EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Upper GI involvement of Crohn's disease. 크론병 환자의 상부위장관 내시경 소견] - 終
[Upper GI involvement of Crohn's disease. 크론병 환자의 상부위장관 내시경 소견] - 終
1. Introduction 대한소화기내시경학회 교육자료, 김광하 교수님 책
3. 크론병 환자의 위 소견
5. References
![]() 1. Introduction (크론병의 상부위장관 침범) - 대한소화기내시경학회 교육자료, 김광하 교수님 책
1. Introduction (크론병의 상부위장관 침범) - 대한소화기내시경학회 교육자료, 김광하 교수님 책
대한소화기내시경학회에서 좋은 교육자료를 보내왔습니다.
PDF 0.4 M
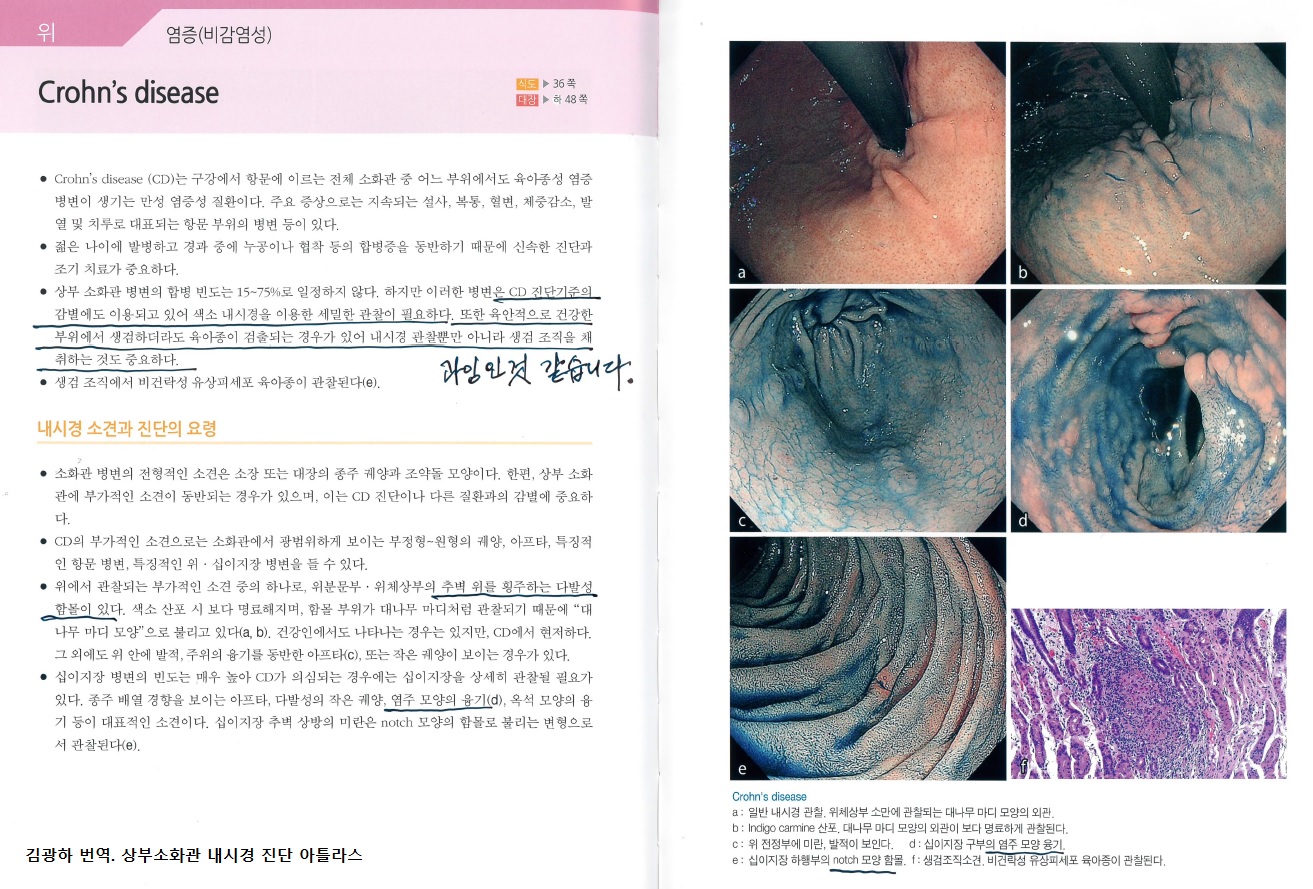
김광하 교수님께서 번역하신 '상부소화관 내시경진단 아틀라스'에도 흥미로운 내용이 있었습니다. 완전히 일본식이네요... 조금은 과잉으로 느껴집니다. 색소내시경이나 조직검사를 꼭 해야 하는 것은 아닙니다.
