 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [항암요법을 하지 않는 의사를 위한 위암항암치료. Chemotherapy for gastric cancer] - 終
[항암요법을 하지 않는 의사를 위한 위암항암치료. Chemotherapy for gastric cancer] - 終
[알림] 위암항암치료는 매우 빠르게 발전하는 분야입니다. 비전문가로서 최근 경향을 따라잡기 위하여 노력하고 그 결과를 아래에 요약하였지만 아직 한참 부족합니다. 최신 치료에 대해서는 전문가와 상의하시기 바랍니다.
1. Introduction
2. Neoadjuvant chemotherapy 선행항암요법
3. Adjuvant chemotherapy 보조항암요법
4. Palliative systemic therapy 고식적 항암요법
5. HER2-positive gastric cancer - Trastuzumab deruxtecan
6. Immunotherapy 면역치료
7. Ramucirumab (VEGFR2 inhibitor)
8. Claudin 18.2
10. Conversion surgery 전환 수술
11. Symposiums
12. FAQs
13. References
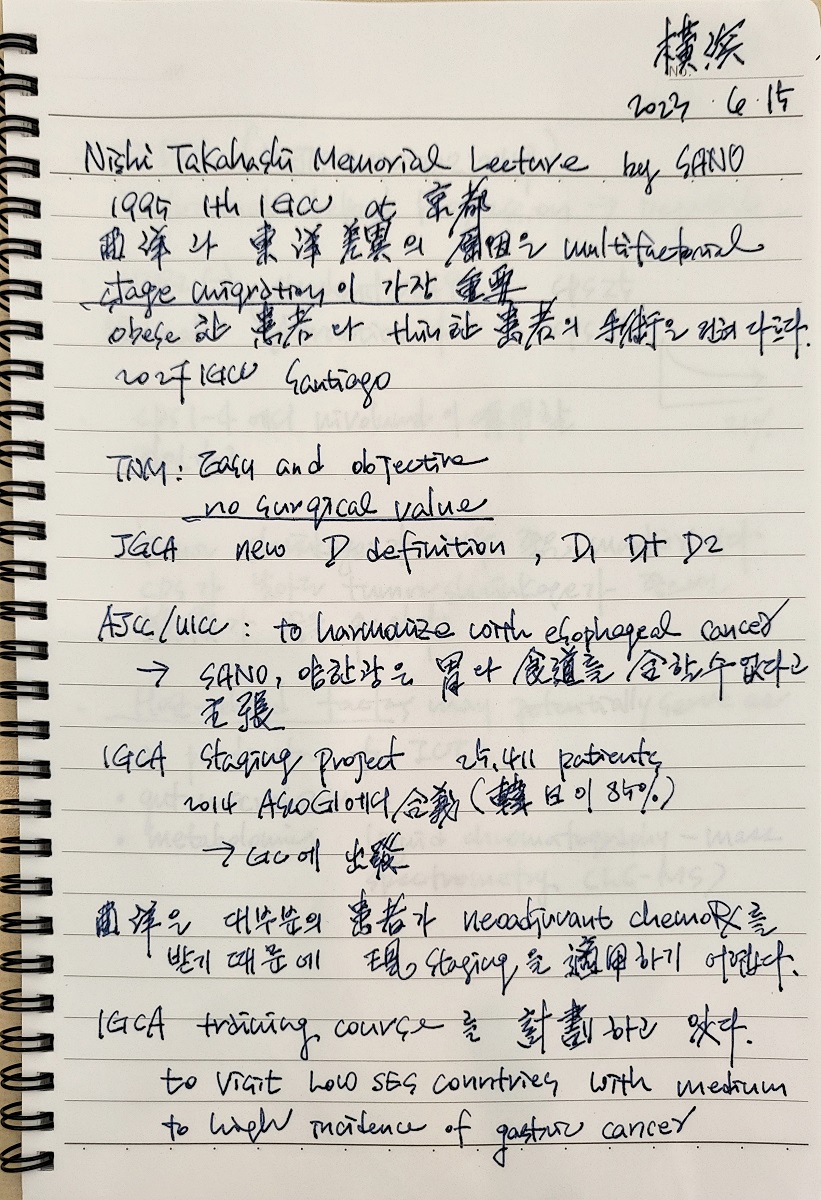
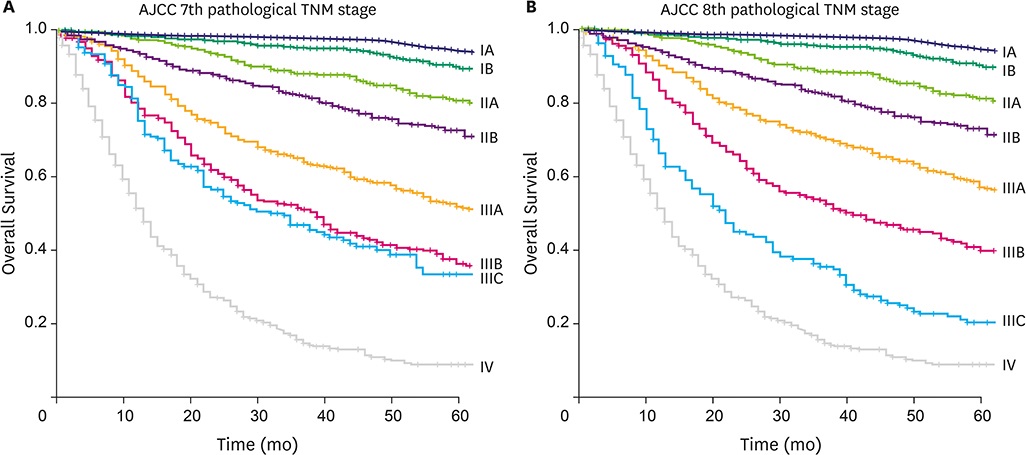
AJCC 8판 위암 병기
2024-9-27 KINGCA. 라선영 교수님 강의 중에서
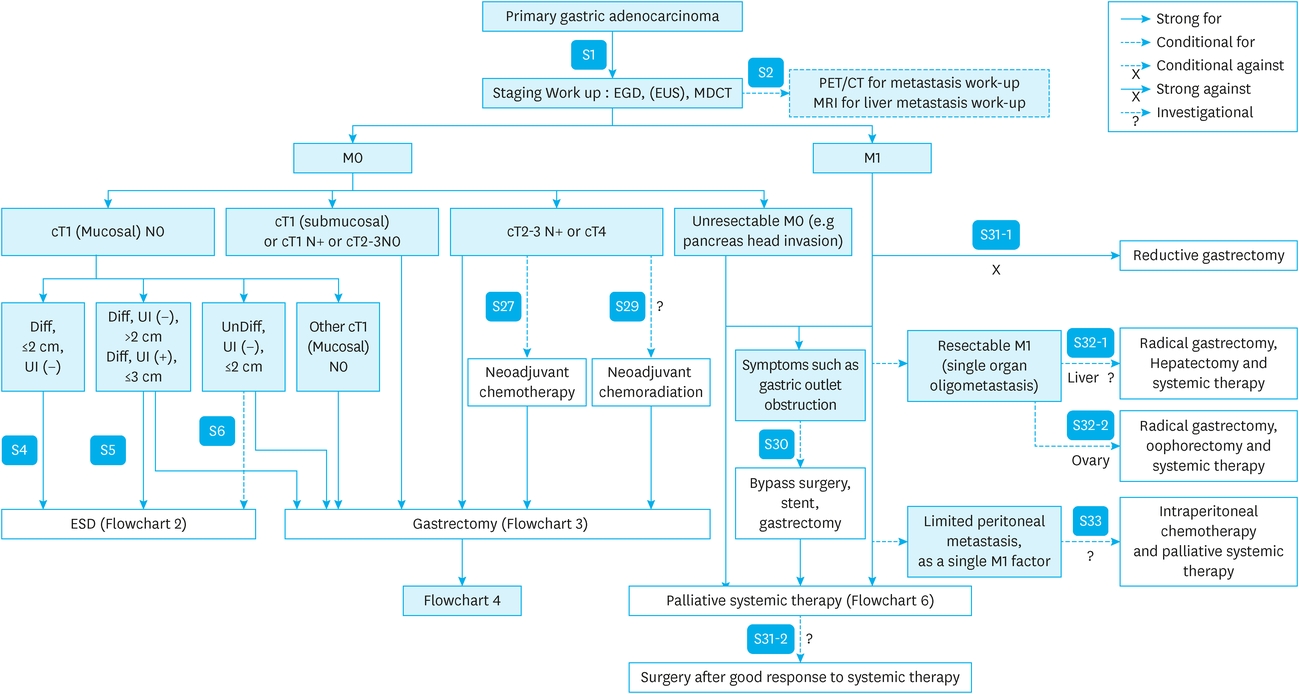
KGCA guideline 2024 neoadjuvant, adjuvant, first-line palliative systemic therapy statements
![]() 1. Introduction
1. Introduction
위암 항암치료는 flow 상 5단계로 생각하고 있습니다.
| Steps of systemic therapy |
|
![]() 2. Neoadjuvant chemotherapy (NACT) 선행항암요법
2. Neoadjuvant chemotherapy (NACT) 선행항암요법
요약: 서양에서는 neoadjuvant chemotherapy 후 수술이 보편적이지만, 우리나라와 일본에서는 대부분 upfront surgery후 adjuvant chemotherapy를 합니다. 우리나라와 일본에서 (1) early detection이 많고, (2) surgeon, endoscopist의 실력이 좋고, (3) upfront surgery후 항암치료를 하는 기존 치료법의 survival이 좋았기 때문입니다. 위암 clinical staging이 충분히 정확하지 않다는 점, 즉 항암치료가 필요하지 않은 환자가 항암치료를 받는 경우가 있다는 점도 고려되어야 합니다. 국내에서 DOS regimen을 이용한 연구가 있었지만 국제적으로는 FLOT regimen이 사용됩니다. 면역항암제의 도입으로 FLOT + IO (immuno-oncology)가 표준으로 떠오르고 있습니다.
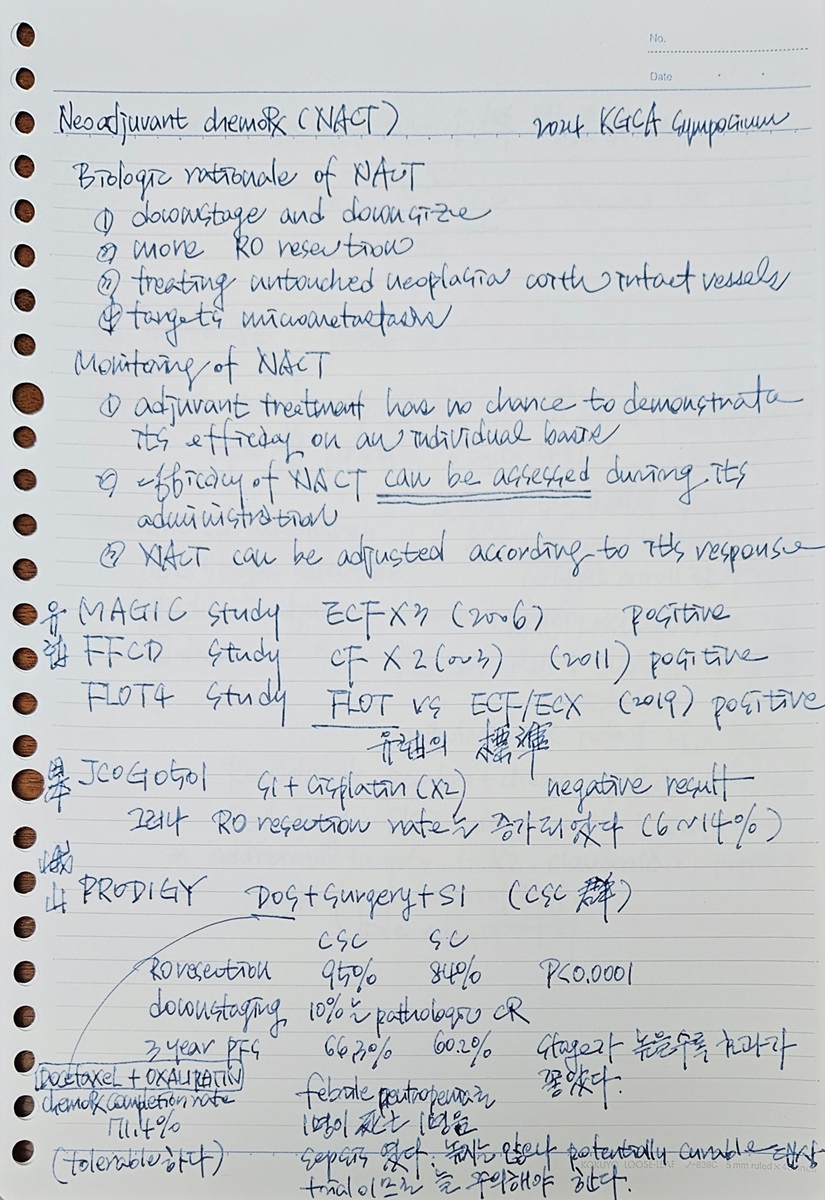
| Rationale for neoadjuvant chemotherapy | |
| Biologic rationale | Monitoring |
| Downstage and downsize More R0 resection Advantage of treating an untouched neoplasia with intact vessels and without fibrotic remodeling of the tumor bed following surgery Targets micrometastases | Adjuvant treatment has no chance to demonstrate its efficacy on an individual basis (no indicating lesions) The efficacy of NACT can be assed during its administration NACT can be adjusted according to patient response |
서양에서는 대부분의 위암 환자가 수술 전 항암치료(neoadjuvant chemotherapy)를 받고 있습니다. 그러나 동양에서는 수술 전 항암치료를 받는 위암 환자는 거의 찾아보기 어렵습니다. 2021년 발표된 일본의 JCOG0501 trial에서 negative result가 나온 것이 영향을 미친 것으로 생각됩니다.
