EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Ulcer or ulceration in ESD] - 終
[Ulcer or ulceration in ESD] - 終
| Position statement on ulcer in the evaluation of EGC (2025-6-17. 이준행) |
| 저는 늘 고민합니다. EGC III 처럼 명백한 cratered ulcer(서양 사람들의 표현입니다)는 ulcer라고 부릅니다. EGC IIc처럼 얕은 함몰부는 shallow ulcer 또는 deep erosion이라 부릅니다. 논리적이어야 하고 politically safe 해야 하고 금전적으로 환자가 손해보면 안 되므로 상황에 따라 선택할 수 밖에 없습니다. Fold 소견이 뚜렷하고, cratered ulcer는 없지만, 그래도 ulcerative lesion이 있는 환자에 준한 치료를 해야 겠다(= 수술을 보내야겠다)고 생각되면 뜸금없이 ulcer finding이라는 말을 씁니다. 다른 식으로 말하면 ESD를 해야 할 것 같으면 ulcer라는 표현을 피하고, 수술을 해야 할 것 같으면 ulcer 혹은 ulcer finding이라는 표현을 선택합니다. 요컨데 육안소견에 근거하여 중립적으로 용어를 선택하면 되는 일을 이것 저것 모두 고려하여 문제가 생기지 않도록 골라 쓰고 있다는 말씀입니다. 왜일까요? Clear한 정의가 없기 때문입니다. 누구나 동의하고 practically 적용할 수 있는 정의가 없으므로 전문가들마다 자기 방식으로 용어를 선택하고 있는 실정입니다. 의학에는 이런 것이 아주 많습니다. Science이면서도 art입니다. Science 아닙니다. 책으로 배울 수 없습니다. 선생과 함께하는 긴 시간이 필요합니다. 도제교육과 끝없는 토론. 의학은 이런 것으로 유지되고 발전합니다. |
![]() 1. Ulcer, ulcerative lesion, ulcer findings, ulcer scar 등 용어의 혼선
1. Ulcer, ulcerative lesion, ulcer findings, ulcer scar 등 용어의 혼선
우리는 의학 용어가 엄밀하게 정의된 상태에서, 여러 전문가들에 의하여 비슷한 의미로 사용되고 있을 것을 기대합니다. 그러나 절대 그렇지 않습니다. 다양한 정의가 있거나 (= 정의가 여러개라는 말은 정의가 없다는 말과 같습니다), 아예 정의가 없는 상태에서 사용되는 용어가 제법 많습니다. 조기위암 내시경 치료와 관련된 분야에서는 ulcer가 문제입니다. Ulcer, ulcerative lesion, ulcer findings, ulcer scar, UL (+) 등 많은 용어가 그야말로 대강 쓰이고 있습니다.
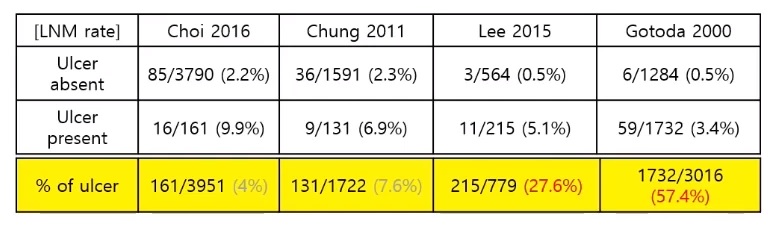
예를 들어 ulcer 혹은 ulcer finding에 대한 여러 연구를 보면 그 빈도가 천차만별입니다. 판정 기준이 다르다는 이야기입니다. 안수민 교수님께서 몇 개의 자료를 보여주셨습니다. Ulcer의 빈도가 4%부터 57.4%까지 차이가 있습니다. 유명한 2020년 Gotoda 연구에서 ulcer finding의 빈도는 mucosal cancer에서 57.4%, submucosal cancer에서 61.5%였습니다. 점막암과 점막하암에서 ulcer finding이 절반 이상이라는 것은 Gotoda 연구에서 사용된 ulcer finding이라는 용어는 적어도 우리가 생각하는 ulcer와는 전혀 다른 무엇이라는 말입니다. 그런데 해당 논문에는 ulcer finding에 대한 정의가 없습니다.
