EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [SI-HUG 2020]
[SI-HUG 2020]
첫 날 마지막 강의
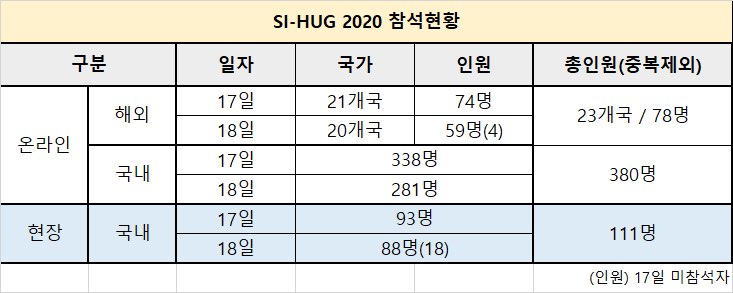
일부 참석자는 off-line으로 다수의 참석자는 off-line으로 진행하였습니다. 전시 부스 중간에 큰 모니터를 설치하여 진행 상황을 살폈습니다.
![]() Day 1
Day 1
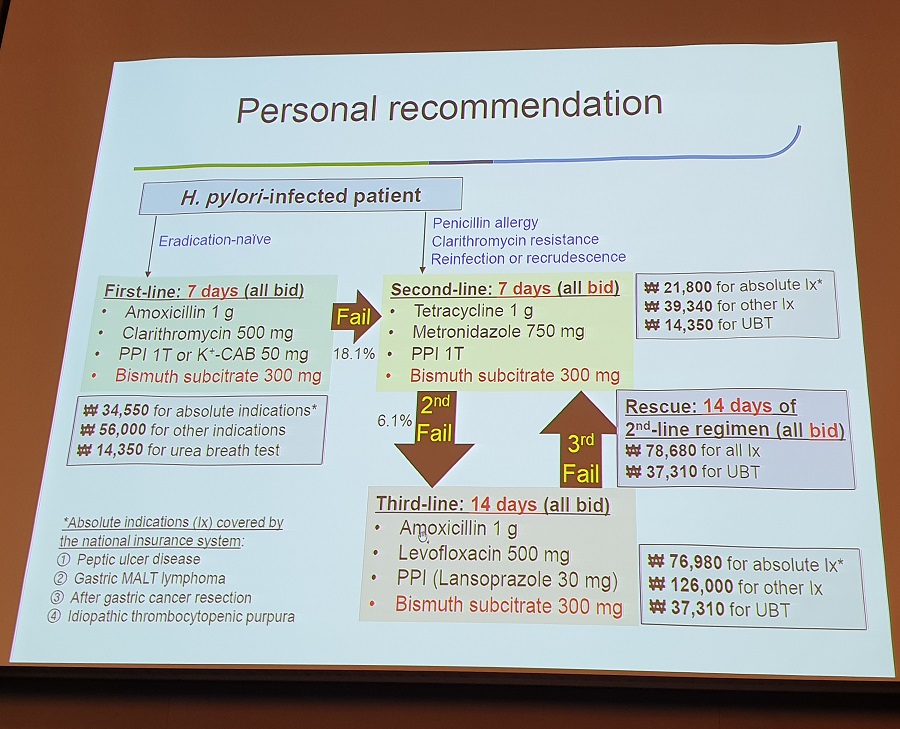
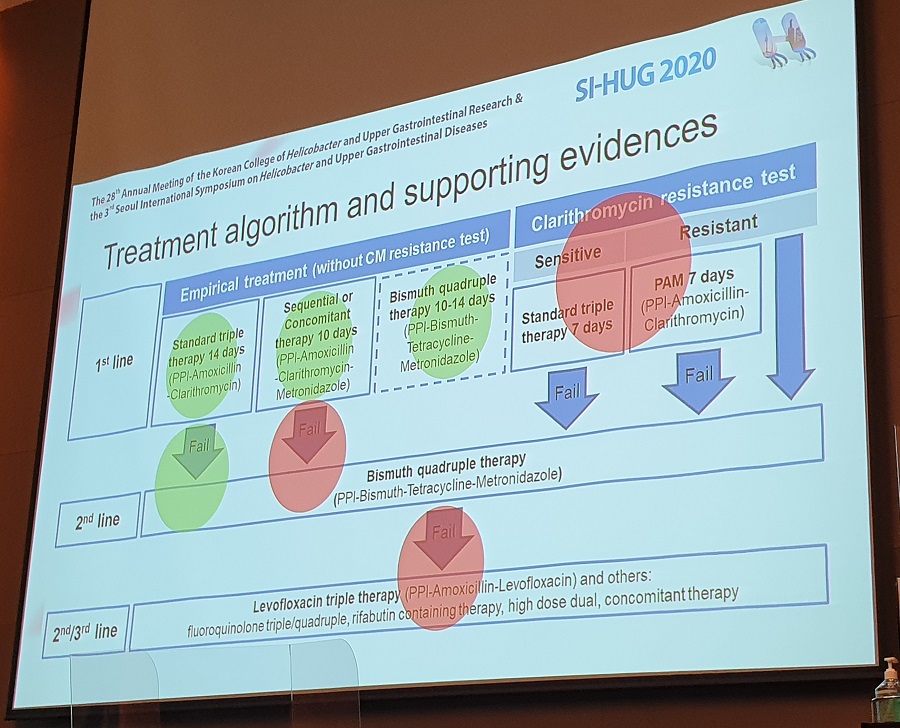
