EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [2014 International Hub in Advanced Endoscopy]
[2014 International Hub in Advanced Endoscopy]
건국대학교 병원의 국제소화기심포지엄(2014 International Hub in Advanced Endoscopy)에 강의차 다녀왔습니다. 올해도 알차게 준비된 행사였습니다.
![]() 1. Update indications of ESD for gastric neoplasm (Takashi Toyonaga, Kobe University)
1. Update indications of ESD for gastric neoplasm (Takashi Toyonaga, Kobe University)
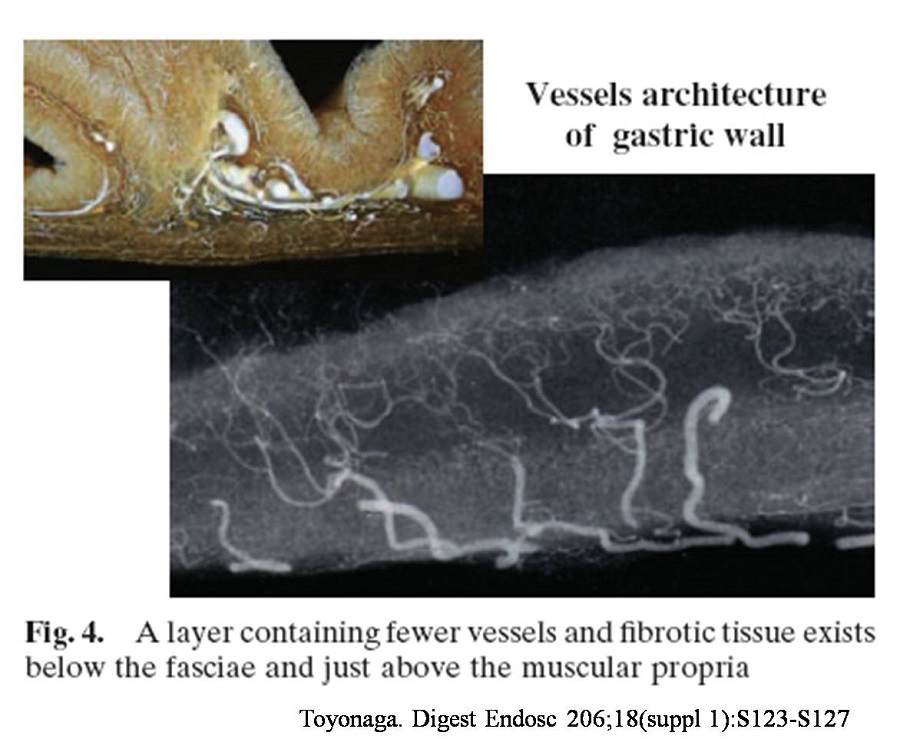
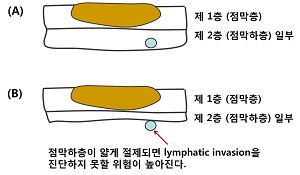
Vessel architecture를 고려하여, 즉 deep SM layer를 절제해야 출혈이 적다는 점 뿐만 아니라 병리결과의 정확한 판정을 위해서도 deep SM layer를 치료해야 한다. 예를 들어 이런 점막암인데 점막하층에 lymphatic invasion이 있다면, 점막하층을 어느 정도 깊게 치료했는가에 따라 병리결과가 정확할 수도 있도 부정확할 수도 있다.
Toyonaga 선생님께서 일전에 대한소화기학회의 영문저널에 기고한 논문 Principles of quality controlled ESD with appropriate dissection level and high quality resected specimen. Clin Endosc 2012;45:362-74를 읽어보시기 바랍니다 (PDF, 8.6 M).

The difference of the density of vessels. (A) The extremely characteristic muscle layers named the oblique muscle layers are symmetrically seen in the anterior/posterior regions of the gastric body. The muscle layer is circularly absent at the inlet of the large vessel. (B) The density and thickness of the vessels in the gastric antrum overwhelmingly differs from those in the gastric body. (Ba) In the antrum, the density of vessel in the submucosal layer is low, and the fibrosis is also minimal, and these allow easy mucosal incision and submucosal dissection. (Bb) In the lesser curvature of the gastric body where the oblique muscle layers exist, as the blood vessels do not diverge frequently and the density of blood vessels are low as in the gastric antrum, the procedure is rather easy if the large penetrating vessels are not hurt by mistake. (Bc) On the other hand, in the anterior/posterior walls of the gastric body, where the oblique muscle layers exist, the greater curvature of the gastric body and lower rectum, the density of blood vessels is high and the diverged vessel network is inevitably hurt, if careful attention is not paid to the depth of mucosal incision and submucosal dissection. (Image and text from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3521937/)
@ 이준행 질문: We showed us Dr. Hanaoka's data published in Endoscopy in 2009. According to that report, the risk of lymph node metastasis and lymphatic invasion is higher for undifferentiated-predominant mixed type than purely undifferentiated type. So, my questin is this. When you see partial area with corkscrew type mucosal pattern, do you or do you not recommend ESD?
@ Takeuchi 박사 답변: Undifferentiated type을 시사하는 corkscrew mucosal pattern이 작으면, 2cm 이하면 그냥 ESD를 하여 병리결과를 본다.