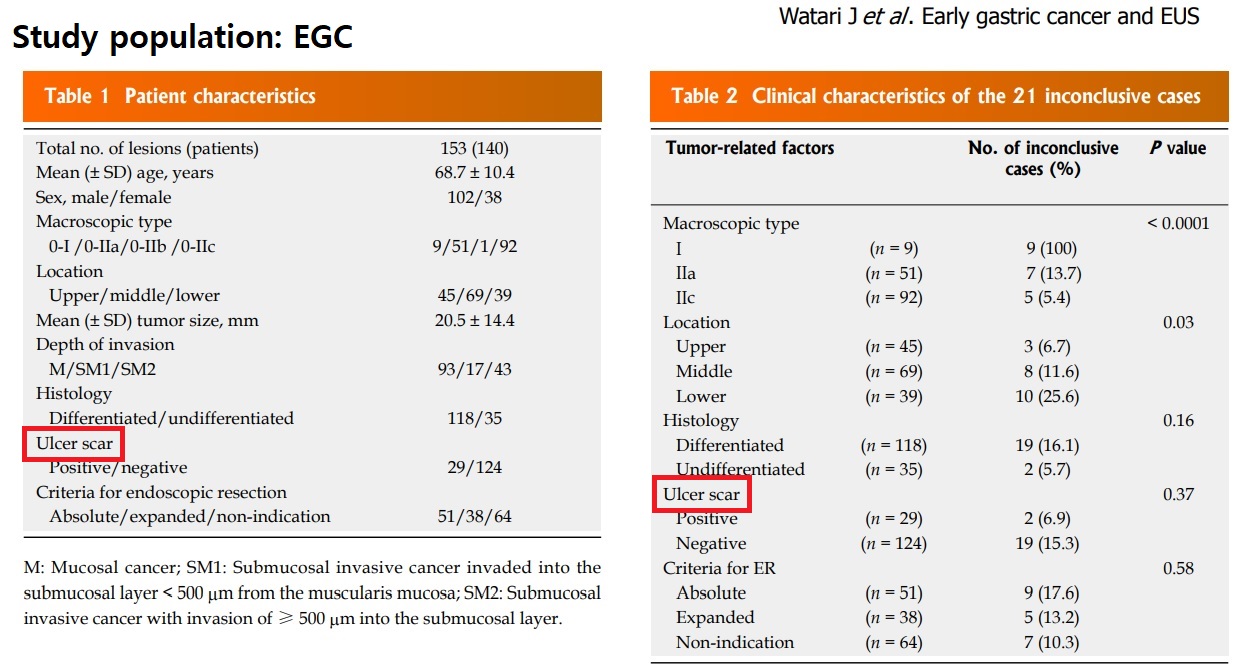
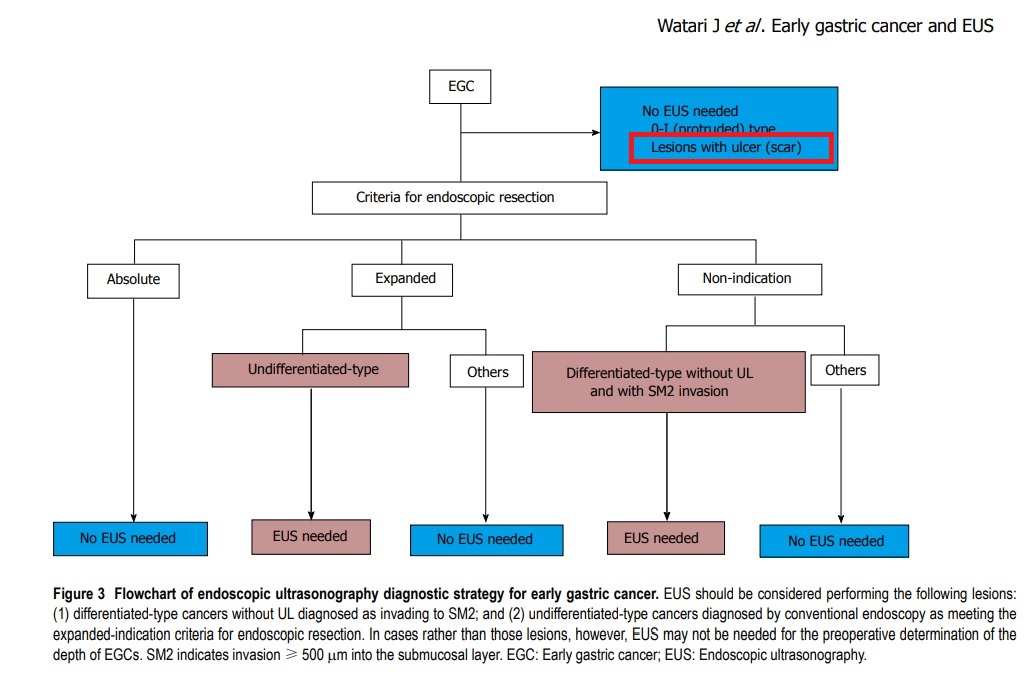
한 일본 연구(Watari 2016)에서 UL (+), UL (-)라는 용어가 쓰이고 있는데 표에서는 ulcer scar라는 말로 바꿔 표현하고 있습니다. 거의 같은 의미로 쓰인 것 같습니다. 그림 3에서는 ulcer (scar)라고 scar를 괄호로 감싸고 있습니다. 우리 생각에 ulcer와 ulcer scar는 전혀 다른 것인데 도대체 어쩌라는 말인지 한국의 상식으로는 이해할 수 없는 일입니다.
