EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Dignostic group classification before and after resection. Pathological discrepancy. Pathological upgrading] - 終
[Dignostic group classification before and after resection. Pathological discrepancy. Pathological upgrading] - 終
![]() 1. Diagnostic group classification (삼성서울병원 2016)
1. Diagnostic group classification (삼성서울병원 2016)
2012년 치료 결과를 분석하여 'Diagnostic group classifications of gastric neoplasms by endoscopic resection criteria before and after treatment: real world experience'라는 제목으로 분석하였습니다 (Lee JH. Surg Endosc 2016 / PDF). Absolute indication EGC, Expanded indication EGC, Beyond expanded indication EGC 등을 '진단명'이라고 붙일 수 없어서 'diagnostic group classification'이라는 말을 만들어 써 보았습니다.
"Background and study aims: There are often discrepancies between the pretreatment evaluation of gastric neoplasms by endoscopy with biopsy and the final diagnosis of resected specimen in terms of pathology and depth of invasion. We evaluated the spectrum of discrepancies between pretreatment and posttreatment diagnosis which may deliver significant differences on clinical practice.
Patients and Methods: A total of 2,041 patients with gastric dysplasia or cancer who underwent curative endoscopic resections or surgeries in 2012 were enrolled. Patients were classified into five different diagnostic groups; low-grade dysplasia (LGD), high-grade dysplasia (HGD), absolute indication early gastric cancer (AI-EGC), beyond absolute indication early gastric cancer (BAI-EGC), and advanced gastric cancer (AGC). The choice of initial treatment and final pathologic diagnosis was analyzed.
Results: The study patients belonged to the following pretreatment diagnostic groups; LGDs in 162, HGDs in 164, AI-EGCs in 396, BAI-EGCs in 824, and AGCs in 495 cases. Posttreatment diagnostic groups were LGDs in 140, HGDs in 121, AI-EGCs in 322, BAI-EGCs in 947, AGCs in 505, and no residual tumor in 6 cases. In general, 6.9% (141/2,041) of cases were down-graded, and 15.9% (324/2,041) were up-graded. Thirty-four percent of pretreatment HGDs (56/164) were changed to cancers after endoscopic resection. Thirty-three percent of pretreatment AI-EGCs (131/396) were re-grouped as posttreatment BAI-EGCs. The additional surgery rate in each pretreatment group was 0.6% in LGD, 4.3% in HGD, 15.7% in AI-EGC, 23.6% in BAI-EGC among the patients with initial endoscopic resection (p < 0.01).
Conclusions: Twenty-three percent of gastric neoplasms changed in their final diagnostic group after endoscopic resection or surgery. This discrepancy should be considered when the initial treatment strategy is being selected."
우리나라에서 ESD 영역은 무척 혼란스럽습니다. 시술 전후 병리 결과가 바뀌는 예가 너무 많기 때문입니다. 일본은 조금만 이상하면 다 암으로 진단을 붙여버리므로 ESD 시행 환자의 대부분이 처음부터 위암입니다. 그런데 우리나라에서는 상당수가 시술 전 adenoma, 시술 후 adenocarcinoma입니다. 이 부분을 frank 하게 보고한 논문이 없어서 마음 먹고 한번 정리한 것입니다.
전체적으로 6.9% (141/2,041)가 down-grade 되고 15.9% (324/2,041)가 up-grade 되었습니다. Diagnostic group classification이 그렇게 바뀌었다는 의미입니다.
Absolute indication으로 판단된 환자의 89.6%가 첫 치료로 ESD가 선택되고 있습니다.
이 결과를 바탕으로 ESD 후 수술이 필요할 확률이 15%라고 설명하고 있습니다.
치료 전 분류에 따라 결과를 보여주는 것과 치료 후 분류에 따라 결과를 보여주는 것은 매우 큰 차이가 있습니다. Expanded indiction의 경우 그 차이가 가장 현저합니다.
각 diagnostic group에 대하여 이와 비슷한 diagram을 만들어보면 재미있을 것 같습니다. Real world에서는 이렇게 복잡한 일이 벌어지고 있는 것입니다.
