 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Management of non-curative endoscopic resection of EGC at SMC]
[Management of non-curative endoscopic resection of EGC at SMC]
2015년 4월 4일 위암학회(KINGCA)에서 조기위암 non-curative resection에 대하여 구연발표를 할 예정입니다. 늘 강의는 합니다만, 구연 발표는 10년 만인지라 약간 긴장되면서 한편 기대되기도 합니다 (Subnote). 게다가 영어발표이기도 하구요...
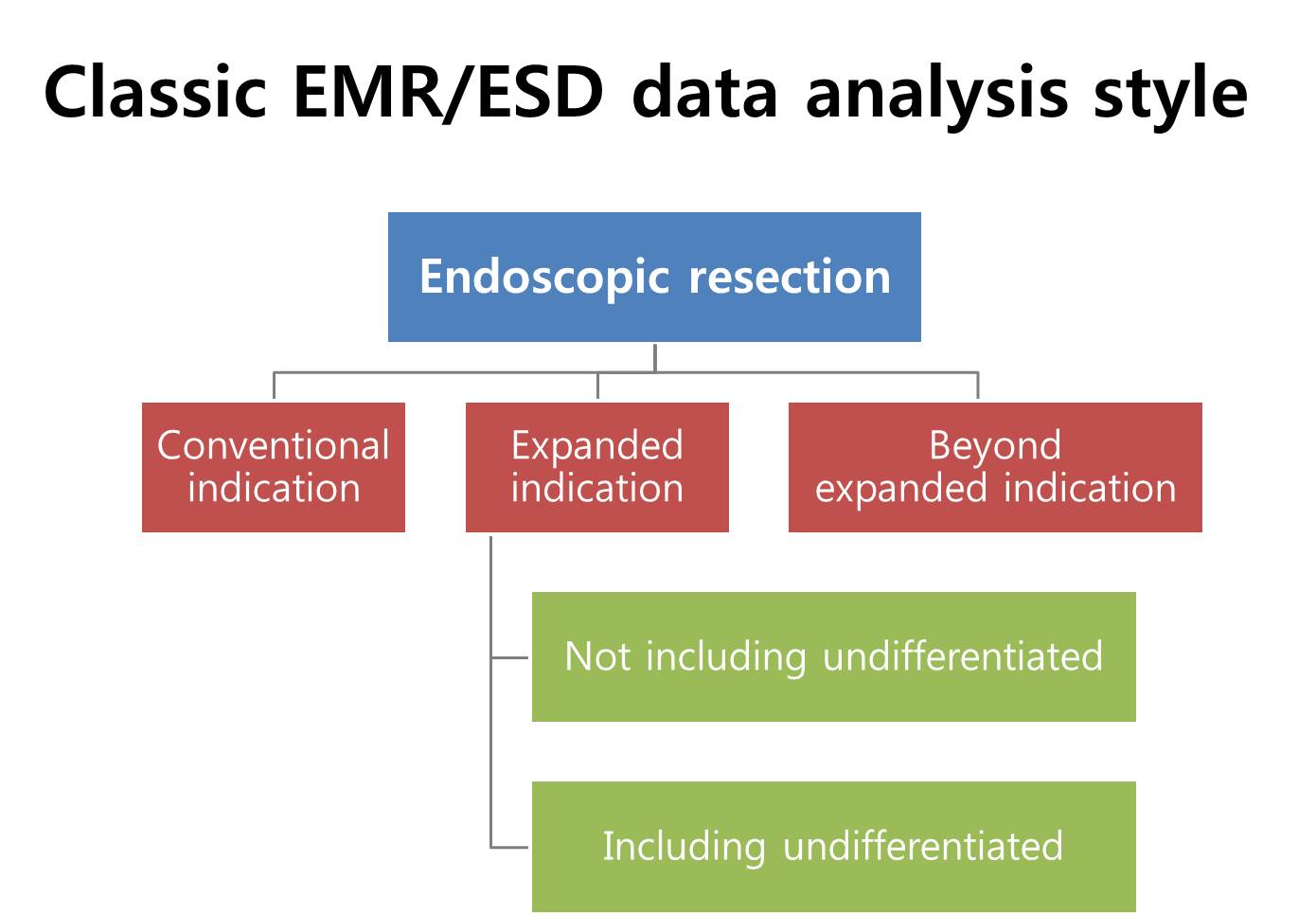
Outcome after endoscopic resection of EGC is usually presented by the indication groups, such as conventional indication, expanded indication and beyond expanded indication. However, it is controversial whether EGCs with undifferentiated histology should be part of expanded indication.
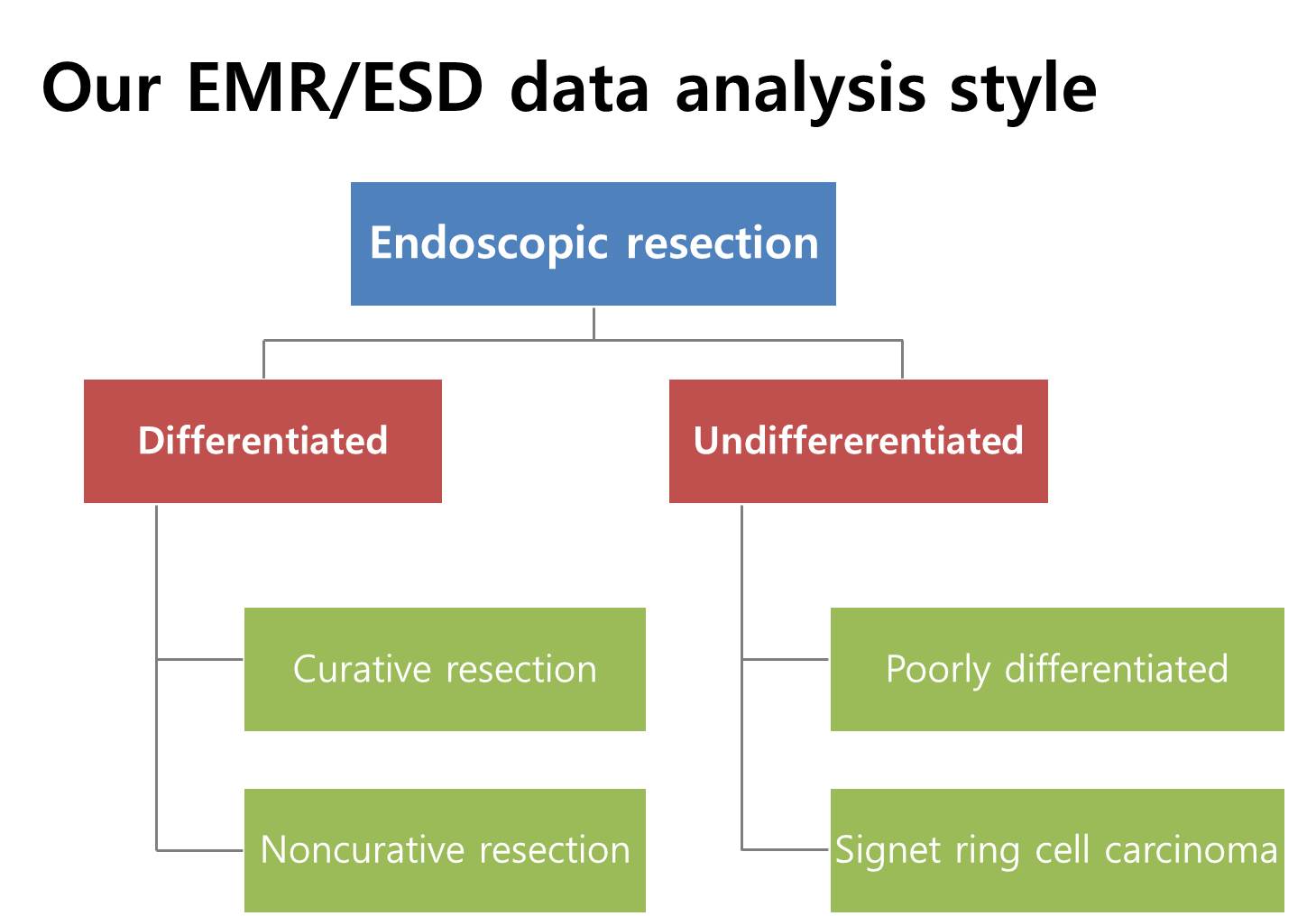
In our institution, we usually recommend surgery for EGCs with undifferentiated histology, so most cases have differentiated histology. After endoscopic resection, the results can be either curative resection or non-curative resection based on the pathological findings.