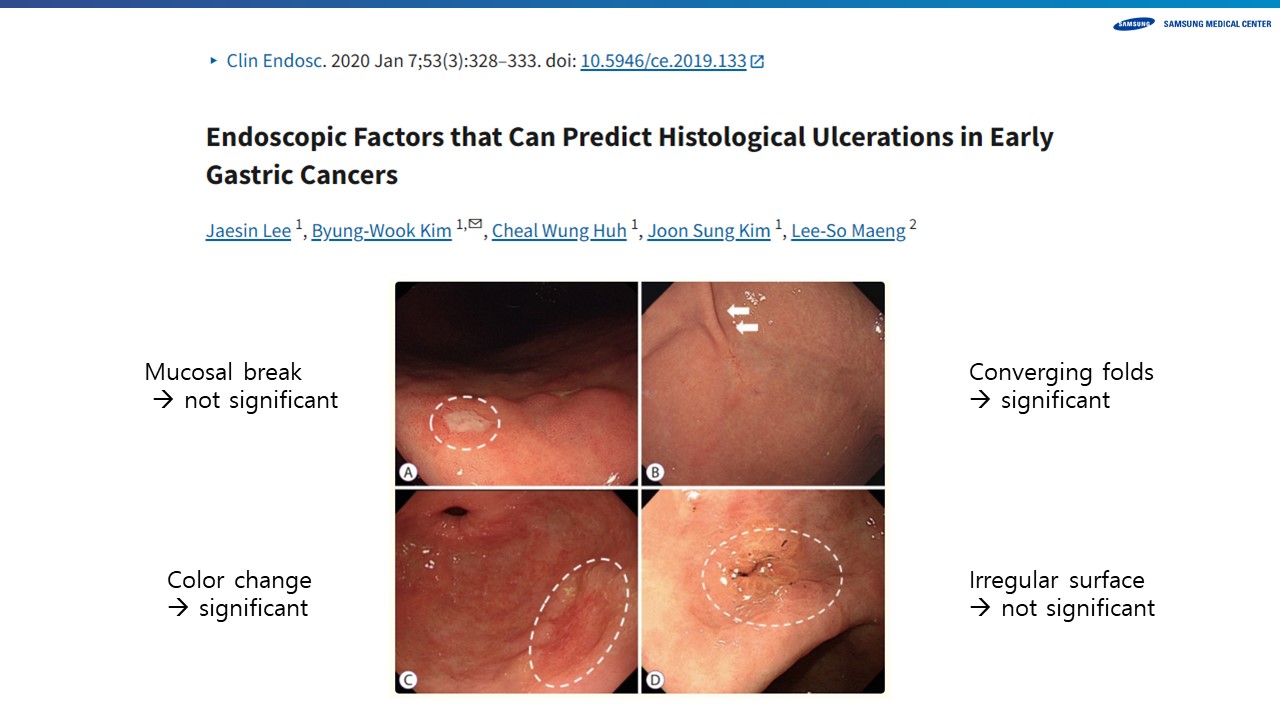
우리나라에서 병리를 정답으로 내시경 육안소견에 따른 ulcer 여부 판정에 대한 연구가 있었습니다.
병리를 정답으로 간주하면 내시경의 ulcer 정답률은 그다지 높지 않았습니다.