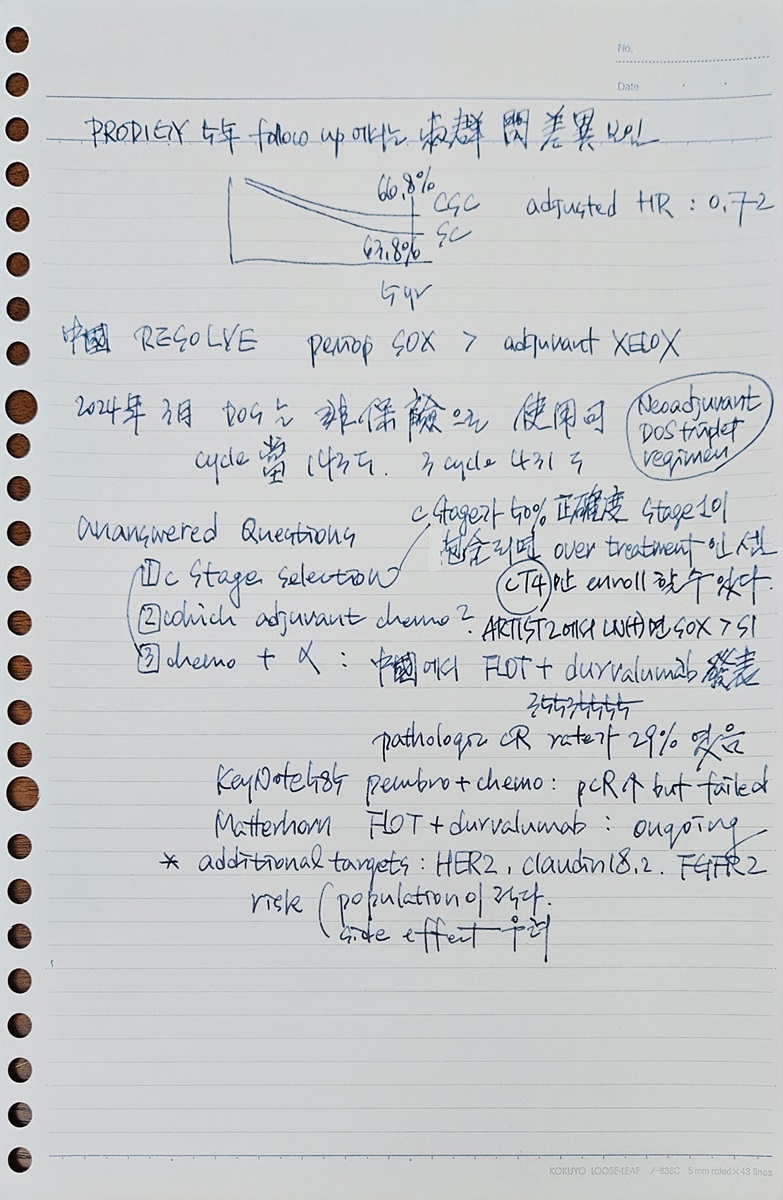
우리나라의 PRODIGY 연구(JCO 2021, 청년의사 2023)와 중국의 RESOLVE 연구(Lancet Oncol 2021)가 발표되어 2022 KGCA 가이드라인에 언급되었지만 아직 임상에 널리 도입되지 못했습니다. 그러나 이미 2022 KGCA 가이드라인에 언급되었고 보험도 됩니다. 임상의사의 판단에 따라 우리나라에서도 NACT를 사용할 수 있는 환경은 마련되었습니다.
PRODIGY. JCO 2021 3년 progression free survival이 66% 대 60%로 의미있는 차이를 보였습니다. 71.4%가 정해진 항암치료를 마칠 수 있어서 tolerable 한 편이었지만, 2명이 neoadjuvant chemotherapy 관련 사망을 보였습니다. 비록 사망자는 매우 적었지만 potentially curable disease에 대한 치료에서 수술 전 사망자가 있다는 것은 늘 걱정입니다. Stage 1 환자가 포함되면 NACT가 overtreatment인 셈이고, NACT 후 수술 시 peritoneal seeding인 것으로 나오면 곤란한 점이 있으므로 staging이 매우 중요합니다. PRODIGY 연구의 장기 추적관찰 시 5년부터 10년 사이 survival benefit을 보였다고 합니다.
PRODIGY 연구 PI 아산병원 종양내과 김형돈 교수님 강의. 2022-8-26. AMC symposium
2022년 KGCA 가이드라인에 일부 환자에서 NACT를 사용할 수 있는 것으로 추천되었습니다. Statement 28: Neoadjuvant chemotherapy as part of perioperative chemotherapy can be considered for patients with resectable locally advanced gastric cancer. 아직은 비급여입니다. NACT 후 수술에서 stage가 1으로 나오면 항암치료가 보험 급여가 되는지 불명확하지만 수술 전 stage를 존중하여 adjuvant chemotherapy가 가능할 것 같습니다.
2024년 3월 대한위암학회 연수강좌에서 류민희 교수님께서 매우 잘 정리된 강의를 해 주셨습니다 (Past, present, and future of neoadjuvant chemotherapy in Korea). 현재의 unanswered question은 (1) patient selection (cStage T4?), (2) adjuvant chemotherapy (stage가 높으면 S1보다 XELOX), (3) chemo+alpha라고 요약하셨습니다.
ICI를 추가하는 것에 대한 관심이 높습니다. Pembronizumab을 더한 Keynote-585은 negative 결과였습니다. 반면 FLOT에 durvalumab을 더한 중국의 Matterhorn 연구(NEJM 2025)는 positive 결과였습니다. 바야흐로 neoadjuvant 영역에서 chemotherapy + alpha 시대가 열리고 있는 것입니다.
HER2, claudin18.2, FGFR2 등에 대한 약을 추가하는 것에 대한 자료는 부족합니다.
2025년 11월 분당서울대병원 위암 single topic symposium에서 분당 서울대병원 혈종 김진원 교수님의 강의 요약입니다. FLOT + durvalumab이 국제표준으로 언급되었습니다.

In the west (world-wide), FLOT + durvalumab in the standard therapy
Perioperative chemotherapy and curative resection in Asia
2025년 12월 현재까지 해결되지 않은 많은 어려움이 있습니다. Durvalumab을 perioperative하게 사용한 경우 재발하였을 때 nivolumab이나 pembronizumab을 사용할 수 없다는 점도 그 중 하나입니다. 한 IO를 사용했는데 재발한 상황에서 다른 IO를 사용할 근거가 부족하다고 해석되기 때문입니다.
항암치료의 regimen은 빠르게 바뀌고 있어서 항상 다시 확인해야 합니다. 2026년 7월 선행항암요법 protocol입니다.
2026-7-11
[Radiologic evaluation before and after Neoadjuvant chemotherapy (NACT)] 2024-3-23 KGCA 심포지엄. 국립암센터 김수진 교수님. 다시 보기
Exclusion of peritoneal seeding: Ascites, irregular peritoneal thickening, soft tissue stranding in intra-abdominal fat, Soft tissue nodule/plaque: most reliable, , omental cake
Unexpedted, intraoperative proven peritoneal seeding: >cT3, T4, Borrmann type 3 or 4, >5.2-8cm, GC/AW, LNE, Praque, ascites
RECIST v 1.1은 irregular shaped GI tract tumor에서는 적당하지 않습니다. ycTNM restaging은 항암치료 전 staging에 비하여 전반적으로 성적이 낮습니다. CT or MR volumetry가 더 유용합니다. 이를 위하여 protocol이 통일되어 있어야 합니다.
[Biomarkers for NACT in gastric cancer] 2024-3-23 KGCA 심포지엄. 가톨릭의대 이성학 교수님. 다시 보기
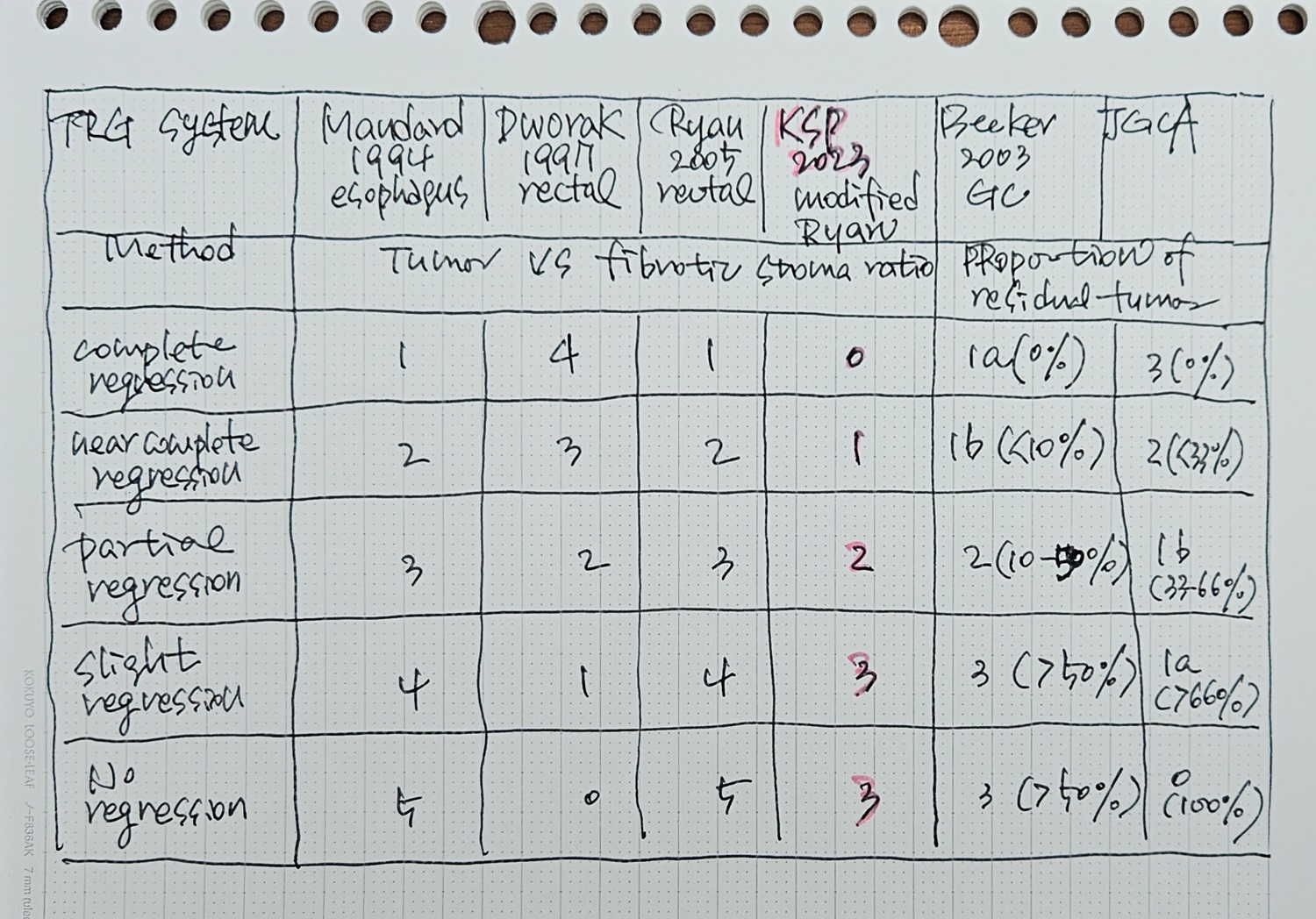
TRG (tumor regression grade): tumor bed에서 남아있는 residual tumor의 비율을 측정하는 방법과 residual tumor와 fibrosis를 고려한 방법이 있습니다.
한국 병리학회에서 제시한 방법이 있습니다. (JTPM 2023) It is a descriptive fourtier system that evaluates residual cancer rather than fibrosis as none, single cells or rare small groups, more than single cells but evident tumor response, and extensive residual cancer cells.
- Grade 0: Complete response (no viable cancer cells)
- Grade 1: Near complete response (single cells or rare small groups of cancer cells)
- Grade 2: Partial response (residual cancer with evident tumor regression, but more than single cells or rare small groups of cancer cells)
- Grade 3: Poor or no resonse
여러 TRG를 비교하면 아래 표와 같습니다. 무척 헷갈립니다.
[Surgical approach after NACT] 2024-3-23 KGCA 심포지엄. 연세대학교 김형일 교수님. 다시 보기
NACT 후 수술에서 합병증이 증가하지 않는다는 것을 보여준 김형일 교수님의 인상적인 슬라이드. 딱 3개 논문 빼고 나머지는 모두 차이가 없었다고 합니다.