@ 이준행 질문: Thank you for your detailed explanation for the differences between two countries. However, there should be some interobservator variations in a single country. I mean all Korean pathologists are not the same, and all Japaneses pathologists are not the same. There may be Konkuk style, Samsung style, Soonchunhayng style, Kobe style, Osaka style, Jichi style, and Singapore style. Would you comment on this issue?
@ Takeuchi 박사 답변: 일본에서 지역이나 병원에 따른 차이는 거의 없다.
@ 이준행 의견: 일본은 서양과 우리나라와 차이는 있지만 일본 내에서는 상당한 정도의 quality control이 되어 있어서 실제 의사들이 느끼는 interobserver cariation은 매우 적은 것 같습니다. 우리도 보다 상세한 토의를 통하여 의견통일을 시도해야 하지 않을까요?
@ 이준행 준비 질문: One of the expanded indication is submucosal cancer less then 500 micrometer invasion and less than 3 cm in diameter. After ESD we sometimes meet SM1 cancer larger than 3cm. what's your recommendation for this situation?
@ 시간 관계상 질문하지 못하여 스스로 답함: 3cm가 넘더라도 SM invasion이 minute하면 경과관찰을 할 수 있다고 여겨집니다. 그러나 SM invasion의 정확한 모양을 아는 것이 중요합니다. 병리과에 내려가서 함께 슬라이드를 보면서 판단하는 것이 중요하다고 생각합니다.
@ 이준행 준비 질문: Pathologists are becoming more and more interested in lymphatic invasion, so we are experiencing mucosal cancers with lymphatic invasion. What' your opinion about one or two focus of lymphatic involvement? Do you think surgery is really required for lymphatic involvement in the mucosa?
@ 시간관계상 질문하지 못하여 스스로 답함. 병리과 의사들이 점점 자세히 봐 줄수록 수술을 보내야 하는 환자가 많아지고 있습니다. 그러나 과거의 기준으로도 재발률이 거의 없었기 때문에 어쩌면 최근들어 우리들이 너무 많은 환자를 외과로 보내고 있다는 느낌입니다. 그러나 가이드라인을 따를 수 밖에 없습니다. 진단기술의 정밀도가 달라지면서 가이드라인을 재검토할 시점이라고 생각합니다.
![]() 2. Gastric adenoma: to resect, ablate or not (이준행, 삼성서울병원)
2. Gastric adenoma: to resect, ablate or not (이준행, 삼성서울병원)
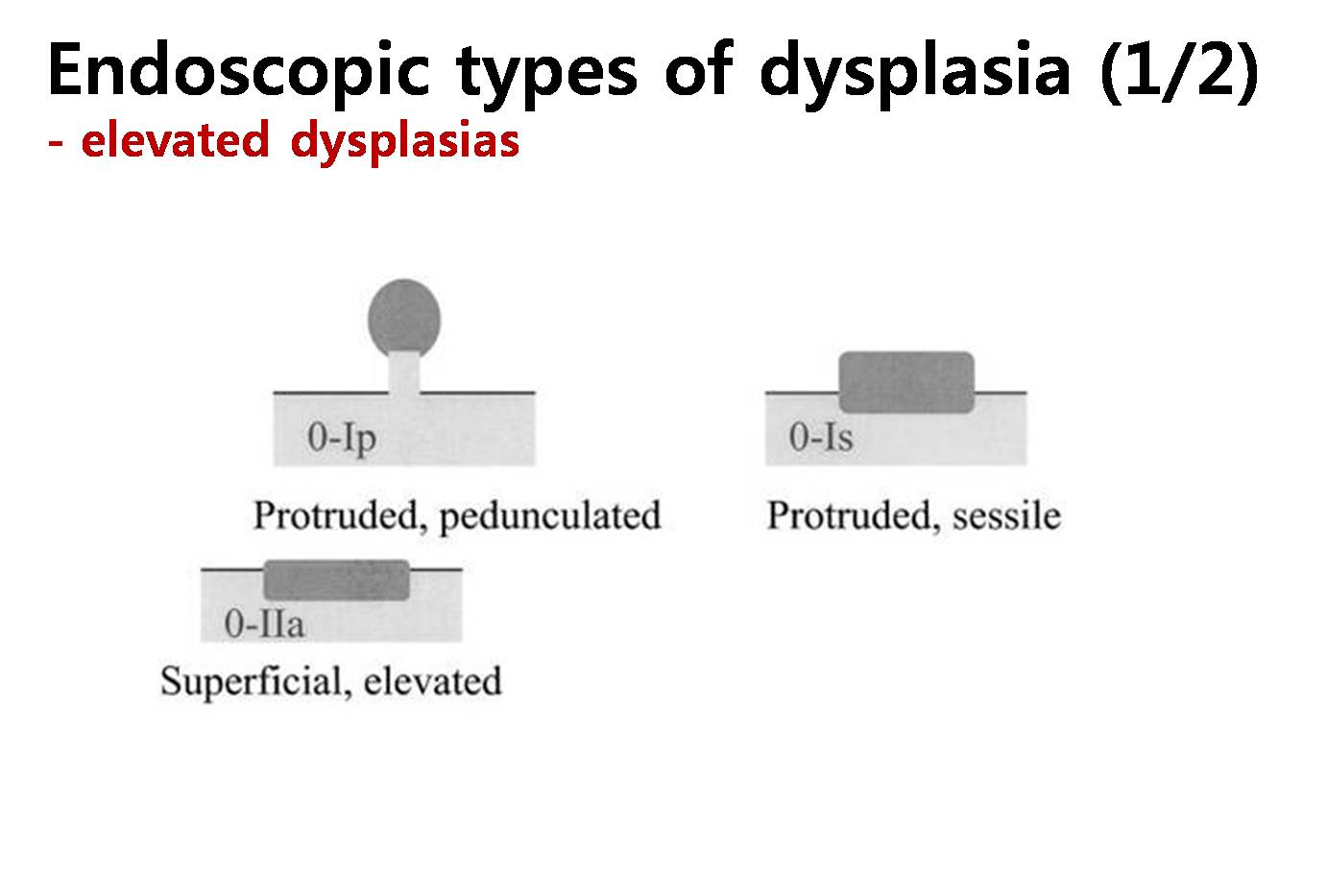
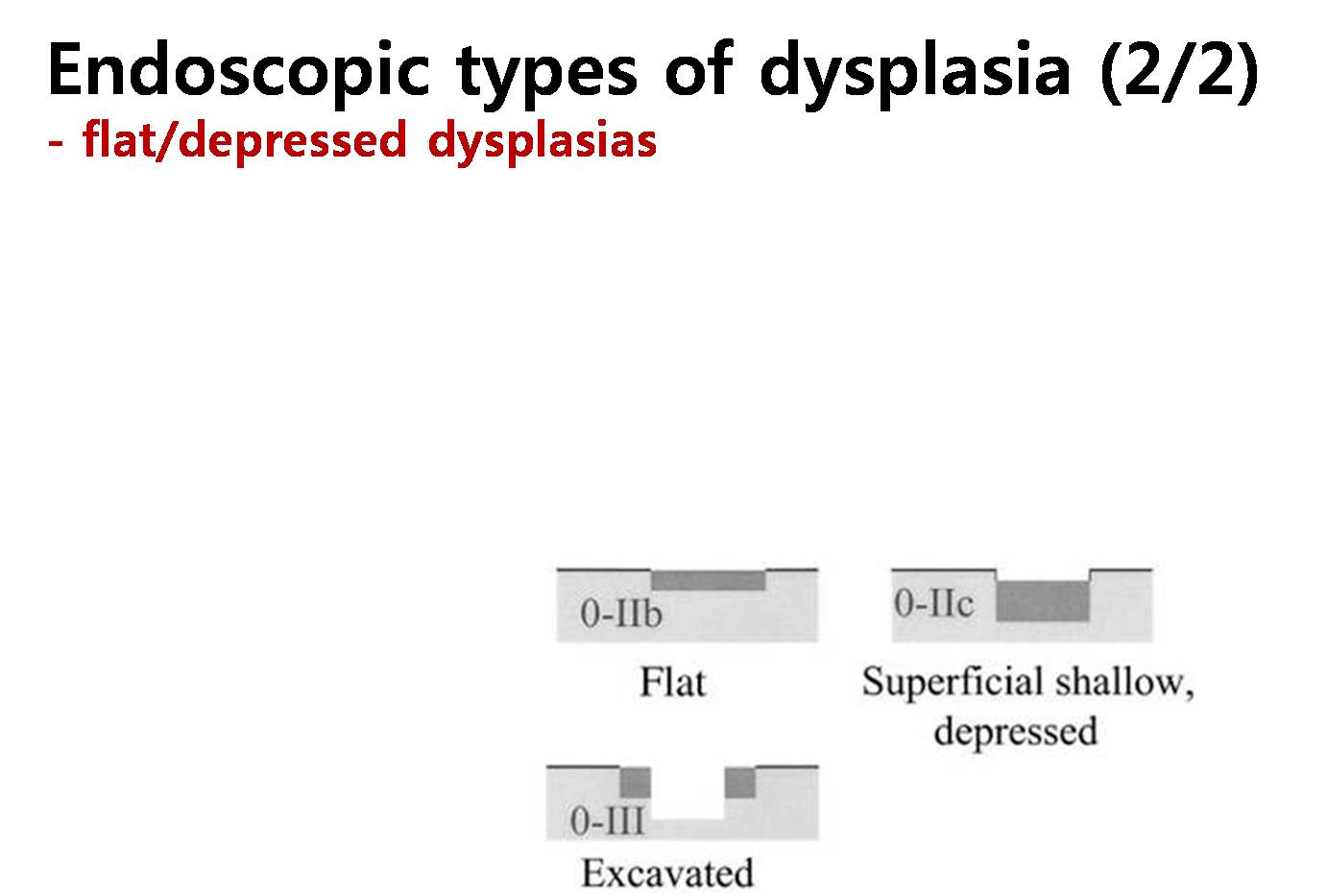
There are no generally accepted definitions of dysplasia and adenoma of the stomach. Dysplasia is best defined as an unequivocal neoplastic epithelial alteration. Detailed histological findings of gastric dysplasias have been described in many literatures. However, endoscopic or gross findings of gastric dysplasia need to be studied in more detail. Macroscopically, two types of dysplasias are recognized: elevated dysplasia and flat/depressed dysplasia.
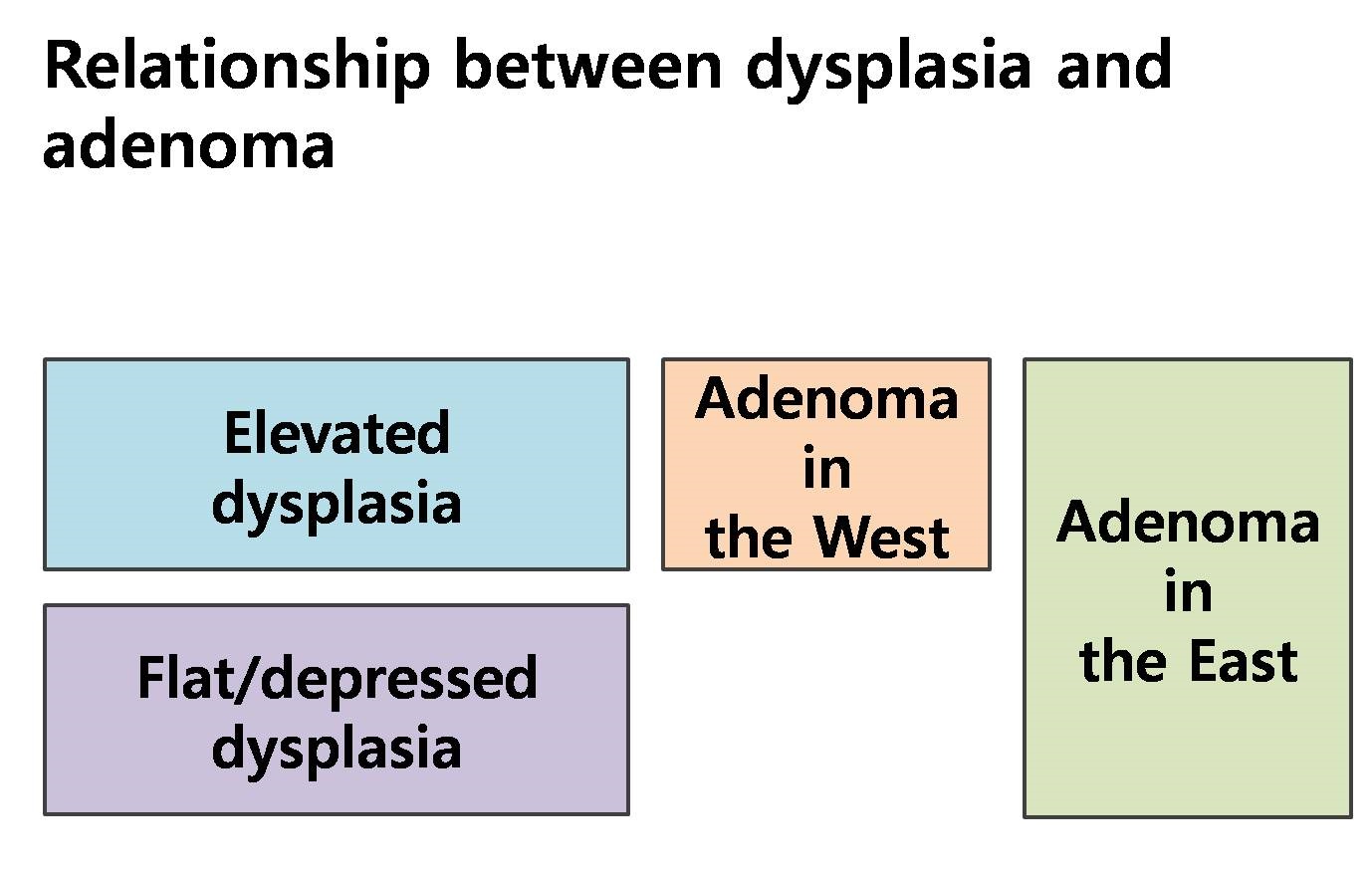
Definition for adenoma is somewhat confusing. In the western countries, adenomas mean elevated or nodular lesions with dysplasia in histology, so only elevated type of dysplasias are considered as adenomas. In the eastern countries, however, both elevated and flat/depressed types of dysplasia are considered as adenomas. Actually, the terms dysplasia and adenoma are thought to be the same thing in the clinical practice. The difference is who prefers what. Usually, pathologists prefer dysplasia, and endoscopists prefer adenoma.
