 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Final posting of EndoTODAY Weekly - The initial biopsy of an AGC may be high grade dysplasia]
[Final posting of EndoTODAY Weekly - The initial biopsy of an AGC may be high grade dysplasia]
A patient was referred with a biopsy result of adenoma with high grade dysplasia.
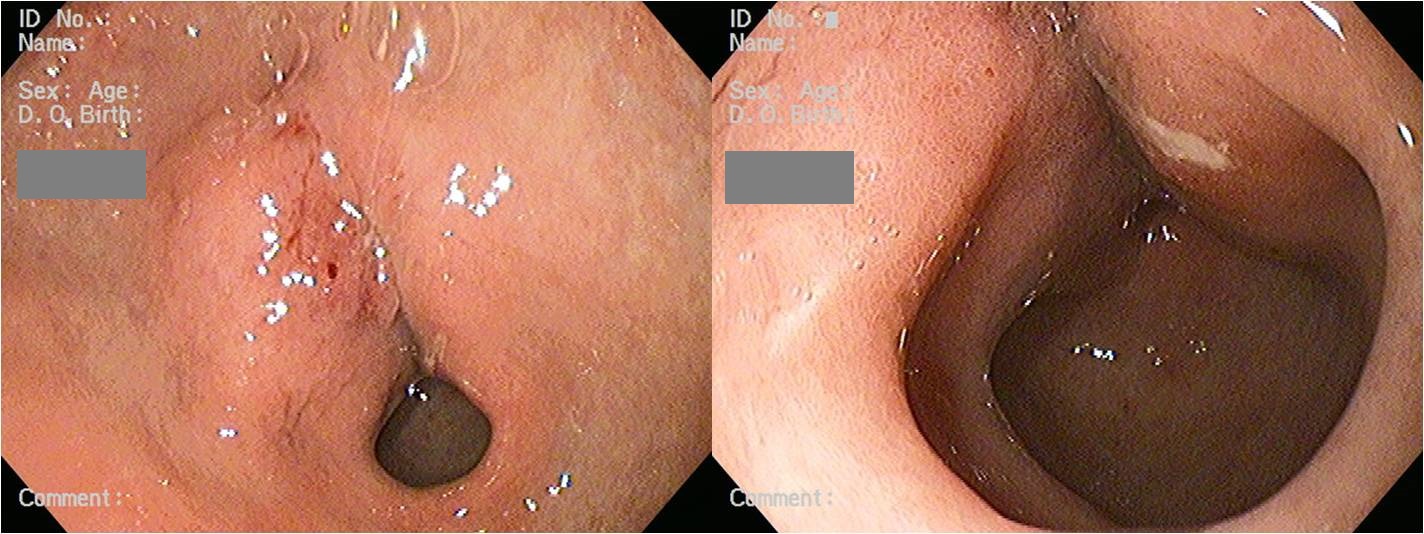
The lesion was located at the lesser curvature side of the distal antrum. The antrum was not fully expanded, so I decided to repeat the endoscopy. An ulcerative area was found in the repeat endoscopy, and malignancy was confirmed in the biopsy. Surgery was done, and the final pathological staging was T3N1.
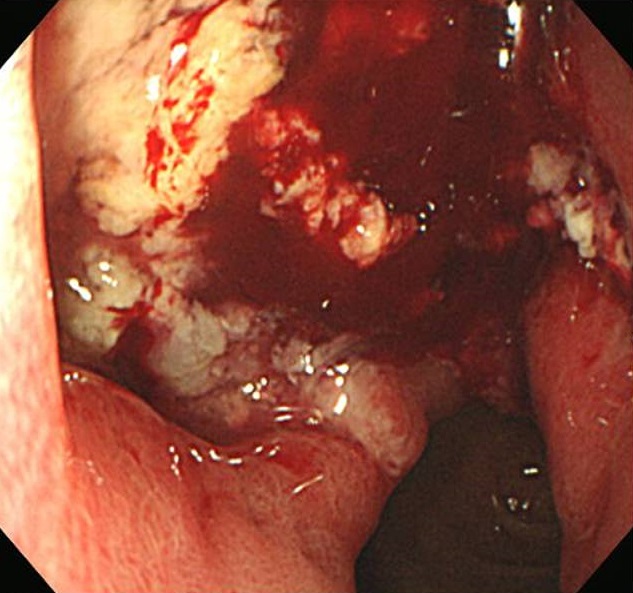
Advanced gastric carcinoma
1. Location : lower third, center at antrum and lesser curvature
2. Gross type : Borrmann type 3
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size : 2.7x2 cm
6. Depth of invasion : penetrates subserosal connective tissue (pT3)
7. Resection margin: free from carcinoma, safety margin: proximal 4 cm, distal 1 cm
8. Lymph node metastasis : metastasis to 2 out of 50 regional lymph nodes (pN1), perinodal extension: absent, (2/50: "1", 0/0; "3", 0/9; "4", 0/17; "4sb", 0/1; "5", 0/1; "6", 1/7; "8a", 0/4; "7", 1/4; "9", 0/5; "11p", 0/1; "12a", 0/1)
9. Lymphatic invasion : present
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. Peritoneal cytology : negative
13. AJCC stage by 7th edition: pT3, N1
![]() [Proceduralist가 되지 맙시다]
[Proceduralist가 되지 맙시다]
미국 소화기학회에서 발행하는 GI & Hepatoogy News에 Should gastroenterologists be accountable for preventing CRC?라는 흥미로운 기사를 소개합니다 미국 대장내시경 전문가들은 자기 환자를 검사하기보다는 누군가로부터 의뢰받아 검사하는 입장인 것 같습니다. Proceduralist라는 용어까지 있는 모양입니다. 기사의 요지는 무신경하게 다른 의사의 요청대로 검사하기 보다는 주인의식을 갖고 환자에게, population에게 최선이 되는 solution을 찾아가자는 것이었습니다. 마음에 와 닿는 문구를 소개합니다. Focusing on quality over quantity라는 소제목이 달린 문장의 시작 부분입니다. "More colonoscopies do not necessarily equal better outcomes." 그렇습니다. 검사를 많이 한다고 꼭 좋은 것은 아닙니다.
![]()