[Neoadjuvant chemotherapy 교육자료]
헬리코박터학회 2026-5 (PDF 0.5M)
![]() 3. Adjuvant chemotherapy. 보조항암요법
3. Adjuvant chemotherapy. 보조항암요법
Indication: stage 2 or more (stage 1은 해당하지 않음)
일반적인 표준 치료: XELOX - Oral pyrimidine-based doublet regimens can be a more favorable treatment option than S-1 alone for pathological stage II with positive LN or stage III gastric cancer.
위암 수술 후 보조항암요법. 홍정용 교수님.
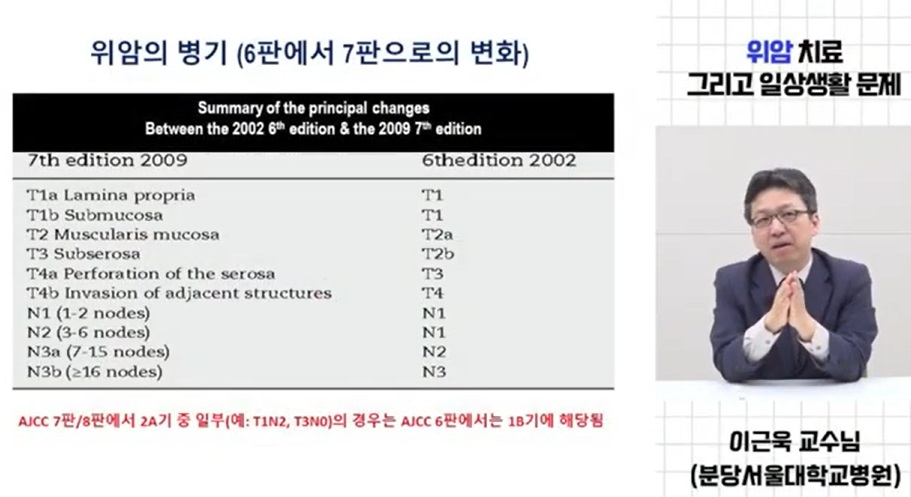
ACTS-GC (Sakuramuto NEJM 2007)와 CLASSIC (XELOX regimen: capecitabine + oxaliplatin) (Bang Lancet 2012)의 비교 - KBDCA 이근욱/안상훈 webinar
CLASSIC 연구 5년 결과(Noh Lancet Oncol 2014)에서 AJCC 6판 병기별 보조항암치료의 효과 - KBDCA 이근욱/안상훈 webinar
2022 KGCA guideline Statement 23
2022 KGCA guideline Statement 23 Forest flot
AJCC staging이 바뀌면서 병기가 달라진 일부 환자에서 보조항암요법의 근거가 명확하지 않은 환자군이 생겼습니다. 병기 변화에 따라 과거 연구에서도 빠지고 새 연구에서도 빠지고... It should be noted that there is currently no evidence to support the use of adjuvant chemotherapy for patients who fall into the category of stage IB by the AJCC 6th edition but stage IIA by the AJCC 7th and 8th editions (pT1N2M0 and pT3N0M0). (2022 KGCA guideline p52)
2024년 현재 우리나라에서 adjuvant 치료는 doublet chemotherapy가 표준입니다 (예. XELOX). Palliative first-line 치료에서 nivolumab의 효과가 입증되면서 adjuvant chemotherapy에 nivolumab을 더하는 것이 효과가 있는지 다국가 전향적 연구가 진행되었습니다. 아쉽게도 결과는 negative였습니다 (ATTRACTION-5 연구. 강윤구 Lancet Gastroenterol Hepatol 2024). 결론을 옮깁니다. "The results of this trial do not support the addition of nivolumab to postoperative adjuvant therapy for patients with untreated, locally advanced, resectable gastric or GEJ cancer."
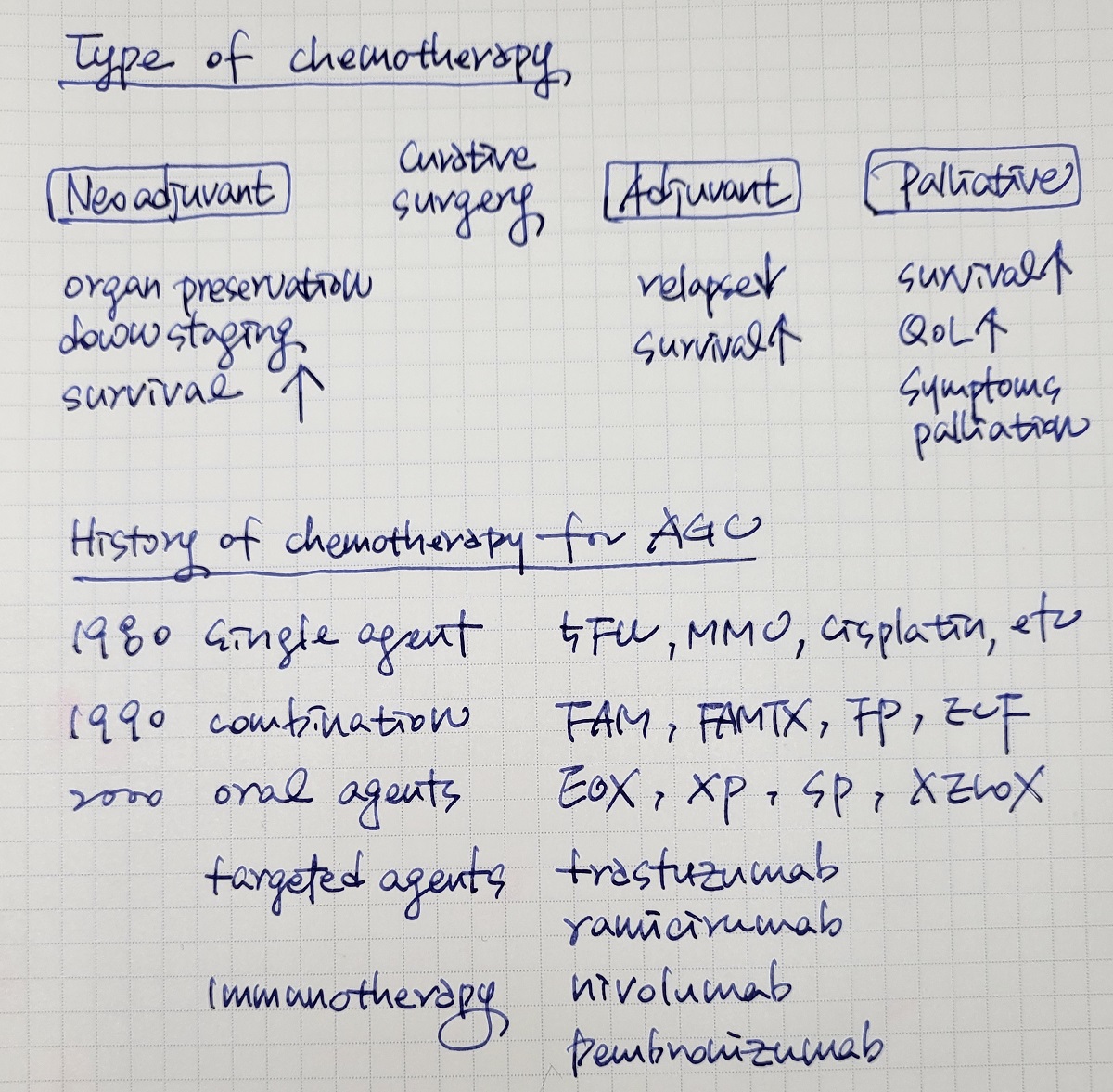
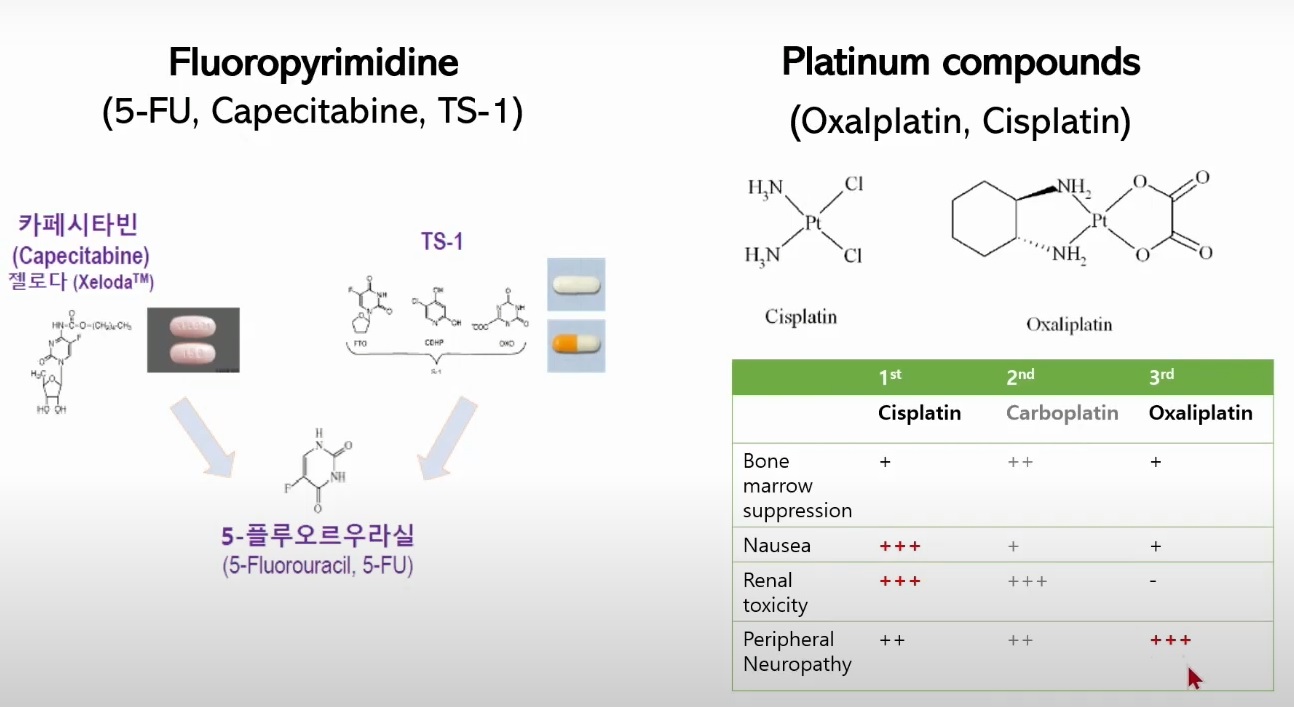
* 참고: 5-fluorouracil (5-FU) 경구제제
![]() 4. Palliative systemic therapy. 고식적 항암요법
4. Palliative systemic therapy. 고식적 항암요법
Representative case in 2025. There was a huge ulceroinfiltrative mass lesion on the lesser curvature side of the antrum. The histology was poorly differentiated tubular adenocarcinoma with PD-L1 CPS 90, HER2 positive, claudin18 negative and intact MLH1. In the CT scan, gastric wall was thickened with hepatopancreatic invasion with multiple perigastric nodes and a few small metastatic nodules in the liver. In the PET/CT scan, hepatic lesions looked more prominent than CT. It’s a cT4bN2+M1 case, and the initial regimen was XELOX with Opdivo.