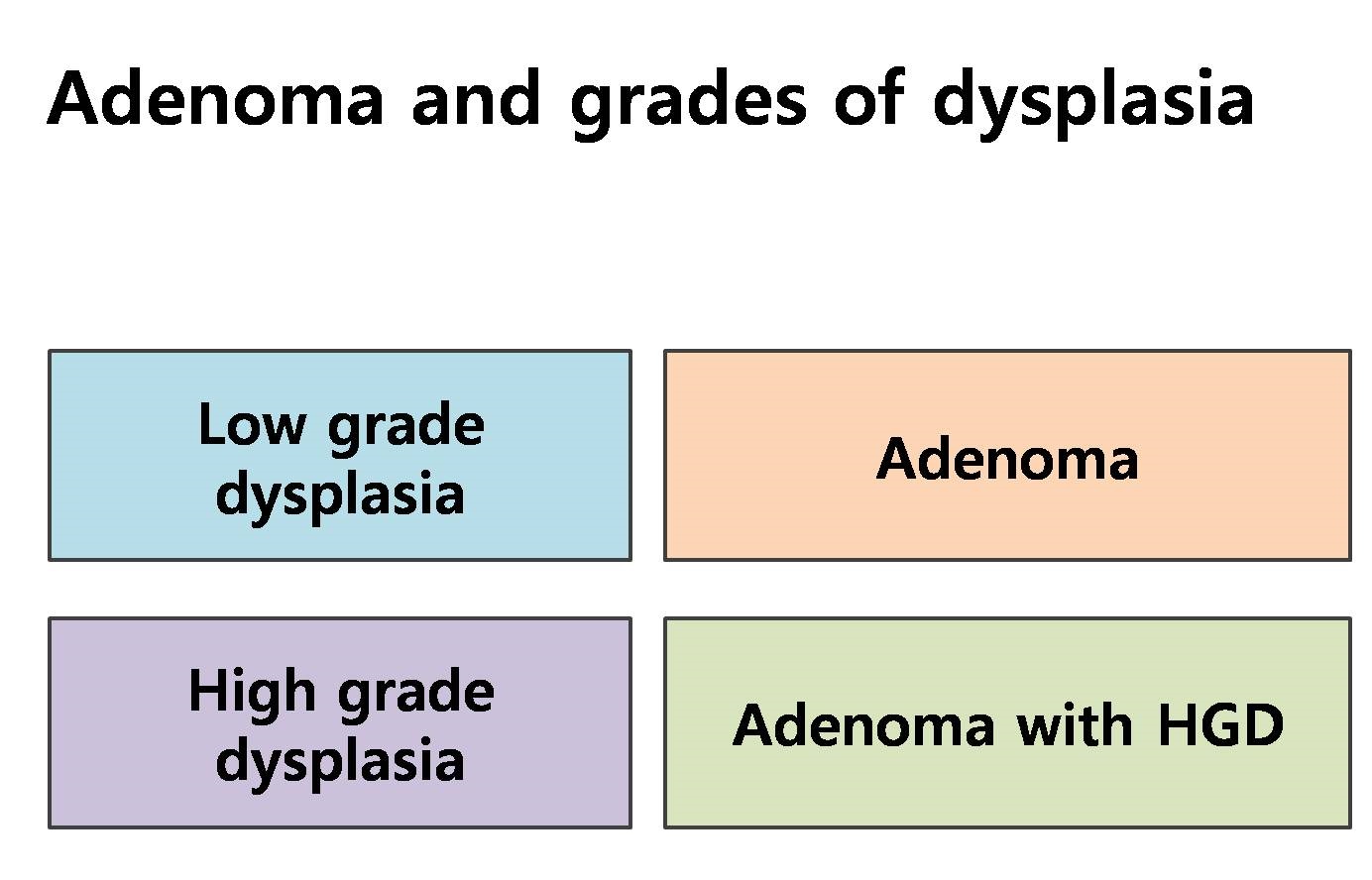
Dysplasias are graded as either high grade or low grade. So, adenomas (= dysplasias) can be divided as adenoma with low grade dysplasia (LGD) and adenoma with high grade dysplasia (HGD). In Korean pathologists' tradition, adenoma usually means adenoma with LGD.
In Korea, gastric adenomas with HGD are usually treated by endoscopic resection. In the final pathology for the resected specimen, 1/3 to 1/2 of adenomas with HGD are upgraded as cancer. Therapeutic approach for adenomas with HGD should be the same for early gastric cancers within absolute indications for endoscopic submucosal dissection (ESD).
Situations for gastric adenomas with LGD are quite different. After endoscopic resection of adenoma with LGD, the risk of histological upgrading is relatively small. About 10-20% of adenomas with LGD are upgraded to adenoma with HGD and 5-10% are upgraded to early gastric cancers. So, the clinical options for adenomas with LGD can be resection (EMR or ESD), ablation, and observation. In the lecture, some data regarding the advantages and disadvantages of each treatment options will be discussed.
We need to start from the definition of dysplasia. What is dysplasia? Most simply, it is an unequivocal neoplastic transformation.
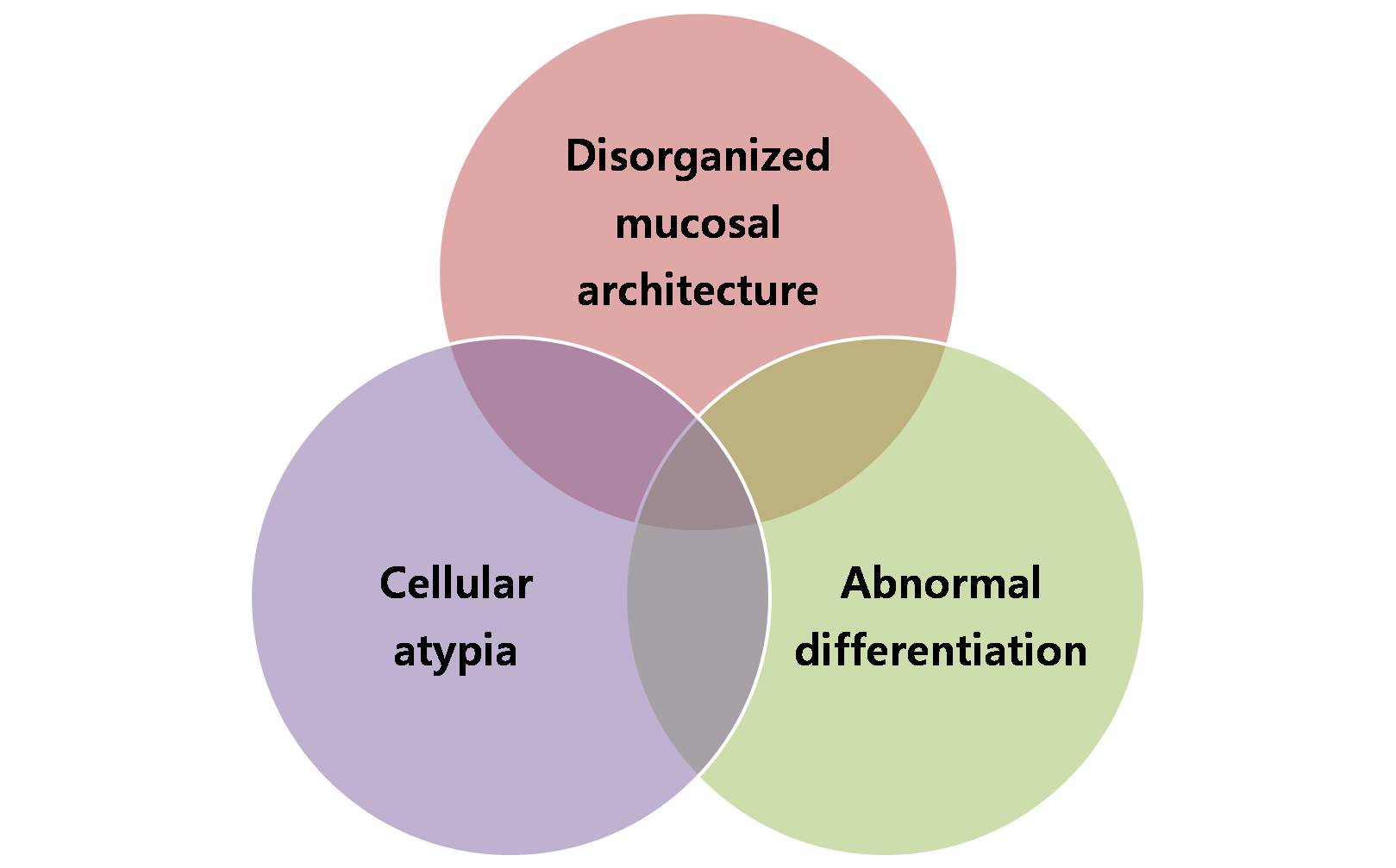
There are three important histological characteristics for gastric dysplasia. They are disorganized mucosal architecture, abnormal differentiation, and cellular atypia.
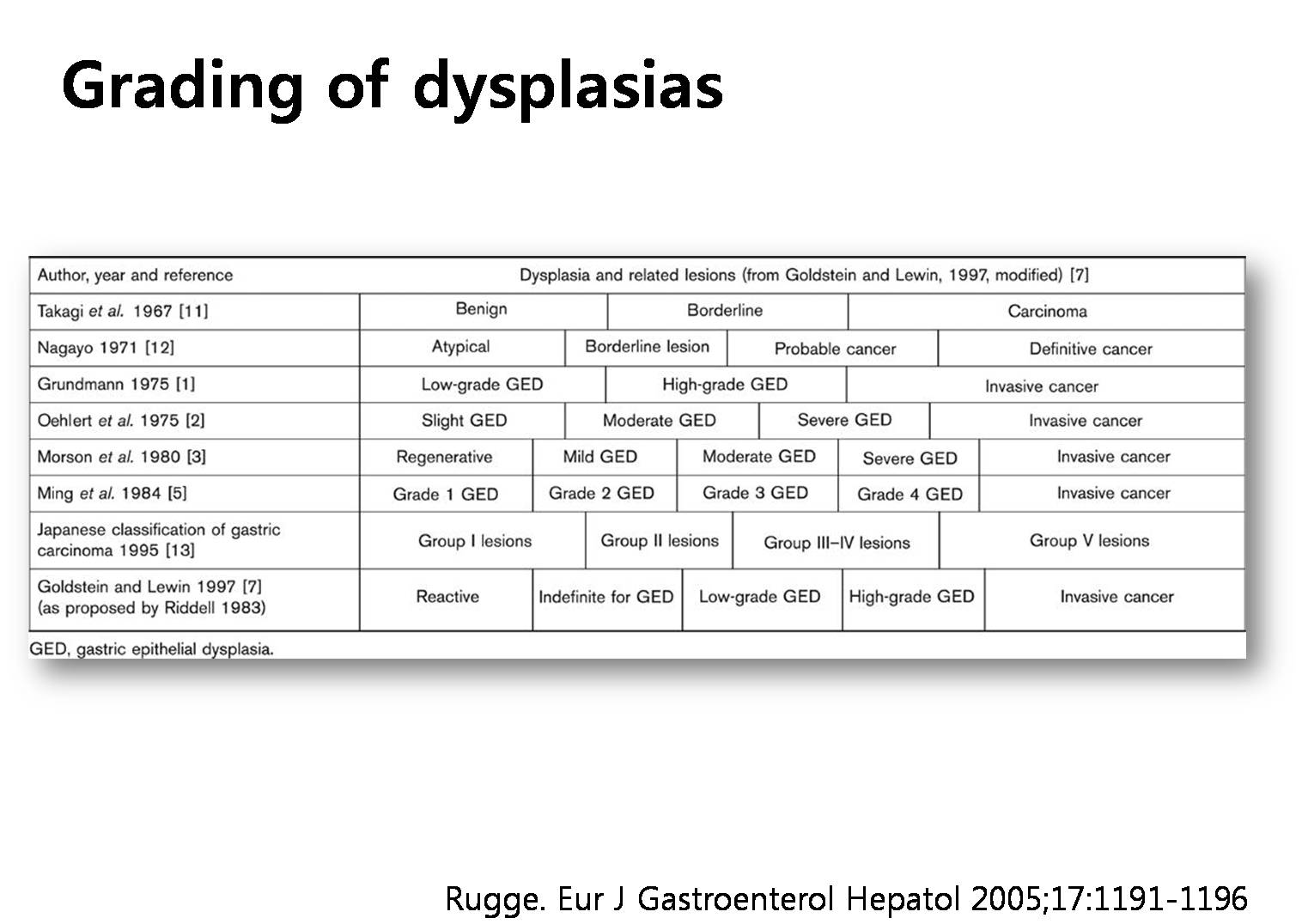
Based on those three characteristics, a lot of grading schemes have been proposed. Isn’t it confusing?