위 도표에서 ESD 前 absolute indication EGC로 판단되었으나 최종적으로 AGC로 나온 환자가 1명 있었습니다. 매우 드문 경우였기에 소개합니다. ESD가 시도되었는데 submucosal adhesion으로 ESD를 마칠 수 없었고 수술을 시행하여 AGC로 확인된 환자였습니다. ESD로 인한 인공궤양때문에 보만 3형으로 분류되었지만 내시경적으로는 EGC-like AGC 즉 Borrmann type unclassified가 가장 적합한 분류라고 생각합니다.
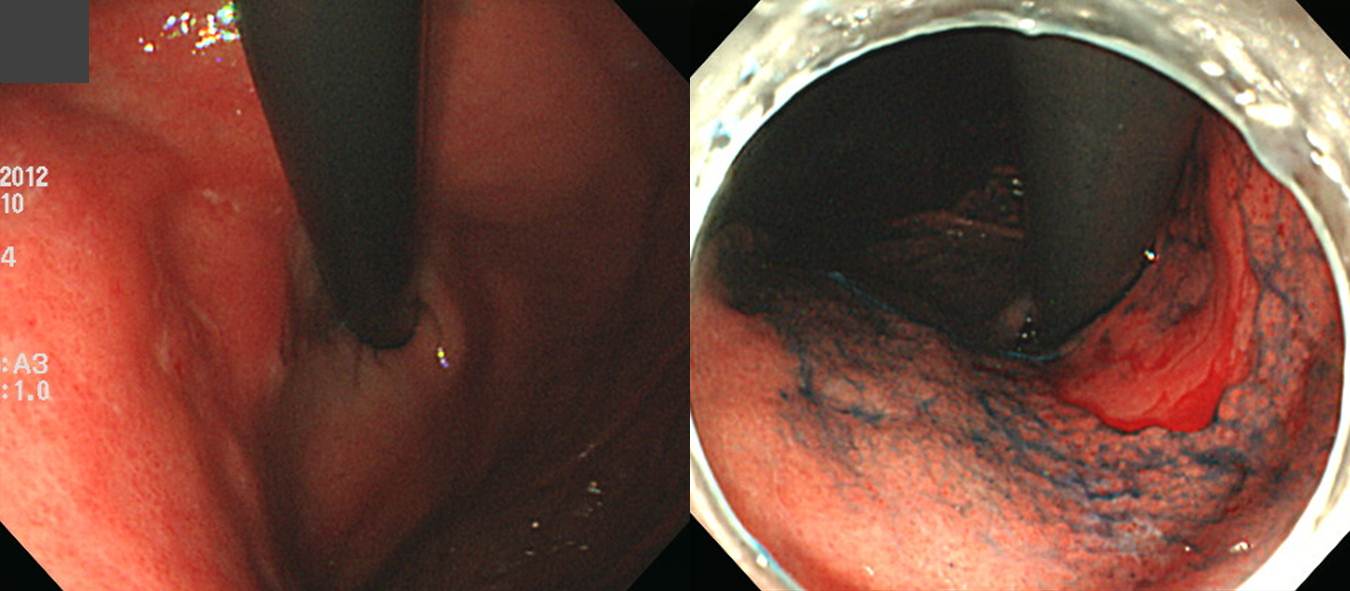
Stomach, total gastrectomy:
Status post endoscopic submucosal dissection (incomplete)
Advanced gastric carcinoma
1. Location : upper third, Center at body and lesser curvature
2. Gross type : Borrmann type 3
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size : 3x1.5 cm
6. Depth of invasion : invades muscularis propria (pT2)
7. Resection margin: free from carcinoma, safety margin: proximal 2 cm, distal 11.4 cm
