 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [KINGCA 구연발표]
[KINGCA 구연발표]
Thank you for your kind introduction.
Clinical outcome of endoscopic treatment for EGCs in the expanded indications is not established. Among them, favorable results have been published about expanded indication lesions with differentiated-type histology. However, data for undifferentiated-type expanded indication lesions are not enough. Most of them are small retrospective studies with unclearly defined inclusion criteria.

In many cases with undifferentiated-type histology in the ESD specimen, the initial biopsy was differentiated-type histology. In our ESD experience for undifferentiated-type EGCs, only 9 out of 59 cases showed undifferentiated-type histology in the initial endoscopic biopsy. This kind of pretreatment and posttreatment histological discrepancy is a big clinical problem.
We re-evaluated the expanded indications with undifferentiated-type histology using a non-selected surgical cohort of endoscopically suspected EGCs. This is not a real clinical outcome result, but an analysis based on clinical simulation. We simulated the selection process of ESD candidates, and evaluated the pathologic outcomes of ESD for undifferentiated-type EGCs.
Among 802 patients who underwent gastrectomy for poorly differentiated adenocarcinoma (PD) or signet ring cell carcinoma (SRC) on endoscopic biopsy, 537 endoscopically suspected EGCs were enrolled. ESD candidates were selected by the expanded indications of ESD, such as (1) 2 cm or smaller in diameter, (2) without ulceration, (3) clinically mucosal lesion and (4) no evidence of lymph node metastasis in abdominal computed tomography.
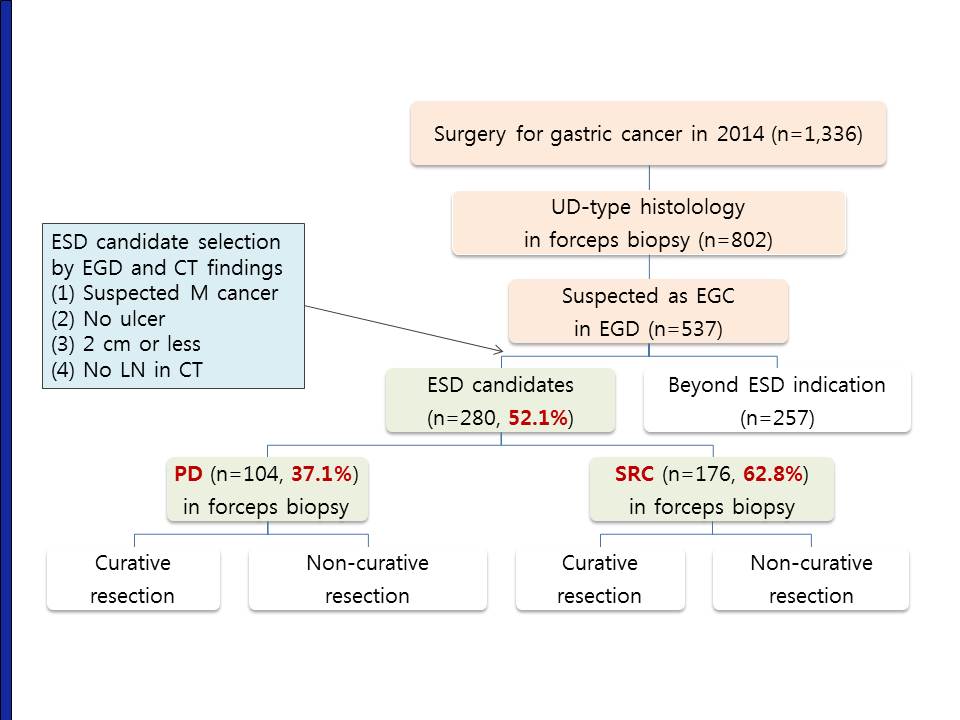
Among 537 endoscopically suspected EGCs, 52 percent were selected as ESD candidates. Among them, 37 percent were poorly differentiated adenocarcinoma and 63 percent were signet ring cell carcinomas. Based on the pathology of the surgically resected specimen, outcomes of ESD simulation were evaluated as either curative resection or non-curative resection.