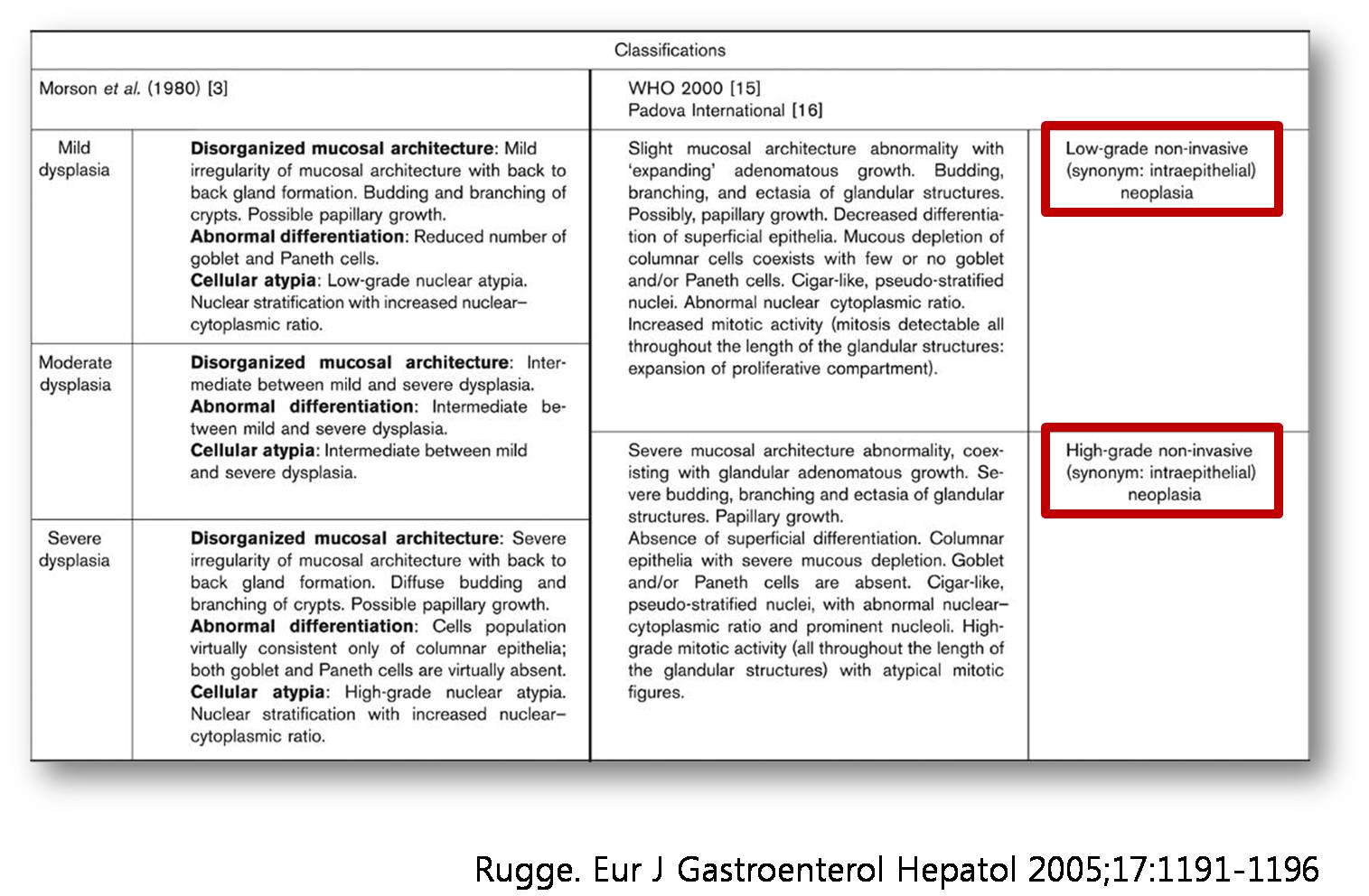
Recently, dysplasias are histologically divided into two groups, low grade dysplasia and high grade dysplasia.
Endoscopically, dysplasias can be divided into elevated dysplasias and flat/depressed dysplasias.
What is the relationship between dysplasia and adenoma? Definition of adenoma is somewhat confusing. In the western countries, adenomas mean elevated or nodular lesions with dysplasia in histology, so only elevated type dysplasias are considered as adenomas. In the eastern countries, however, both elevated and flat/depressed dysplasias are considered as adenomas. Actually, the two terms dysplasia and adenoma are thought to be the same thing in the clinical practice. The difference is who prefers what. Usually, pathologists prefer dysplasia, and endoscopists prefer adenoma.
Dysplasias are graded as either high grade or low grade. So, adenomas (= dysplasias) can be divided as adenoma with low grade dysplasia (LGD) and adenoma with high grade dysplasia (HGD). In Korean pathologists' tradition, adenoma usually means adenoma with LGD.
Ideally, there should be no difference in the histological diagnosis of adenoma and cancer, because everybody is using the Vienna classification. However, it’s not so simple.
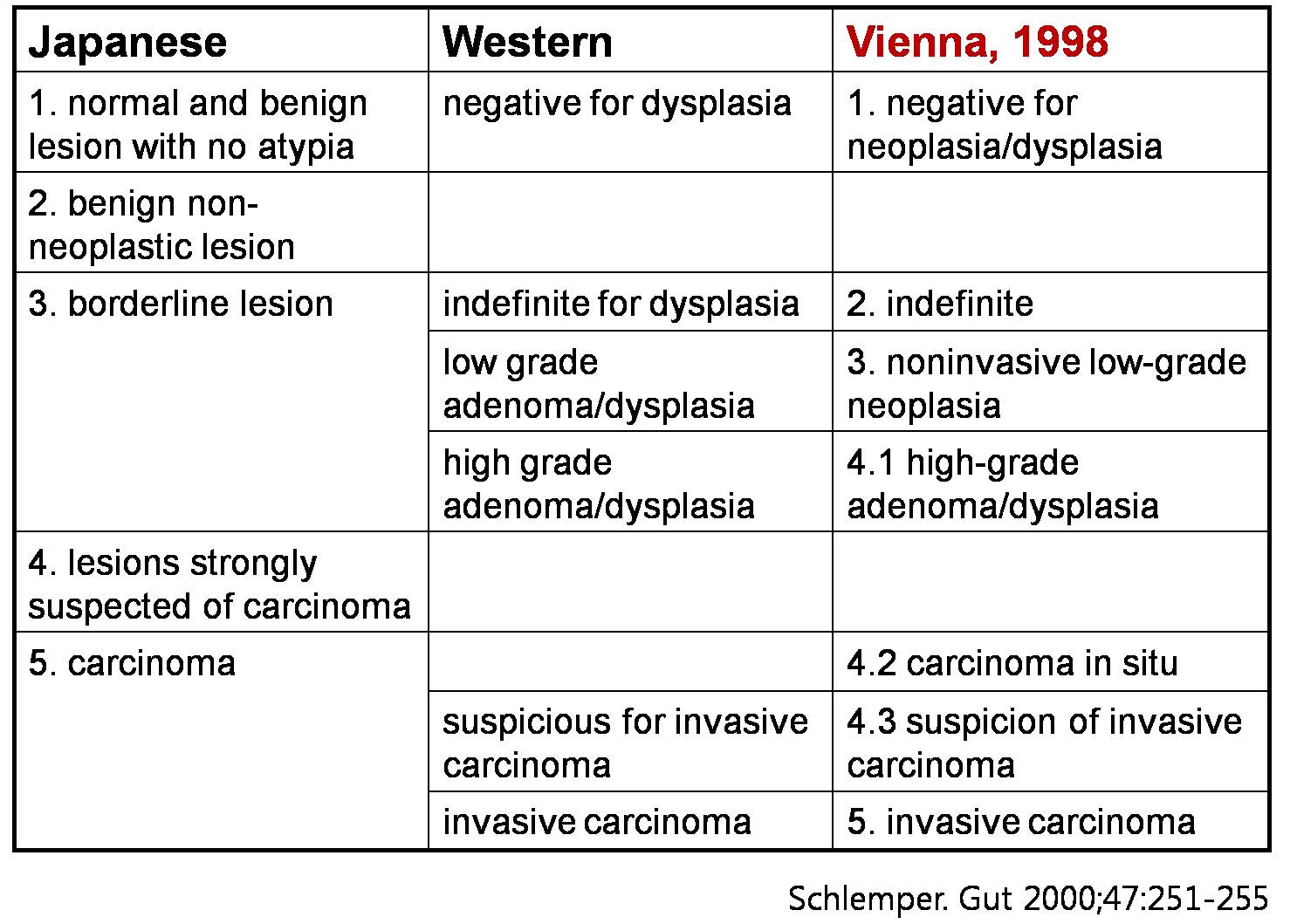
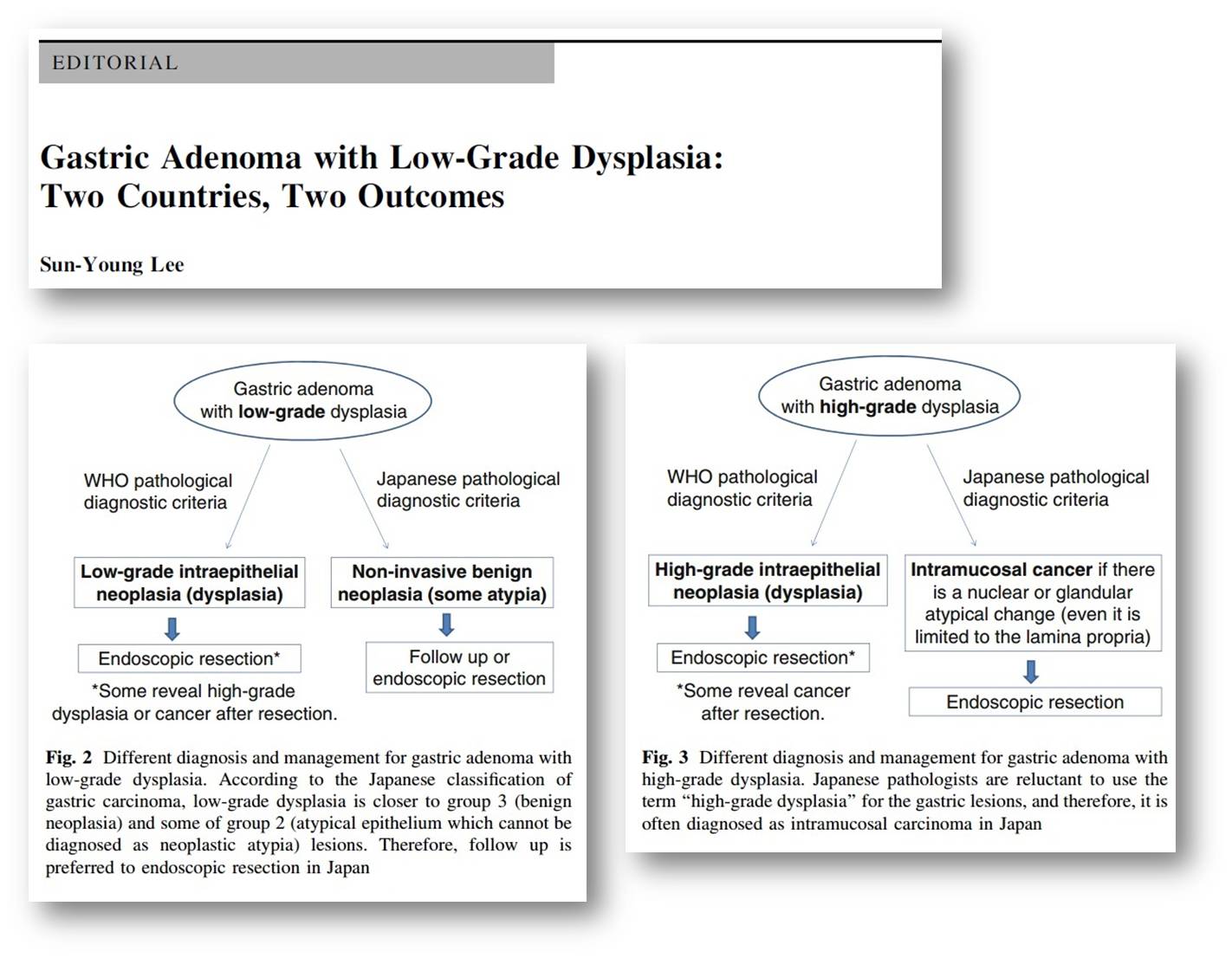
The concept of cancer may be different between countries. In Japan, structural and cytological features are important. In the western countries and in Korea, evidence of invasion is much more important. Actually, we think that most cases of HGD in the western system and Korea, as well as some LGD, become carcinoma in the Japanese system.