이선영 교수님께서는 1,2,3차 치료에 모두 bismuth를 bid로 쓸 것을 제안하셨습니다.
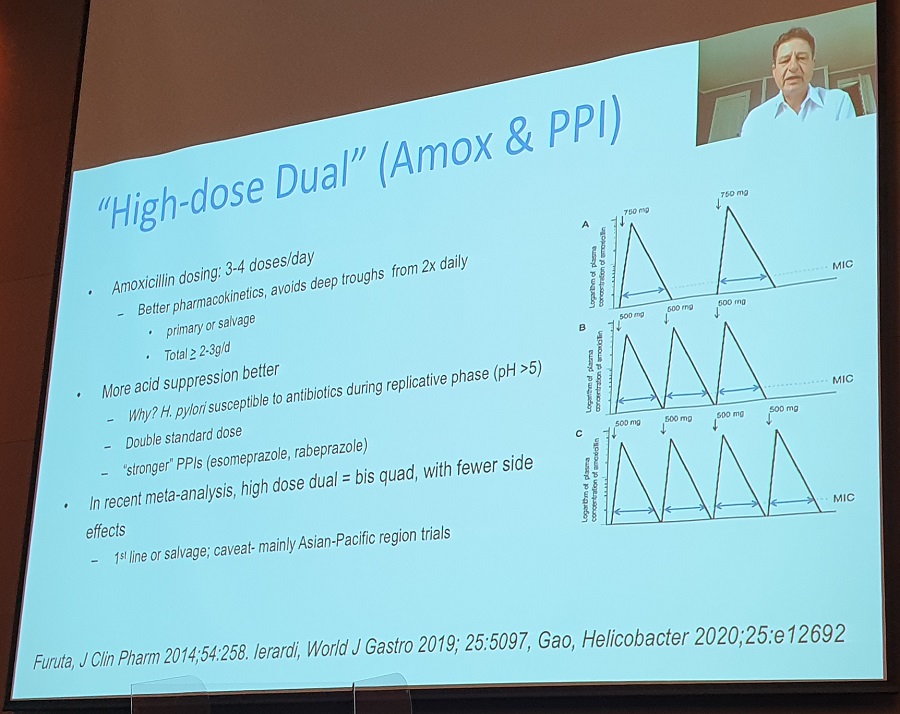
Hamamatsu 대학의 Furuta 교수는 PPI twice daily 포함 3제 요법의 제균율이 75% 수준인데 Vonoprazn 포함 제균요법의 제균율은 90% 수준이라고 발표하였습니다. PPI를 4회 투여하면 CYP2C19 rapid metabolizer에서도 충분한 정도의 위산 억제를 할 수 있으므로 vonoprazan allergic 환자에서는 PPI를 4회 사용하는 처방을 사용할 수 있다고 합니다.