8. Lymph node metastasis : no metastasis in 38 regional lymph nodes (pN0)
9. Lymphatic invasion : present
10. Venous invasion : not identified
11. Perineural invasion : present
12. Peritoneal cytology : negative
[참고 자료]
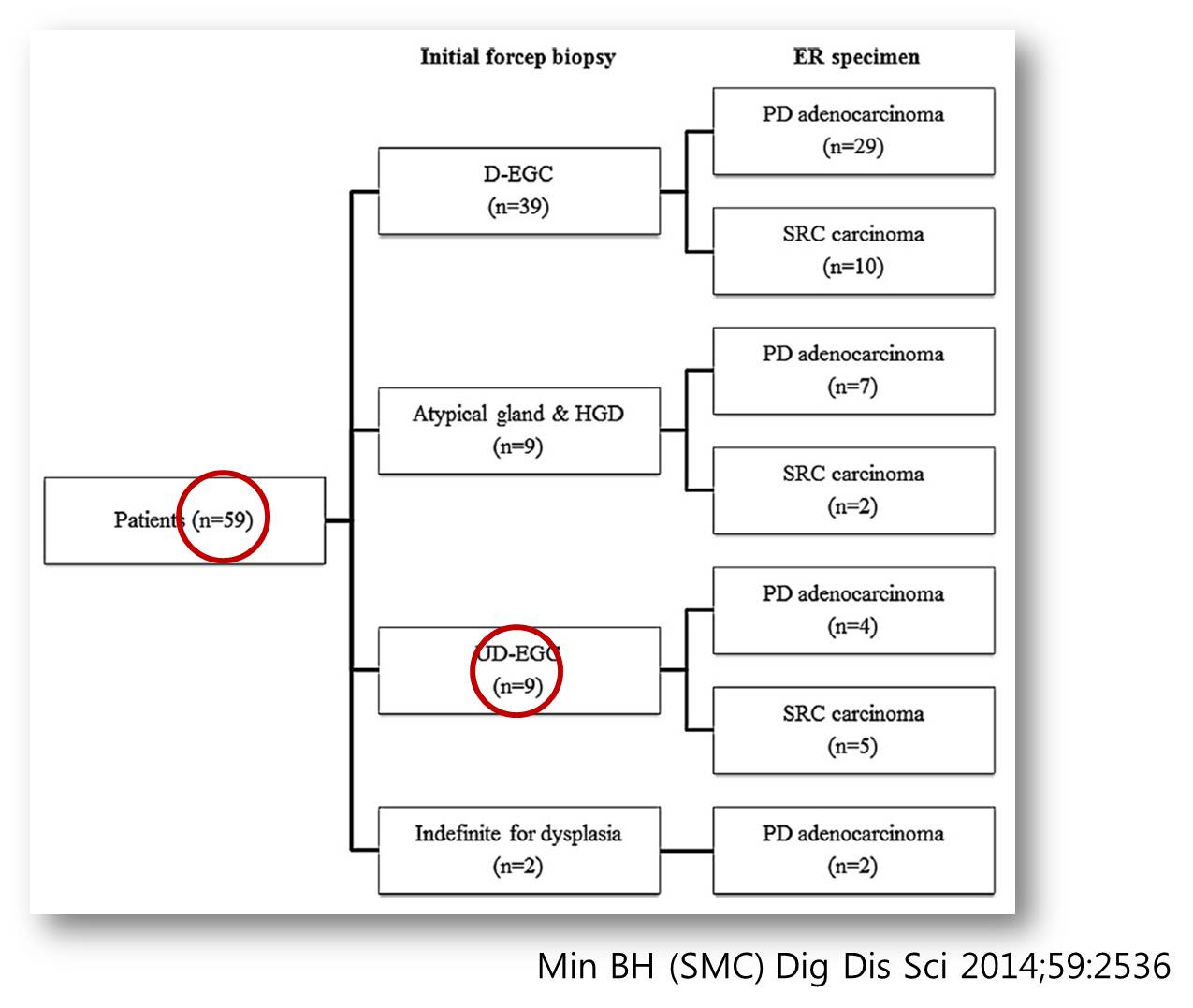
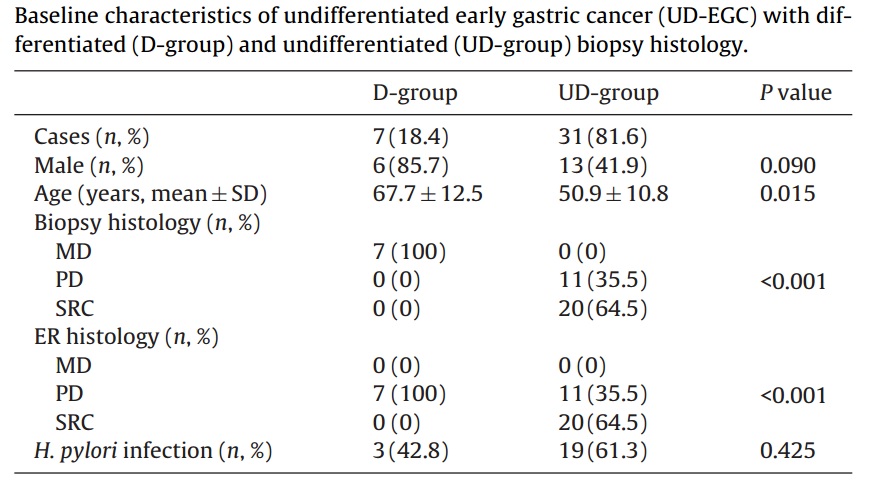
1) 2014년 삼성서울병원 논문입니다 (Dig Dis Sci 2014). 약 9년간 2,194명의 ESD를 치료했는데 그 중 치료 후 undifferentiated-type이 59예(2.7%)였습니다. Undifferentiated-type 59예 중 50예(84.7%)가 치료 전에는 differentiated-type, atypical gland, indefinite for dysplasia였습니다. 치료 전 조직검사에서도 undifferentiated-type으로 나온 경우는 9예 (15.2%)에 불과하였습니다. Undifferentited-type을 ESD하는 경우가 거의 없는 병원에서 보이는 경향을 대표한다고 할 수 있습니다 (참고: 