병리학적으로는 focally enhanced gastritis가 특징적입니다.
![]() 2. 크론병 환자의 식도 소견
2. 크론병 환자의 식도 소견
자료제공: 건국대 이선영 교수님
![]() 3. 크론병 환자의 위 소견
3. 크론병 환자의 위 소견
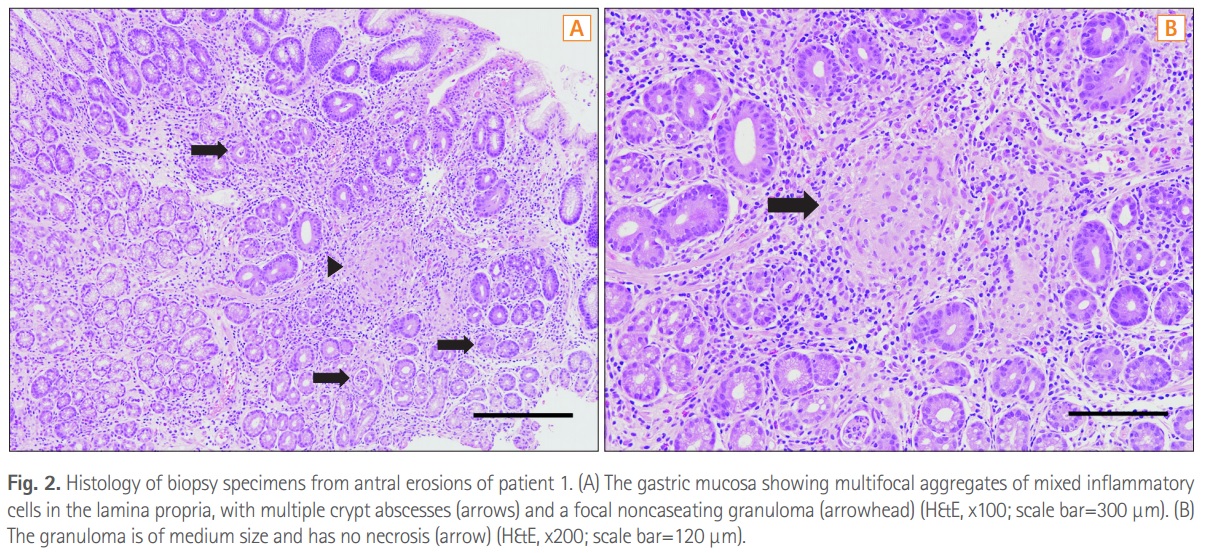
Intestinal Research 2016년 첫호에 실린 Gastric lesions in patients with Crohn’s disease in Korea: a multicenter study를 소개합니다. 크론 환자에서 gastric noncaseating granuloma가 prognostic value를 가질 수 있다는 결론이 신선했습니다.