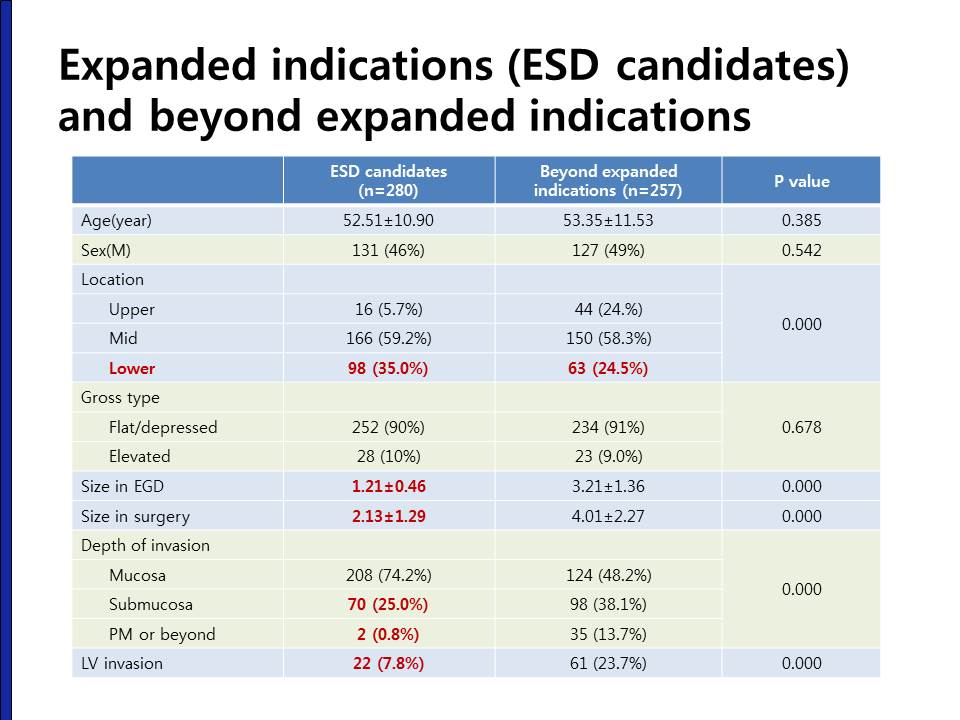
This is the comparison between expanded indication lesions and beyond expanded indication lesions. In ESD candidate lesions, the endoscopically estimated size was 1.2 cm and the size in the resected specimen was 2.1 cm, which means the size is usually underestimated in endoscopy. ESD candidates were basically endoscopically suspected mucosal lesions, however, 26% of them were at least submucosal cancers. Lymphovascular invasion were seen in 7.8%.

We compared the clinical and pathological characteristics between PD type expanded indication lesions and SRC type expanded indication lesions. Age, sex, and the location were similar. There were more elevated lesions in the SRC type EGCs. There were more submucosal cancers in PD-type EGCs. The rate of lymphovascular invasion was slightly higher in PD type EGCs. As a whole, the rate of curative resection was 32% in PD type EGCs, and 48% in SRC type EGCs. The difference was statistically significant.