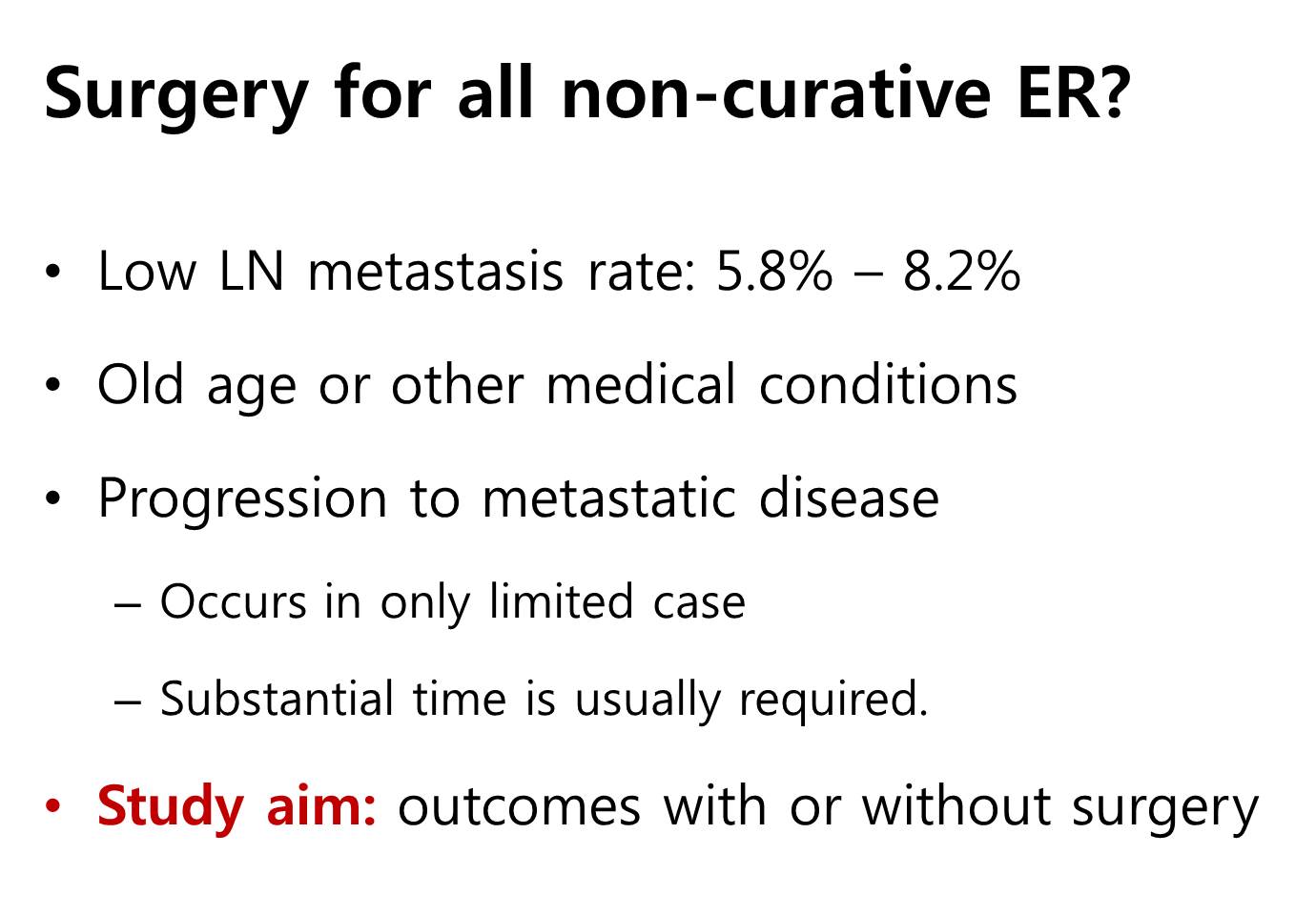
Standard treatment for non-curative resection is surgery, but it’s not clear whether surgery is always required. First, the risk of lymph node metastasis is less than 10%. Second, the risk of surgery is high due to old age and other medical conditions. Finally, progression to metastatic disease occurs in only limited cases, and substantial time is required. So in this study, we evaluated the outcome of non-curative resection with or without additional surgery.

This is a retrospective study for more than two thousand cases, which were endoscopically resected from 2,000 to 2011 at Samsung Medical Center.
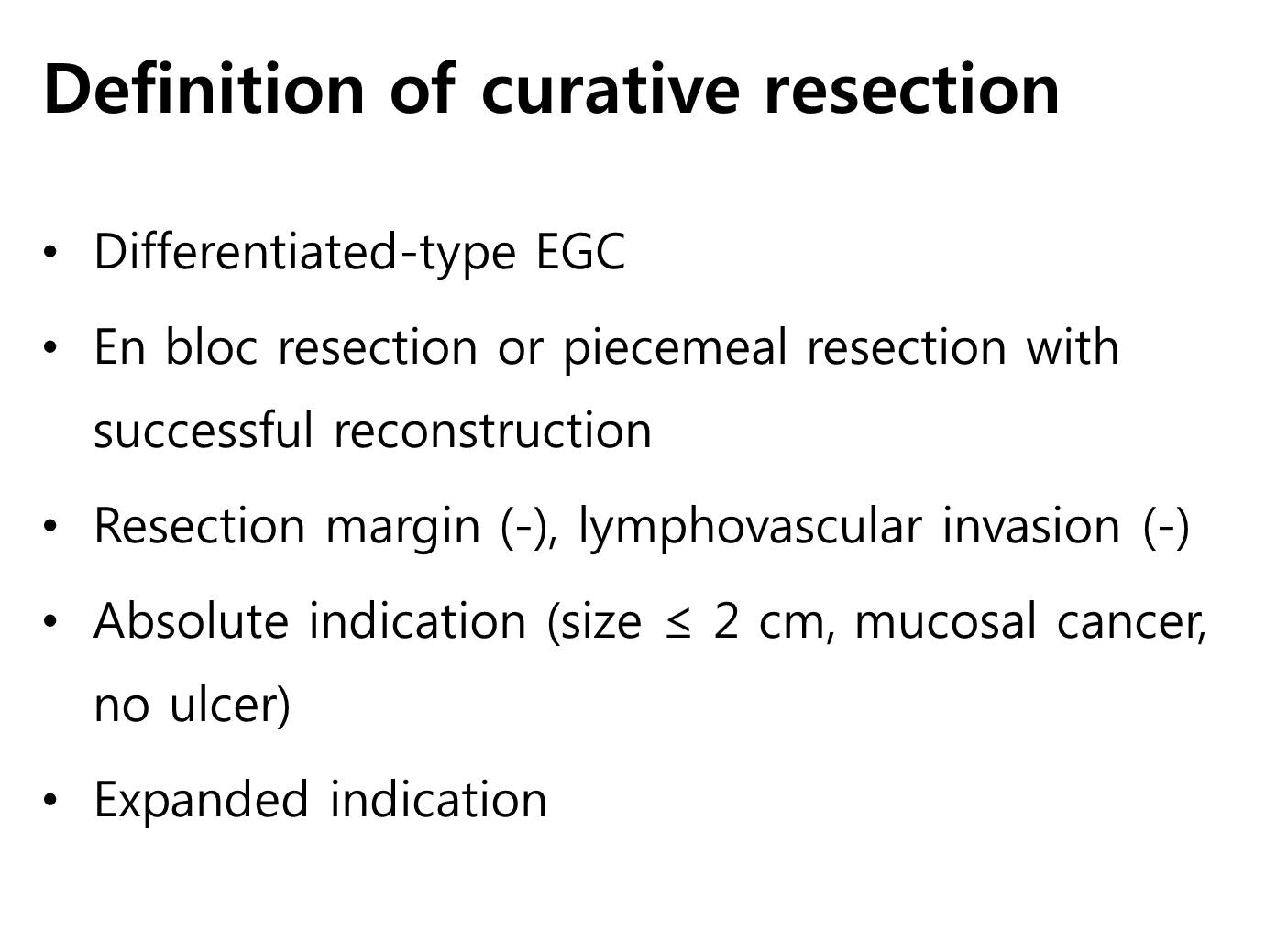
Definition of curative resection is shown in this slide. All cases have differentiated histology, and both cases within absolute indication and expanded indication were included.