국립대만대학의 Liou 교수
| Empirical therapy after two eradication failures |
| - Avoid empirical reuse of clarithromycin, metronidazole, and levofloxacin.
- Empirical reuse of amoxicilin and tetracyclin is allowed. - Rifabutin may be used ad rescue therapy after third-line treatment - Sitafloxacin is preferred if available. |
Second-line therapy (Steven F. Moss)
| Interchangeable use of PPIs based on relative potency (Clin Gastroenterol Hepatol 2018) | |
| Drug at lowest available dosage | Omeprazole equivalent |
| Pantoprazole 20 mg | 4.5 mg |
| Lansoprazole 15 mg | 13.5 mg |
| Omeprazole 20 mg | 20 mg |
| Esomeprazole 20 mg | 32 mg |
| Rabeprazole 20 mg | 36 mg |
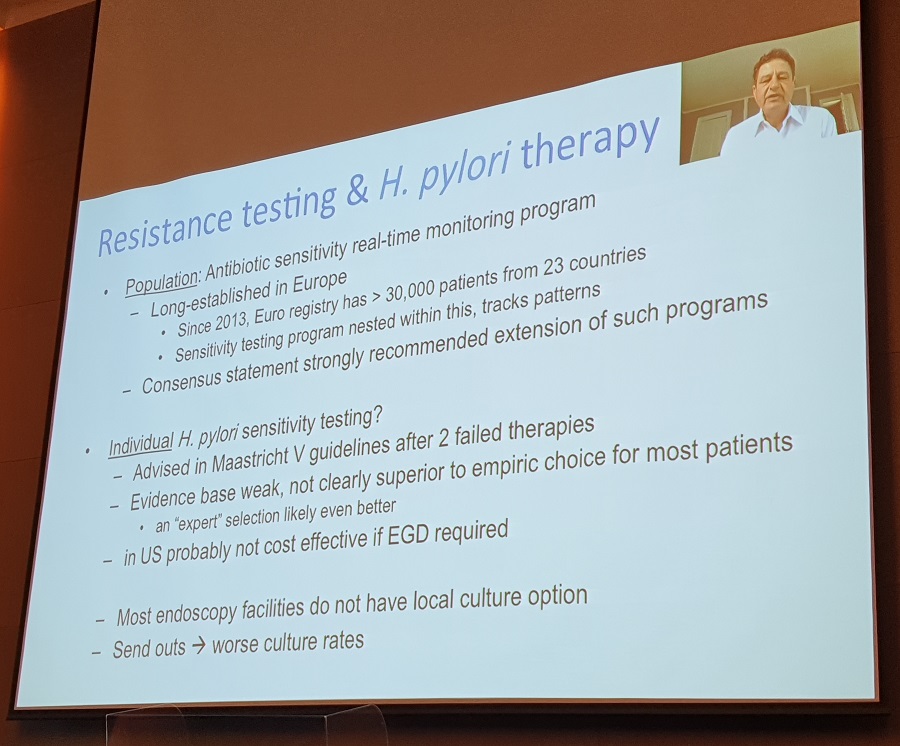
| Resistance testing and Hp therapy | |
| Population | Antibiotic sensitivity real-time monitoring program Long-established in Europe Since 2013, Euro registry has > 30,000 patients from 23 countries |
| Individual | Advised in Maastricht V guidelines after 2 failed therapies Evidence base weak, not clearly superior to empiric choice for most patients In US, probably not cost effective if EGD required Most endoscopy facilities do not have local culture option Send out → worse culture rates |
일본 헬리코박터학회 회장인 Koto 선생님: Only Japan keeps the triple therapy as the first-line eradication because VPZ can be used instead of PPI.
[헬리코박터 치료 약제 선택 가이드라인]
[이준행 런천 강의 - 제일약품 dexlansoprazole]
Thank you Mr chairman for your nice introduction.
I have no conflict of interest regarding today’s presentation.
The prevalence of GERD was already quite high in the early 2000.
And it is much higher these days. In the screening endoscopy setting, 10% have erosive esophagitis and 7% have reflux symptoms without mucosal breaks.
This is the average physiological pHs in the GI tract.
