EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [2015-8-1. ESD 연구회 하계 워크샵 (메이필드 호텔 로터스 룸)]
[2015-8-1. ESD 연구회 하계 워크샵 (메이필드 호텔 로터스 룸)]

![]() 1. 대한내시경학회 ESD 데이타베이스 online registry (가톨릭대 박재명 교수님).
1. 대한내시경학회 ESD 데이타베이스 online registry (가톨릭대 박재명 교수님).
향후 국내에서 다기관연구가 보다 활발하게 진행될 수 있을 것 같습니다. 그 동안 큰 병원 데이타만 발표되고 작은 병원 데이타는 드러나지 않았던 문제가 상당부분 해결될 것 같습니다.
![]() 2. 식도암 ESD 적응증 (가톨릭대 박재명 교수님)
2. 식도암 ESD 적응증 (가톨릭대 박재명 교수님)
삼성서울병원에서 T1 식도암의 림프절 전이 위험성을 분석한 바 있습니다 (J Gastroenterol Hepatol 2008). 결과 부분을 옮기면 아래와 같습니다.
"The frequency of lymph node involvement was 6.25% (4/64) in mucosal cancers and 29.3% (39/133) in submucosal cancers (P < 0.001). In patients with M1 (n = 32) and M2 (n = 14) cancers, no lymph node metastasis was found. In multivariate analysis, size larger than 20 mm, endoscopically non-flat type, and endo-lymphatic invasion were significant independent risk factors for lymph node metastasis. "
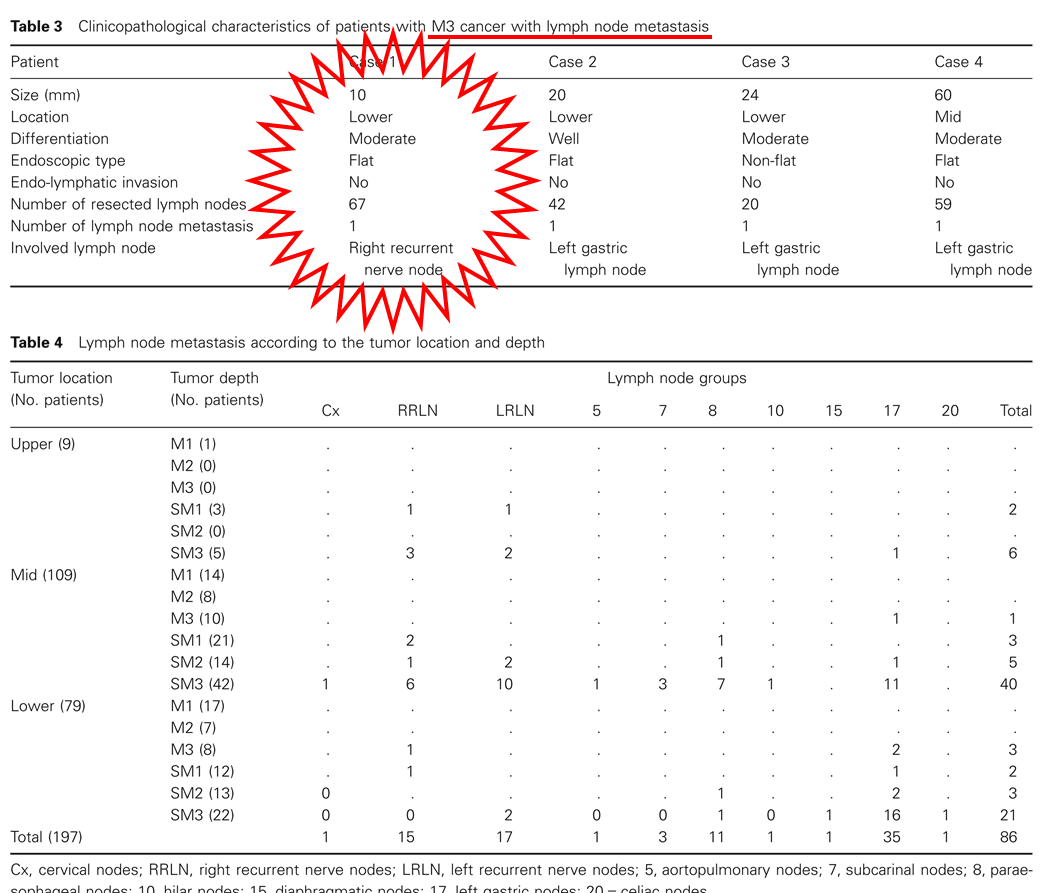
M3 암에서 림프절 전이가 갑자기 많아지고, SM에서는 더욱 많다는 점이 중요합니다. 위암에서도 depth of invasion에 따라 림프절 전이가 많아지지만 식도암에서는 그 차이가 더욱 현저합니다.