![]() 2. 2021년 일본 위암 가이드라인에 언급된 UL1과 관련된 부분
2. 2021년 일본 위암 가이드라인에 언급된 UL1과 관련된 부분
Histological predominance and intratumoral ulcerative fndings (UL)
A tumor consisting of components of both diferentiatedtype and undiferentiated-type carcinoma is, nevertheless, classifed into one of the two types according to the quantitative predominance. In addition, when more than one histological type is found in a tumor, all histological types are to be recorded in the order of quantitative predominance, e.g., tub2>tub1. The diagnosis of UL1 is principally made based on the histological evidence of ulcerative fndings. However, the histological diagnosis of UL is sometimes difcult because of a biopsy-derived scar. Thus, endoscopic and/or radiological evidence should also be taken into consideration when making a conclusive diagnosis. A biopsy-derived scar is usually observed histologically as fbrosis restricted to small areas just beneath the muscularis mucosae. If it cannot be discriminated from the ulcer scar, it should be classifed as UL1.
2021 일본 위암 가이드라인 6th의 좌측 병리 부분에서 UL의 결정은 principally 병리에 따른다고 되어 있다. 그러나 시술 전 내시경 소견에서도 버젓이 UL이 언급되어 있다.
2021 일본 위암 가이드라인 6th의 Indication 별 림프절 전이 부분.
UL1은 histology 진단인데 잘 모르겠으면 endoscopy나 radiology를 참고하라는 병리의사들의 제안이 있었던 것 같습니다. (일본은 병리 의사들의 power가 막강합니다.) 그러나 ESD candidate를 정할 때에는 병리가 없으므로 내시경 소견을 따를 수 밖에 없을 것 같습니다. 그런데 도대체 ulcerative findings가 무엇일까요?
![]() 3. 2023년 우리나라 병리 가이드라인에 언급된 ulcer관련 내용
3. 2023년 우리나라 병리 가이드라인에 언급된 ulcer관련 내용
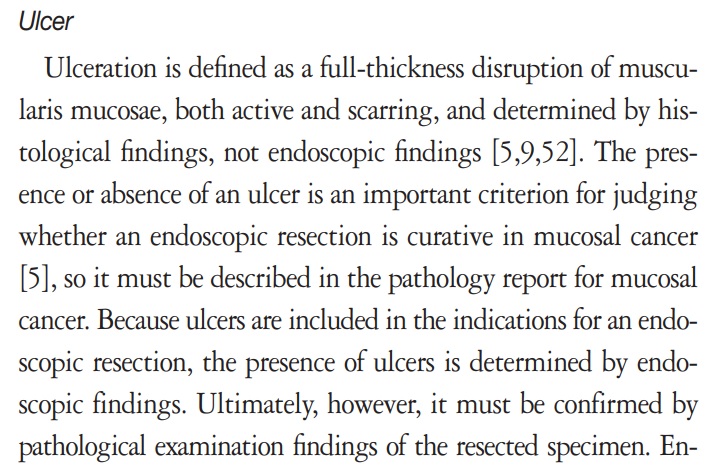
Ulceration is defined as a full-thickness disruption of muscularis mucosae, both active and scarring, and determined by histological findings, not endoscopic findings. The presence or absence of an ulcer is an important criterion for judging whether an endoscopic resection is curative in mucosal cancer, so it must be described in the pathology report for mucosal cancer. Because ulcers are included in the indications for an endoscopic resection, the presence of ulcers is determined by endoscopic findings. Ultimately, however, it must be confirmed by pathological examination findings of the resected specimen. Endoscopic diagnosis is difficult in the absence of a mucosal break, and ulcer-negative endoscopy findings with ulcer-positive pathology findings were reported in 4.6%-5.5% of cases.