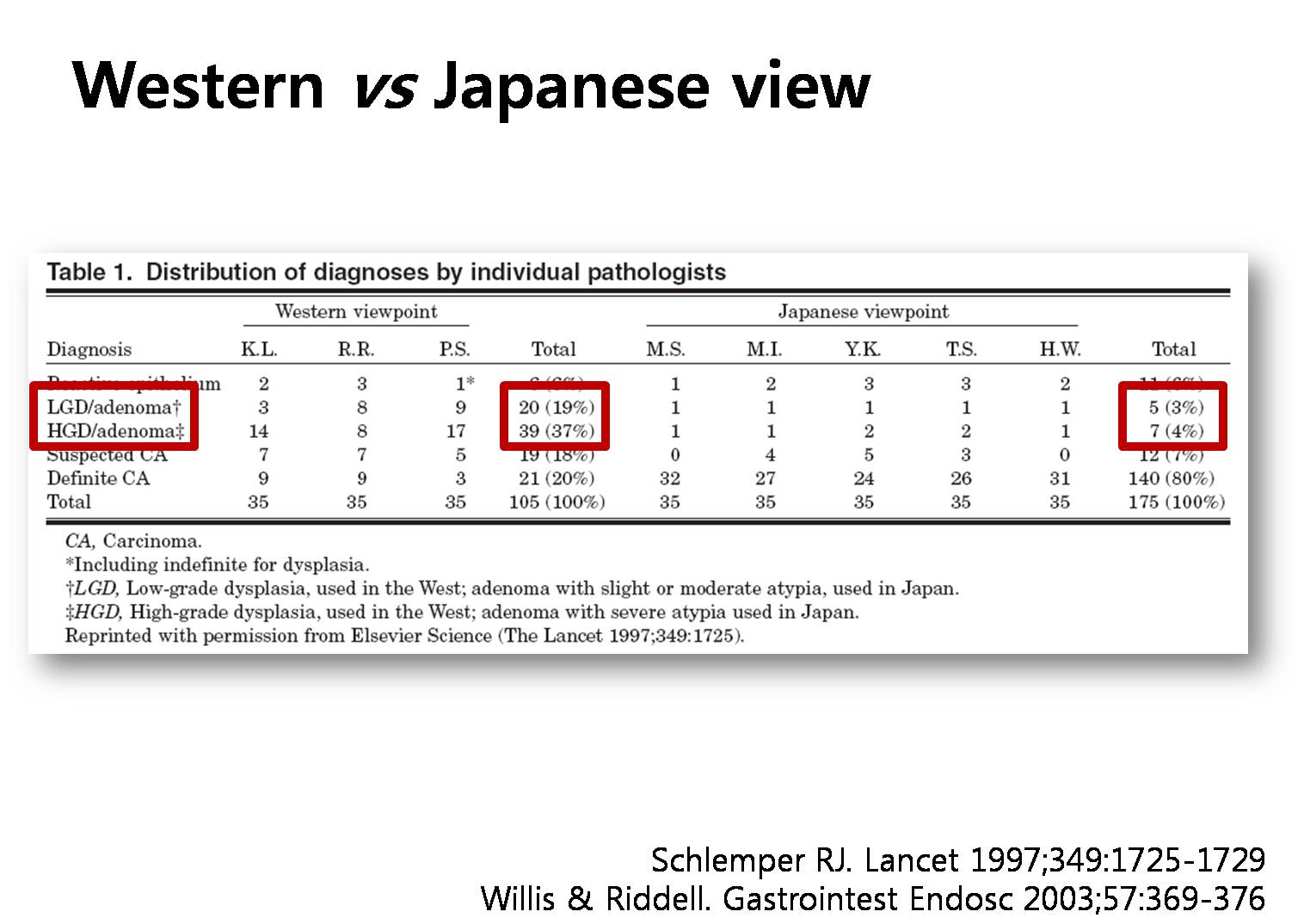
This is a famous study comparing the pathological diagnosis of gastric neoplasm between western countries and Japan. About half of the cases were adenomas by the western point of view. However, only 7 percent were adenomas by Japanese doctors. There is a huge difference. Korean pathologists seem to be close to western doctors in the diagnosis of gastric adenomas.
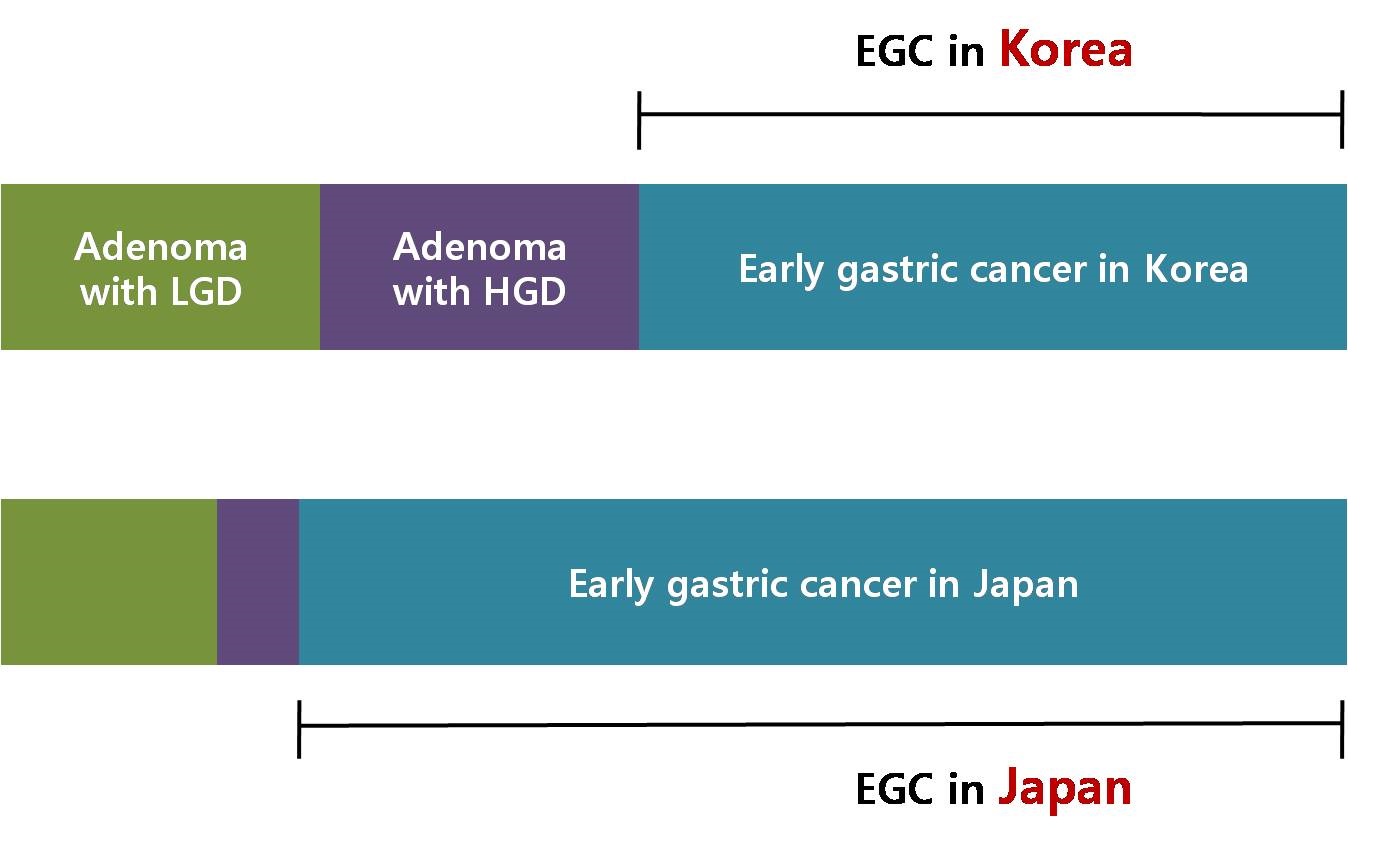
This is my understanding of this confusing situation. Three blocks are adenoma with LGD, adenoma with HGD and EGC in Korea. The next three blocks are diagnoses in Japan. So, most cases of adenoma with HGD in Korea may be EGCs in Japan.
Professor Sun Young Lee at Konkuk University discussed this dilemma in the recent editorial. Most cases of low grade dysplasias are endoscopically resected in Korea, but observation is frequently chosen in Japan. High grade dysplasias are endoscopically resected not only in Korea but also in Japan. But the diagnosis is different.