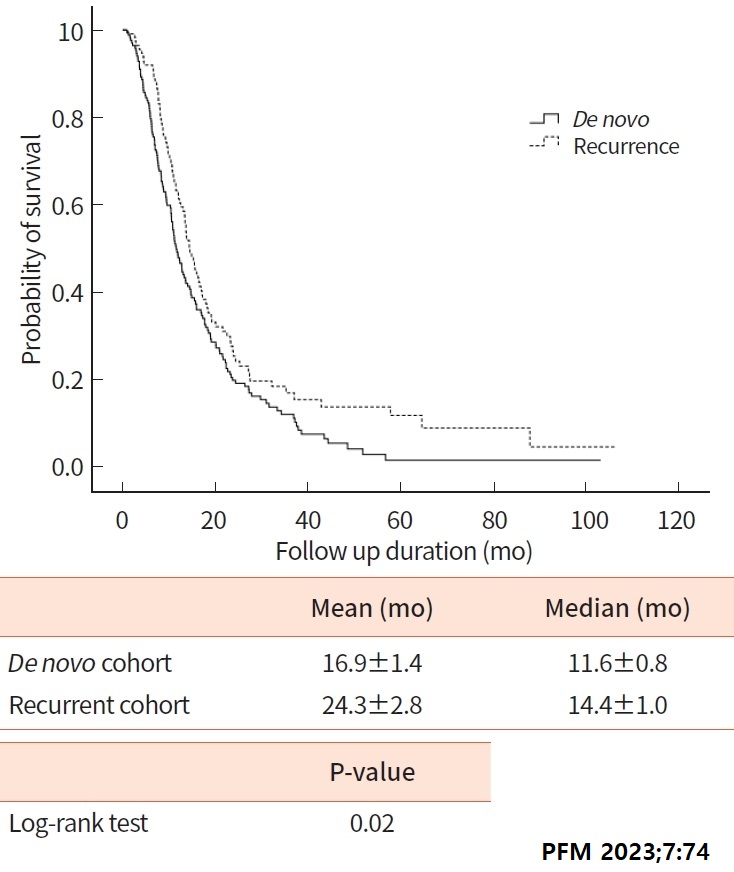
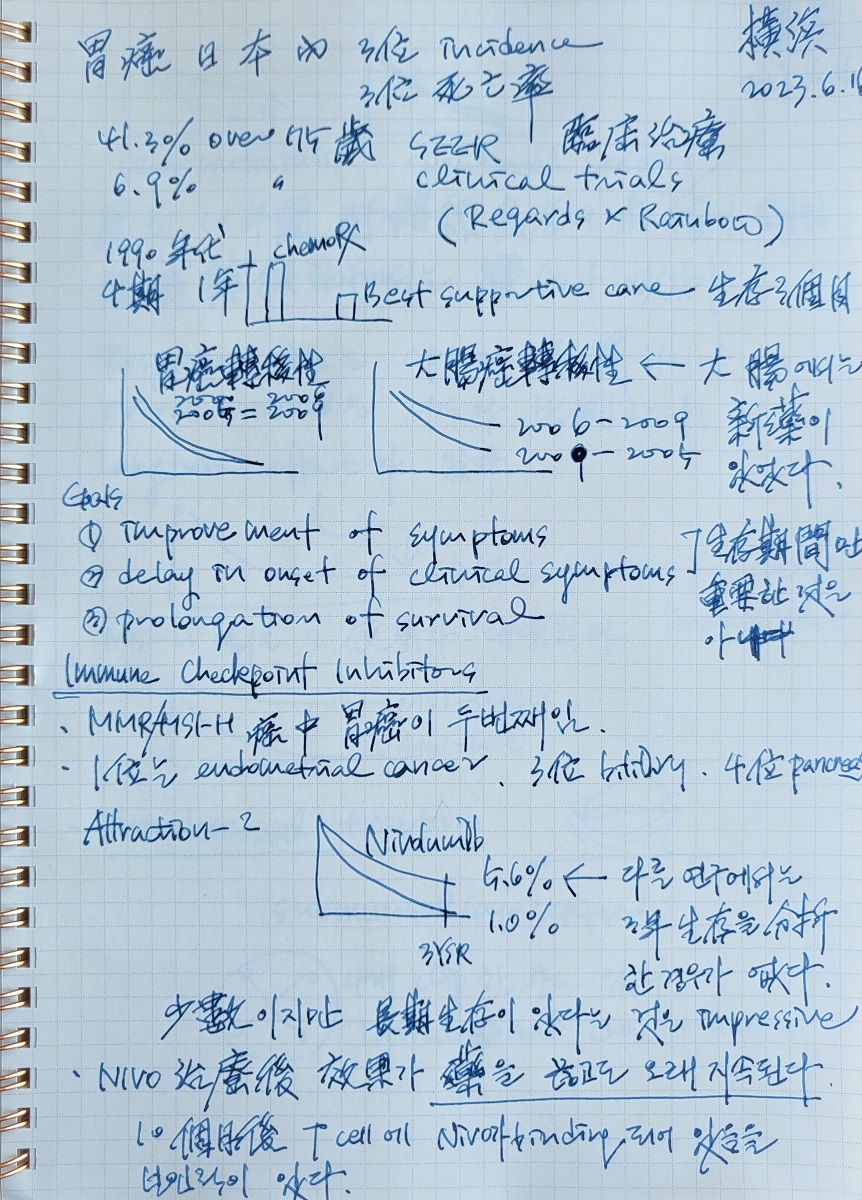
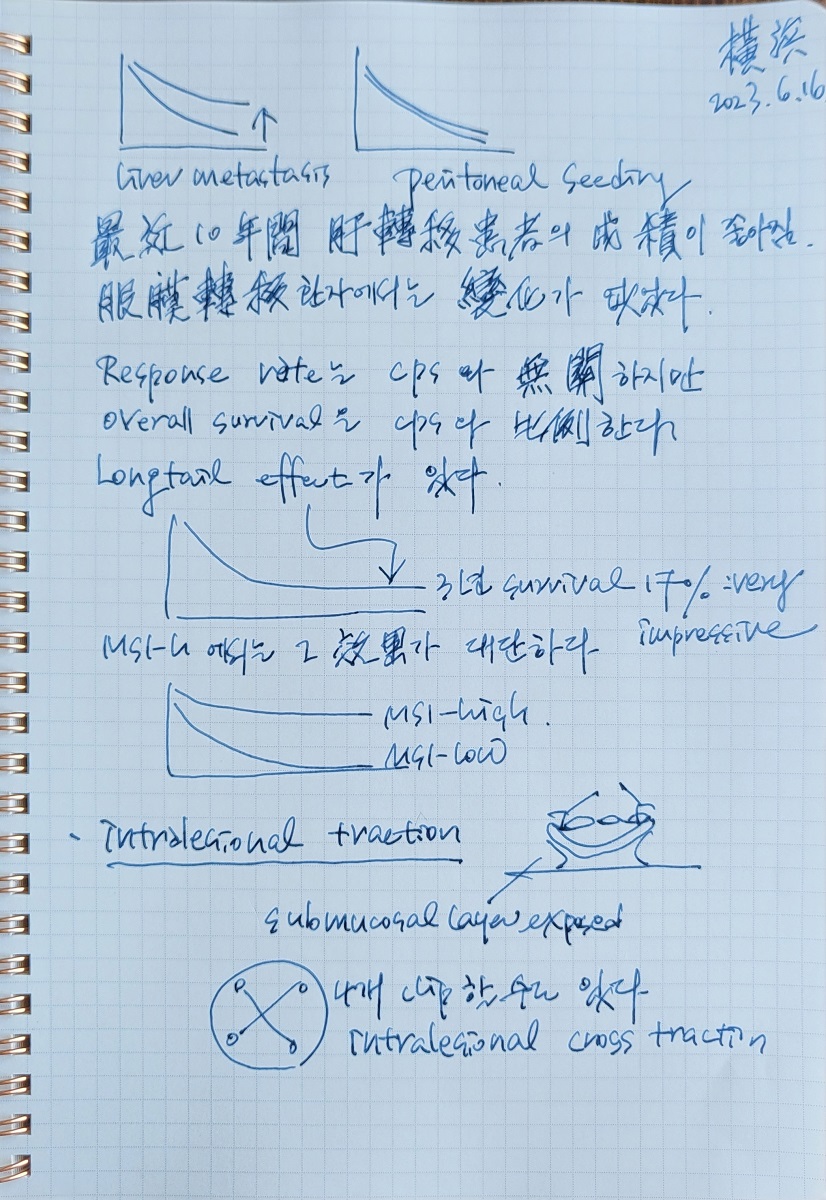
2017년 Cochrane Review에 의하면 best supportive care에 비한 항암치료의 survival benefit는 6.7개월이었습니다 (Cochrane Database Syst Rev 2017). 삼성창원병원에서 de novo stage IV 위암과 recurrent stage IV 위암의 survival을 비교하여 발표하였습니다. 2012년부터 2022년에 enroll된 환자들인데 면역항암제가 도입되기 이전 우리나라의 평균적인 4기 위암 치료 성적을 보여주고 있다고 생각되어 소개합니다. 면역항암제가 도입된 이후에는 성적이 많이 좋아졌습니다.
위암도 molecular phenotype을 나누고 biomarker에 따라 치료하는 시대가 오고 있습니다.
Nakamura. Nat Rev Clin Oncol 2021
Nakamura. Nat Rev Clin Oncol 2021
Nakamura. Nat Rev Clin Oncol 2021
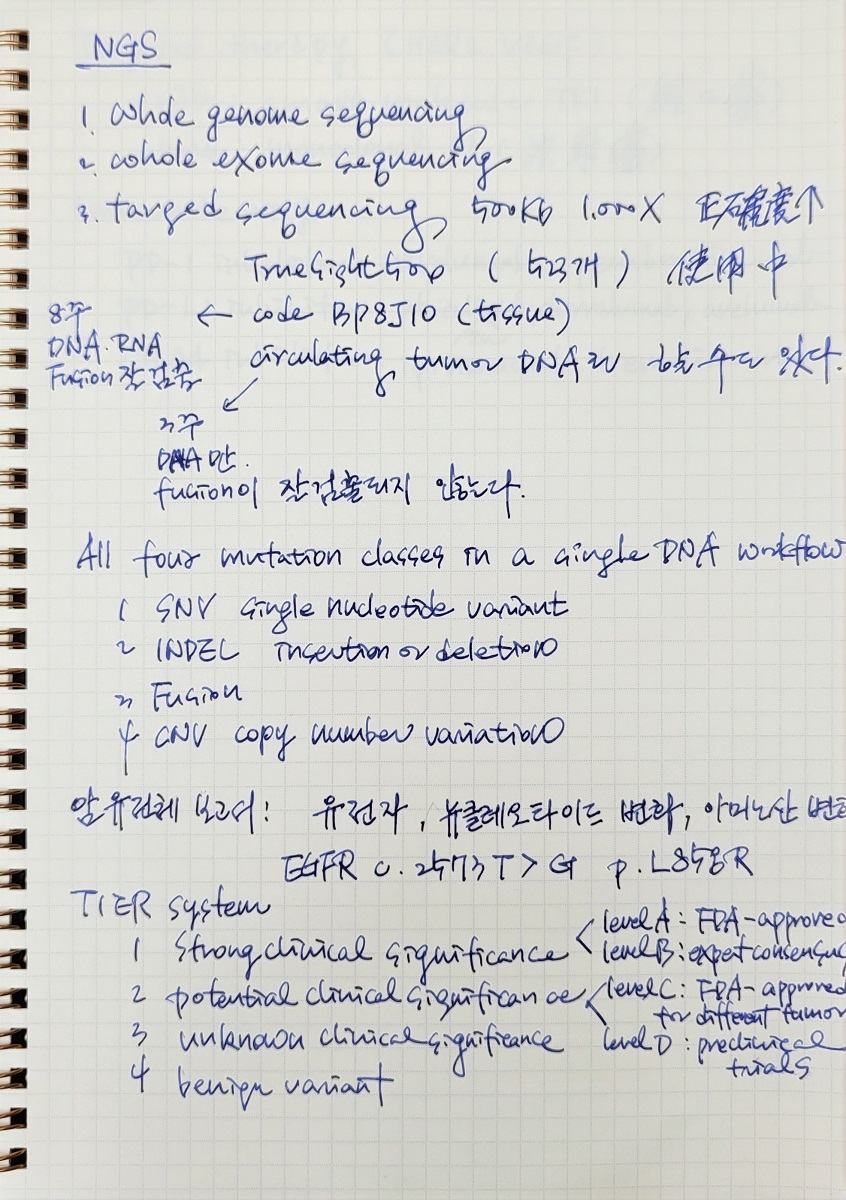
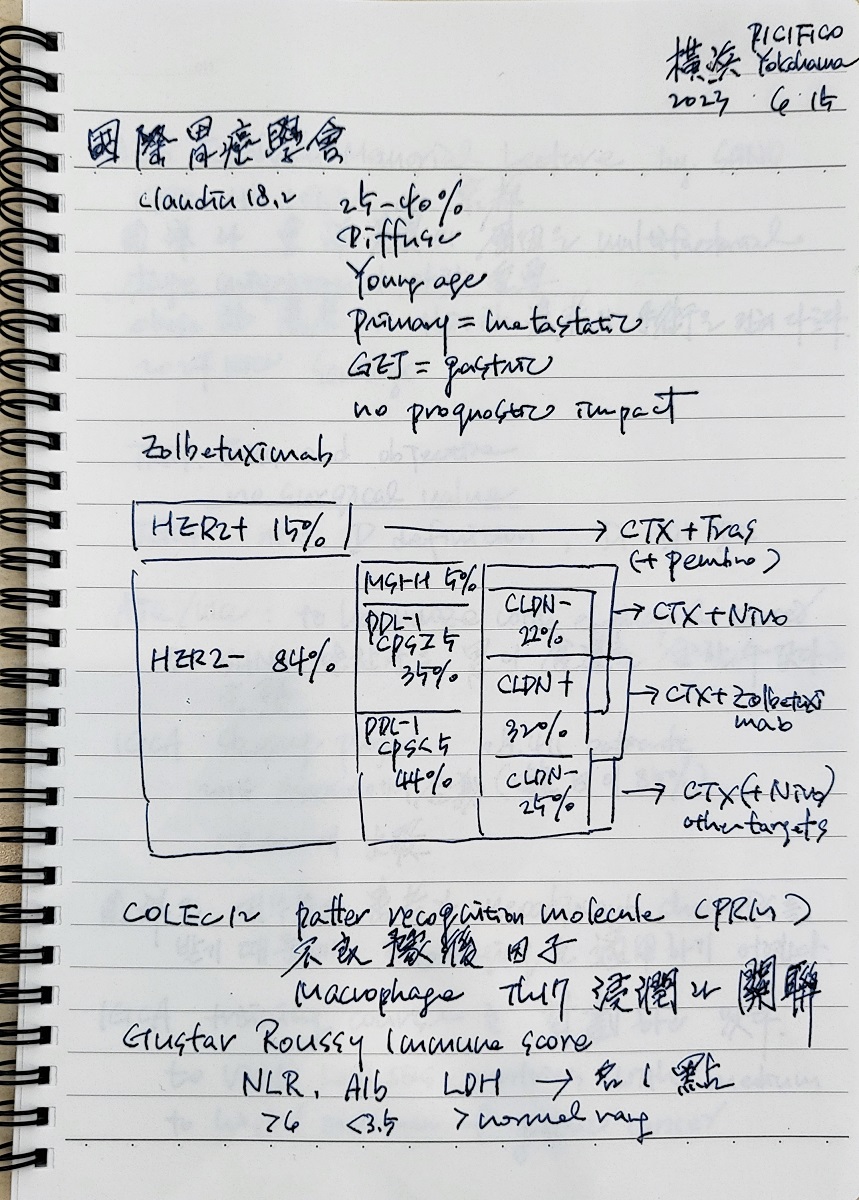
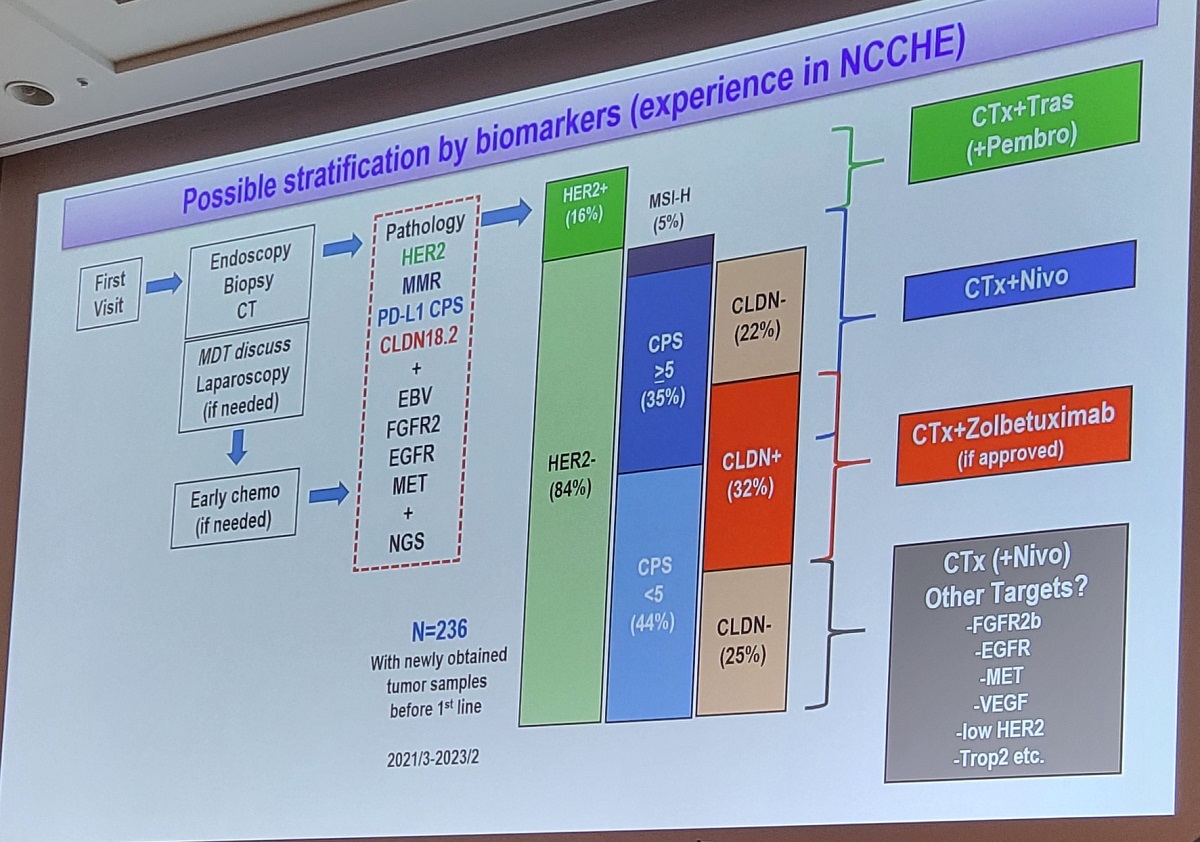
위암 환자의 첫 내시경 조직검사를 처방할 때 위암의 subtype 분류와 추가 치료를 위하여 몇 가지 marker 검사를 하고 있습니다. 내시경실에서는 일반 조직검사(H&E 염색)까지만 처방하고 면역염색은 병리과에서 필요한 것들을 추가 입력하고 있습니다. 2025년 8월 시점에서 흔히 적용하고 있는 c-erbB-2 (HER-2, 처방코드 BP3A12), MLH1 (처방코드 BP3C25), PD-L1 28-8 (처방코드 BP3E06), claudin 18.2 입니다. 필요한 경우 EBV 등의 검사를 추가합니다. 일반적으로 HER2 양성이 15%, Claudin 18.2 양성이 30%, PD-L1 CPS >= 5가 35% 정도입니다. 가능하면 NGS (next generation sequencing) 검사를 통하여 보다 많은 정보를 획득하여 다양한 가능성을 탐색하고 있습니다.
위암에서 여러 marker의 양성률
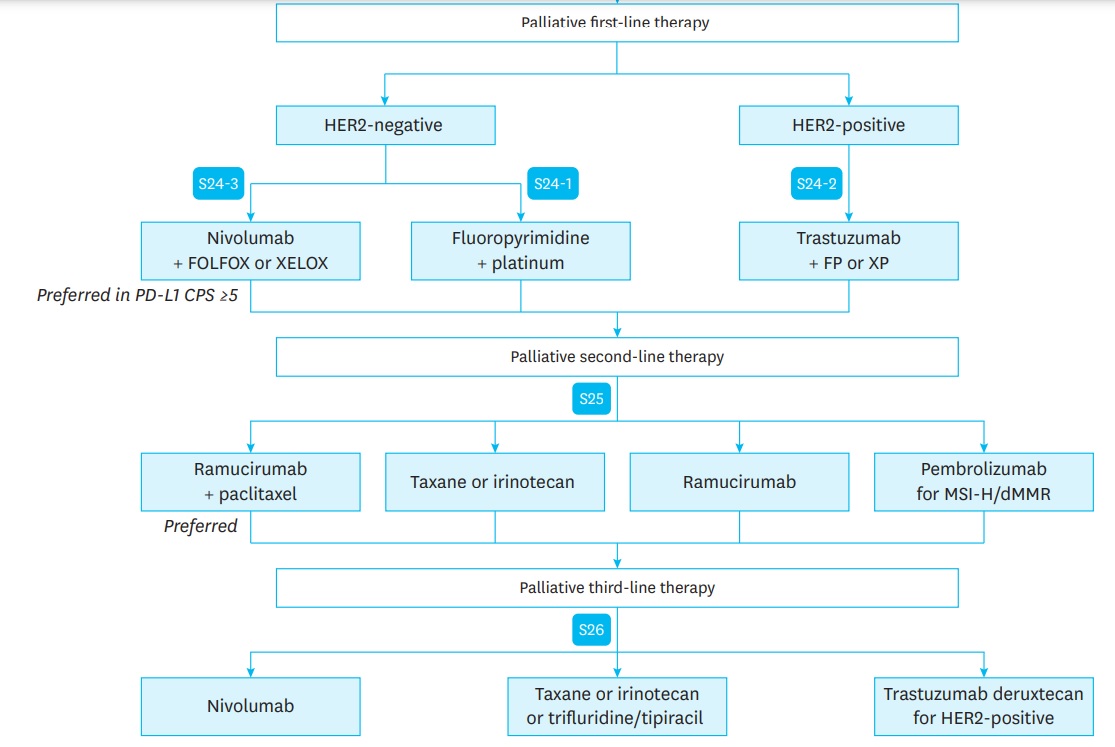
2022년 대한위암학회 가이드라인의 systemic therapy에 비하여 2024년 대한위암학회 가이드라인 systemic therapy는 상당한 발전이 있었습니다. HER-2 negative에서는 2022년에는 nivolumab만 있었는데 2024년에는 pembronizumab과 zolbetuximab이 추가되었습니다. HER-2 positive에서는 pembronizumab을 쓸 수 있는 부분이 추가되었습니다.