2014년 이후부터는 작은 undifferentiated type에 한하여 종종 ESD를 하고 있습니다). Posttreatment 분석에서는 undifferentiated-type이라도 pretreatment 분석을 해보면 differentiated-type이 적지 않다는 점을 강조하였습니다.
2) 2014년 연세대학교 강남세브란스병원 논문입니다 (Pathol Res Pract 2014). 약 9년 간 조기위암 289예를 치료했는데 그 중 치료 후 undifferentiated-type이 38예(13.1%)였습니다. 치료 후 undifferentiated-type 38예 중 7예(18.4%)가 치료 전에는 differentiated-type이었습니다. Undifferentited-type에 대한 ESD에 대하여 비교적 적극적인 mind를 가진 병원의 경향을 대표하다고 할 수 있습니다.
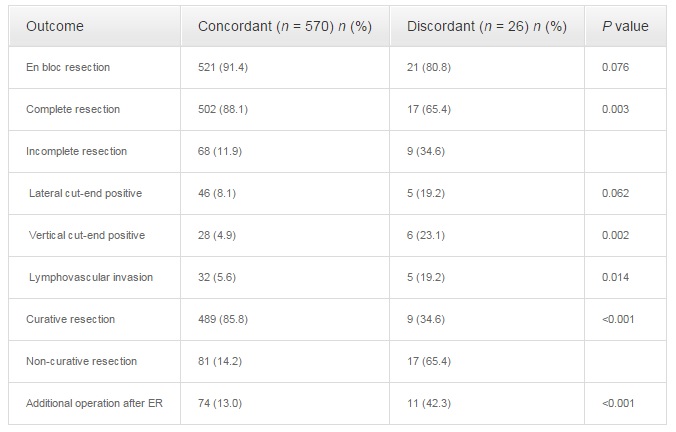
3) 2014년 연세대학교 신촌세브란스병원 논문입니다 (Surg Endosc). 약 7년 간 치료 전 조직검사 differentiated-type 596병소를 치료했는데, 그 중 치료 후 undifferentiated-type으로 바뀐 경우가 26예 (4.3%)였습니다. 같은 기간 치료 전 조직검사 undifferentiated-type은 몇 예가 있었은지는 밝히지 않았습니다.