The natural history of adenoma is not clear yet. In this old study, the low grade adenomas progressed to cancer in 15% in 10 years.

Excluding palliative surgeries, we have endoscopically or surgically treated more than seventeen hundred gastric cancers in 2012 at Samsung Medical Center. Among them, 72% were early gastric cancers. In early gastric cancers, cases within absolute indications were 25%. There were 263 cases of gastric adenomas in a single year.

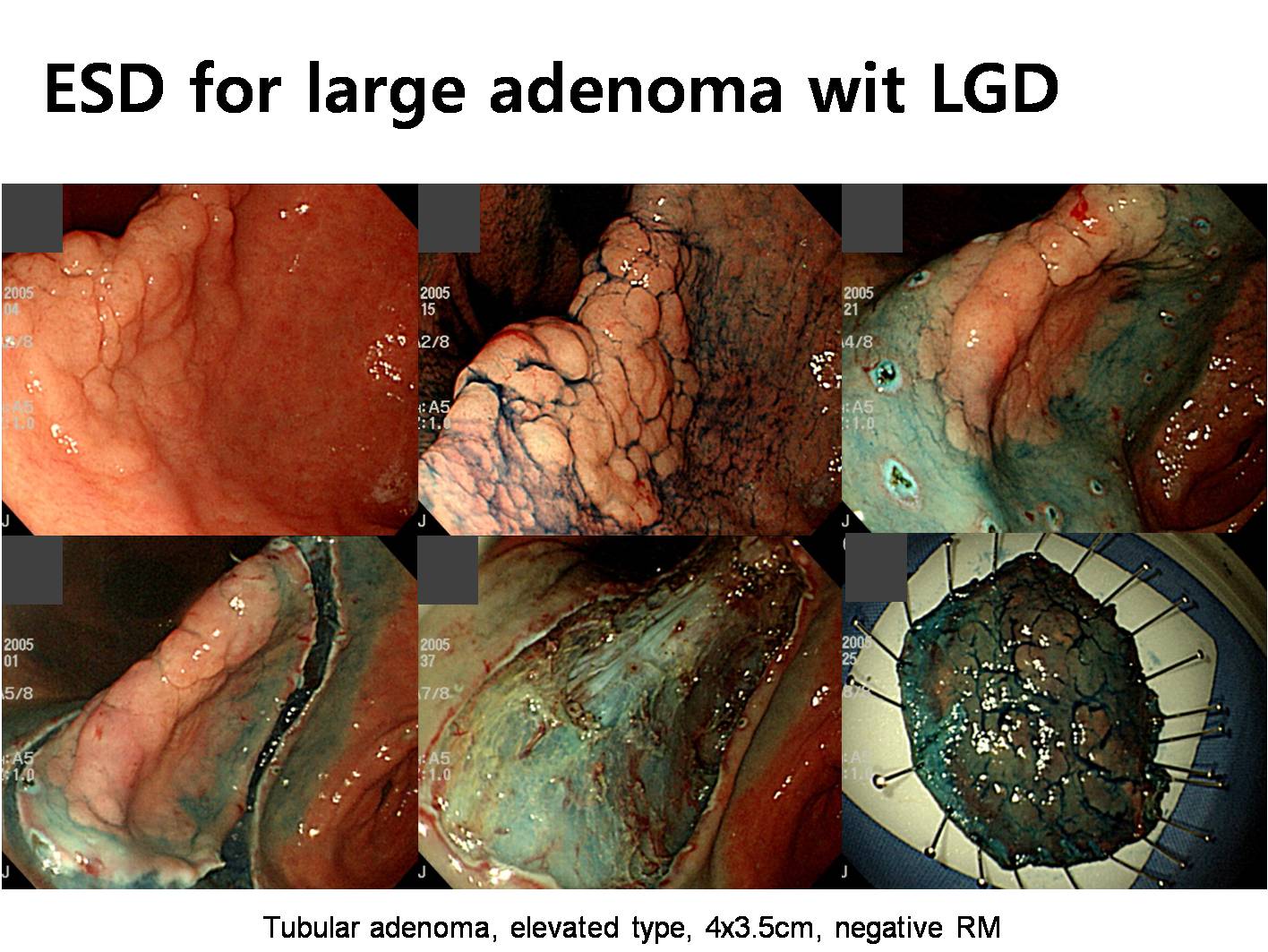
This is an example of endoscopically treated adenoma with low grade dysplasia.
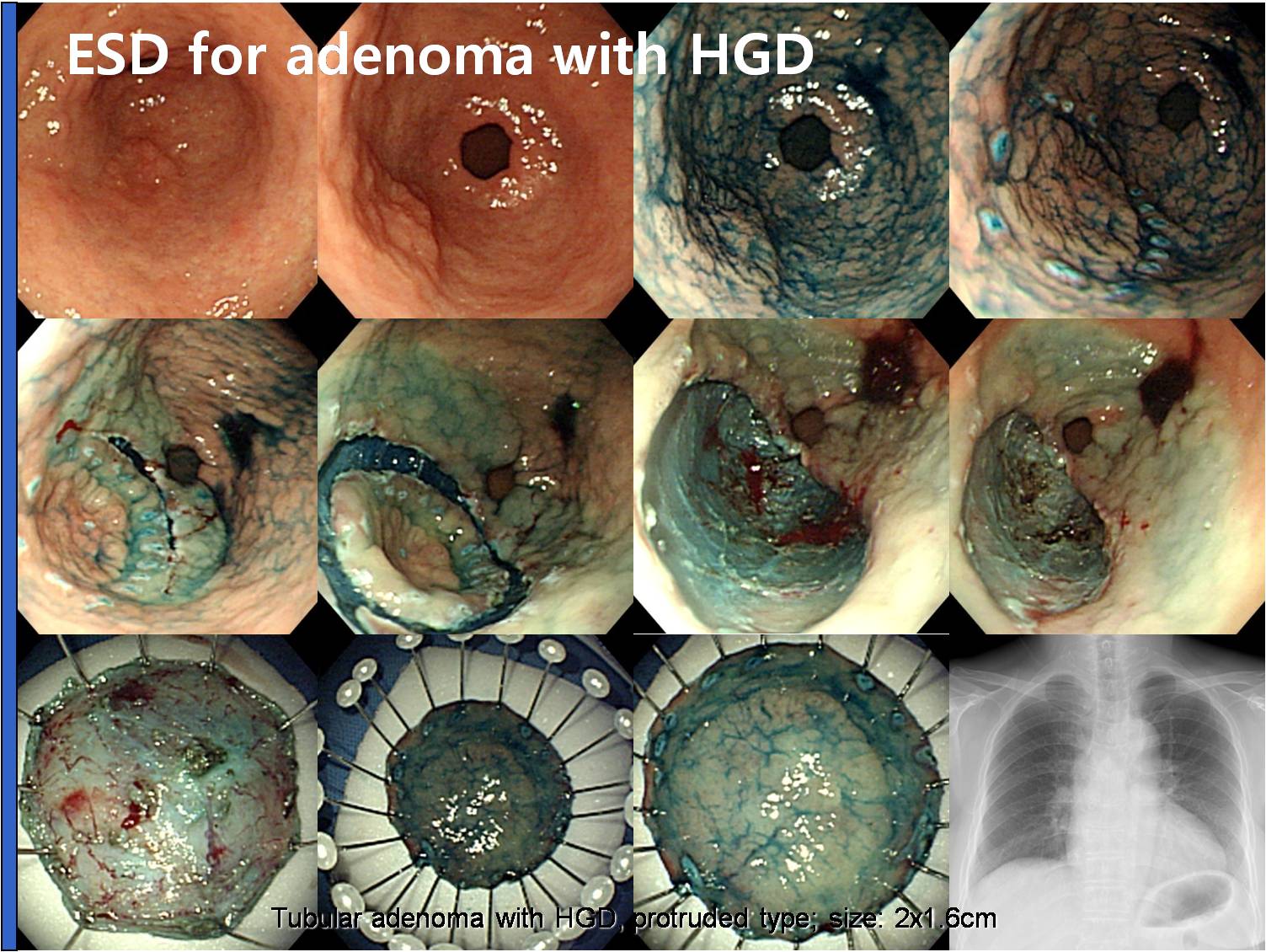