KGCA guideline 2024의 first-line systemic therapy
KGCA guideline 2024의 second/third-line systemic therapy
![]() 5. HER2 positive gastric cancer
5. HER2 positive gastric cancer
HER2는 4기 위암의 15%에서 양성이며 EGJ cancer에서 조금 더 흔합니다.
c-erB-2 positive (+)
방영주 교수님의 ToGA trial (Bang. Lancet 2010) 이후 HER2 양성 위암의 palliative chemotherapy는 trastuzumab 기반으로 진행되고 있습니다.
현재 사용하고 있는 IHC 기준을 적용한 분석
2022년 대한위암학회 가이드라인 Statement 24-2는 아래와 같습니다.
| Statement 24-2: Palliative first-line trastuzumab combined with capecitabine or FU plus cisplatin is recommended in patients with HER2 IHC 3+ or IHC 2+ and ISH-positive advanced gastric cancer (evidence: high, recommendation: strong for). [참고] 3+면 바로 사용하고 2+면 추가 검사를 한 후 사용한다는 의미입니다. |
![]() [Trastuzumab deruxtecan] 항체약물복합제 antibody-drug conjugate (ADC)
[Trastuzumab deruxtecan] 항체약물복합제 antibody-drug conjugate (ADC)
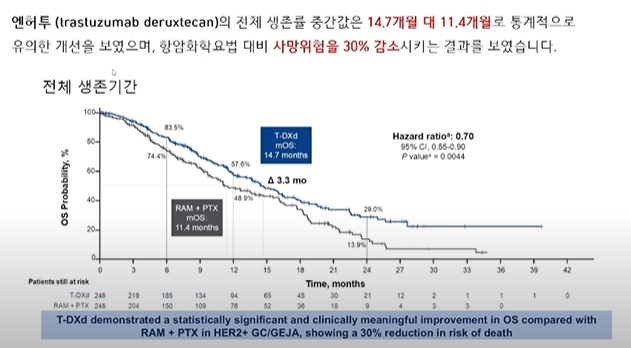
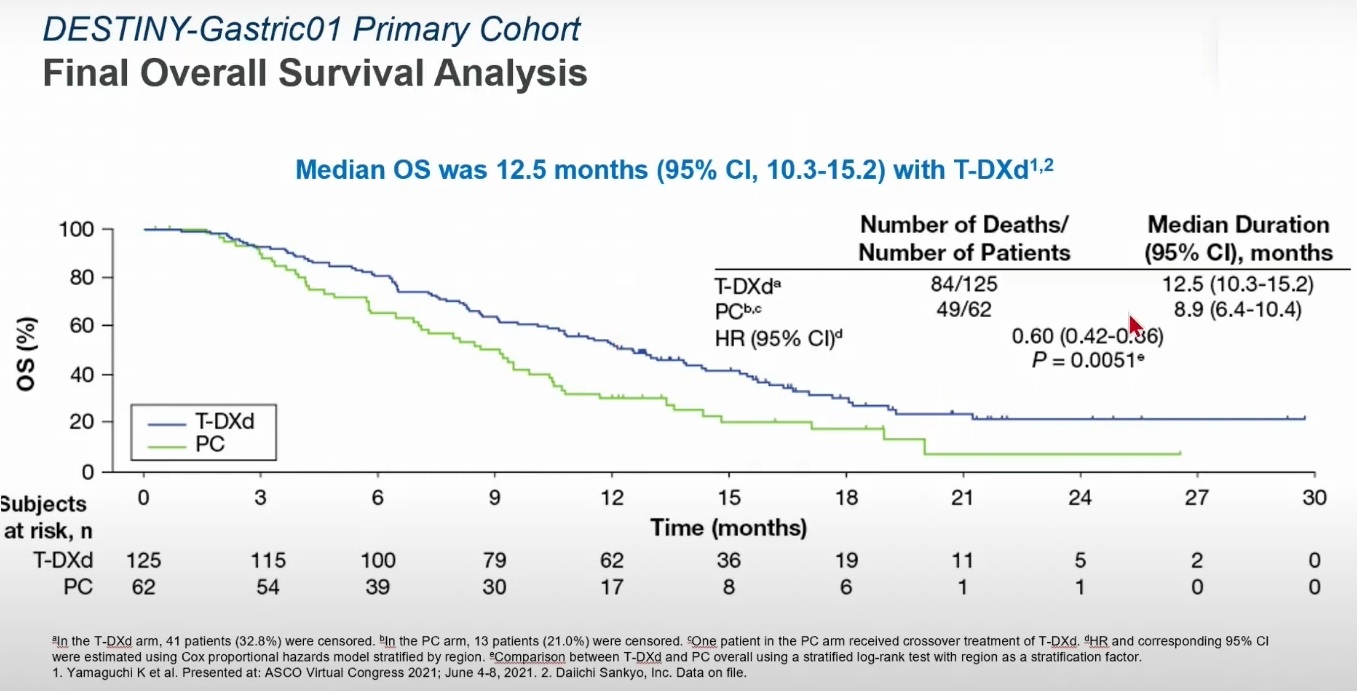
Topoisomeraze 1 inhibitor를 붙인 antibody-drug congugate (ADC) trastuzumab deruxtecan (T-Dxd, ENHERTU, 엔허투)이 HER2 양성 위암에서 사용될 수 있습니다 (Kotani and Shitara. Ther Adv Med Oncol 2021). 2024년 4월부터 HER2 양성 진행성/전이성 위암 3차 이상 치료에 건강보험 급여적용이 가능해졌습니다 (관련뉴스). 1차 또는 2차 치료에 대한 효과도 기대되어 임상 연구가 진행되고 있습니다.
trastuzumab deruxtecan의 구조 (www.biochempeg.com)
trastuzumab deruxtecan의 구조 (www.adcreview.com)
HER2 양성 위암은 trastuzumab 기반의 항암치료가 기본이지만 pembronizumab을 더하여 도움이 된다는 결과가 있습니다 (Lancet 2023).