Methods: Among 492 patients with CD receiving upper gastrointestinal (GI) endoscopic evaluation in 19 Korean hospitals, we evaluated the endoscopic findings and gastric histopathologic features of 47 patients for our study. Histopathologic classification was performed using gastric biopsy tissues, and H. pylori infection was determined using the rapid urease test and histology. Results: There were 36 men (76.6%), and the median age of patients at the time of upper GI endoscopy was 23.8 years (range, 14.2-60.5). For CD phenotype, ileocolonic disease was observed in 38 patients (80.9%), and non-stricturing, nonpenetrating disease in 31 patients (66.0%). Twenty-eight patients (59.6%) complained of upper GI symptoms. Erosive gastritis was the most common gross gastric feature (66.0%). Histopathologically, H. pylori-negative chronic active gastritis (38.3%) was the most frequent finding. H. pylori testing was positive in 11 patients (23.4%), and gastric noncaseating granulomata were detected in 4 patients (8.5%). Gastric noncaseating granuloma showed a statistically significant association with perianal abscess/fistula (P=0.0496).

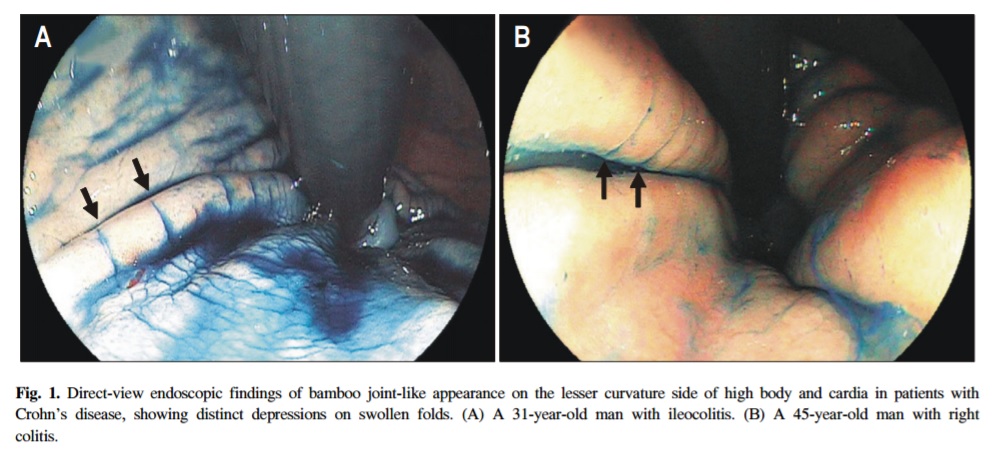
성균관대학교 강북삼성병원 박동일 교수님팀에서 크론병 환자의 위내시경에서 관찰되는 bamboo joint-like appearance에 대한 논문을 발표한 바 있습니다 (강문수. 대한소화기내시경학회지 2006).
Typical gastroduodenal endoscopic findings in a Crohn's disease patient in remission stage (lizuka M. WGJ 2012)라는 제목의 일본 논문에도 좋은 사진이 있었습니다.
Gastroduodenal endoscopic findings of the patient. A: Endoscopic view of bamboo-joint-like appearance on the lesser curvature of the gastric body and cardia; B: Bamboo-joint-like appearance was more clearly observed by spraying with indigo carmine dye; C: Endoscopic view of notches on the Kerckring’s folds of the duodenum; D: Notch sign was more clearly observed by spraying with indigo carmine dye; E: The bamboo-joint-like appearance was localized in the lesser curvature of the upper gastric body and cardia.
2021년 건국대 내시경 퀴즈 중 관련 증례가 있었습니다.
Granulomatous gastritis in Crohn's disease
On-line에서 무료로 PDF를 볼 수 있는 몇 개의 논문을 소개합니다.
