부터 2012년까지 ESD에 대하여 1,848개의 영문 논문이 PubMed에 등재되었습니다. ESD에 대한 논문이 가장 많이 실린 저널은 Gastrointestinal Endoscopy였고 (26.9%), 다음이 Journal of Gastroenterology and Hepatology였습니다. 이선영 교수님의 결론 슬라이드를 아래에 옮깁니다.
Publications tend to increase when; (1) therapeutic endoscopy is for common diseases, (2) technique is easy to perform, (3) published papers are from various countries, and (4) papers are published in various journals. These will lead to future review articles, multicenter studies, and meta-analysis papers. This will further increase in publications and citations on this issue.
![]() Principles of quality controlled ESD (Professor Takashi Toyonaga, Kobe University Hospital, Japan)
Principles of quality controlled ESD (Professor Takashi Toyonaga, Kobe University Hospital, Japan)
Toyonaga 선생님의 강의는 2013년 7월 7일 부울경 세미나의에서 연세대학교 강남세브란스병원 윤영훈 교수님 강의와 관련된 내용이었습니다. 안전한 ESD를 위해서는 피가 나지 않을 곳(avascular stratum just above the muscle layer)을 조심스럽게 dissection하는 것이 요점입니다. 강의 abstract의 일부를 아래에 옮깁니다.
"For safe and reproducible procedure of ESD, the appropriate dissection of the ramified vascular network in the level of middle submucosal layer is required to reach the avascular stratum just above the muscle layer. The horizontal approach to maintain the appropriate depth for dissection beneath the vascular network enables treatment of difficult cases with large vessels and severe fibrosis. The most important aspact of ESD is the precise evaluation of curability. This approach can also secure the quality of the resected specimen with enough depth of the submucosal layer."
Toyonaga 선생님께서 일전에 대한소화기학회의 영문저널에 기고한 논문 Principles of quality controlled ESD with appropriate dissection level and high quality resected specimen. Clin Endosc 2012;45:362-74를 읽어보시기 바랍니다.

The difference of the density of vessels. (A) The extremely characteristic muscle layers named the oblique muscle layers are symmetrically seen in the anterior/posterior regions of the gastric body. The muscle layer is circularly absent at the inlet of the large vessel. (B) The density and thickness of the vessels in the gastric antrum overwhelmingly differs from those in the gastric body. (Ba) In the antrum, the density of vessel in the submucosal layer is low, and the fibrosis is also minimal, and these allow easy mucosal incision and submucosal dissection. (Bb) In the lesser curvature of the gastric body where the oblique muscle layers exist, as the blood vessels do not diverge frequently and the density of blood vessels are low as in the gastric antrum, the procedure is rather easy if the large penetrating vessels are not hurt by mistake. (Bc) On the other hand, in the anterior/posterior walls of the gastric body, where the oblique muscle layers exist, the greater curvature of the gastric body and lower rectum, the density of blood vessels is high and the diverged vessel network is inevitably hurt, if careful attention is not paid to the depth of mucosal incision and submucosal dissection. (Image and text from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3521937)
![]() [References]
[References]
1) EndoTODAY 코드
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.