![]() 6. 면역치료. Immunotherapy. Immune checkpoint inhibitor
6. 면역치료. Immunotherapy. Immune checkpoint inhibitor
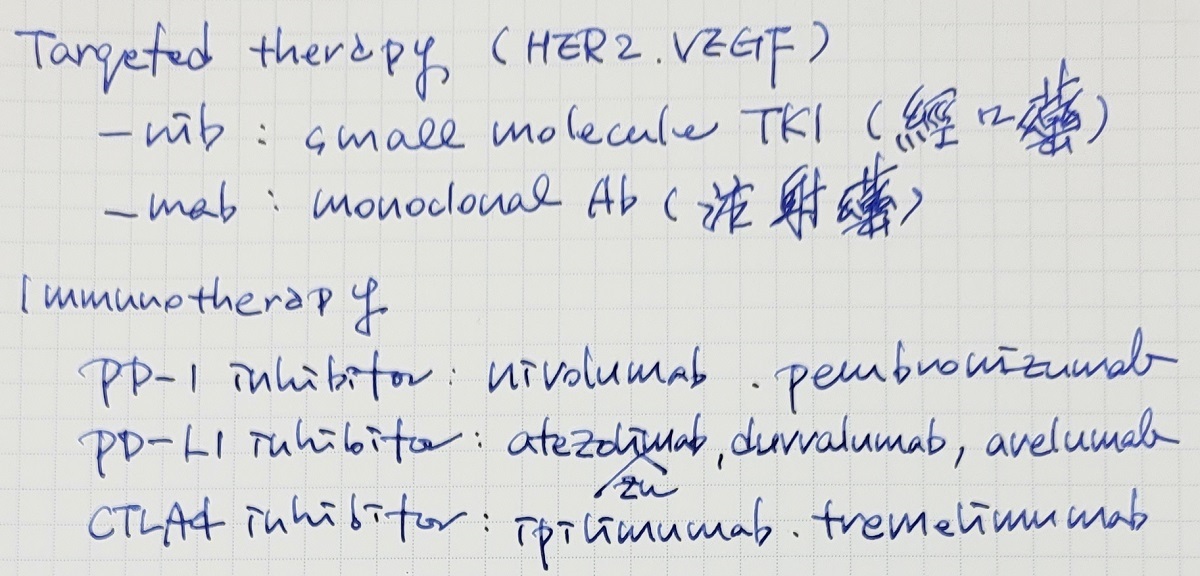
Immune checkpoint inhibitors (ICI)는 아래 그림에서 보이는 바와 같이 크게 세개의 target molecule이 있습니다.
source: The Pharmaceutical Journal 2018
The T-cell receptor binds to an antigen found on the major histocompatibility complex on the surface of the cancer cell.
1) This is a stimulatory response and activates T cells to remove pathogens or cancer cells (shown as the positive circles). A co-stimulatory receptor also exists (CD28), which binds to a ligand (CD80). This results in an increased immune response toward the cancer cell
2) CTLA-4 has a stronger affinity to CD80 and so competes with the co-stimulatory pathway to inhibit the response and ‘switch it off’
3) When a strong TCR stimulus exists, the inhibitor molecule CTLA-4 is upregulated and transported to the surface of the cell; a similar process occurs with PD-1
4) The checkpoint inhibitors act by blocking the inhibitory response by targeting CTLA-4, PD-1 or the ligand PD-L1.
![]() [주요 연구]
[주요 연구]
Trial 홍수입니다. (2023년)
5 major landmark trials in gastric cancer Study Setting Primary endpoint Condition Attraction-2 (Lancet 2017) 3L - Nivo > Placebo OS 5.3 mo vs. 4.1 mo Any patients Keynote-061 (Lancet 2018) 2L - Pem = PTX OS 9.1 mo vs. 8.3 mo PD-L1 CPS >1 Checkmate-649 (Lancet 2021) 1L - Nivo-Chemo > Chemo OS 14.4 mo vs. 11.1 mo PD-L1 CPS >5 Keynote-859 (Lancet Oncol 2023) 1L - Pembro-Chemo > Chemo OS 13.0 mo vs. 11.4 mo PD-L1 CPS >1 Keynote-811 (Lancet 2023) 1L - Pem-Tmab-Chemo > Tmab-Chemo OS 20.0 mo vs. 16.9 mo HER2 (+)
1) Attraction 2 (Lancet 2017) 3rd-line으로 heavily pretreated 아시아 HER2 음성 위암에서 nivolumab의 효과를 처음으로 입증. Median overall survival was 5·26 months (95% CI 4·60-6·37) in the nivolumab group and 4·14 months (3·42-4·86) in the placebo group (hazard ratio 0·63, 95% CI 0·51-0·78; p<0·0001).
2) Keynote-061 (Lancet 2018) 2nd-line으로 previously heavily treated 환자에서 pembronizumab과 paclitaxel을 비교하여 비슷하였다는 결론.
3) Keynote-062 (JAMA Oncol 2020) Pembronizumab에 대한 negative study. Pembrolizumab or pembrolizumab plus chemotherapy was not superior to chemotherapy for the OS and PFS end points tested.
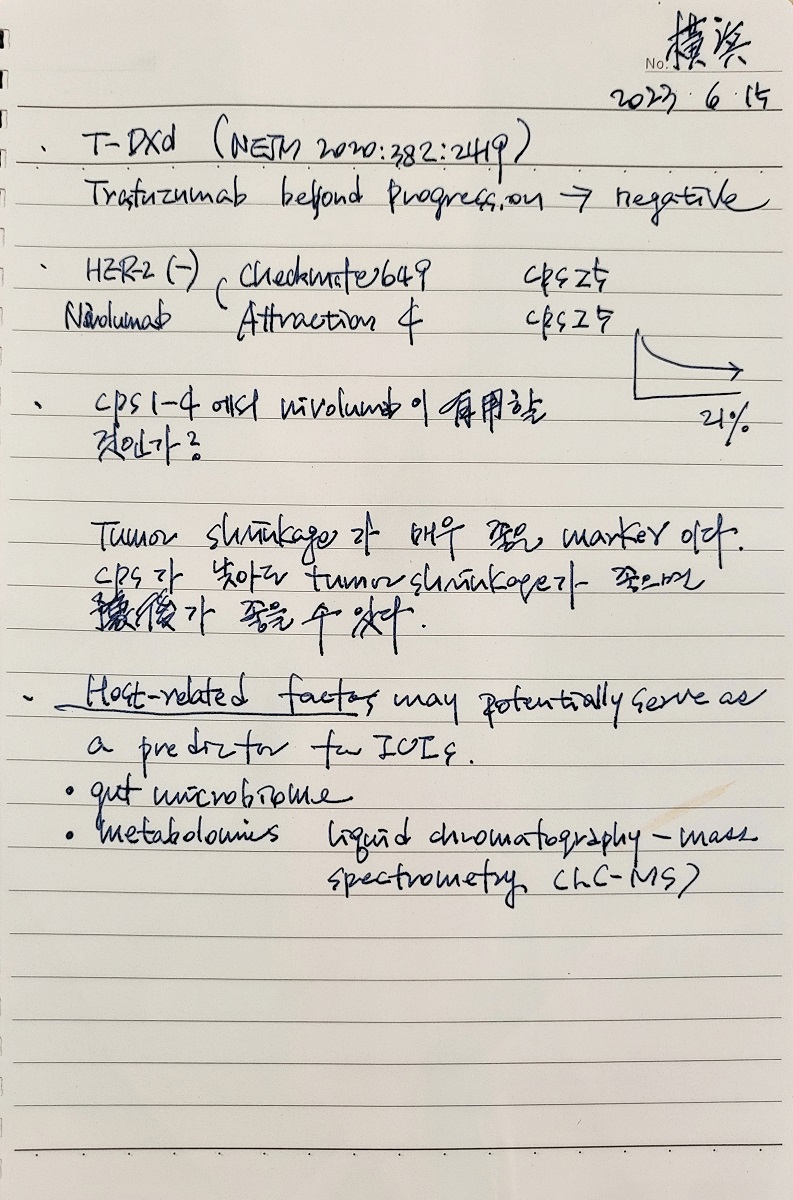
4) Attraction 4 (Lancet Oncol 2022) 아시아인 대상 (일본, 한국, 대만). First-line palliative setting HER2 음성 위암에서 nivolumab이 overall survival은 연장시키지 못했지만 progression free survival은 유의하게 증가시킴.
5) CheckMate-649 (Lancet 2021) 서양인 대상. First-line palliative setting HER2 음성 위암에서에서 nivolumab이 progression free survival과 overall survival을 모두 유의하게 증가시킴. The median follow-up for OS was 13·1 months (IQR 6·7-19·1) for nivolumab plus chemotherapy and 11·1 months (5·8-16·1) for chemotherapy alone. PD-L1 IHC 28-8 (DAKO)를 사용하여 CPS를 계산
CPS에 따른 차이
Overall
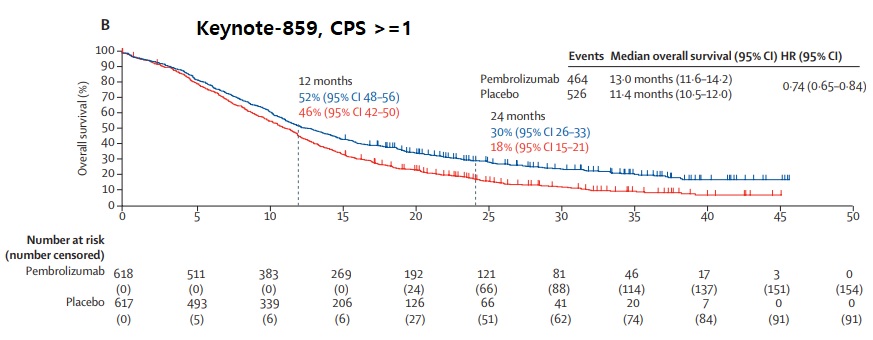
6) Keynote-859 (Lancet Oncol 2023) 연세대 라선영 선생님이 first author인 논문. First-line palliative setting HER2 음성 위암에서 pembronizumab이 overall survival을 유의하게 증가시킴. Median overall survival was longer in the pembrolizumab group than in the placebo group in the ITT population (12·9 months [95% CI 11·9-14·0] vs 11·5 months [10·6-12·1]; hazard ratio [HR] 0·78 [95% CI 0·70-0·87]; p<0·0001), in participants with a PD-L1 CPS of 1 or higher (13·0 months [11·6-14·2] vs 11·4 months [10·5-12·0]; 0·74 [0·65-0·84]; p<0·0001), and in participants with a PD-L1 CPS of 10 or higher (15·7 months [13·8-19·3] vs 11·8 months [10·3-12·7]; 0·65 [0·53-0·79]; p<0·0001). PD-L1 IHC 22C3 (Agilent)를 사용하여 CPS를 계산.
7) Keynote-811 (Lancet 2023) First-line palliative setting HER2 양성 위암은 trastuzumab 기반 항암치료가 표준이지만 pembronizumab을 더하면 도움이 된다는 연구의 interim analysis입니다. Compared with placebo, pembrolizumab significantly improved progression-free survival when combined with first-line trastuzumab and chemotherapy for metastatic HER2-positive gastro-oesophageal cancer, specifically in patients with tumours with a PD-L1 combined positive score of 1 or more. Overall survival follow-up is ongoing and will be reported at the final analysis.
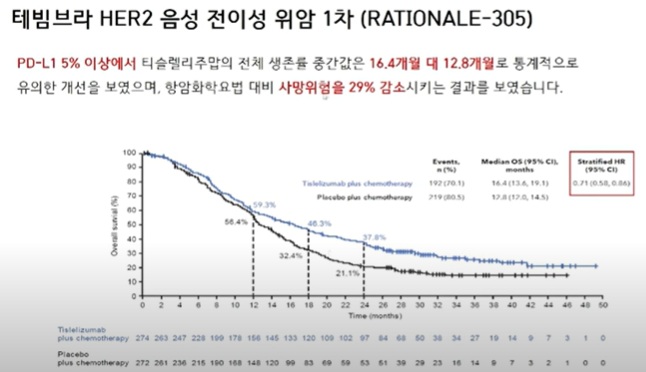
8) RATIONALE-305 (BMJ 2024) HER-2 negative regardless of PD-L1 score. 결과: Tislelizumab plus chemotherapy showed statistically significant improvements in overall survival versus placebo plus chemotherapy in patients with a PD-L1 TAP score of ≥5% (median 17.2 months v 12.6 months; hazard ratio 0.74 (95% confidence interval 0.59 to 0.94); P=0.006 (interim analysis)) and in all randomised patients (median 15.0 months v 12.9 months; hazard ratio 0.80 (0.70 to 0.92); P=0.001 (final analysis)).