This is the immediate endoscopic outcome. The rate of non-curative resection is 16.7%.
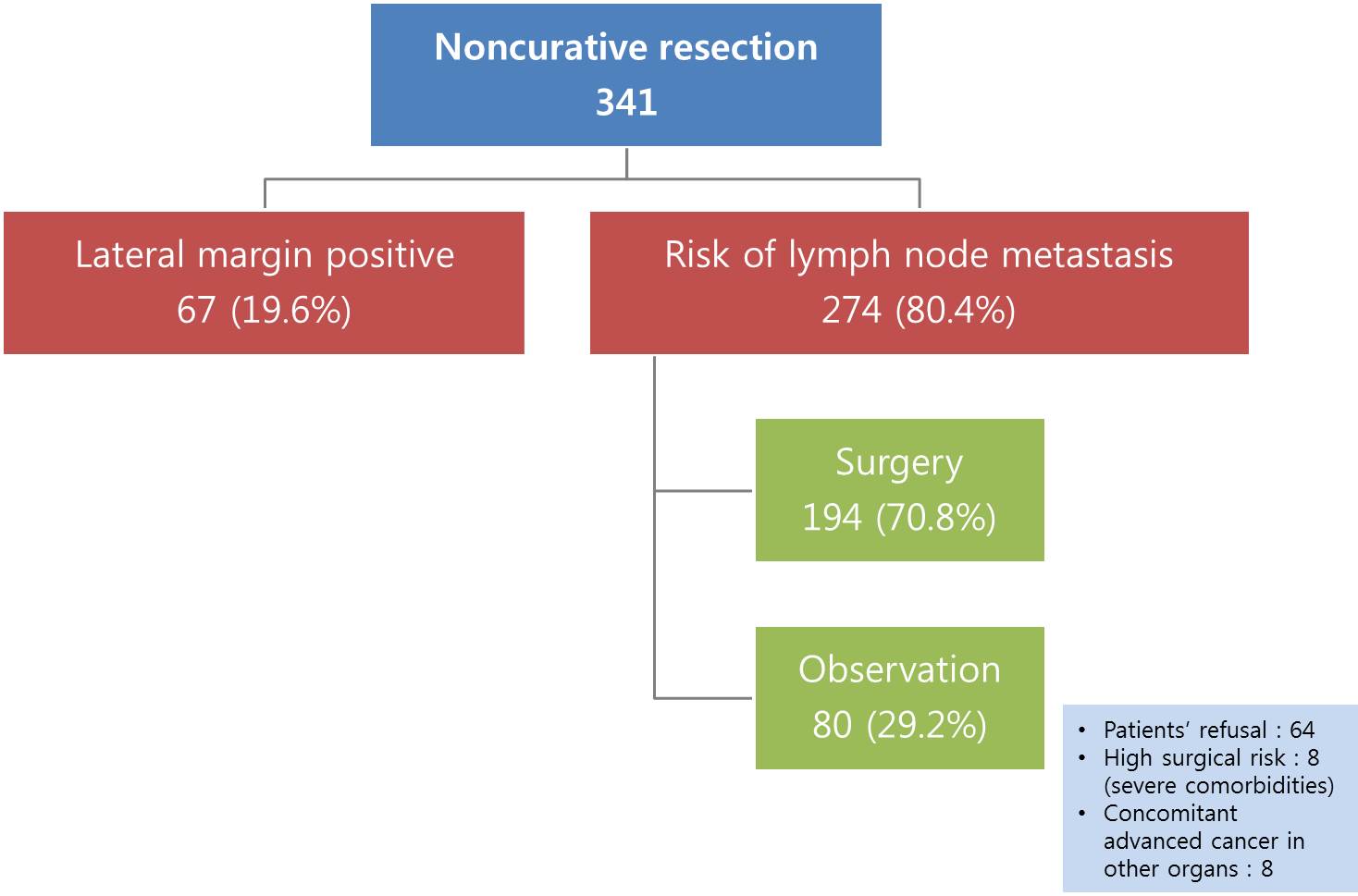
There are two subgroups in non-curative resection. One is lateral margin positive only group, and the other is cases with risk of lymph node metastasis. Lateral margin positive cases were excluded in this study, because most of them are treated by additional endoscopy. In cases with risk of lymph node metastasis, 70% were operated, and 30% were observed without surgery. The main reason of observation is patient’s refusal to surgery.
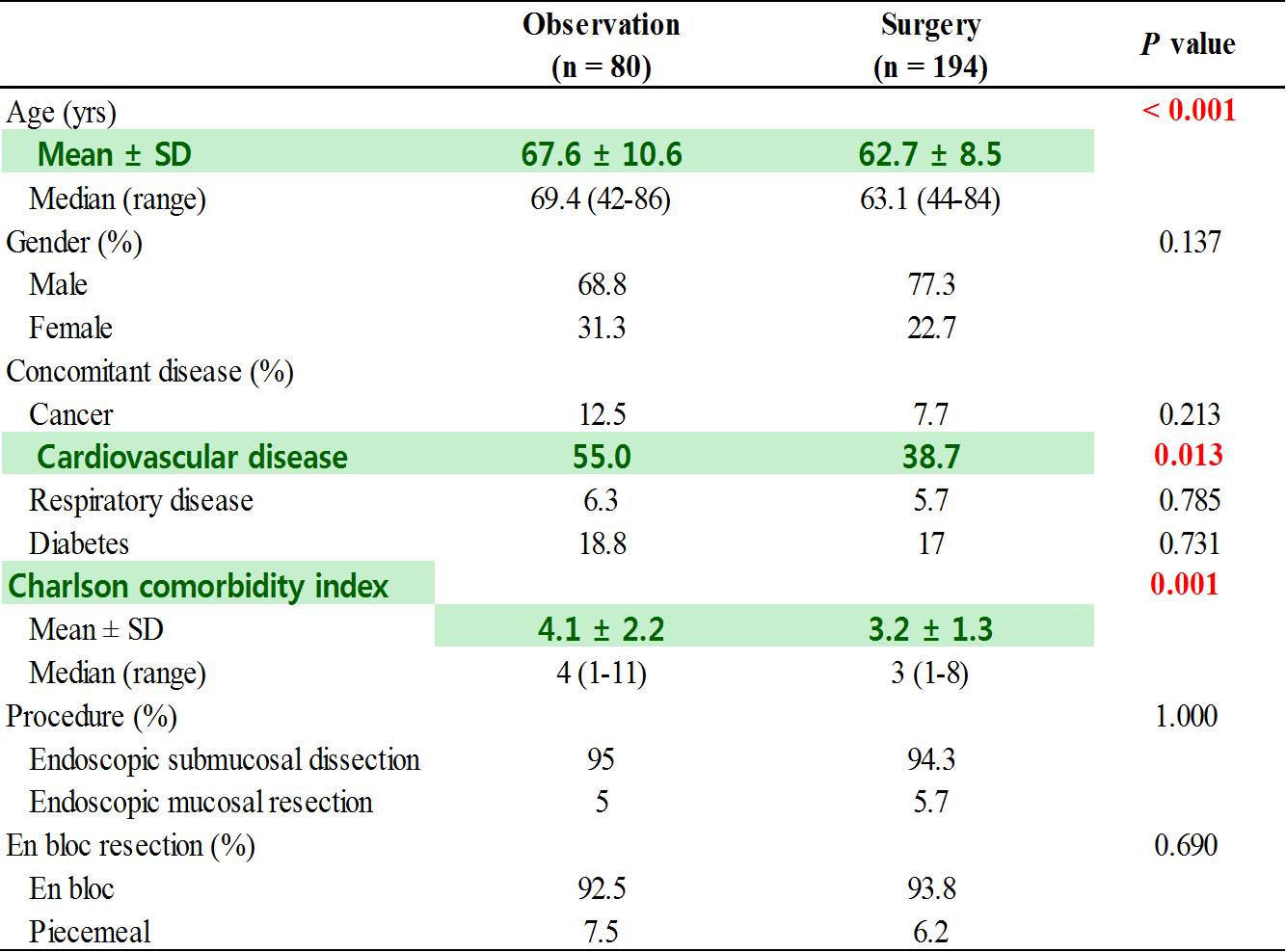