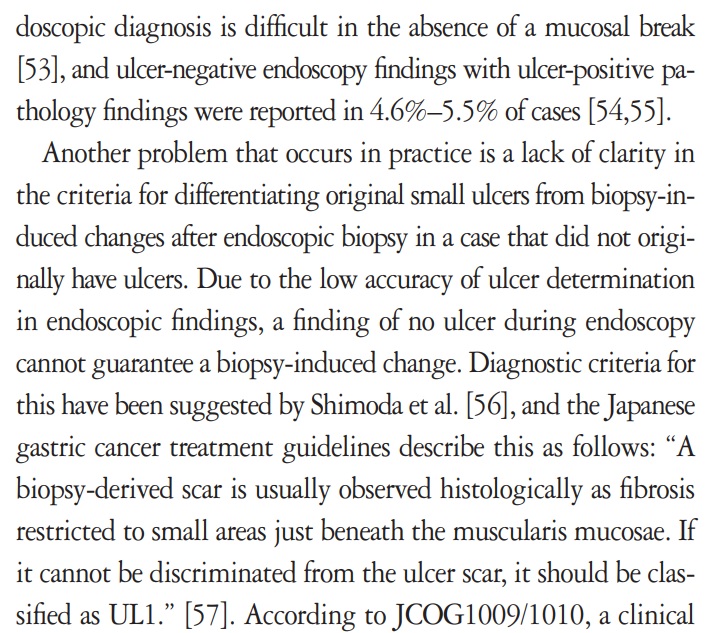
Another problem that occurs in practice is a lack of clarity in the criteria for differentiating original small ulcers from biopsy-induced changes after endoscopic biopsy in a case that did not originally have ulcers. Due to the low accuracy of ulcer determination in endoscopic findings, a finding of no ulcer during endoscopy cannot guarantee a biopsy-induced change. Diagnostic criteria for this have been suggested by Shimoda et al., and the Japanese gastric cancer treatment guidelines describe this as follows: “A biopsy-derived scar is usually observed histologically as fibrosis restricted to small areas just beneath the muscularis mucosae. If it cannot be discriminated from the ulcer scar, it should be classified as UL1.”
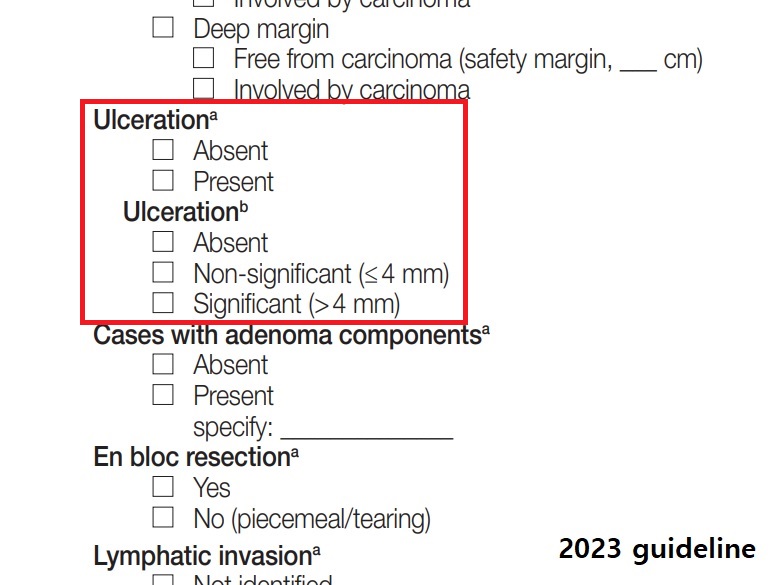
According to JCOG1009/1010, a clinical study on undifferentiated-type EGC: “UL was judged as present if the muscularis propria was completely disrupted and if fibrosis in the submucosal layer was observed to be wider than the range of disrupted muscularis propria.”. In our study group, ulcer size was measured in the ongoing GIPSG study on the criteria for curative resection, and the possibility of offering differentiation criteria for this problem was investigated. We found that the risk of lymph node metastasis with an ulcer of 4 mm or less was the same as in cases with no ulcer. Using that criterion, very small ulcers can be excluded from the risk factors for lymph node metastasis, which removes the need to differentiate them from biopsy-induced changes. The grading of ulcer size is reflected as a conditional element. The method for measuring the size of an ulcer is similar to that used to measure the submucosal invasion width. If an ulcer (full-thickness disruption of the muscularis mucosae) is observed on only one section, write the actual size measured on the slide. If it is observed across two or more slices, write the larger of the following two values: (1) the actual size measured on the slide with the largest disruption size or (2) the number of slices spanned by the disruption×2 mm (thickness of slice). The ulcer size is measured only within the tumor. If the ulcer spans the tumor and surrounding mucosa, measure the ulcer size only within the tumor area.
같은 병리 가이드라인의 ESD report form을 보면 더 이해하기 어려운 부분도 있습니다. 4mm 기준으로 나누는 것인입니다. 본문을 읽어보면 조직검사에 의한 변화를 림프절 전이 위험에 포함시키지 않기 위한 노력 같습니다. 어렵습니다.
![]() [FAQs]
[FAQs]
Web symposium에서 비슷한 증례를 토의한 바 있어 소개합니다. 이 환자는 MM 암이었습니다.

![]() [References]
[References]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.