![]() [Good response factors]
[Good response factors]
(1) PD-L1: 2022 KGCA guideline에는 palliative first-line setting에서 immunue checkpoint inhibitor에 대한 statement와 Forest plot이 제시되었습니다. 2023년 9월 1일부터 CheckMate-649 (Lancet 2021) 연구에 의거 PD-L1 (28-8) CPS 5 이상(삼성서울병원의 후향적 분석에 의하면 전체 환자의 45%로 추정됨)인 환자에서 nivolumab이 급여로 인정되었습니다. CPS가 5보다 낮은 환자에서 nivolumab의 효과가 없는 것이 아니어서 인정비급여로 사용할 수 있습니다. 그런데 PD-L1 22C3을 사용한 연구에서 pembronizumab이 효과적이라는 Keynote-859 (Lancet Oncol 2023) 연구가 발표되면서 혼란이 예상됩니다. Nivolumab 연구와 pembronizumab 연구의 PD-L1 검사 방법이 달랐기 때문입니다. 앞으로 두 약을 모두 사용하게 되면 PD-L1을 두 가지 방법으로 측정하여 수치가 높은 약제를 선택해야 할 지도 모르겠습니다. (28-8 방법의 CPS가 높으면 nivolumab을 사용하고 22C3 방법의 CPS가 높으면 pembronizumab을 사용한다?) 그러나 한 항목에 대하여 서로 다른 두 검사가 인정될지 걱정입니다. 다행스럽게 두 검사법이 comparable 하다는 연구가 있습니다 (J Gastrointest Oncol 2021).
Statement 24-3: Palliative first-line nivolumab (옵디보) combined with capecitabine or FU plus oxaliplatin (XELOX or FOLFOX) is recommended in patients with PD-L1 CPS ≥5 and HER2-negative advanced gastric cancer (evidence: high, recommendation: strong for).
Comments on immune checkpoint inhibitors in 2022 KGCA guideline
Forest plot for palliative first-line immune checkpoint inhibitor in 2022 KGCA guideline
(2) MSI high: MSI high인 환자에서 ICI의 효과가 좋습니다. 4기 위암 환자의 10-15%가 MSI-H입니다. 조건이 복잡합니다만 pembrolizumab도 사용할 수는 있습니다. 2022 KGCA guideline에는 다음과 같이 언급되어 있습니다. "In Korea, pembrolizumab was approved in patients with several inoperable or metastatic solid tumors, including gastric cancer with MSI-H or dMMR, who have progressed following prior treatment and who have no satisfactory alternative treatment options."
(3) Host related factor를 ICI의 반응을 예측하는 지표로 사용하는 연구들이 있습니다. Microbiome이나 metabolomics 등
![]() [면역항암제의 부작용]
[면역항암제의 부작용]
김좌훈 교수님
![]() [임상에서의 활용]
[임상에서의 활용]
김좌훈 교수님
2023년 9월부터 PDS 5 이상인 경우 nivolumab (옵디보)가 보험 급여가 시작되었습니다. 그런데 PDS가 낮더라도 효과가 없는 것이 아닙니다. PDS 4이하에서는 비급여로 사용할 수 있습니다. PDS 5 이상인 경우가 45%이므로 55%의 환자는 급여 혜택을 볼 수 없는 문제가 있습니다.
CheckMate-649 (Lancet 2021) Nivolumab (옵디보)의 효과. CPS 5이상인 환자에서 생존기간을 3개월 연장. KBDCA 이근욱/안상훈 webinar
![]() [질문/토론]
[질문/토론]
![]() 7. Ramucirumab (VEGFR2 inhibitor)
7. Ramucirumab (VEGFR2 inhibitor)
Rainbow 연구 (Lancet Oncol 2014)
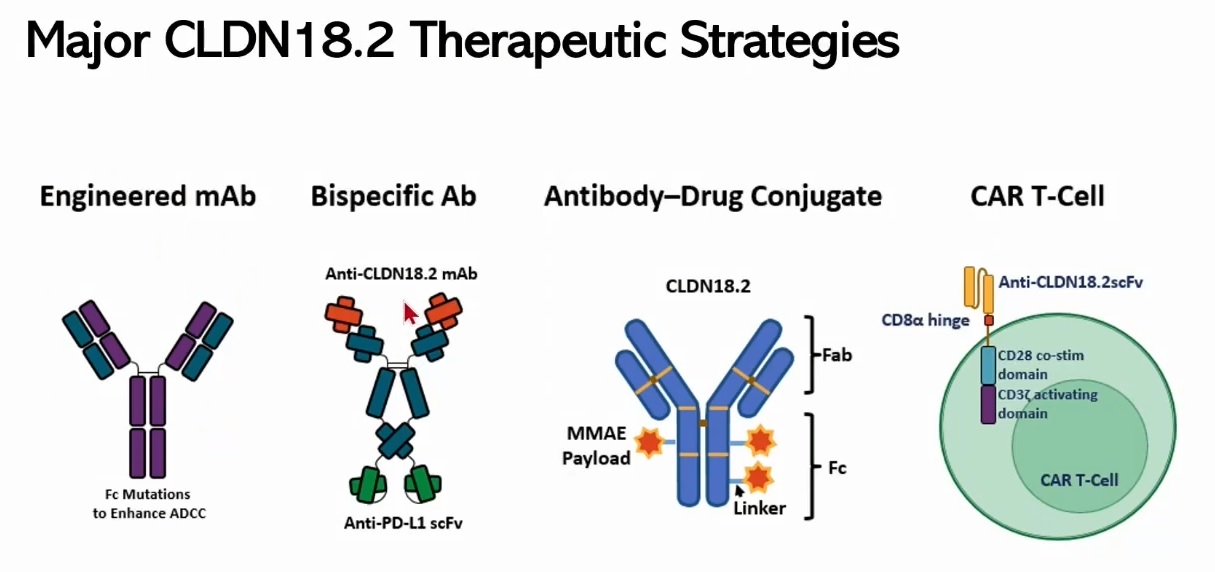
![]() 8. Claudin 18.2
8. Claudin 18.2
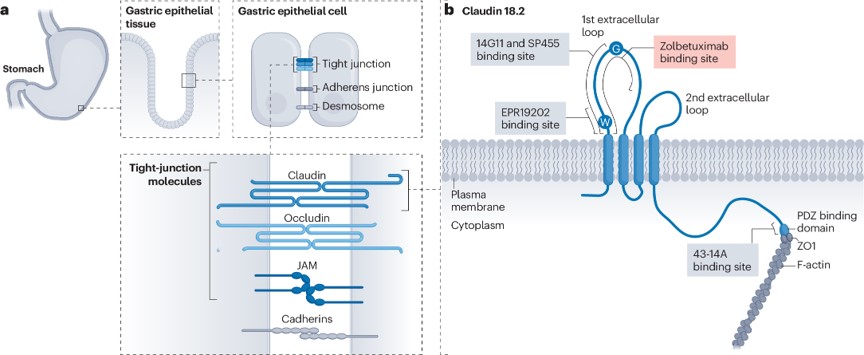
Claudin 18.2 (CLDN18.2) is an important component of tight junction proteins that regulates tissue permeability, paracellular transport, and signal transduction.
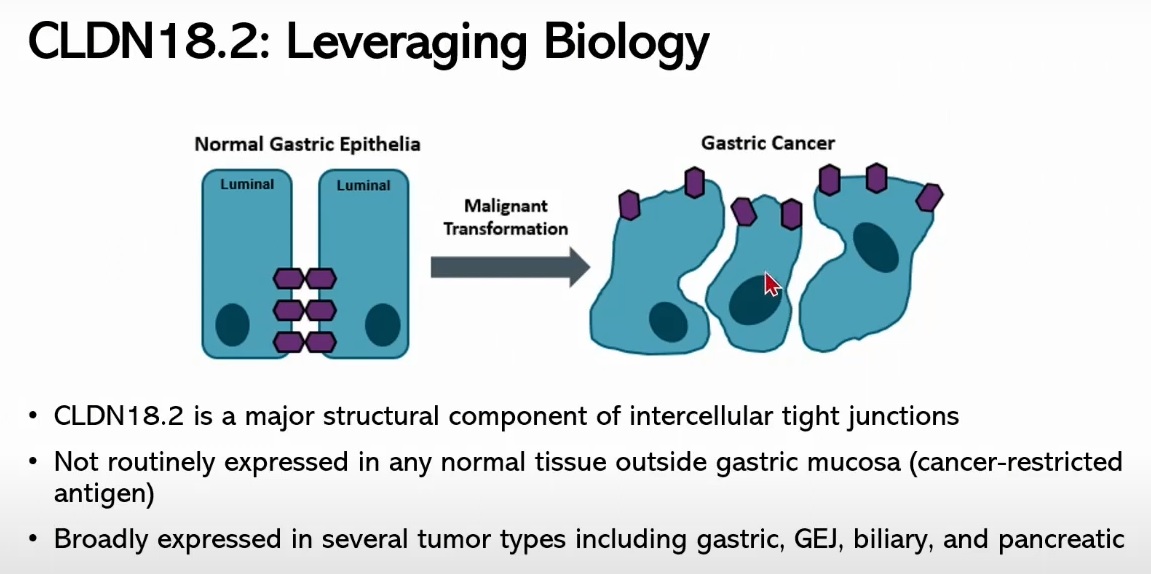
75%라는 cutoff가 너무 strict하여 향후 적응증 확대에 대하여 우려가 있어 상세한 report를 요구하는 목소리가 있습니다.
4기 위암에서 CLDN 18.2는 30-40%에서 양성을 보입니다. 앞으로의 중요한 치료 target입니다.
Claudin 18.2 양성 위암에서 claudin 18.2에 대한 단일클론항체인 zolbetuximab을 추가한 경우 전이성 위암 환자의 생존기간이 연장되었습니다.
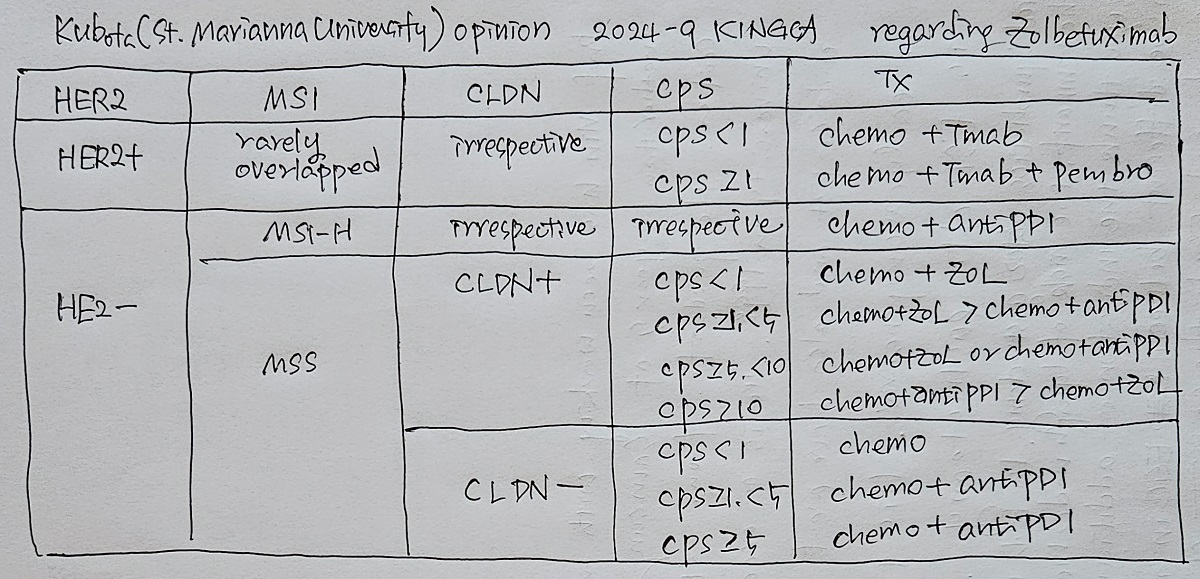
Zolbetuximab (빌로이)은 2024년 10월 approval 되었고 2025년부터 처방되고 있습니다. 2025년 6월 현재 보험 급여는 되지 않고 있습니다.
* 참고: [2025-6-16 청년의사] 빌로이 등장으로 위암 표적 치료 한 단계 격상 (삼성서울병원 김지연교수님)
[질문/토론]
2024-9-26 KINGCA. PD-L1 CPS와 Claudin이 모두 양성일 때 어떤 약제를 선택해야 하는지 hot discussion이 있었습니다. KGCA guideline 2024에서는 연구 결과가 부족하므로 결론을 제시하지 않았습니다.
