EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [기능성 소화불량증. Functional dyspepsia. FD] - 終
[기능성 소화불량증. Functional dyspepsia. FD] - 終
1. Symptoms
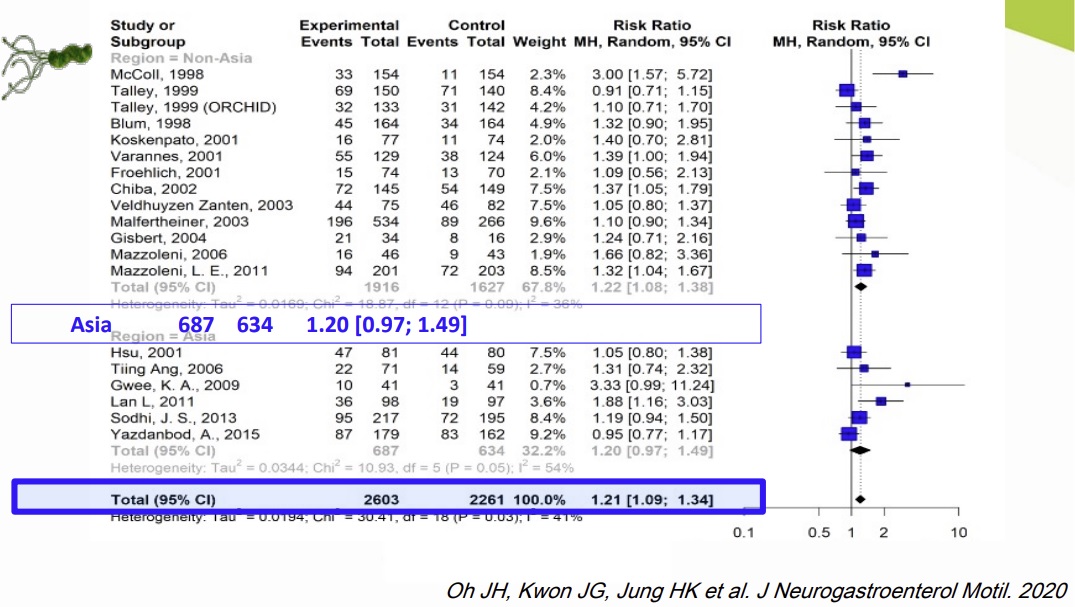
2. Helicobacter associated dyspepsia
4. Treatment
5. Symposiums
6. FAQs
7. References

2023-5-4. 순천향의대 이태희 교수. 닥터빌 log-in 要
설명만 잘 해드려도 좋아지는 환자가 많습니다.
경상도에서 오셨는데 검사해보기 전부터 좋아졌습니다. 설명의 힘입니다.
약간의 트름은 병이 아닐 수 있습니다.
![]() 1. Symptoms
1. Symptoms
| Subtype | Symptoms |
| PDS | postprandial fullness, early satiation |
| EPS | epigastric pain, epigastric burning |
2020-10-29 이풍렬 교수님 comment: Satiety와 satiation은 다른 의미입니다. Satiety는 배부른 상태이고 satiation은 물리는 것, 더 못 먹겠다는 느낌입니다.
![]() 2. Helicobacter associated dyspepsia
2. Helicobacter associated dyspepsia
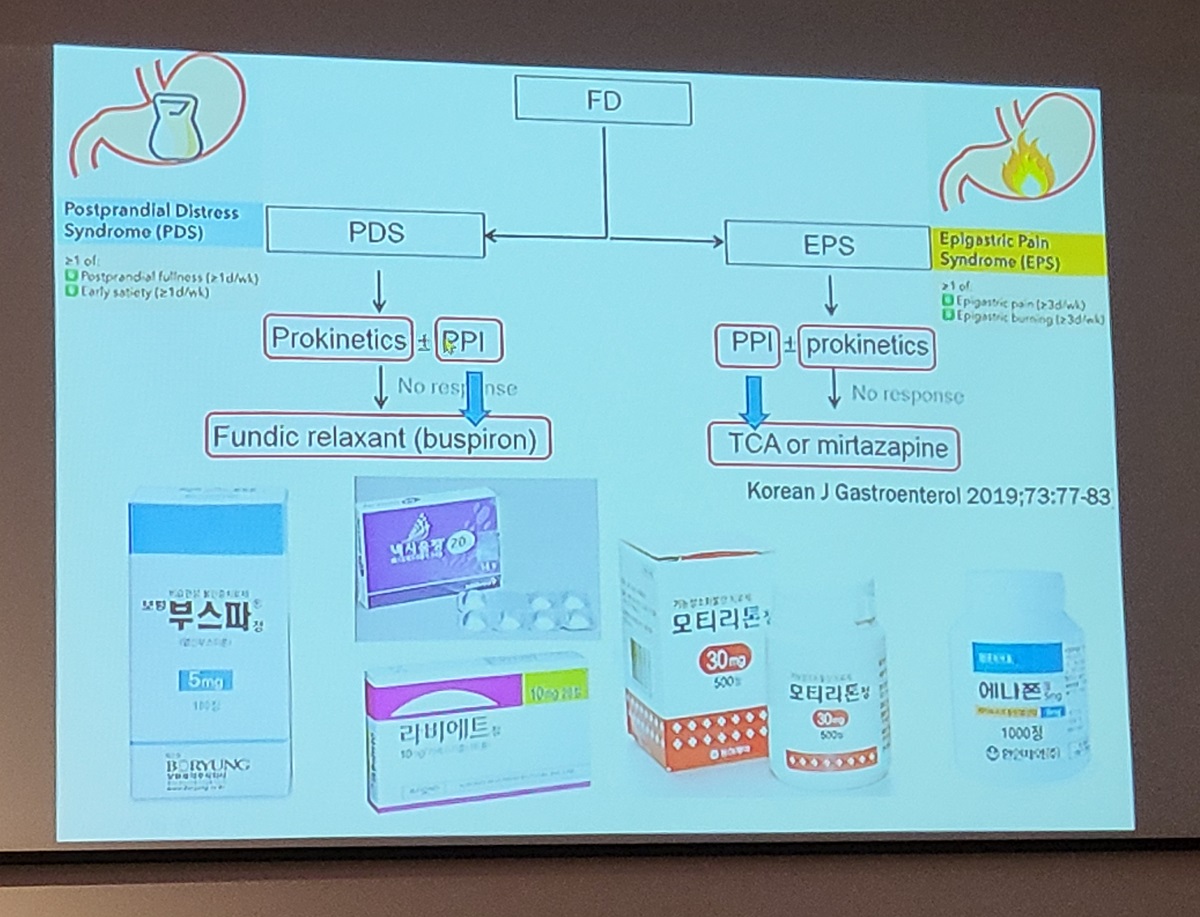
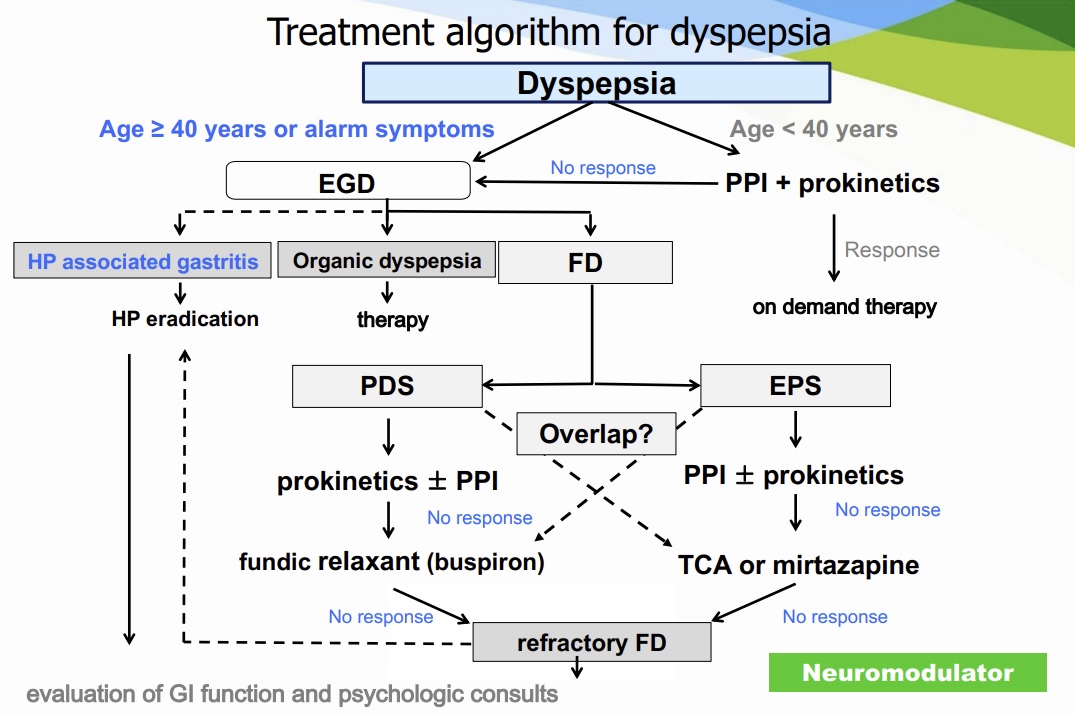
![]() 4. Treatment
4. Treatment
헬리코박터 제균치료 NNT = 14
증상 cure에 대해서는 14이지만 증상 호전에 대해서는 9, 제균 성공한 사람의 증상 성공은 4.5였습니다.
PPI NNT=10
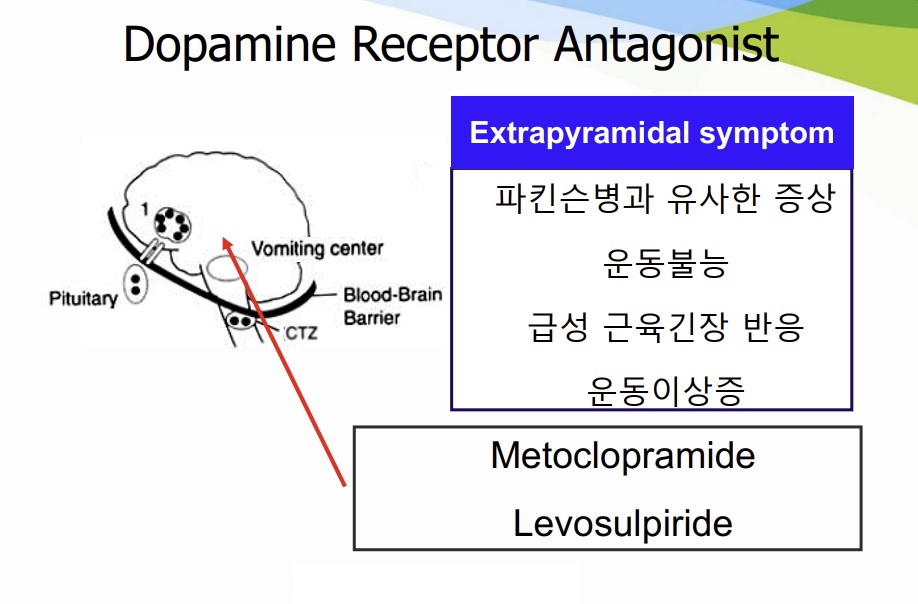
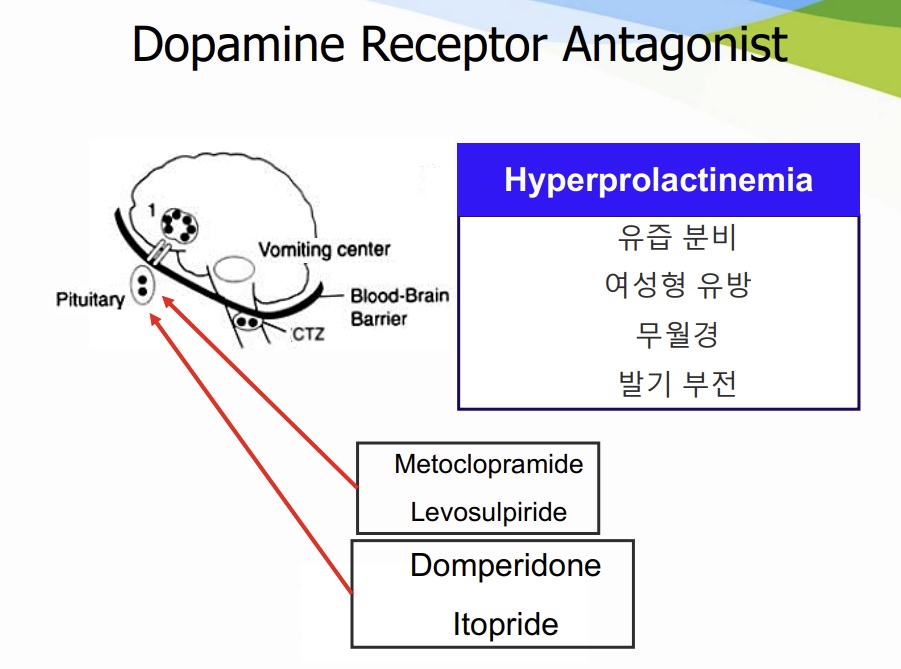
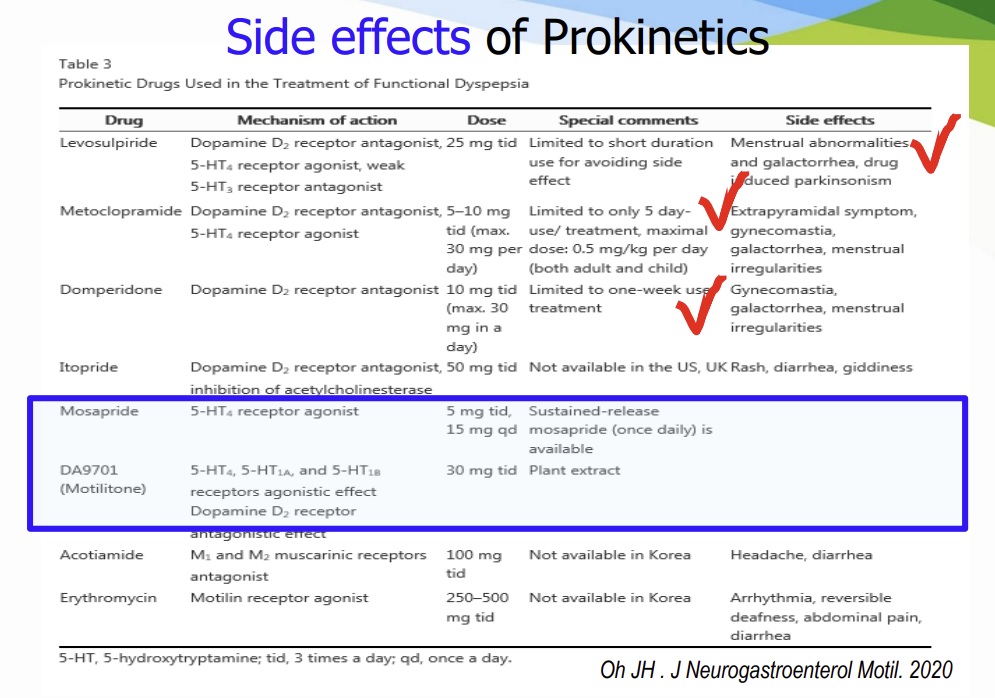
Prokinetics D2 antagonist NNT = 12 (Metoclo, motilium은 심장 부작용, 신경 부작용 우려가 있어서 mosapride가 많이 사용되고 있습니다.)
Acotiamide (Z-338) fundus relaxing and gastroprokinetic properties. NNT=6로 cisapride와 비슷한 수준인 것으로 생각됨.
* 참고: Clin Gastroenterol Hepatol 2018 리뷰
![]() 5. Symposiums
5. Symposiums
[2013-12-15] 기능성 소화불량증 집담회
2013-12-15. 기능성 소화불량증 집담회
2013-12-15. 기능성 소화불량증 집담회
[2017-6-17] 연세대학교 강남세브란스 심포지엄. Recent update of pathogenesis of functional dyspepsia. Hiroto Miwa (Hyogo, Japan)