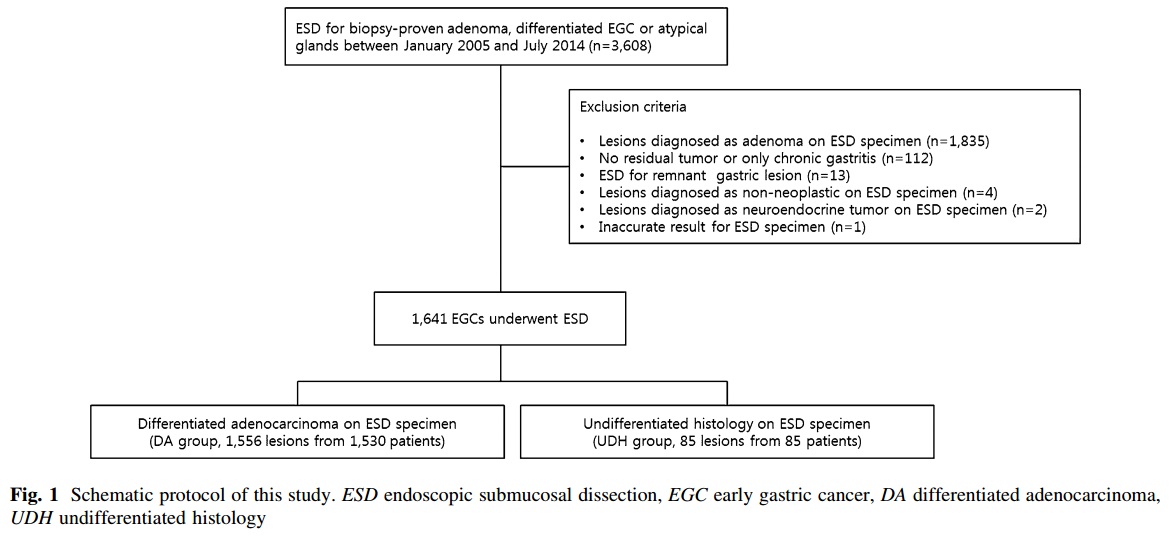
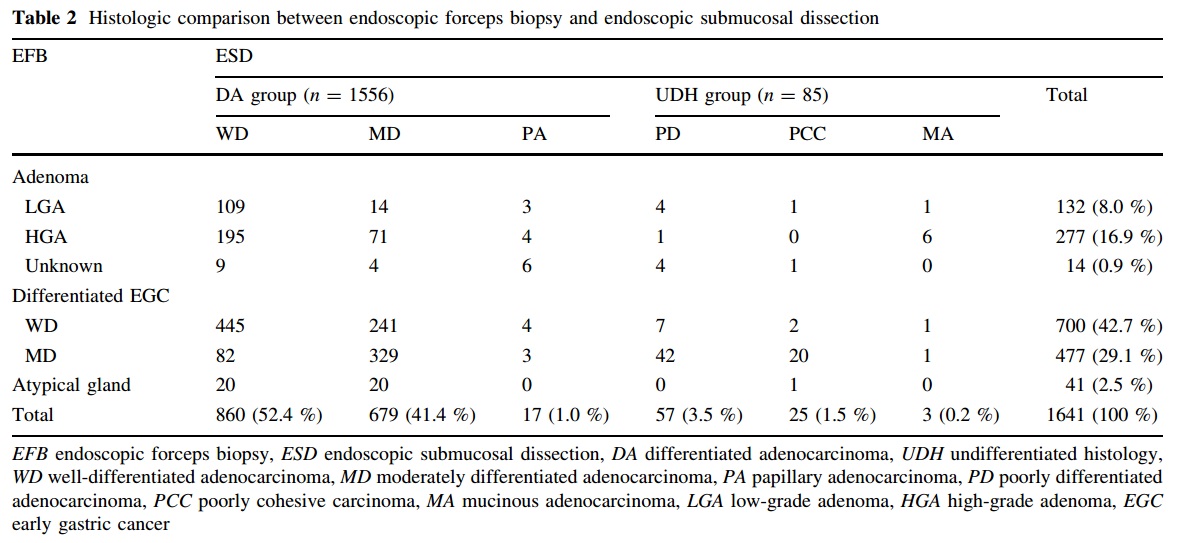
4) 2016년 서울대학교병원 논문입니다 (Choi JM. Surg Endosc 2016). Biopsy-proven differentiated type EGC 1,641 병소를 ESD 하였을 때 5.2% (85 병소)가 undifferentiated로 바뀌었습니다. 관련된 인자는 female sex, age < 65 years, large endoscopic size, depressed morphology, surface nodularity, whitish discoloration 였습니다. 같은 기간 치료 전 조직검사 undifferentiated-type은 몇 예가 있었은지는 밝히지 않았습니다.