Today, I’d like to talk about Dexilant. Lansoprazole is a racemic mixture of R- and S-forms. Dexlansoprazole is the R-form of lansoprazole. The R-form has a slower clearance rate and correspondingly higher circulating plasma concentrations than the S-form
Dexilant capsules contains 2 types of granuldes, granule 1 and granule 2. Granule 1 begins releasing drug within an hour of dosing, and granule 2 provides a second release of drug several hours later. The enteric coating layer is different that granule 1 start to release at pH 5.5, and granule 2 start to lease at pH 6.7.
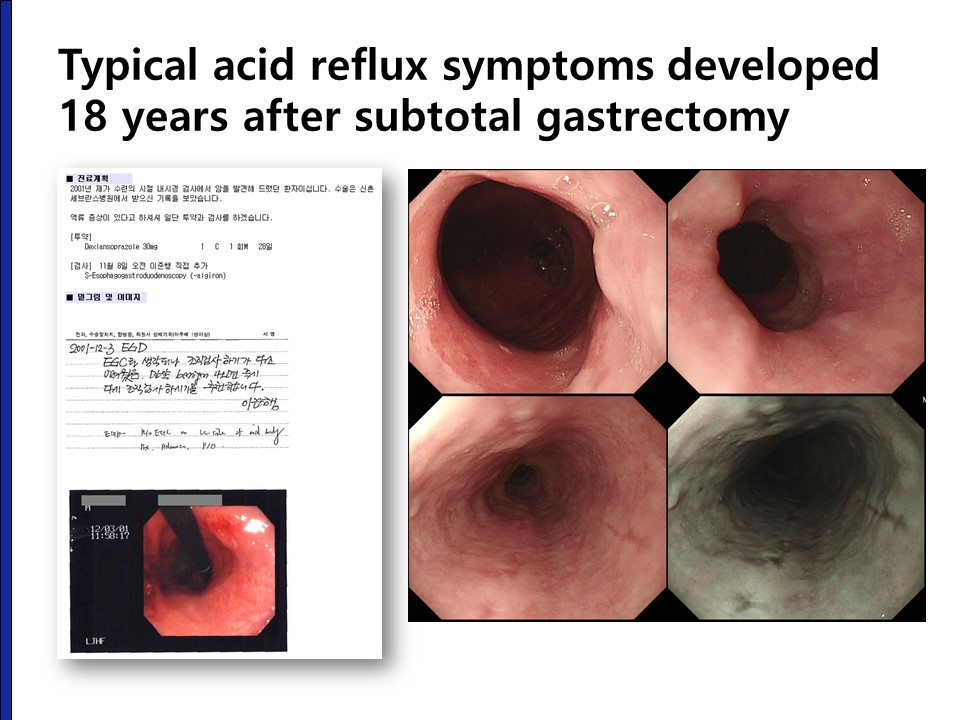
When I was a GI fellow, I found a cancer lesion during the screening endoscopy. 18 years later, she visited my outpatient clinic with typical acid reflux symptoms. In the mid to lower esophagus, there were multiple longitudinal mucosal breaks. The symptom responded very well to the dexlansoprazole.
Do you think our patients are happy enough?
Patients are not satisfied as much as doctors. As you can see in this questionnaire results, the proportion of very satisfied or well controlled is higher by doctors’ assessment (blue bar) than the patients’ assessment (green bar). I can say that some patients are not happy enough, and there are some areas of improvement.
I’d like to start by reviewing a very important survey performed in Asia.
Patients are still unhappy with reflux medications. Symptoms like pain and discomfort is relieved in about 75%, but almost same percent of patient said that reflux symptoms still have negative impact on their well being.
What is important for the ideal GERD medication? Asian patients hoped long-term safety, effect on nocturnal symptoms, and they wanted to enjoy daily activities.
So there are many areas of unmet needs, such as night-time heartburn, PPIs-dependence on food for efficacy, individual variation, poor symptom control in advanced grades of erosive esophagitis, and non-erosive reflux diseases. Dexilant is very useful for these areas.
From now on, I’d like to talk about management of night-time symptoms or breakthrough symptoms with Dexlilant.
The frequency of night-time symptoms are very high. Most GERD patients have both daytime and night-time symptoms.