When we compared the two groups, patients in the observation group were older and have more cardiovascular diseases, and have higher Charlson comorbidity score…
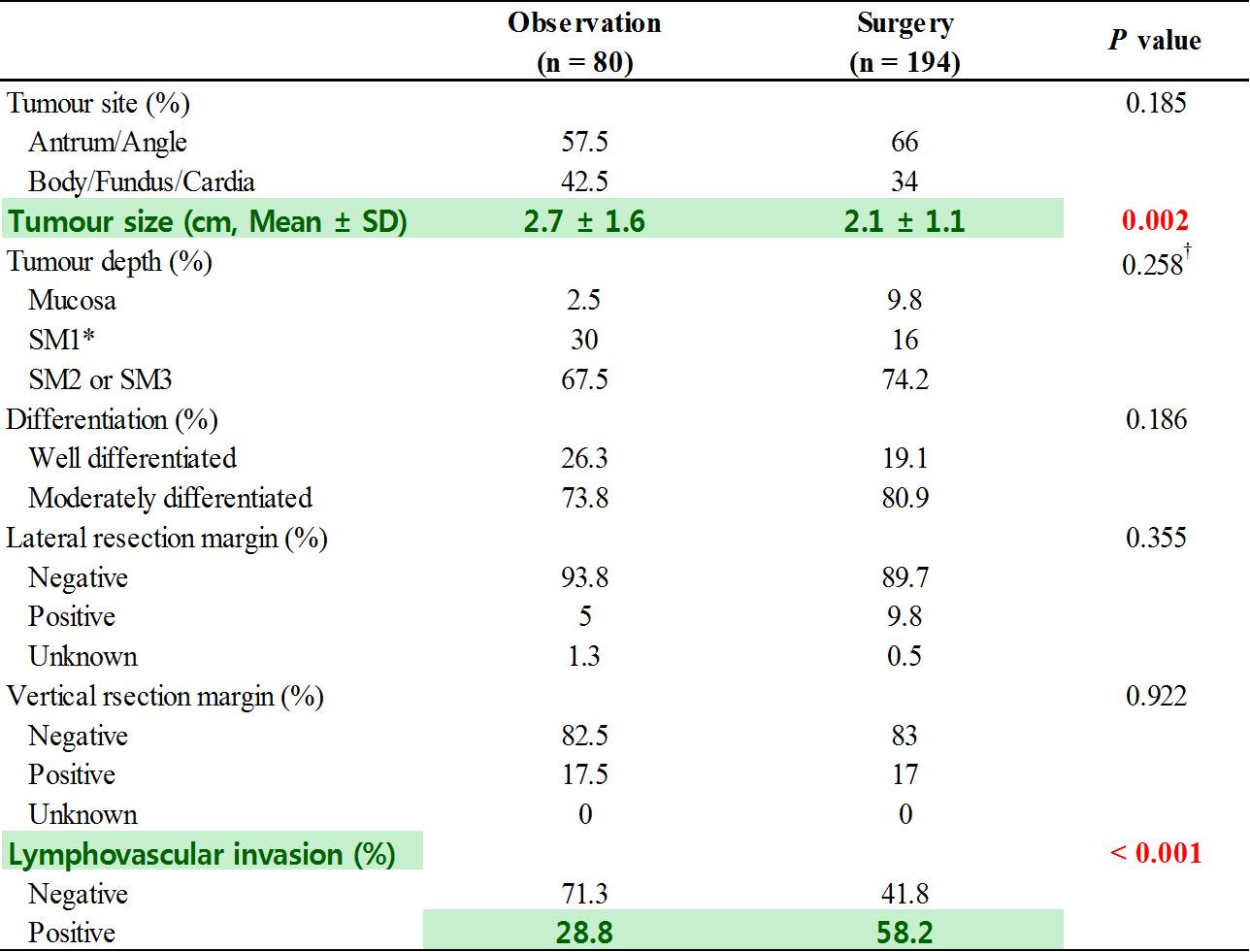
And have bigger tumor. The rate of lymphovascular invasion was higher in the surgery group.
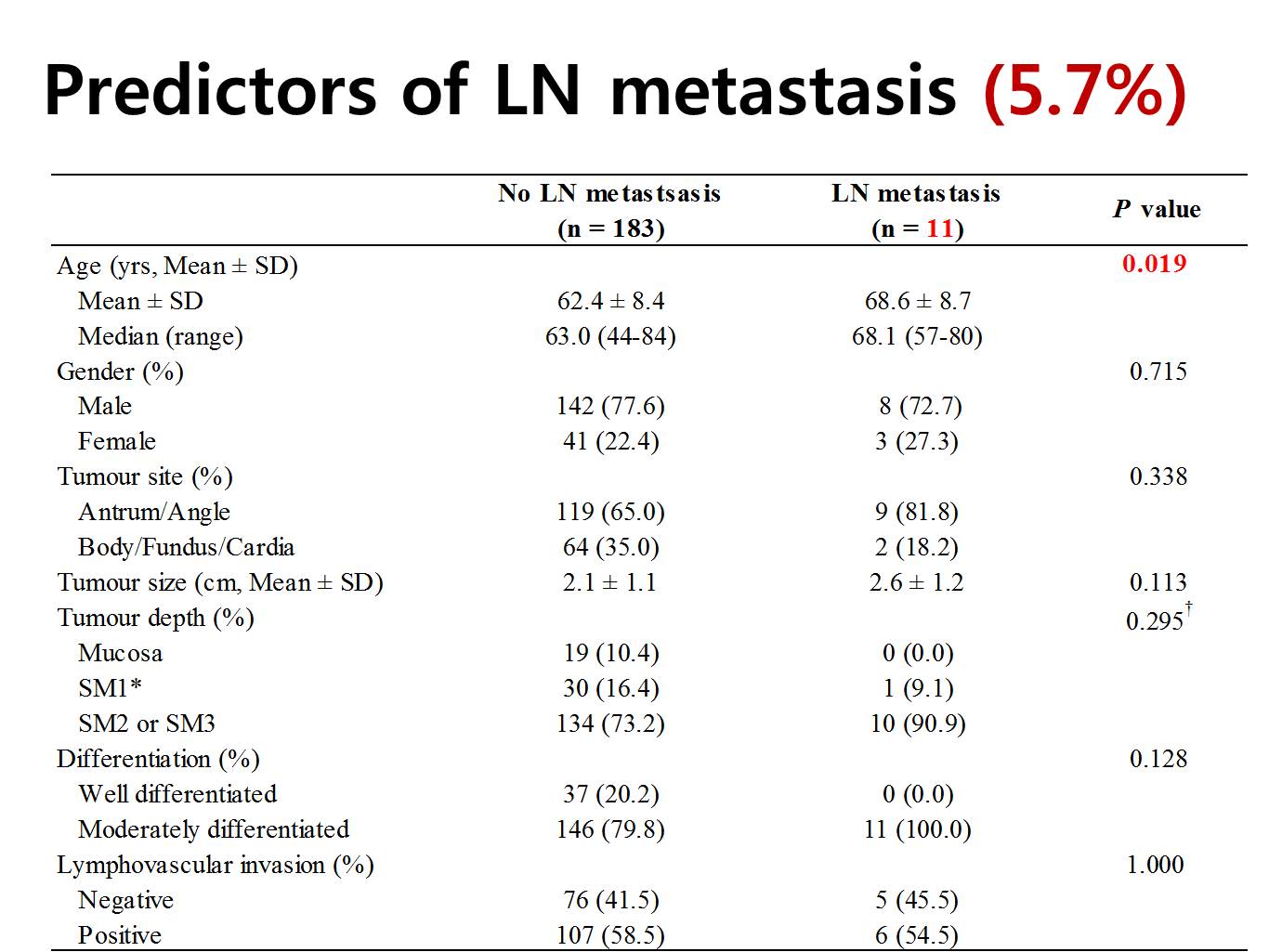
In the surgery group, 11 have lymph node metastasis, which means 5.7%. Patients with lymph node metastasis were older. To our surprise, the rate of lymph node metastasis was not different by the tumor size, depth of invasion, histological differentiation, and lymphovascular invasion in the endoscopically resected specimen. So, basically we found no predictor of lymph node metastasis in this analysis.