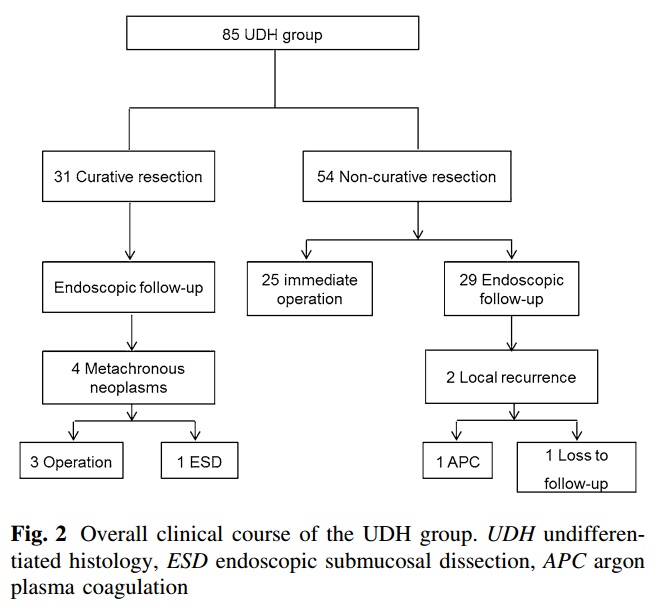
Undifferentiated type histology로 바뀐 85예의 curative resection rate는 36.5%(31/85)였습니다. 비록 undifferentiate type histology라고 하더라도 처음에 differentiate type이었고 ESD 적응증에 속했다면 curative resection이 나왔을 때에는 예후가 좋다는 것을 알 수 있습니다.
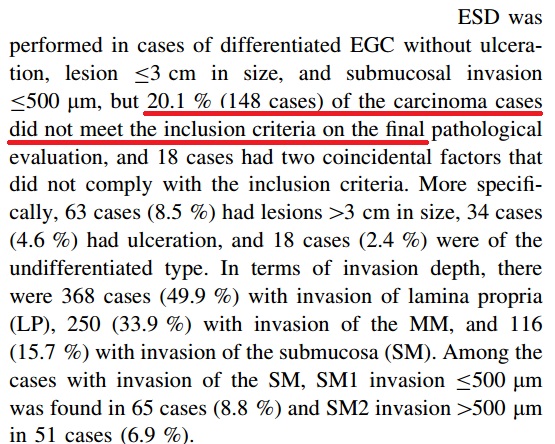
5) 2015년 11월 Gastric Cancer지에 NECA 연구의 병리 part 결과가 E-pub으로 발표되었습니다 (Kim JM. GC 2015 - Epub). 문득 옛 일이 생각났습니다. NECA 연구의 기획 단계에 참여했다가 중간에 빠져서 여러 선생님께 심하게 꾸중을 들었던 아픈 기억이 있습니다.
이번 연구에서 beyond expanded indication 증례가 20.1%였습니다. 다소 높은 편이 아닐 수 없습니다. 다기관 연구였던 것과 관련된 것으로 추정됩니다.
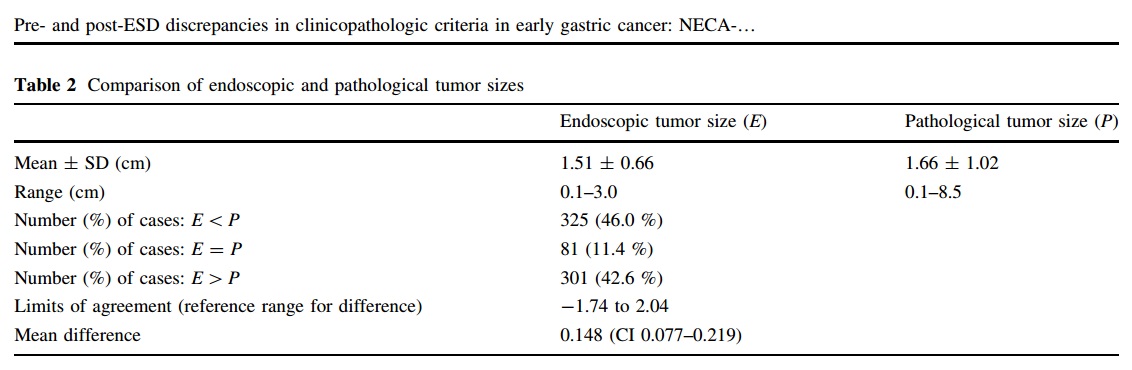
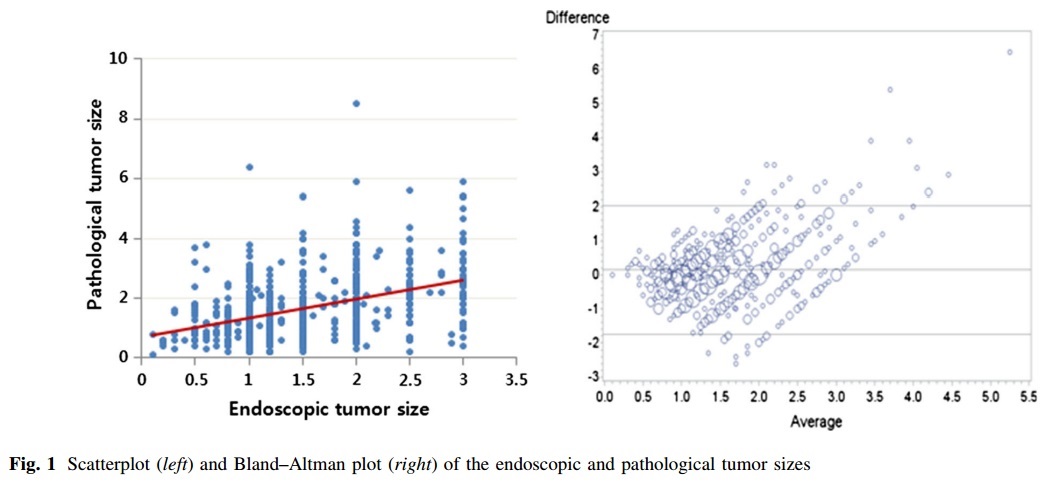