This is a classic meta-analysis evaluating the PPI for the treatment of GERD. About 20 percent of patients did not respond to the PPI medication for 6 to 8 weeks. And the most common reason of conventional c PPI failure was nocturnal symptoms.
Before making a conclusion of PPI failure, careful evaluation of the patient’s symptom is very important. The patient had typical dysphagia and nocturnal symptoms, and there was no PPI response. What’s your impression?
In the endoscopy and barium esophagography, the findings were typical of achalasia.
And, endoscopic myotomy was done successfully.
As you can see clearly in the previously case, motility disorders should be considered in the evaluation of refractory heartburn.
Insomnia is not included in the previous table. In some patients, however, it is difficult to say which one is the main symptom, insomnia or nocturnal reflux. I recommended insomnia clinic for this elderly woman, and she was very happy about it.
Some refractory patients have severe hiatal hernia, which needs to be surgically corrected.
We humans mostly walk and work upright. It is difficult for the acid in the stomach to reflux into the esophagus when upright position. In the sleeping position, however, the acid in the stomach easily enter the esophagus because the esophagus and the stomach is the same level. This is one of the reason why reflux is so common in the evening.
Breakthrough symptom is not uncommon. 38 % answered that they have breakthrough symptoms.
Most patients with breakthrough symptoms experience them at night
Many physicians change from once daily to twice daily PPI dosing to control the nocturnal symptoms.
Only active proton pumps can secrete acid; however, not all pumps become activated. Only activated pumps can be blocked by PPIs.
One of the major limitations of the most PPI is that their half-life is very short.
As I mentioned earlier, Dexilant capsules contains 2 types of granuldes, granule 1 and granule 2. Granule 1 begins releasing drug within an hour of dosing, and granule 2 provides a second release of drug several hours later. The enteric coating layer is different that granule 1 start to release at pH 5.5, and granule 2 start to lease at pH 6.7.
The DDR formulation results in a plasma concentration-time profile with two distinct peaks. First peak by rapid release from granule 1, second peak by slow release from granule 2.
So the drug concentration curve have two peaks as shown in this slide.
The two peak plasma concentration is reflected by the intragastsric pH, showing rapid onset and longterm effect.
Clinically, patients in the Dexlansoprazole group experienced significantly fewer GERD-related sleep disturbances
Nights without GERD symptoms in the Dexilant group is more than 90%.
This is my case. He has been suffering nighttime symptoms even after medication. I changed into Dexilant and the night-time symptom was controlled. He is happy.
The next topic is that Dexilant can be taken after the meal.
Standard PPI should be taken before the breakfast. The problem here is that many Korean people don’t take breakfast.
In this survey, only 36% of Korean people take breakfast everyday. Without breakfast, when should I take the PPI?
In this study, irregular dietary intake was one of the risk factors for GERD. Odds ratio was 2.3.
This survey shows that more than half of patients take PPIs at suboptimal timing.
Dexilant can be taken at any time. This slide shows that the pH graph is almost the same regardless of PPI dosing time except for the very beginning. Fasting, 30 minutes after, 5 minutes before and 30 minutes before the diet.
The mean intragastric pH was almost the same for fasting dose, 30 minutes after, 5 minutes before and 30 minutes before the diet.
Final topic is the effect of Cytochrome2C19 polymorphism.
Many patients are taking clopidogrel and warfarin, and the main concern is the risk of bleeding.
Another concern is that clopidogrel is metabolized by cytochrome 2C19, and it has a cross reaction with some PPIs. Compared with omeprazole and esomeprazole, lansoprazole and dex-lansoprazole are not influenced by clopidogrel co-medication.
In addition, dex-lansoprazole was not significantly influenced by CYP2C19 polymorphism.
It also does not affect the anticoagulant activity of warfarin. Drug-drug interaction seem to be small, so can be safely used in patients taking multiple medications.
Ladies and gentlemen. I’d like to conclude this luncheon lecture by saying that Dexilant is a strong long-acting PPI with dual delayed release (DDR) technology. It has excellent control of breakthrough symptoms including night-time heartburn, and can be taken after the meal, and safely used with clopidogrel and warfarin.
![]() [References]
[References]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.