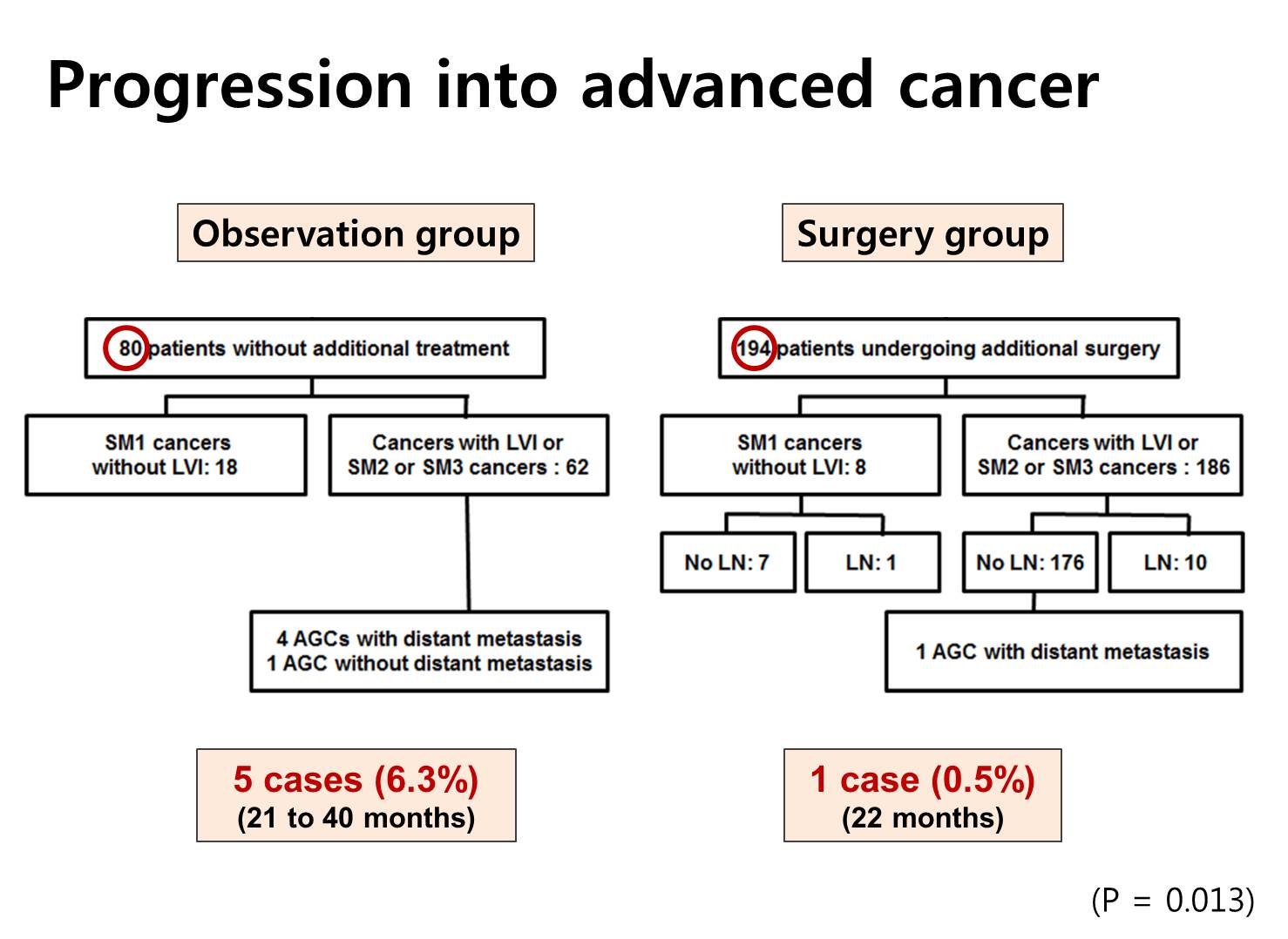
Rate of progression into the advanced cancers were different between 2 groups. Five advanced cancers were found in the observation group, and only one metastatic disease was found in the surgery group. This difference - 6.3% versus 0.5% - was statistically significant.
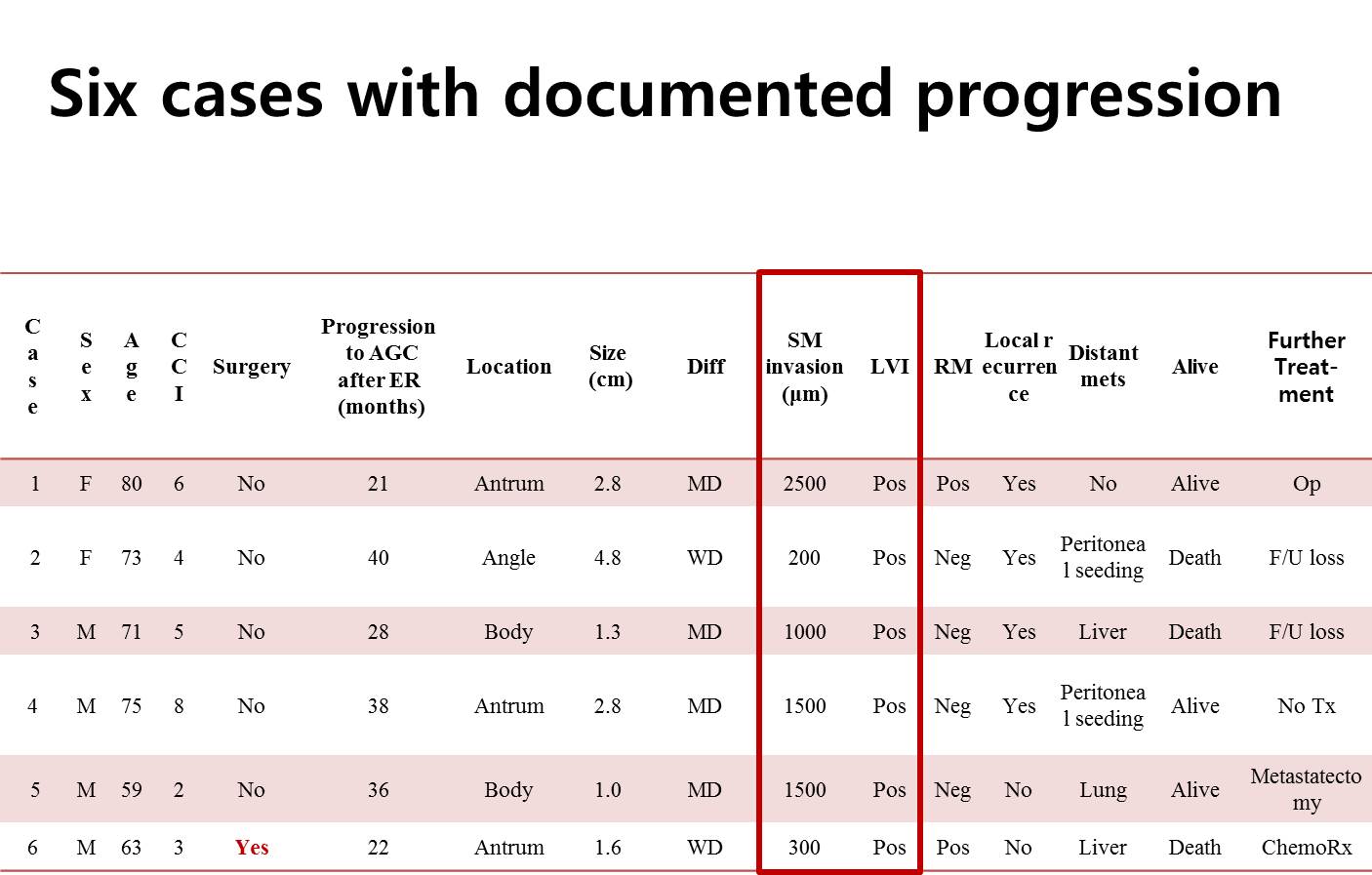
This is the summary of six cases with documented progression of gastric cancer. As you can see, all cases have submucosal invasion of more than 200 micrometer and all have evidence of endolymphatic invasion.