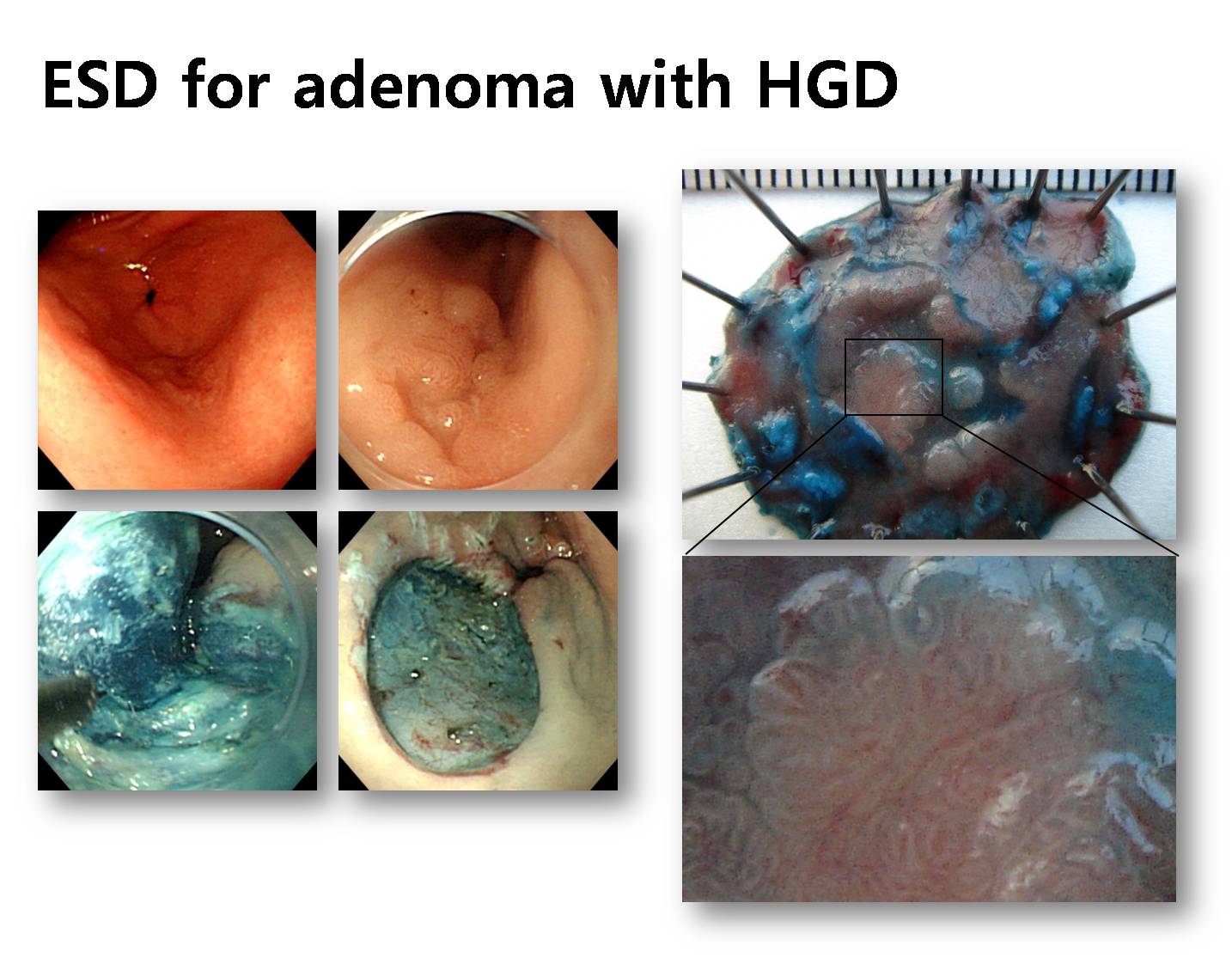
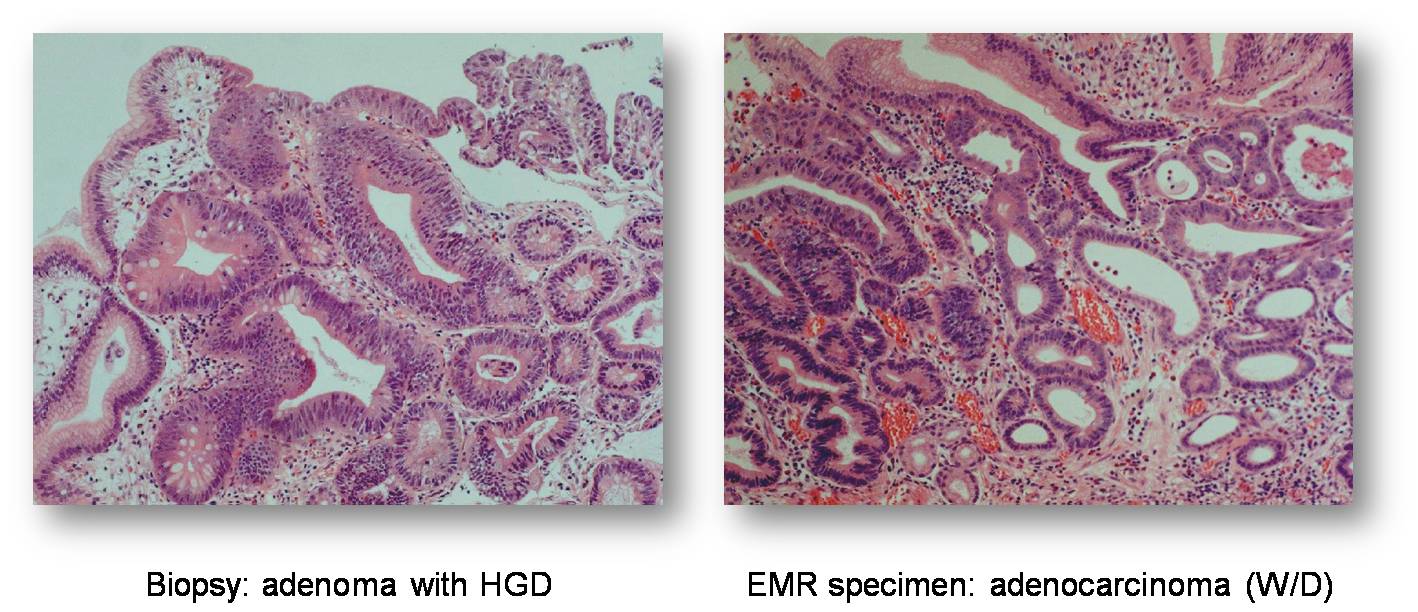
Almost the same thing except that it was an adenoma with high grade dysplasia.
I performed ESD for a small depressed adenoma with LGD.
However, the final ESD pathology was adenocarcinoma.
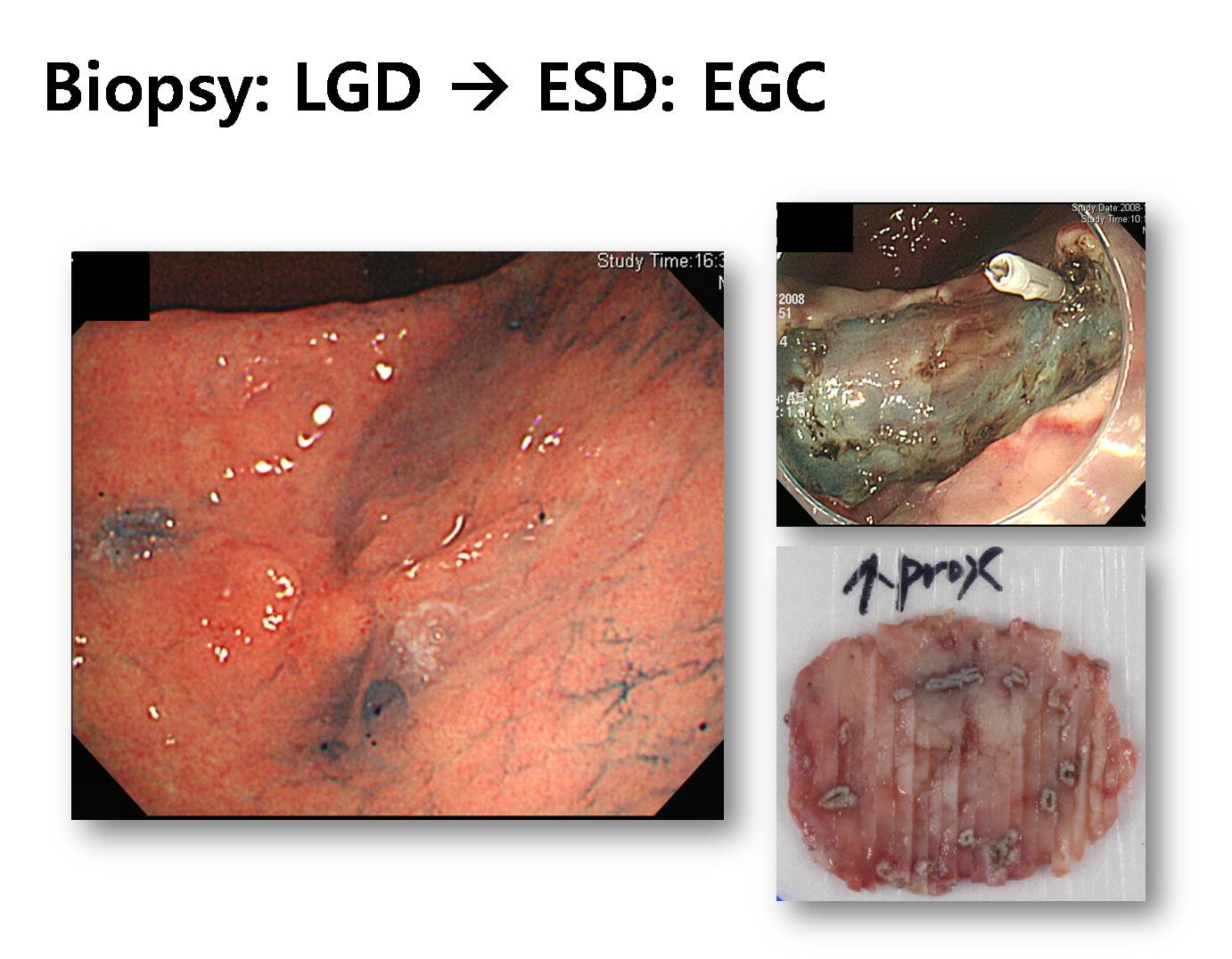
It’s another example of gastric cancer with initial biopsy of adenoma. In this case, the initial biopsy was adenoma with low grade dysplasia.
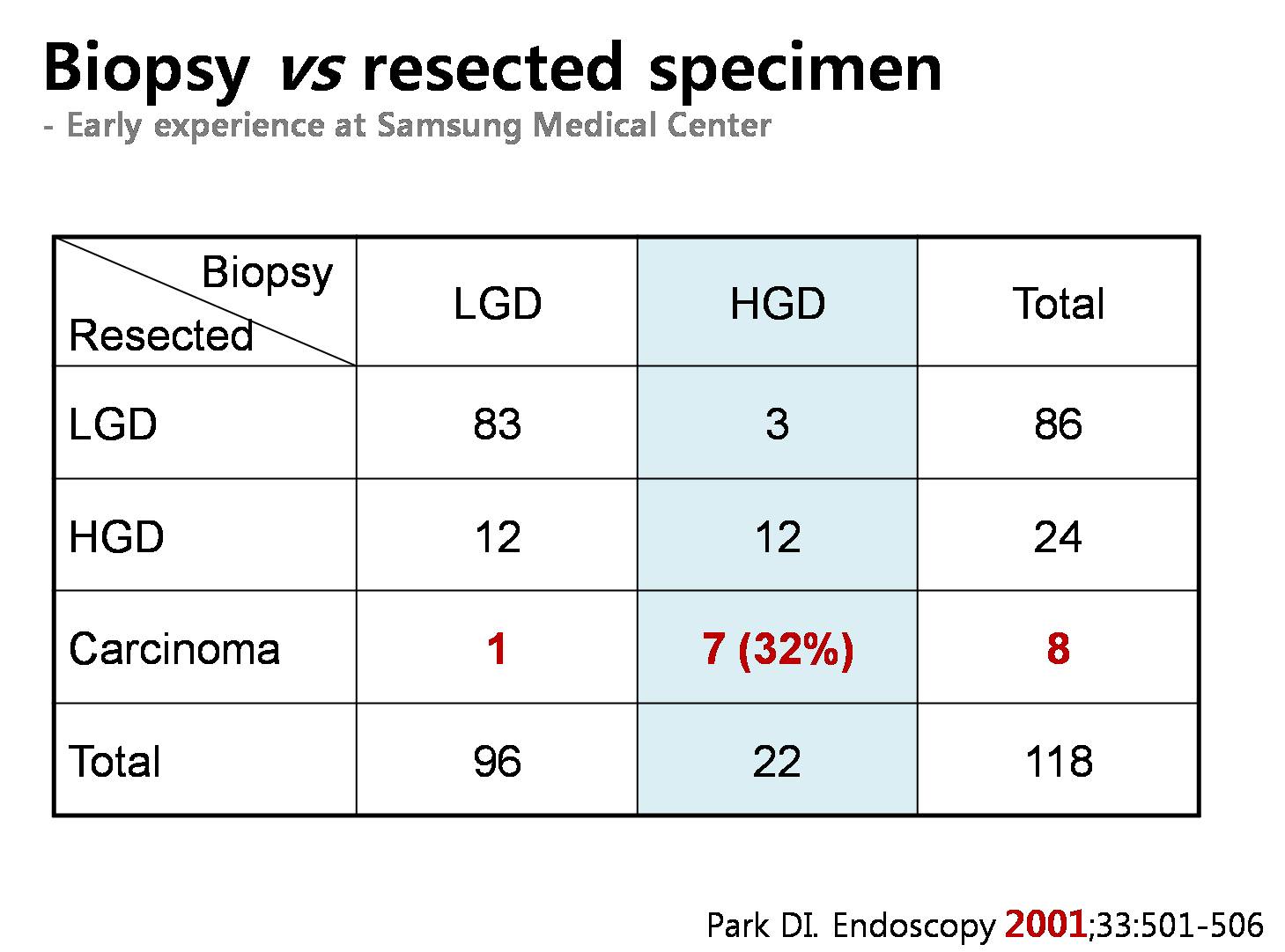
In this old report from my institution, 7 out of 22 adenomas with HGD were actually carcinomas in the endoscopically resected specimen.