![]() 9. IP chemotherapy
9. IP chemotherapy
Ishigami Hironori 등의 Phoenix-GC study (JCO 2018)에서 IP chemotherapy에 대한 좋은 결과를 보여주었습니다. 그러나 2023년 현재 우리나라에서 IP chemotherapy는 보험 적용을 받지 못하는 적응증외 치료입니다. 안타깝습니다. 임상연구로 enroll 할 수 밖에 없는 상황입니다.
분당서울대병원 강소현, 김형호 교수님의 최근 리뷰를 소개합니다. Intraperitoneal chemotherapy for gastric cancer: A contemporary perspective (Chin J Cancer Res 2023)
2023년 12월 9일 위암복막전이연구회 심포지엄의 초청강사로 오신 Ishigami Hironori 선생님께서 세 가지 방법을 아래와 같이 비교하셨습니다.
| Key factors | HIPEC | PIPAC | Long-term IP |
| Potency of the drug | ** | * | *** |
| Intraperitoneal concentration | ** | ** | ** |
| Duration of tumor exposure | * | ** | *** |
| Depth of drug infiltration | *** | *** | ** |
| Frequency and duration of treatment | * | ** | *** |
![]() 10. Conversion surgery. 전환 수술
10. Conversion surgery. 전환 수술
Conversion surgery의 conversion은 무슨 뜻일까요? Palliative intent의 치료에서 curative intent의 치료로 전환한다는 의미입니다. Conversion therapy is defined as the treatment strategy in which therapy is converted from systemic medical treatment with a palliative intent to curative surgical treatment of primary and/or metastatic tumors, with the aim of complete resection (R0 resection) of tumors that were originally considered unresectable or marginally resectable for technical and/or oncological reasons. (Kim TH. J Gastric Cancer 2025)
Palliative chemotherapy가 발전하면서 conversion surgery에 대한 관심이 높아지고 있습니다. 독일의 3상 연구였던 RENAISSANCE trial은 negative 결과였습니다. 2021년 국제 다기관 후향적 연구에서는 상당히 희망적인 발표되었습니다 (CONVO-GC-1 study. Yoshida. Ann Gastroenterol Surg 2021).
맨 위 그래프에서 5년 survival이 36.7%이었습니다. Subgroup analysis에서 R0 resection이 되었던 환자의 5년 생존율은 놀랍게도 50%였습니다. 다만 모든 4기 위암 환자에서 이런 결과가 나온 것이 아니라는 점에서 주의해야 하겠습니다. 항암치료를 하여 반응이 아주 좋아서 수술까지 하게 되었던 환자 중 R0 resection인 경우이므로 아주 소수의 환자에 해당한다고 할 수 있습니다.
Yoshida. Ann Gastroenterol Surg 2021 - KBDCA 이근욱/안상훈 webinar
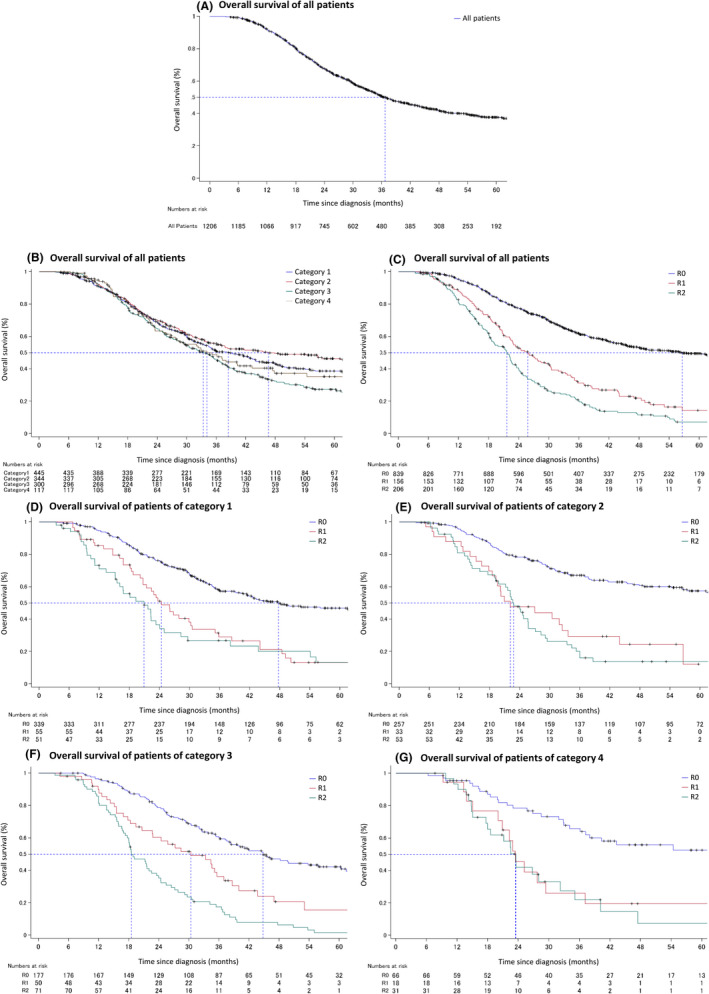
일본에서의 또 다른 연구입니다 (BMC Surgery 2022)
Kaplan-Meier survival curves for patients stratified by the initial status of stage IV disease (a) and the residual tumor status (b). IR=initially resectable disease, including patients with category 1 stage IV gastric cancer; UR=unresectable disease, including patients with category 2-4 stage IV gastric cancer.
다음은 삼성서울병원의 conversion surgery 결과입니다 (Biomedicines 2023).
Palliative chemotherapy 환자의 3.9%에서 conversion surgery가 시도되었습니다.
R0 resection이 가능하였던 환자의 5 YSR가 절반이라는 다기관 연구(Ann Gastroenterol Surg 2021)와 일치하는 단일기관의 연구결과입니다. 특히 17.7% (21/118)는 병리학적 CR이었고 이들은 예후가 아주 좋았습니다.
매우 happy한 증례입니다.
2024년 KINGCA에서 conversion surgery에 대한 expert consensus meeting이 있었습니다 (Kim TH. JGC 2025).
"Most experts agreed that conversion therapy provides a survival benefit for selected patients who respond to systemic therapy and undergo R0 resection (88.3%). Patients with limited metastases were considered good candidates (94.2%). The optimal timing was based on the response to systemic therapy (70.6%). The regimen was recommended to be individualized (100%) and the duration to be at least 6 months (88.3%). A minimally invasive approach (82.3%) and D2 lymph node dissection (82.4%) were considered for surgery. However, resection for metastases with a complete clinical response after systemic therapy was not advocated (41.2%). "
이 중에서 수술은 D2가 좋다는 점에 대하여 일본인 의사들은 고개를 갸우뚱하였다고 합니다.
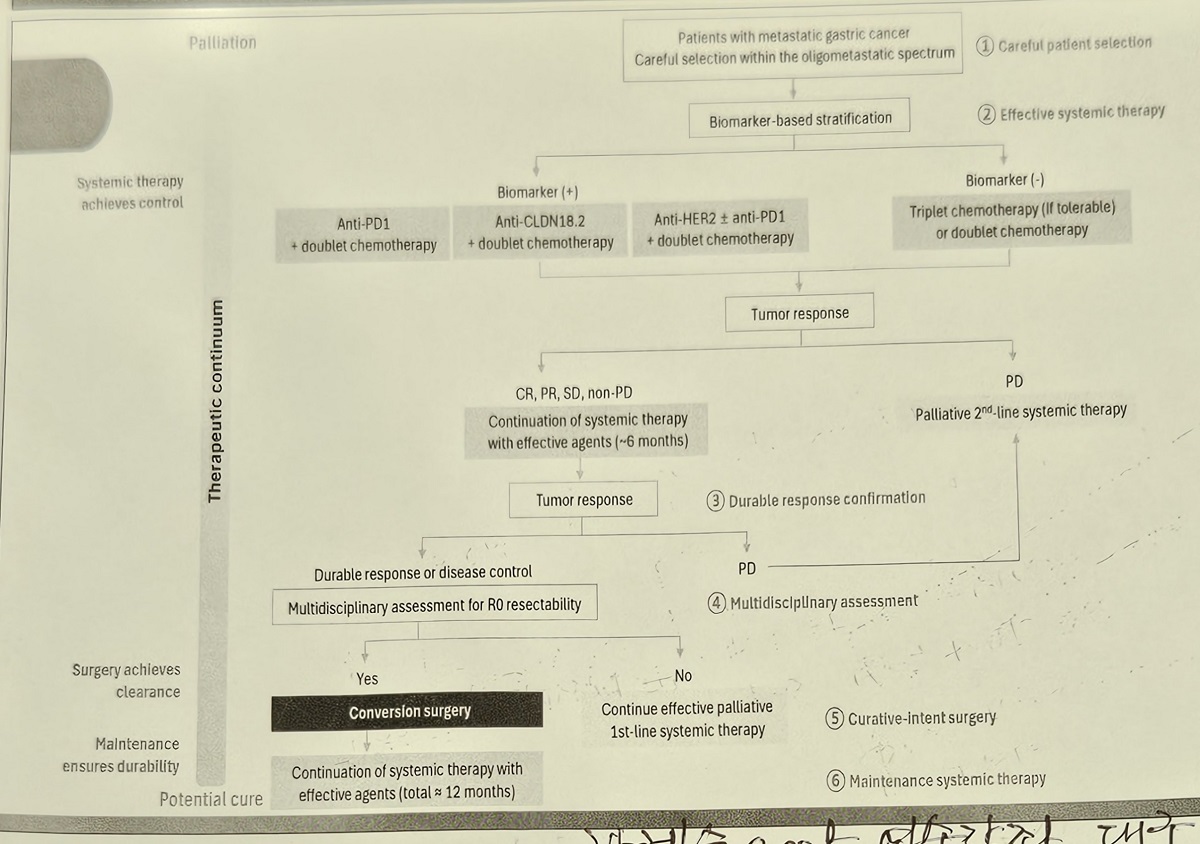
2026-3-28 위암학회 심포지엄(대구 EXCO)에서 한혜숙 선생님께서 멋지게 정리해 주셨습니다. (1) Careful patient selection, (2) Effective systemic therapy, (3) Durable response confirmation, (4) Multidisciplinary assessment, (5) Curative-intent surgery, (6) Maintenance systemic therapy가 모두 중요합니다.
![]() [Symposiums]
[Symposiums]
[2023-6-13] IGCC 2013
[2023-12-9] 위암복막전이연구회 (고려대학교 구로병원 새롬교육관 1F 대강당)
[2024-11-15] KDDW
2024-11-15. KDDW
[2026-3-28] 위암학회 심포지엄. 대구 EXCO
![]() [FAQ]
[FAQ]
[2015-2-4. 애독자 질문]
TS-1의 이름에 무슨 뜻이 숨겨져 있나 잠시 인터넷 검색을 해봤는데, 유럽에서 Teysuno라는 상품명으로 팔리며, TS-1과 발음이 유사한 외엔 어떤 의미도 못찾았습니다. 다만 pubmed에서 검색 시, 아래 그림 파일처럼 2011년도에 실린 논문이 있던데, 아무리 생각해봐도 TS-1이 titanium silicate는 아닌 것 같아서요?
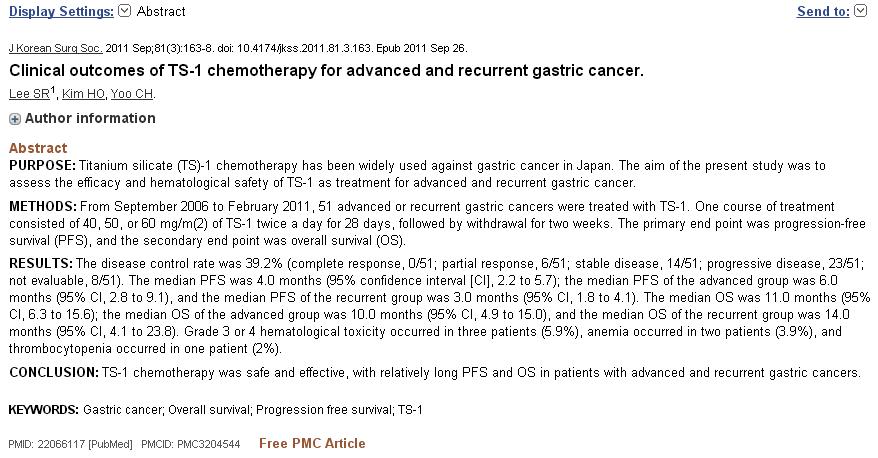
[2015-2-5. 이준행 답변]
논문에 실린 내용이 다 옳은 것은 아닐 것입니다. 저도 titanium silicate는 아닐 것 같아서 친한 oncologist에게 문의하였고 아래와 같은 답변을 받았습니다. 참 엉터리같은 작명법이라고 생각되었습니다. 아마 일본 스타일 같습니다.
"TS-1 은 사실 조합글자라고 합니다.
T: TAIHO...일본 제약회사 이름
S: 소아쿠센터(임상약개발센터)의 영문 앞자..S이러한 조합으로 TS-1 이라는 약 상품명이 나와게 되었다고 합니다. 출처는 TS-1 제약회사입니다."
![]() [References]
[References]
1) 위암항암치료
2) 전립선암 항암치료
![]() © 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.
{kind=link}
{kind=link}
{kind=link}
{kind=link}