The next two slides are the main findings of this study. We compared the overall survival by some factors. As you can see in the figures, age less than 65, low Charlson score, and additional surgery were related with longer survival.
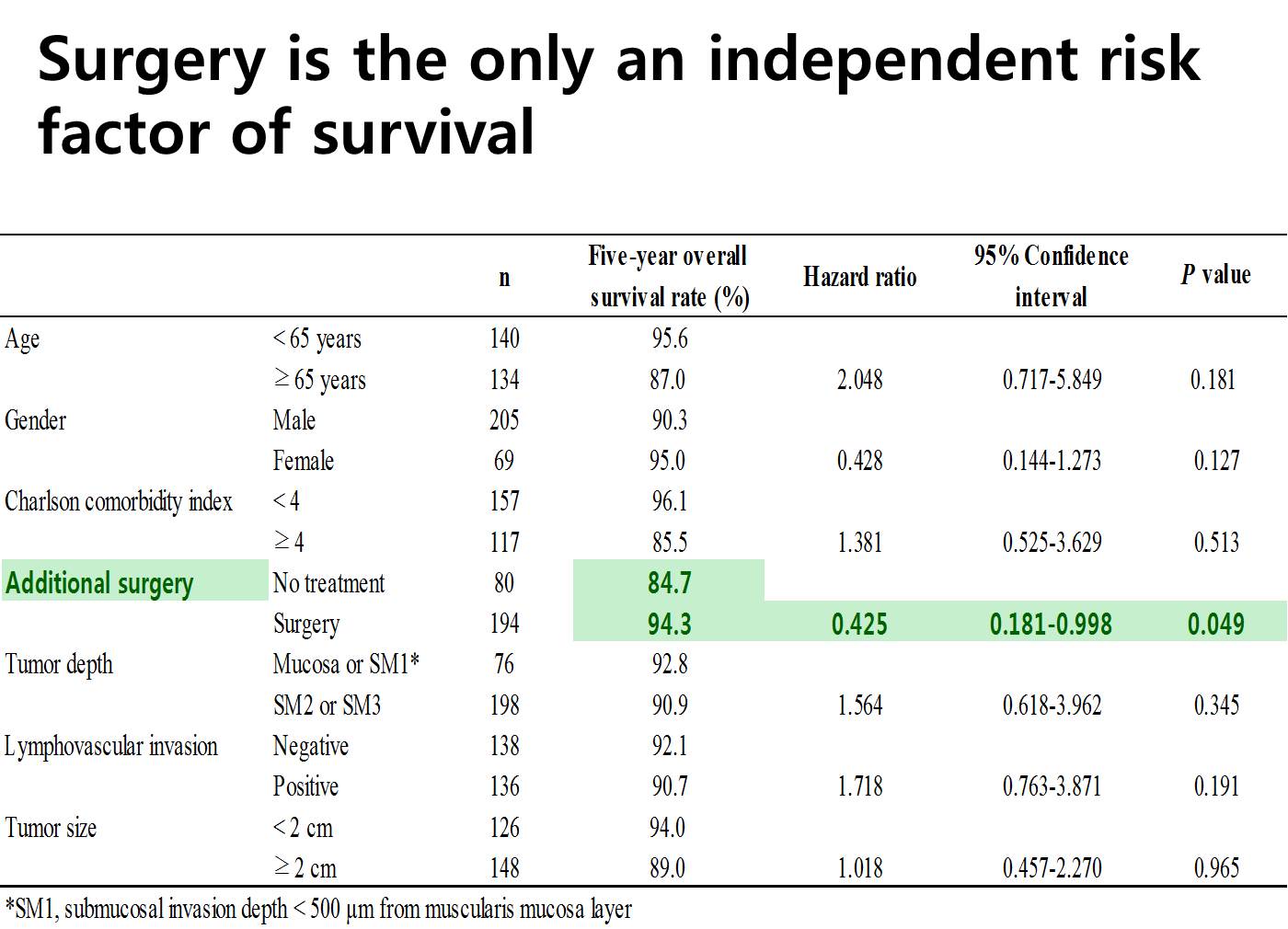
In the Cox proportional hazard model, additional surgery was the only significant independent factor related to the longer survival. So surgery was beneficial for patients with non-curative resection after ESD.

From now on, I’d like to show you some of the interesting cases. The patient refused surgery, and multiple hepatic metastasis developed 28 months later.