소개의 말: It's great honor to introduce the next speaker professor Hiroto Miwa. After graduating Kagoshima University, he has been working as one of the best researchers in the field of functional gastrointestinal disorders. He is now the professor of Medicine, Hyogo College of Medicine and has been serving as the Vice president of Japanese Society of Gastroenterology. His topic today is funtional dyspepsia.
[Abstract] Dyspepsia is one of most common symptom and approximately 10% of general population has chronic dyspeptic symptoms without apparent organic causes, which is functional dyspepsia. Although FD is one of most important functional GI disorders, its pathogenesis is highly complicated. Possible pathogenic factors for FD includes, acid, H.pylori infection, motility disorders, gastric hypersensitivity and so on. Among those, it is well recognized that motility disorders and gastric hypersensitivity are the factors that directly induce GI symptom manifestation. However, what brings these physiological impairment has remained to be addressed.
Recently the importance of duodenum as a pathogenic center of functional dyspepsia has been gradually and widely recognized. Stimulus or inflammation to duodenum may bring the physiological impairment of the stomach. In fact, early reports demonstrated that intraduodenal application of lipid and acid alter visceromotor function of the stomach. These data suggest that stimulation to duodenum causes motility and sensory dysfunction of the stomach which result in generation of dyspeptic symptoms even in normal subjects. However, unlike the normal subjects, FD patients have dyspeptic symptoms chronically. What is the difference between duodenum of FD patients and that of normal subjects?
I assume duodenum of FD patients is primed, in other words, the duodenum of FD patients is ready to be activated. Two factors, which is presence of low grade inflammation and increased mucosal permeability may be responsible for this phenomenon. There are many reports describing low grade inflammation in FD patients, and the consensus seems to be made recently that both mast cells and eosinophils were increased especially in the second portion of the duodenum. One of the factors that brings the infiltration of eosinophils or mast cells in duodenal mucosa may be severe GI infection, which is known as “post-infectious FD”. Low grade inflammation must be a remaining of severe inflammation, however other clear causes for low grade infiltration is not known. The increased permeability of duodenal mucosa in FD patients was first reported recently by Belgium group, which was proven using biopsy specimens from duodenum mucosa and Ussing chamber. Regarding the factors that makes mucosal permeability increased in duodenal mucosa, much is not known. However, there is a recent report demonstrating that small intestinal permeability is increased in psychological stress condition, which is inhibited by pre-administration of mast cell stabilizer, suggesting that the psychological stress increases intestinal permeability by a mast cell-dependent mechanism possibly through CRH axis.