여러 변수가 분석되었는데 제 관심을 끈 것은 크기 차이였습니다. 생각보다 편차가 작았습니다. 내시경으로 측정한 크기와 병리 크기의 평균 차이가 1.5 mm 밖에 되지 않았으니까요. 2 cm로 생각하고 시술했는데 8.5cm가 나온 것도 있지만...
![]() 2. Diagnostic group classification at National Cancer Center (국립암센터 2016)
2. Diagnostic group classification at National Cancer Center (국립암센터 2016)
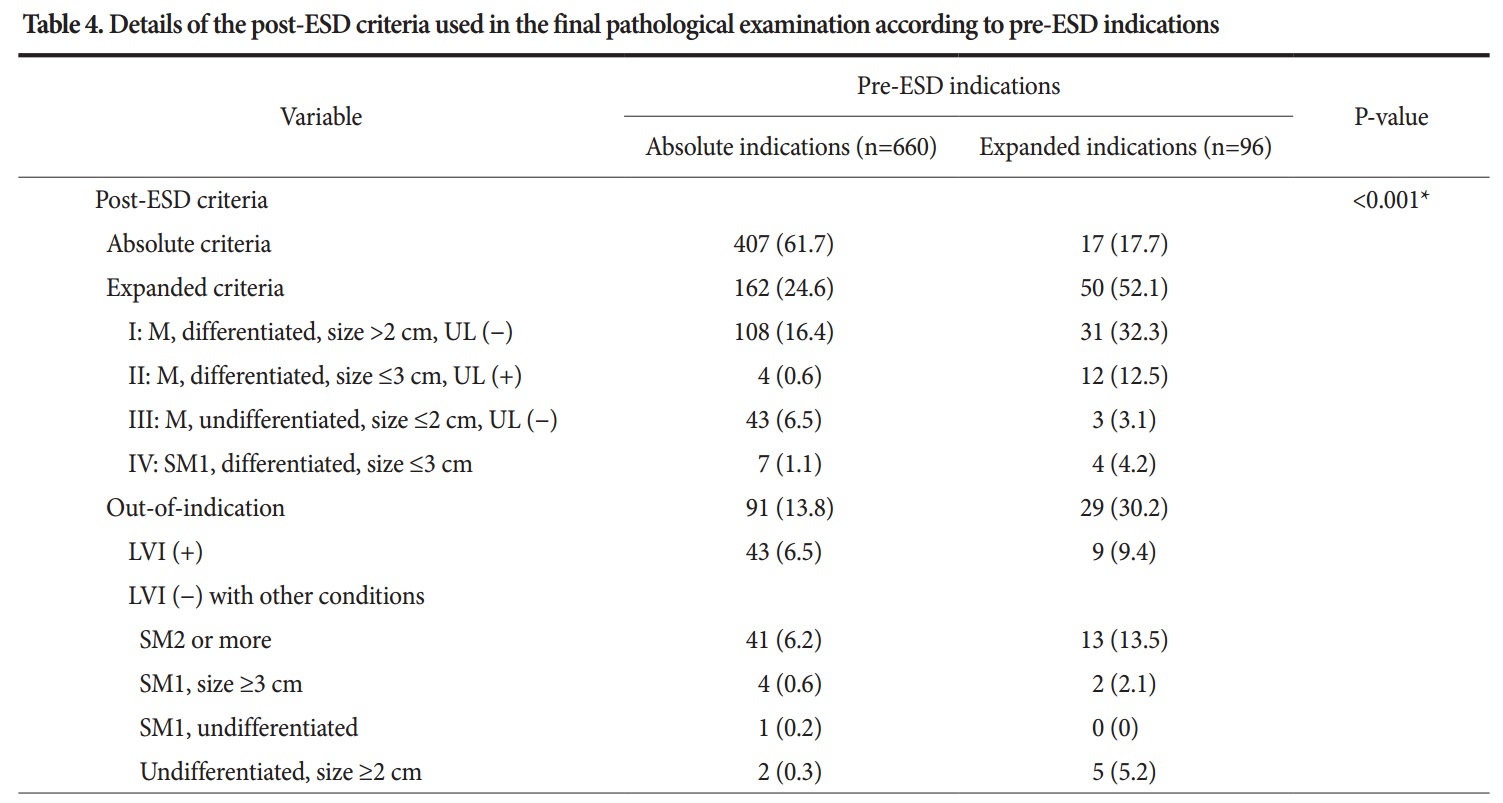
Diagnostic group classification이라는 용어를 사용하지는 않았으나 국립암센터에서도 ESD 전후 병리 진단의 차이에 대한 좋은 자료를 발표하였습니다.
ESD 전 absolute indication으로 평가하였던 환자의 13.8%가 out-of-indication으로, 즉 수술이 필요한 것으로 나왔고, ESD 전 expanded indication으로 평가하였던 환자의 30.2%가 out-of-indication으로 나왔다는 이야기입니다.
![]() 3. A prediction model for pathological upgrading (Nanjing Medical University 2023)