The next case is very similar.
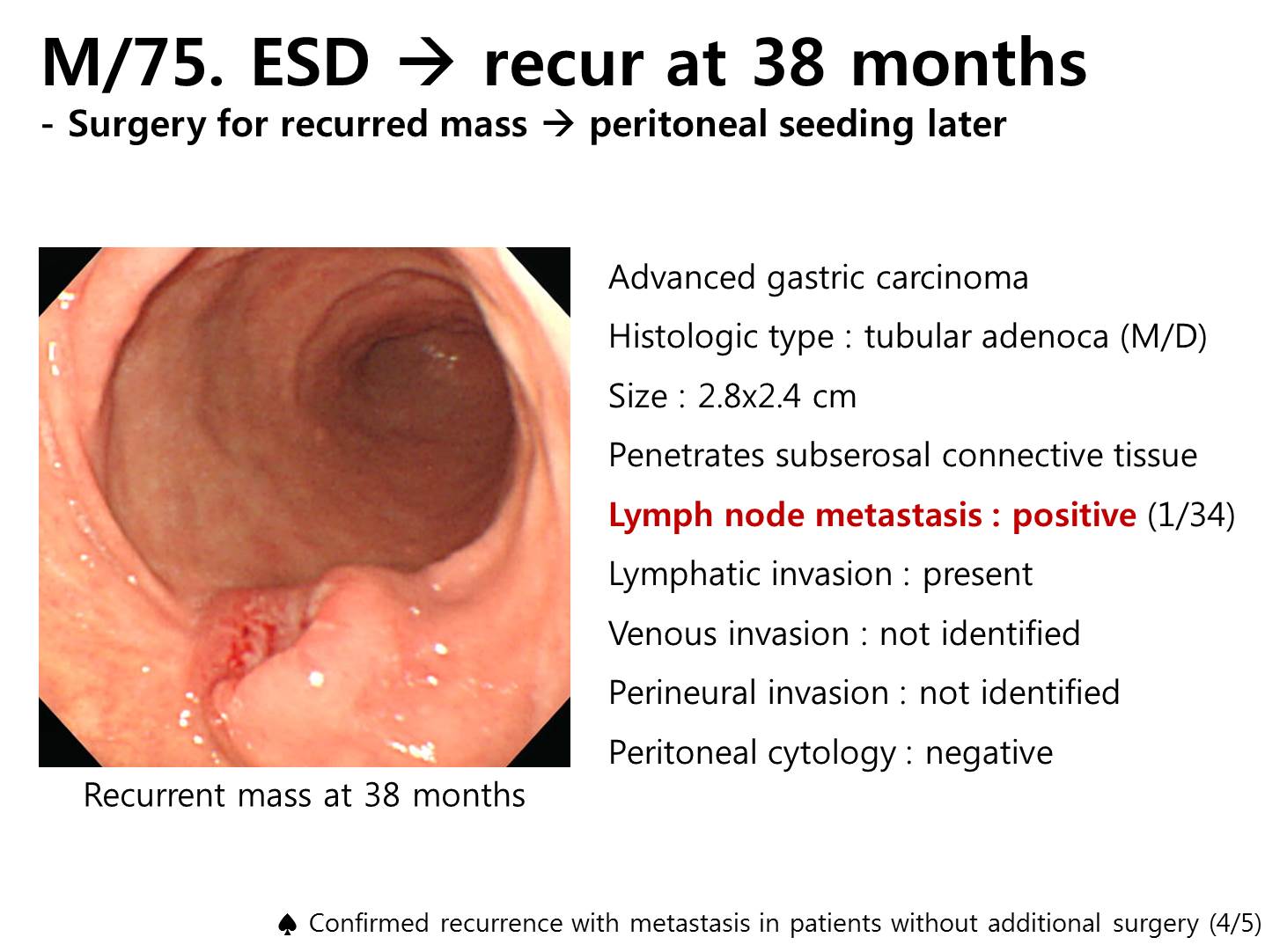
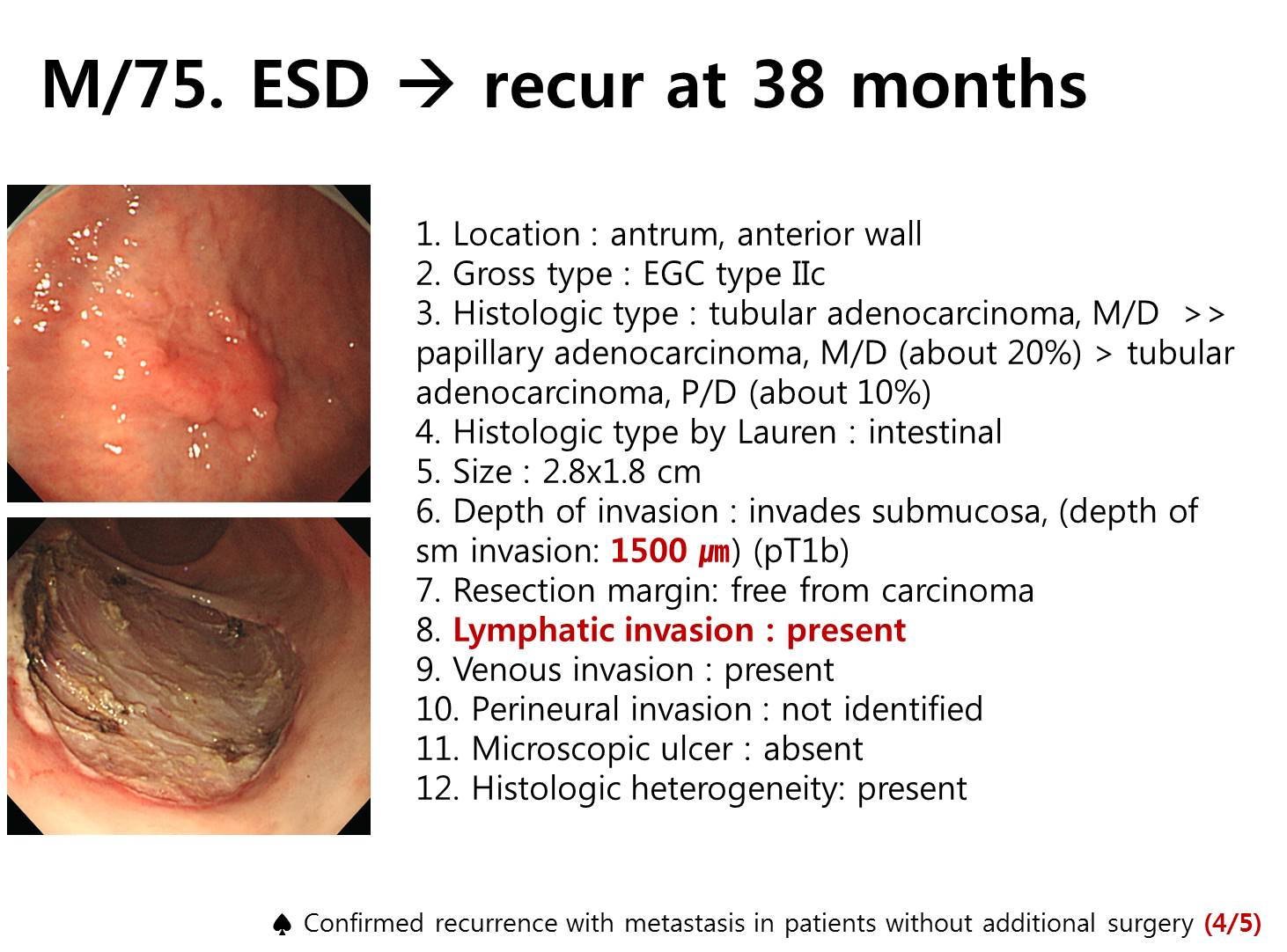
Advanced gastric cancer was found 38 months later. Subtotal gastrectomy with lymph node dissection was done. Depth of invasion was subserosal layer and one lymph node was involved.
However, peritoneal seeding was found during the follow up.
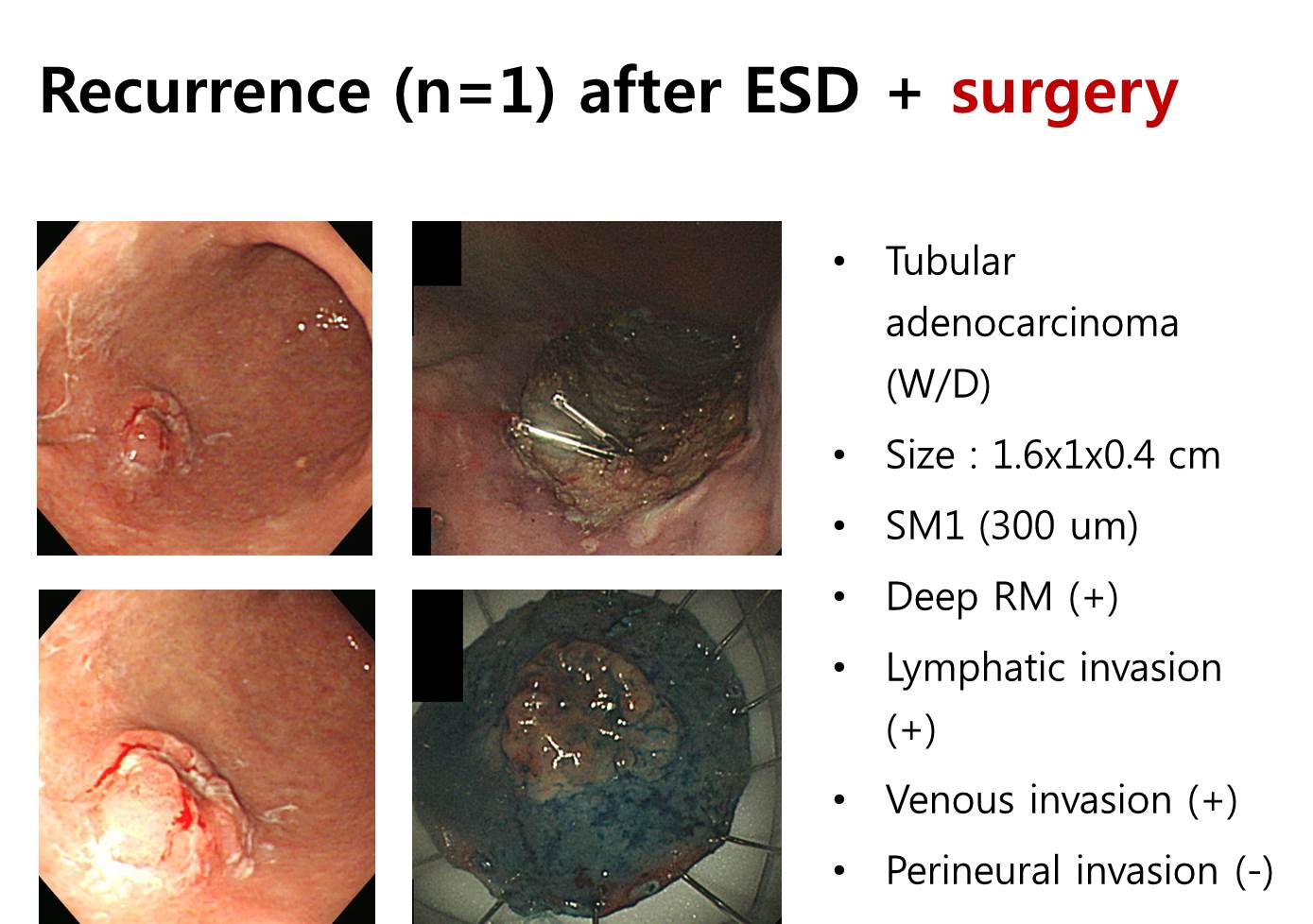
The third case shows that surgery cannot prevent all recurrences. Surgery was done immediately after non-curative resection by ESD.