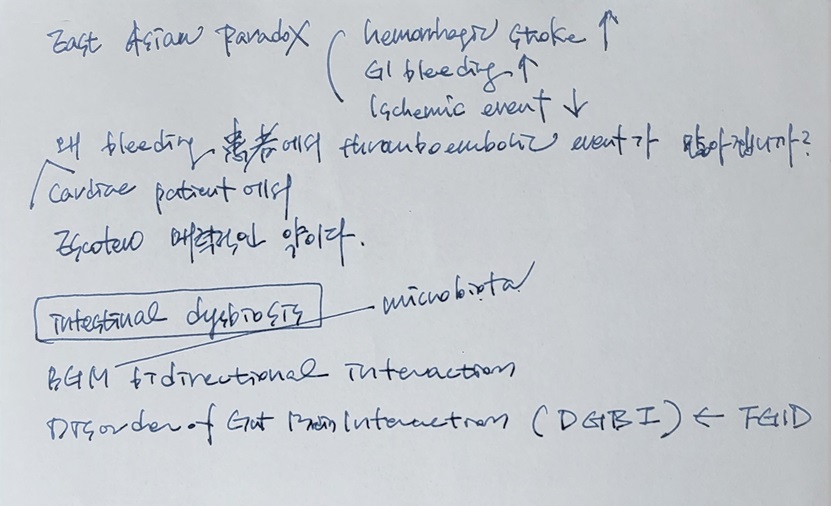
Very recently, the data have been presented suggesting the important role of bile in pathogenesis of functional dyspepsia. The researchers have shown that the bile was associated with increased mucosal permeability and especially secondary bile is correlated with the permeability in FD patients. Furthermore, they showed that one of several bile salt receptor in duodenum is increase in FD patients. It is a future matter of debate that “what’s happening in duodenum of FD patients?” Luminal factors or luminal antigens must play some roles in duodenum, which include acid, bile, nutrients including lipid, microbiome and product of microbiome. It would be possible that interaction of such factors with duodenum may explain pathogenesis of functional dyspepsia.
[이준행 질문] You emphasized the role of low grade inflammation and increased mucosal permeability of the duodenum in the pathogenesis of FD symptom development. I wonder what is the role of Helicobacter pylori in the development of chronic low grade inflammation or permeability change of the duodenal mucosa. After eradication treatment, could you tell me what kind of histological or functional changes happen?
[Miwa 선생님 답변] 헬리코박터 양성 FD 환자와 음성 FD 환자 사이에서 십이지장 염증이나 permeability는 차이가 없습니다. 헬리코박터 제균치료가 크게 효과적이지 않은 것은 이것 때문인 것으로 생각합니다.
[이동호 교수님 질문] 항염증제나 probiotics의 효과는 어떠합니까?
[Miwa 선생님 답변] Rebamipide는 여러 임상연구에서 효과가 없었습니다. Probiotics에 대해서는 희망이 있지만 자료가 부족합니다. 연구가 필요합니다.
[2022-4-23] 경주 심포지엄. 김수진 교수님 강의
[2022-6-8] 동아ST web seminar 오정환 교수님 강의
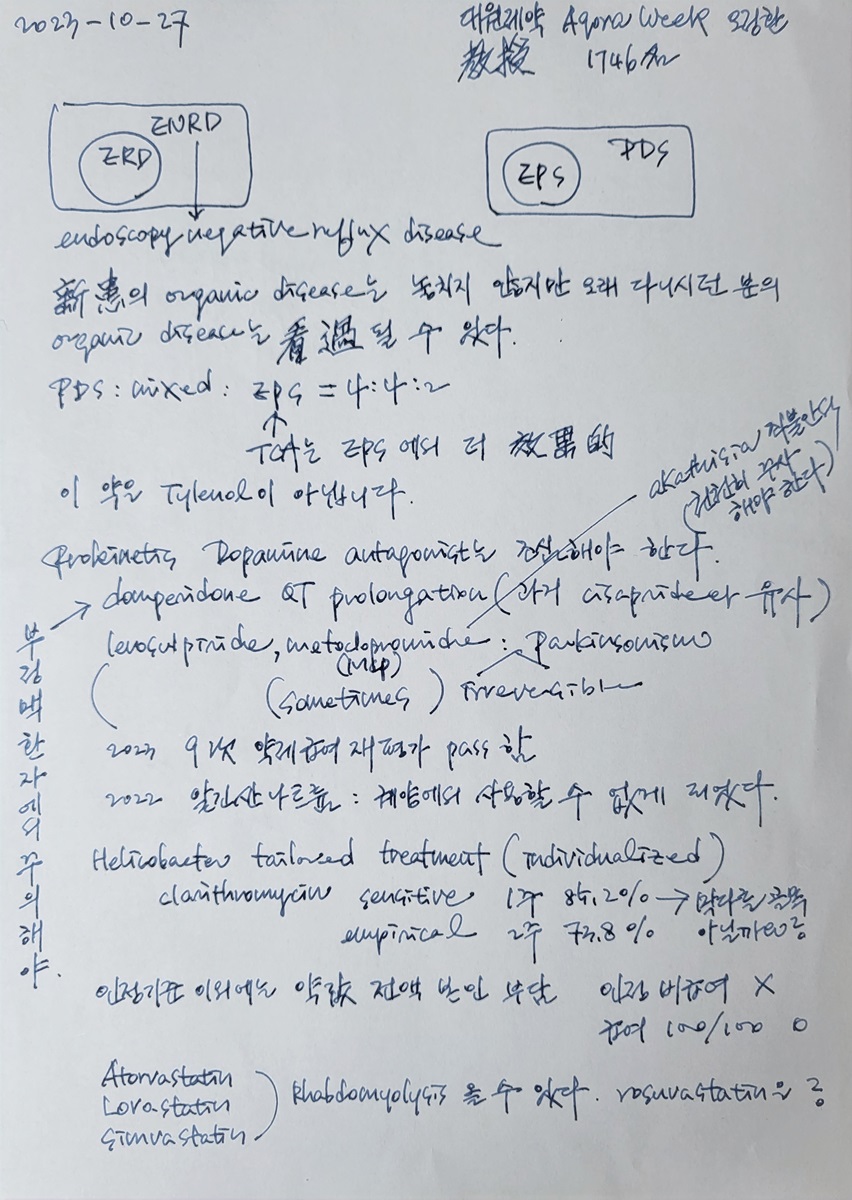
신환의 organic disease는 놓치지 않지만 오래 다니시던 분의 organic disease는 간과될 수 있습니다.