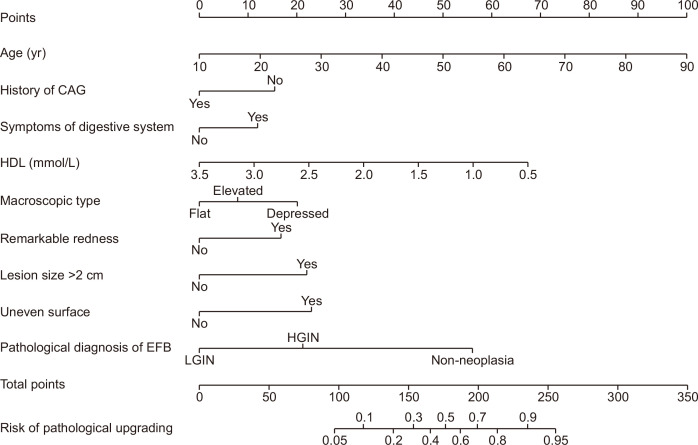
3. A prediction model for pathological upgrading (Nanjing Medical University 2023)
![]() [FAQ]
[FAQ]
[2017-12-21]
병리과와 회의를 했습니다. ESD 후 절제표본에 대한 병리 수가에 대하여 정부 고시가 있었다고 합니다. ESD 절제 표본을 악성 질환과 양성 질환에 따라 코드를 달리하겠다는 내용이었습니다. ESD 후 암인지 아닌지는 결과가 나와 봐야 아는 것인데 또 ESD 전 시술에 따라 가격을 달리하는 이상한 정책이 나왔습니다. 언제까지 이런 이상한 정책을 계속 만들 것인지 한심하기 그지 없습니다.

![]() [References]
[References]
1) EndoTODAY 위암 004 분화조직형 위암 ESD 후 미분화조직형 위암으로 변경되어 보고된 증례
![]() © 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Jun Haeng Lee
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Jun Haeng Lee