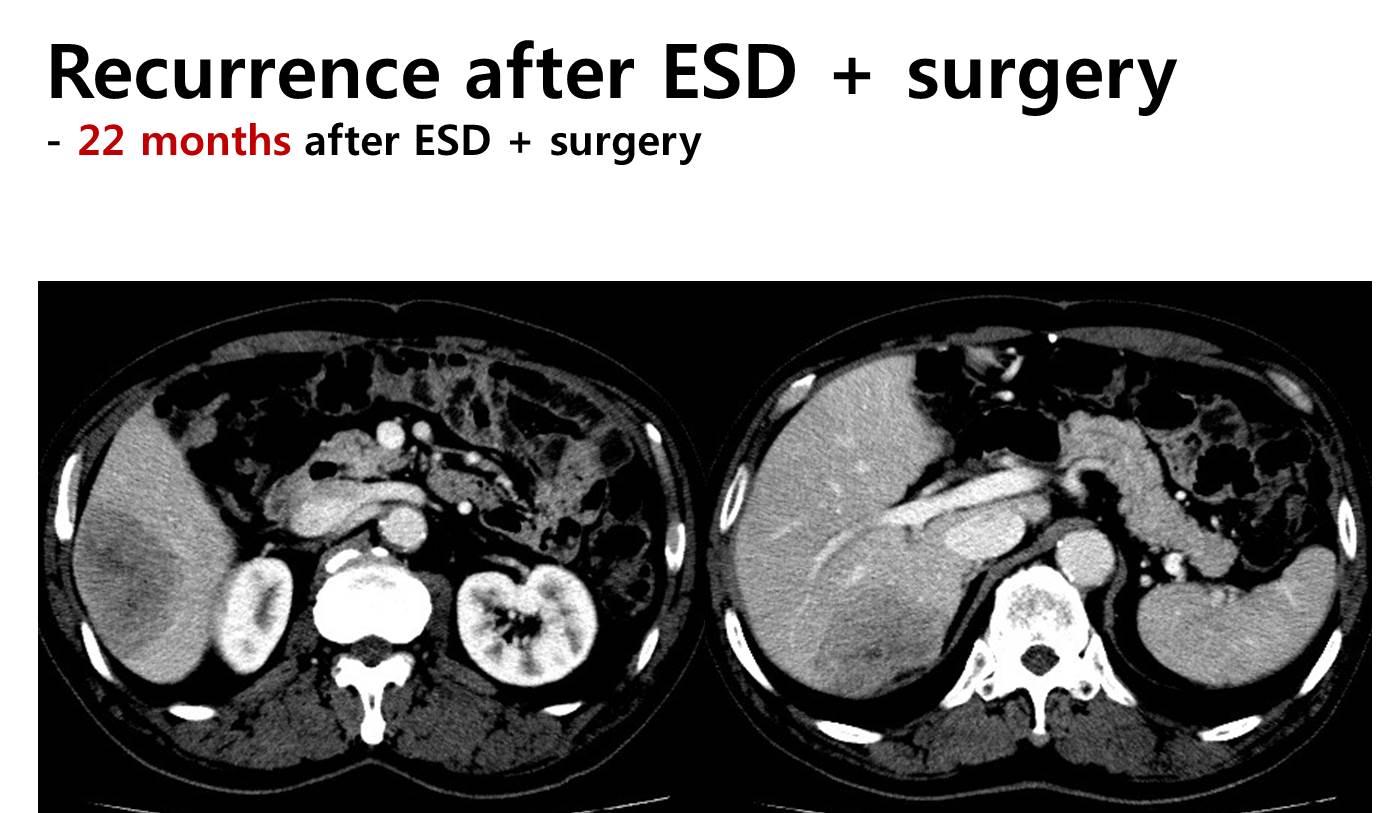
However, multiple hepatic metastases were found 22 months later.
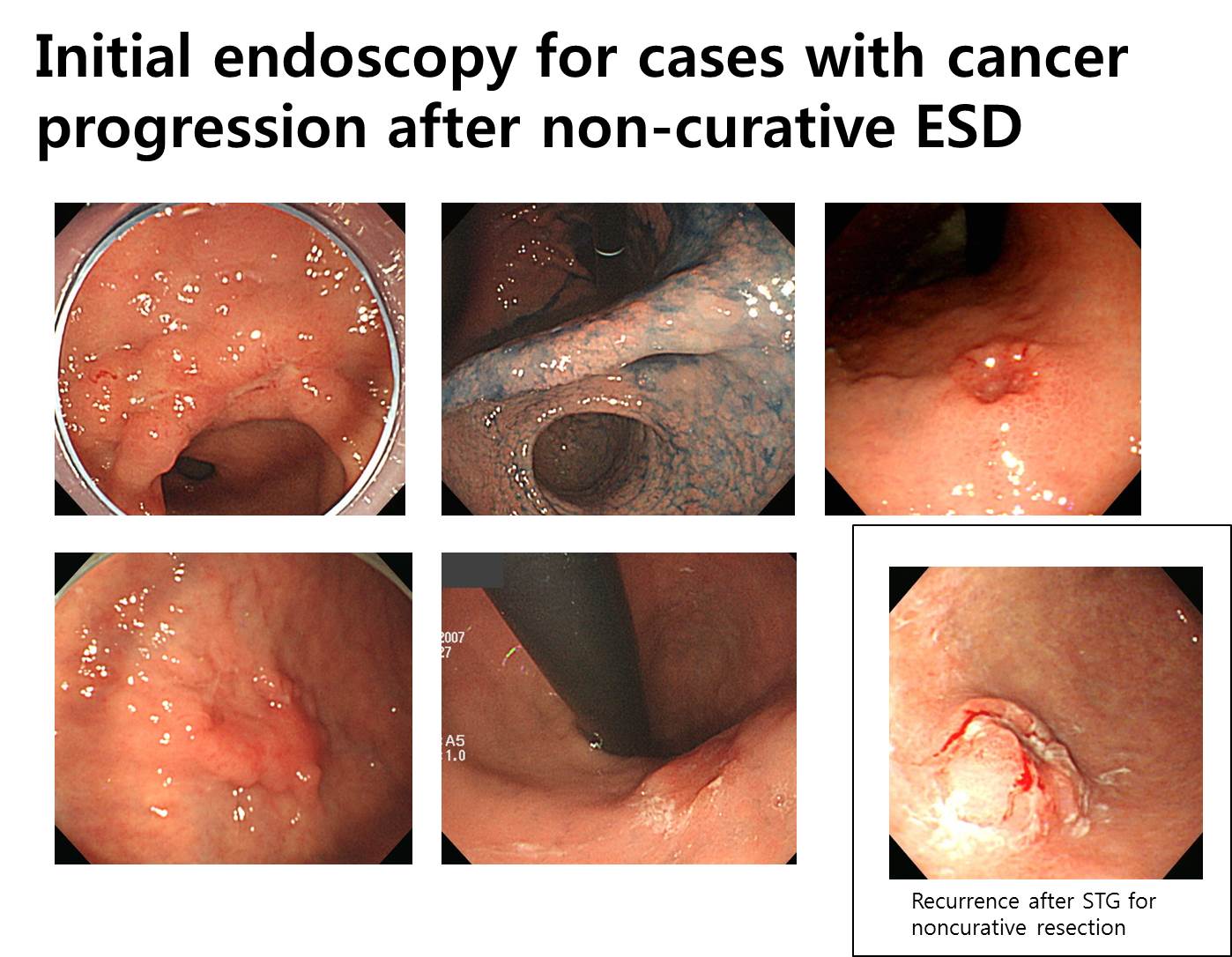
This is the initial endoscopy of the six cases. Some are elevated, some are depressed, and some are flat. There is no uniform characteristics.

Ladies and gentlemen. I’d like to conclude my presentation by saying that progression to advanced stage in non-curative resection without surgery is at least 6.3% within 40 months. In this setting, additional surgery confers a survival benefit and should be positively considered.
![]() [참고자료]
[참고자료]
2) Kim ER. Follow-up after non-curative resection Br J Surg 2015
© 일원내시경교실 바른내시경연구소 이준행