We reviewed the discrepancy between pre-treatment diagnostic groups and post-treatment diagnostic groups. As you can see in this complicated slide, the rate of discrepancy is more than expected. For adenoma with LGD, about 34 percents were upgraded as high grade dysplasias or cancers. For adenomas with HGD, 34 percents were upgraded as cancers.

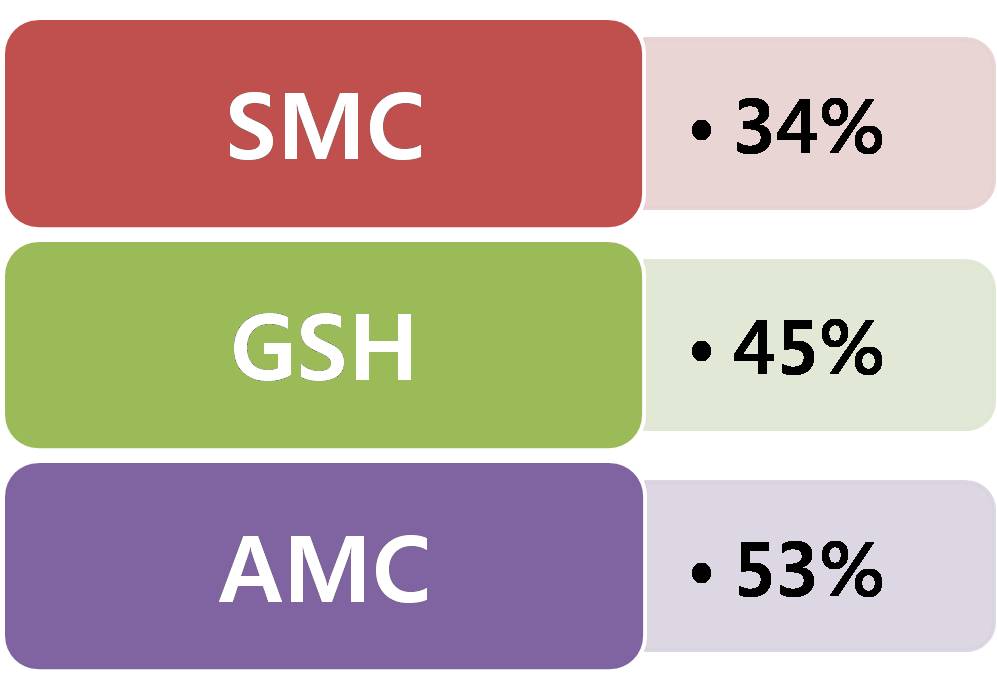
This is a personal communication. About 1/3 to half of cases with high grade dysplasia are upgraded into cancers at Samsung Medical Center, Gangnam Severance Hospital, and Asan Medical Center.
In this report from Yonsei University, 51 out of 273 endoscopically resected low grade adenomas were upgraded into either HGD or adenocarcinoma. They evaluated the risk factors for upgrading, and recommended endoscopic resection for larger lesions and lesions without white discoloration
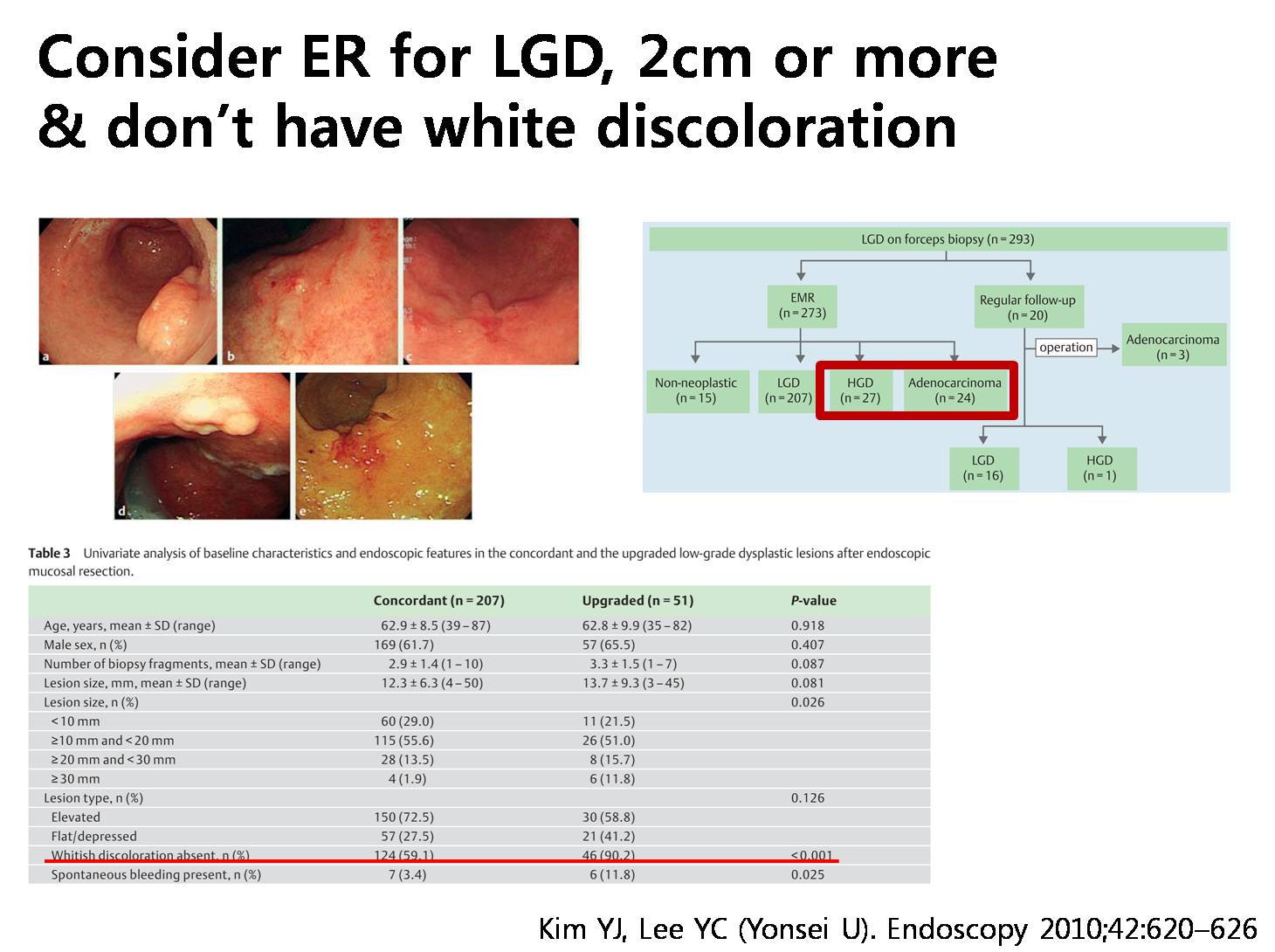
So, small pale flat elevated low graded adenomas can be easily treated by ablation therapy using argon plasma coagulation.

Ladies and gentlemen. I’d like to conclude my short presentation. For adenomas with HGD, endoscopic resection, preferably ESD, is recommended. For adenomas with LGD, endoscopic resection is preferred for larger lesions or lesions with central depression. Ablation is an easy and effective treatment for small pale flat/elevated adenomas with LGD.
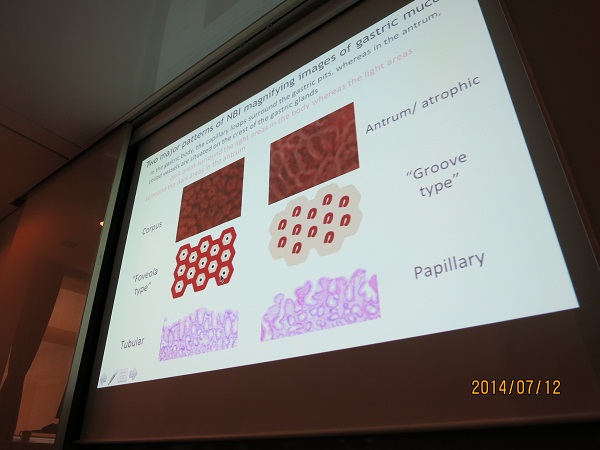
![]() 3. Magnifying endoscopy using NBI (Yoji Takeuchi, Osaka Medical Center for Cancer and Cardiovascular Disease)
3. Magnifying endoscopy using NBI (Yoji Takeuchi, Osaka Medical Center for Cancer and Cardiovascular Disease)


![]() 4. Gastric neoplasm: differences between Japan and Korea (이선영, 건국대학교)
4. Gastric neoplasm: differences between Japan and Korea (이선영, 건국대학교)
강의의 결론: Gastric adenoma with LGD should be resected outside Japan because the term "LGD" outside Japan means something significant that requires resection. Efforts should be made to develop unified international guideline for the management of gastric adenoma with LGD by overcoming the differences in the diagnostic criteria that are currently used in different countries and lead to different natural course.
@ 이준행 의견: LGD도 대부분 치료가 필요하다는데는 동의하지만 모두 다 resection해야 하는가는 좀 더 연구해야 한다고 생각합니다. 저는 상당수를 소작술로 치료하고 있습니다.
![]() 5. Toyonaga 선생님의 대장 ESD live demonstration 장면
5. Toyonaga 선생님의 대장 ESD live demonstration 장면

시술자 Toyonaga 선생님과 moderator 성인경 선생님.

Live demonstration을 보기 위한 열기

병원 지하 강당 앞에 붙어 있는 내시경 광고. 무슨 내시경일까???
![]()