PDS : mixed : EPS = 4:4:2
TCA는 EPS에서 더 효과적이다.
"이 약은 Tylenol이 아닙니다."
"소화의 시작은 amylase부터입니다. 잘 씹어 드십시오."

[2023-4-15] 제천 심포지엄
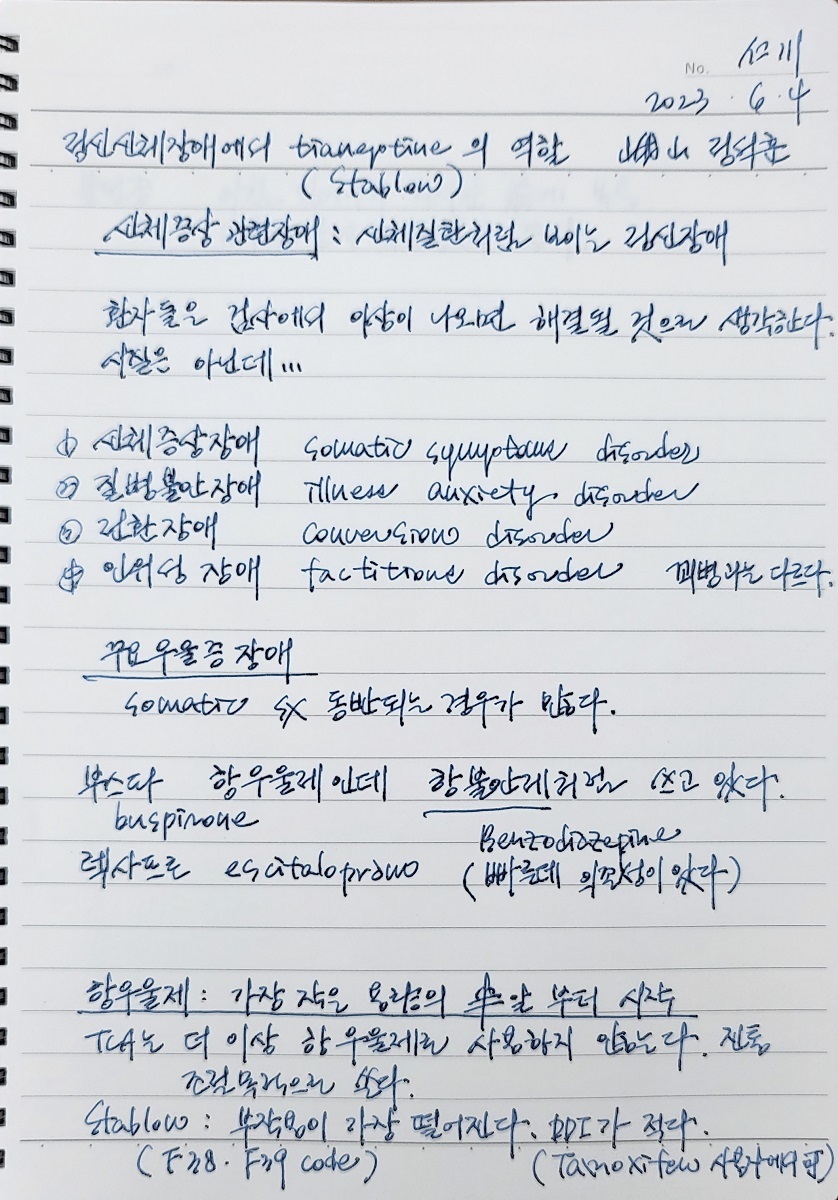
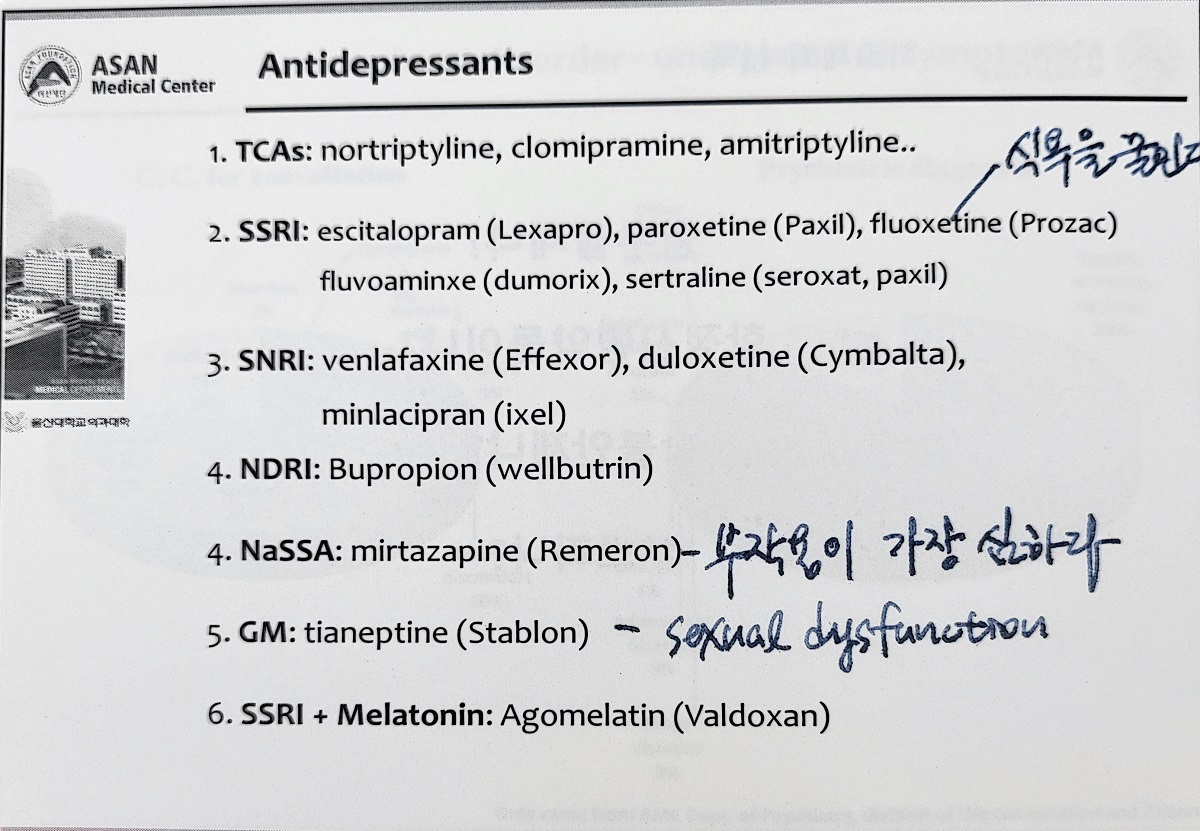
[2023-6-4] 인천 심포지엄. 아산병원 정신건강의학과 정석후 교수님 강의
[2023-7-12] 그녀들의 수다 - 대웅제약 닥터빌 web-seminar
그녀들의 수다 대웅제약 닥터빌 log-in 要
그녀들의 수다 대웅제약 닥터빌 log-in 要
[2023-10-27] 오정환 교수님 강의
[2024-1-14] 문희석 교수님 강의