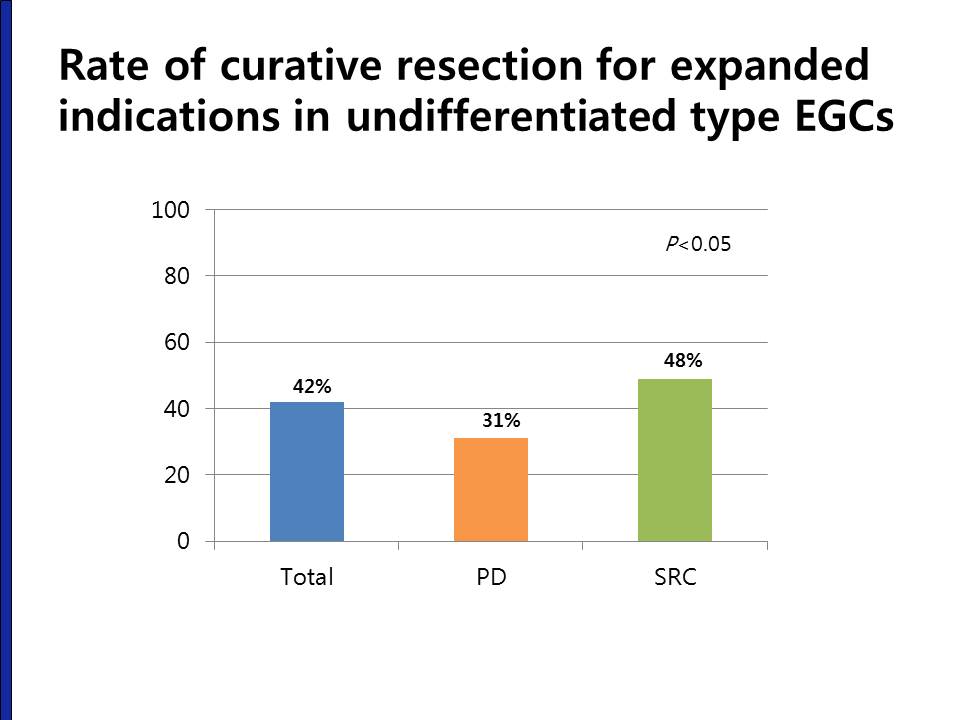
Once again, the overall rate of curative resection for expanded indication undifferentiated type EGCs was only 42%. Especially, the curative resection rate in PD type EGCs was less than one third.
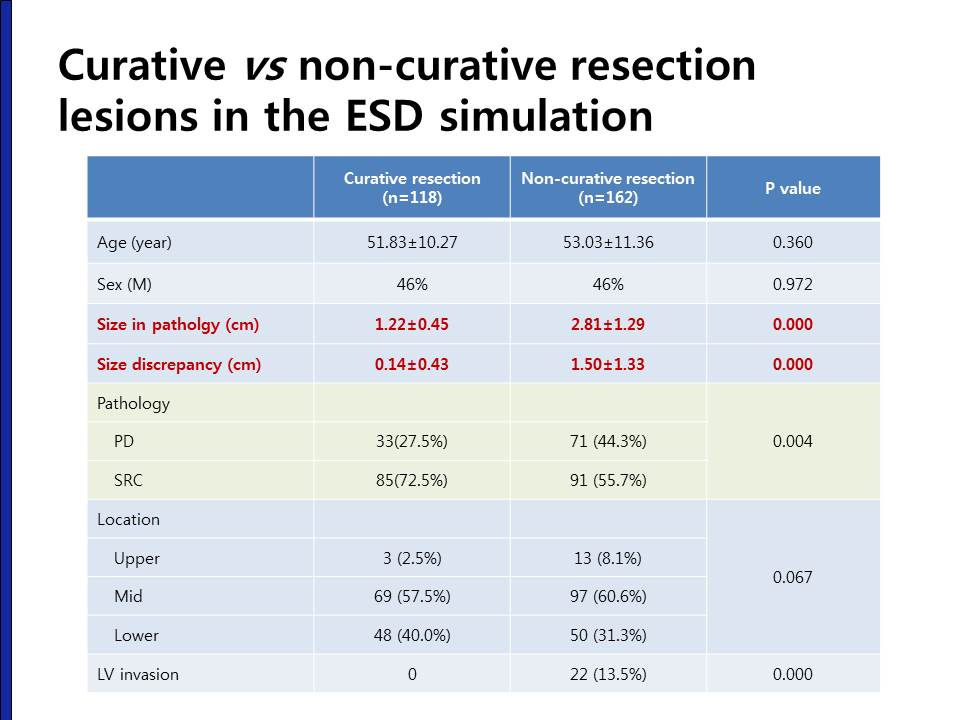
When we compare the characteristics between the curative resection lesions and non-curative resection lesions, there were no differences in terms of age, sex, location and gross type. However, the size in the curative resection group was smaller than the non-curative resection group. The size discrepancy between endoscopy size and pathology size was only 0.14 cm in curative resection group, but the size discrepancy was 1.5 cm in the non-curative resection group. This size discrepancy was one of the major reasons of non-curative resection.