![]() 4. 크론병 환자의 십이지장 소견
4. 크론병 환자의 십이지장 소견
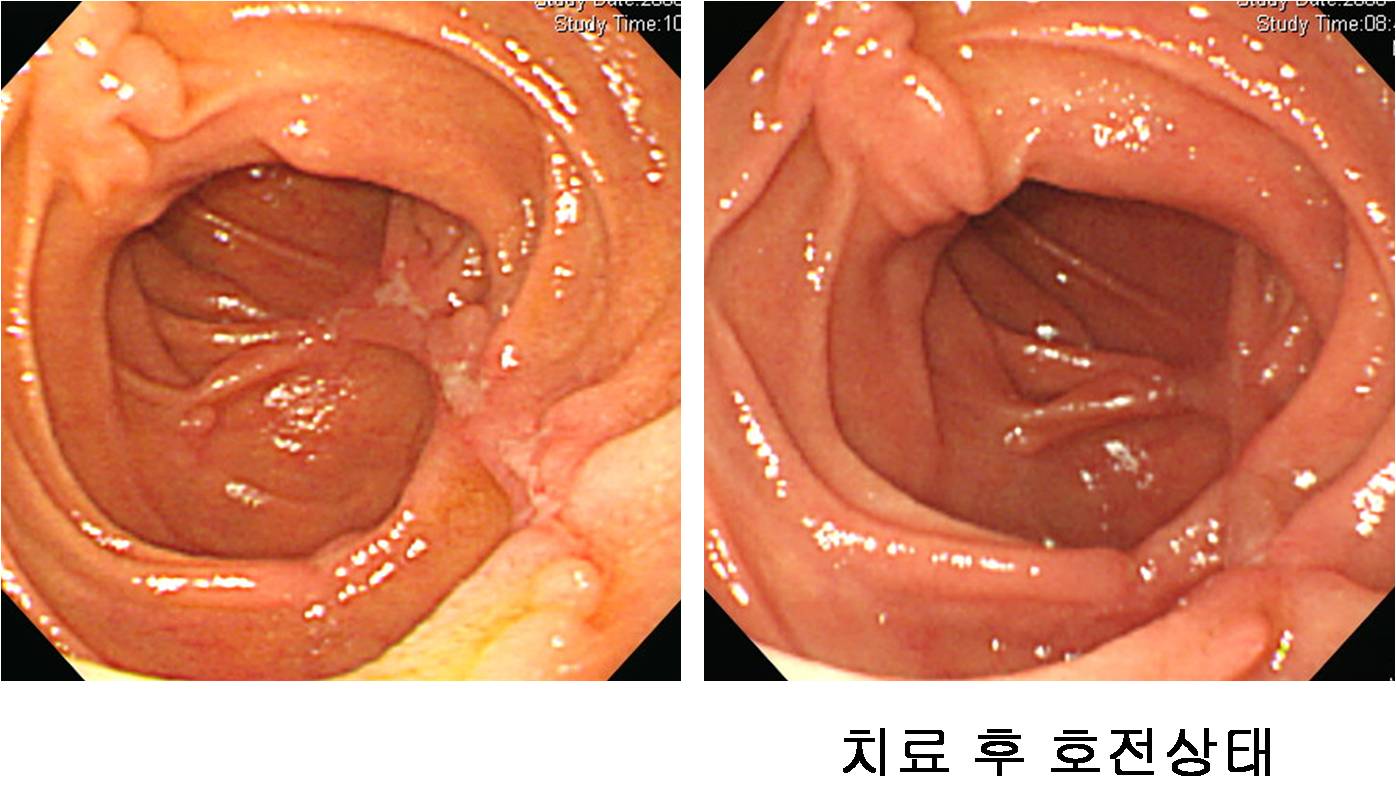
크론병은 보통 하부위장관 질환이지만 간혹 상부위장관 침범을 보이기도 합니다. 소장수술을 통하여 크론병으로 확진된 바 있는 50대 여성으로 duodenum에서도 크론병의 전형적인 longitudinal ulcer가 잘 보였던 경우입니다. 이 정도 특징적이면 크론병의 십이지장 침범으로 진단하는데 무리가 없다고 생각됩니다. 크론병 치료를 하면서 호전된 점도 supporting evidence일 것입니다. 그러나 간혹 애매한 소견만 보인 환자에서는 상부위장관 질환과 크론병과의 관련성을 입증하기 어렵습니다.
![]() [References]
[References]
2) 증례로 알아보는 염증성 장질환에서 치료 내시경은 어떻게. 2023년 대한소화기내시경학회 제67회 세미나. 삼성서울병원 홍성노 교수님.
log-in 要
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.