[2024-5-19] 자규보 심포지엄 다음 날 유익한 강의가 있었습니다.
![]() [FAQ]
[FAQ]
[2018-9-16. 이준행 혼잣말]
FD 혹은 GERD라고 오시는 환자 중 FD나 GERD가 아닌 분들이 많습니다. 우울증이거나 불면증인데 내과에서 적절하게 치료받지 못한 경우도 적지 않습니다. 불면증이 주 원인으로 생각되어 정신건강의학과 불면증 clinic으로 안내하였는데 환자가 크게 만족하고 고맙다고 말씀하셨습니다.

불면증이 진단되지 않아서 불필요하게 PPI를 드시는 분이 많습니다. 환자에게 잘 주무시는지 물어보면 어떨까요?
[2024-6-9] Metoclopride는 아예 사용하지 않는 것이 좋을 것 같습니다. 대한민국에서 너무 위험합니다.
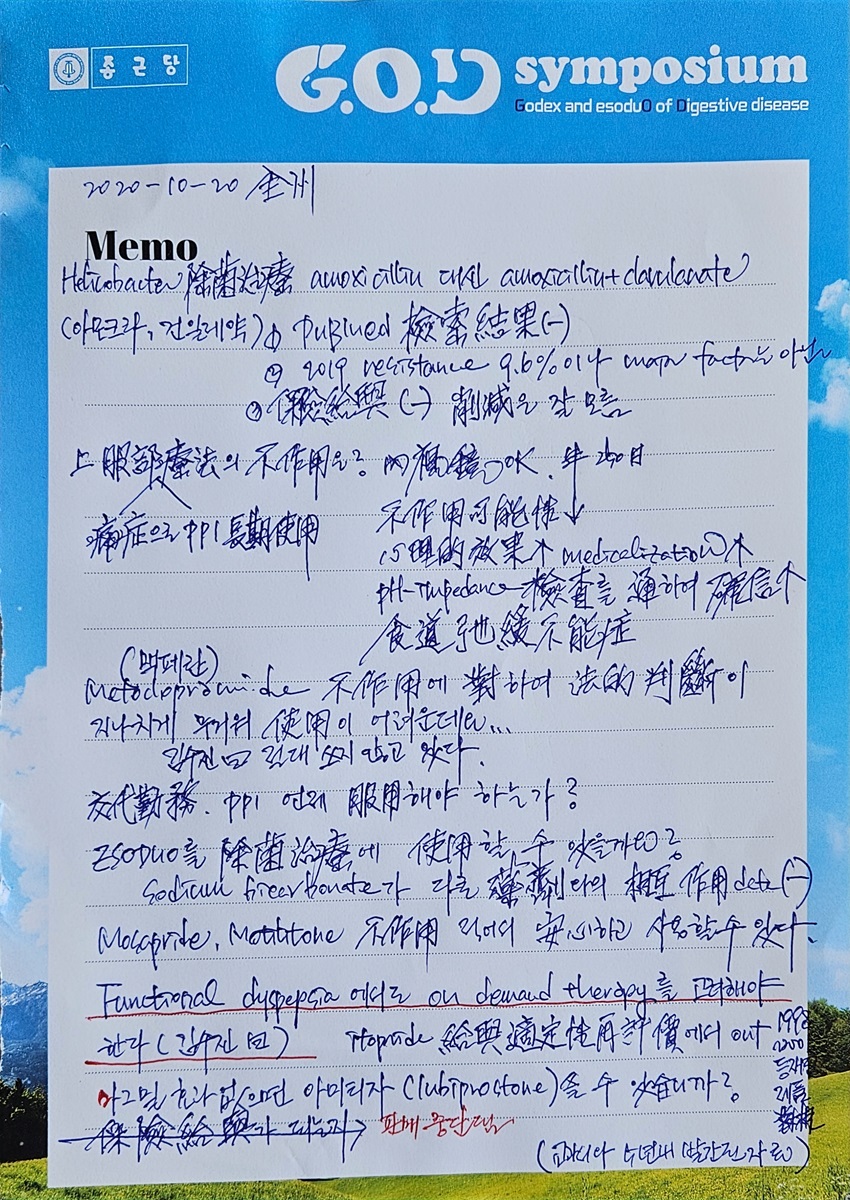
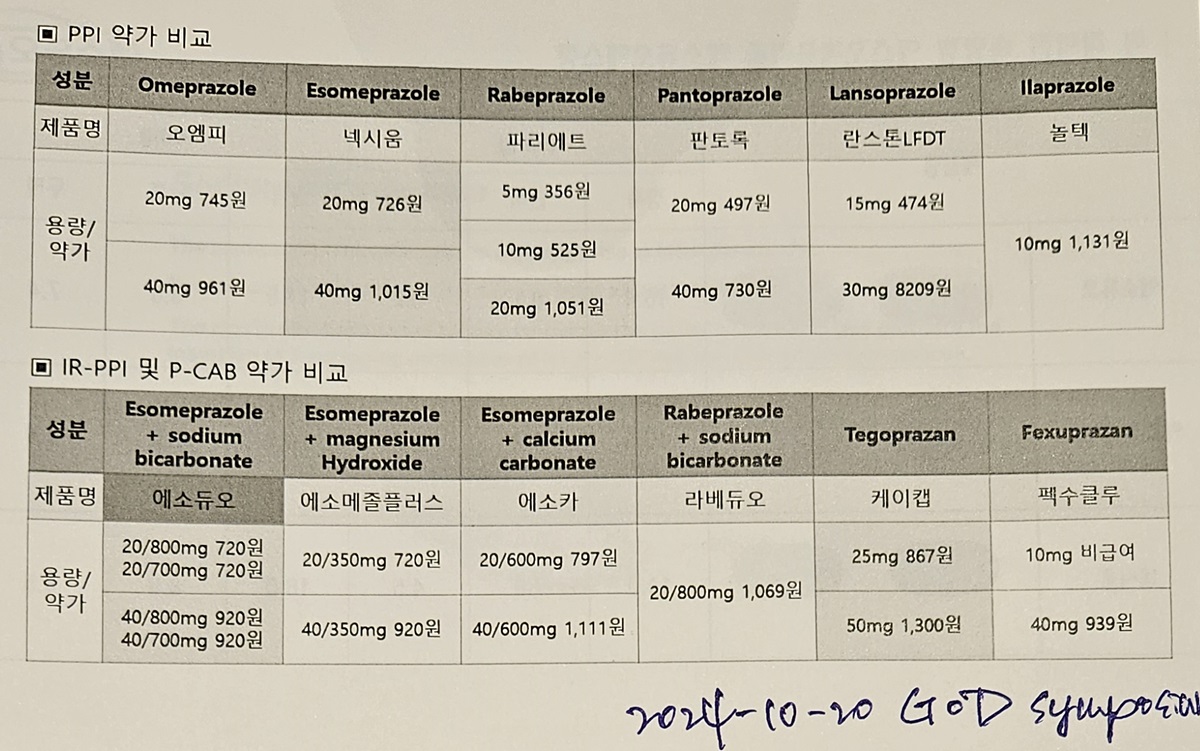
[2024-10-20] 종근당 전주 심포지엄
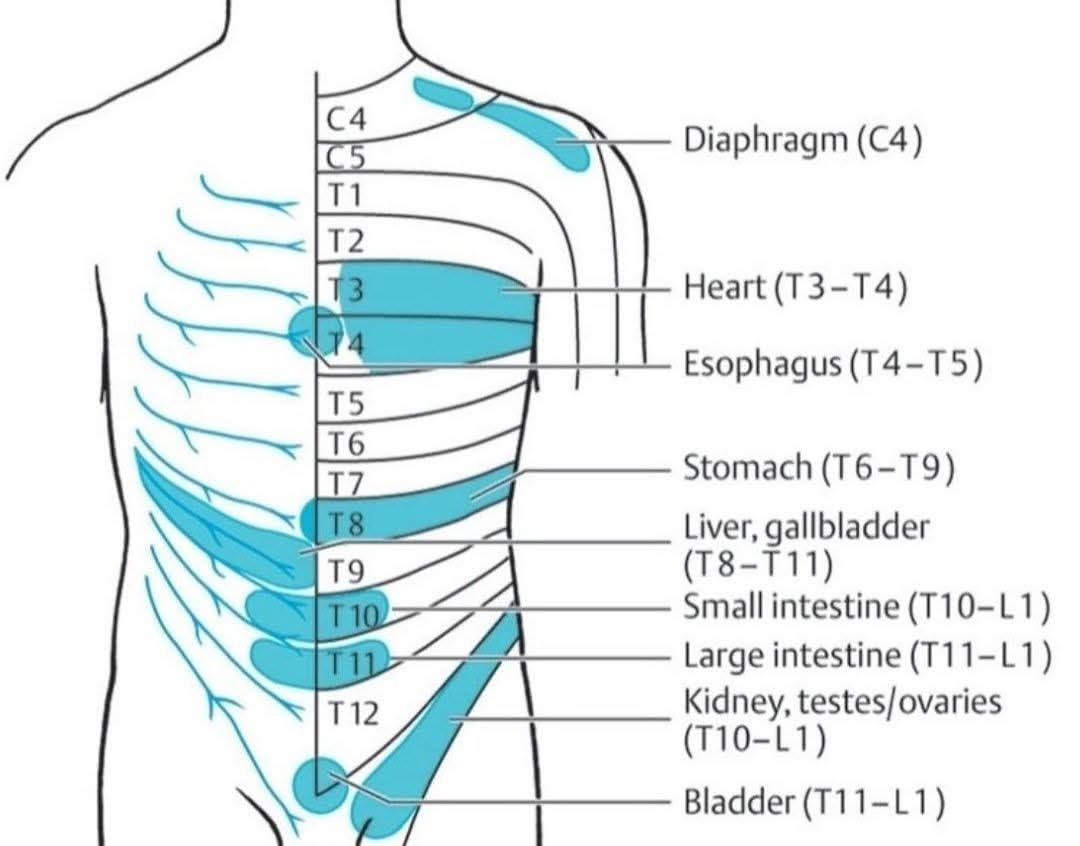
[2025-9-23] 어느 Facebook에서 가지고 옴. 복통과 방사통 radiating pain
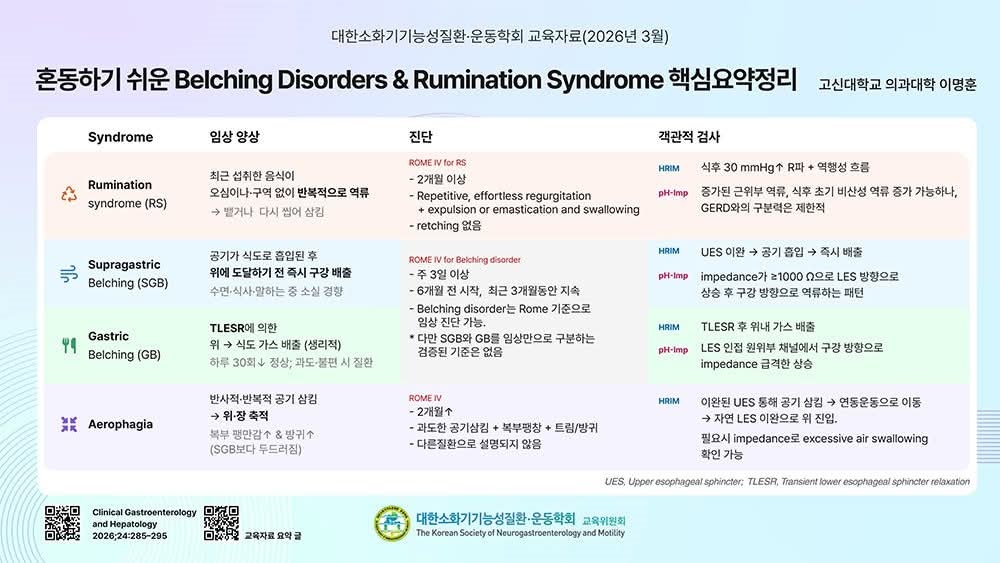
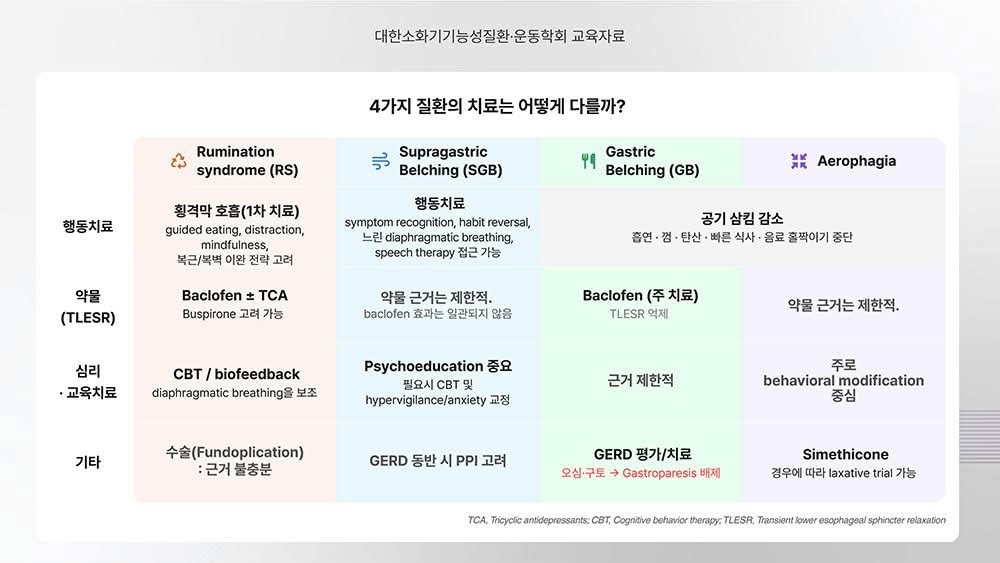
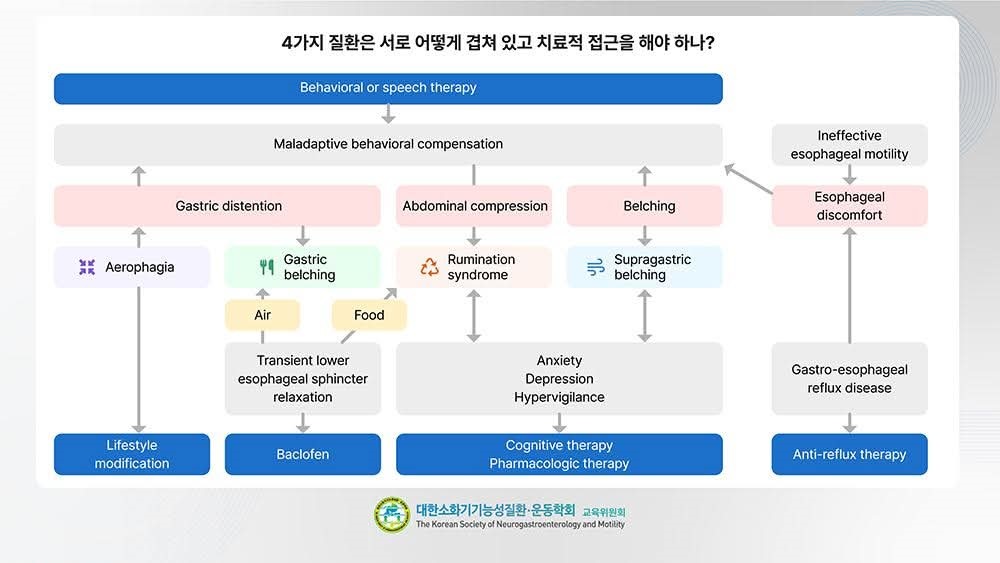
[2026-4-2] 운동학회 교육자료. Rumination syndrome, Supragastric belching, Gastric belching, Aerophagia
[2026-6-19] 명사 특강 - 건국대 김정환 교수님 on functional dyspepsia
![]() [References]
[References]
1) 차재명 교수님 - 비온뒤 인터뷰
YouTube
2) 2022-6-8. 기능성소화불량증 동아 ST 강의. 오정환 교수님 (관리자용)
3) 2023-2-14. 비온뒤 이준행 인터뷰
4) 소화기약물 웹세미나 2024
[2024-10] 이토프라이드 itopride 보험 out
[2025-7] 맥페란 주사가 파킨슨병 악화? 대법원 '파기환송'
![]() © 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.