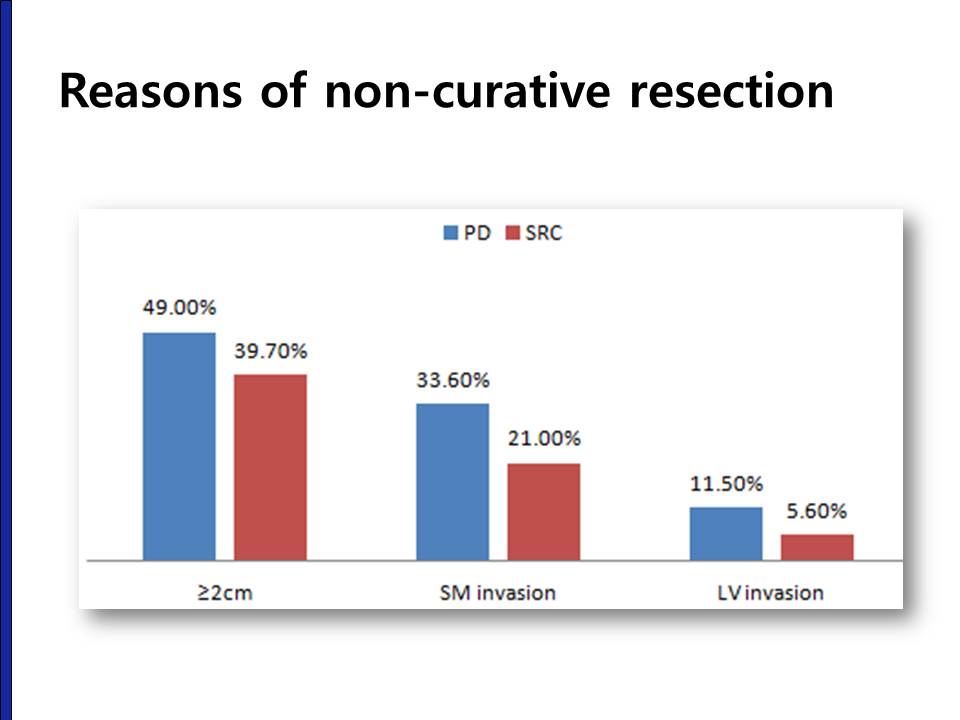
This graph shows the reasons of non-curative resection in out ESD simulation. The most common reason was the size larger than 2 cm, followed by SM invasion and LV invasion.

There were three cases with lymph node metastasis in the curative resection group. Two were PD-type and one was SRC-type in the forceps biopsy. In the final surgical pathology, they was PD type mucosal cancers with SRC components larger than 1.0 cm.

Because the size was the most common reason of non-curative resection, we modified the expanded indication criteria into 1.5 cm, 1 cm and 0.6 cm. When a size criterion of 1 cm was applied, the number of ESD candidates were decreased by 51.4% and the curative resection rate was increased into 54%. However, this increase in the curative resection rate was mostly seen in the SRC type EGCS. The curative resection rate in PD type was almost the same in the smaller lesions.
Now, I'd like to summary our findings. Among EGCs with undifferentiated type histology, ESD candidates meeting the expanded indications were 51%. Overall curative resection rate was 42%, but the curative resection rate in PD-type EGCs was lower than in SRC-type EGCs. Among curative resection cases, lymph node metastasis was found in 2.5%, and they were mucosal cancers larger than 1 cm in size. In SRC-type EGCs, the curative resection rate was increased with smaller size criterion, while the curative resection rate was below 50% in smaller size criterion in PD-type EGCs.
Ladies and gentlemen. I'd like to conclude my presentation by saying that in undifferentiated-type EGCs, ESD should be considered in more selected patients, such as tumor size < 1 cm with histology of SRC to achieve better outcomes.
© 일원내시경교실 바른내시경연구소 이준행