M3 식도암 중 림프절 전이를 보인 것은 대부분 장경 20mm 이상이었습니다. 그러나 장경 10 mm 분화형 M3 식도암에서 림프절 전이를 보인 증례도 있었습니다.
일본에서의 보고에 의하면 M2 식도암에서도 간혹 림프절 전이가 있다고 합니다 (Kodama. Surgery 1998).
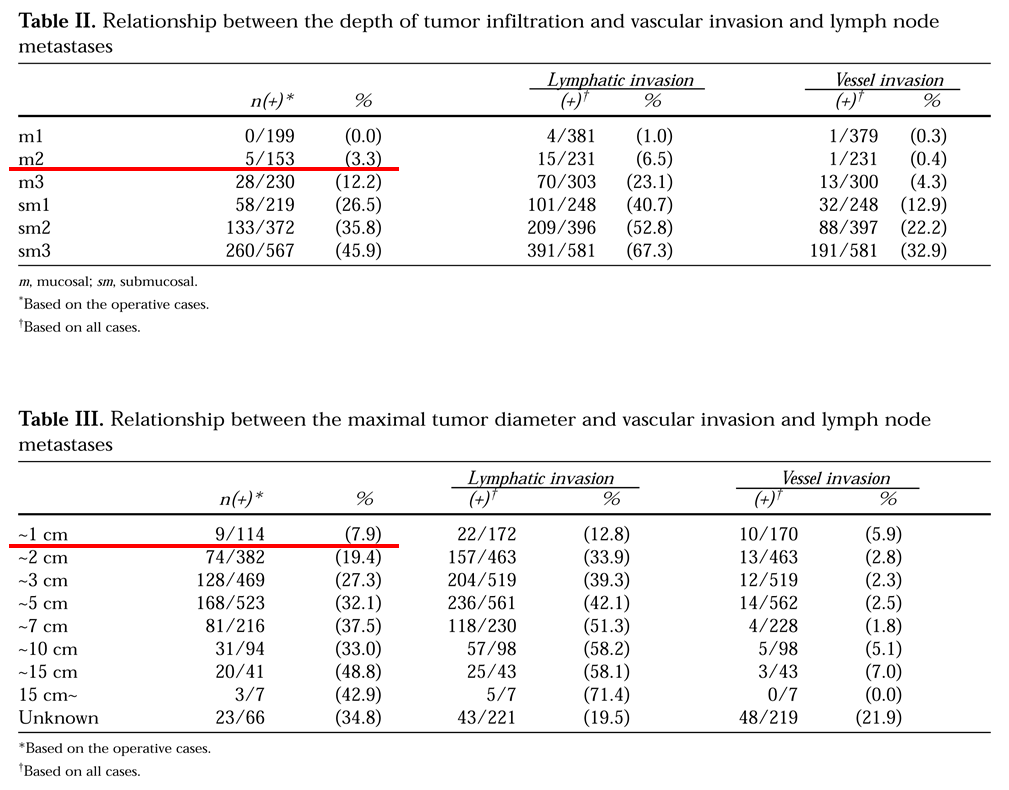
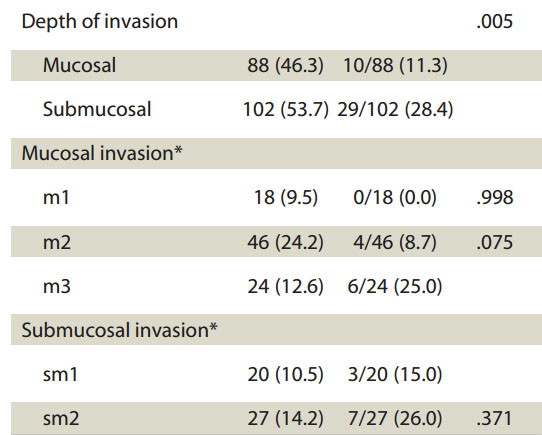
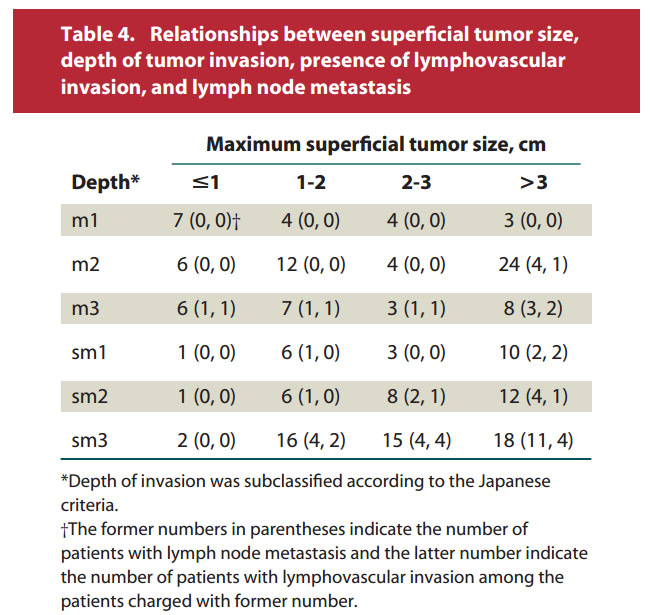
2011년 아산병원에서 발표한 자료입니다. 점막암의 11.3%, 점막하암의 28.4%에서 림프절 전이가 있었습니다. 아산병원에서는 심달도와 크기에 따른 림프절 전이 양상을 제시하여 실제 임상에서 매우 도움이 되는 자료를 보여주고 있습니다. 예를 들어 M2 병소도 3 cm 이상이 되면 24명 중 4명에서 림프절 전이가 있다는 것입니다.
중국 식도암 림프절 전이 자료: Parameters predicting lymph node metastasis in patients with superficial esophageal squamous cell carcinoma
일본 식도암 내시경 치료 후 survival에 대한 자료: Long-term outcome and metastatic risk after endoscopic resection of superficial esophageal squamous cell carcinoma: The 5-year overall survival rates of patients with EP/LPM, MM, and SM cancer were 90.5, 71.1, and 70.8%, respectively (P=0.007).
![]() 3. 위암 ESS 적응증 (한양대 이항락 교수님)
3. 위암 ESS 적응증 (한양대 이항락 교수님)
기존 내시경 적응증은 수술 후 병리를 근간으로 정해진 것이므로 내시경 소견이 충분히 고려되어 있지 않습니다. 아래는 가장 대표적인 동경암센터 자료입니다.

내시경 소견을 고려하면 ESD 적응증을 새롭게 update 할 수 있을 것입니다. 한양대에서 2014년 내시경학회에서 발표한 연구의 결론입니다. 내시경으로 평가한 궤양과 병리학적으로 평가한 궤양이 매우 다르다는 내용입니다.
The discrepancy between endoscopic ulcer and pathologic ulcer was 46.15%(48/104).
내시경 소견으로 SM invasion을 예측할 수 있다는 아래 논문도 참고하면 좋을 것 같습니다.
Abe S. Depth-predicting score for differentiated early gastric cancer. Gastric Cancer 2011
![]() 4. 조기대장암 ESD (성균관대 장동경 교수님)
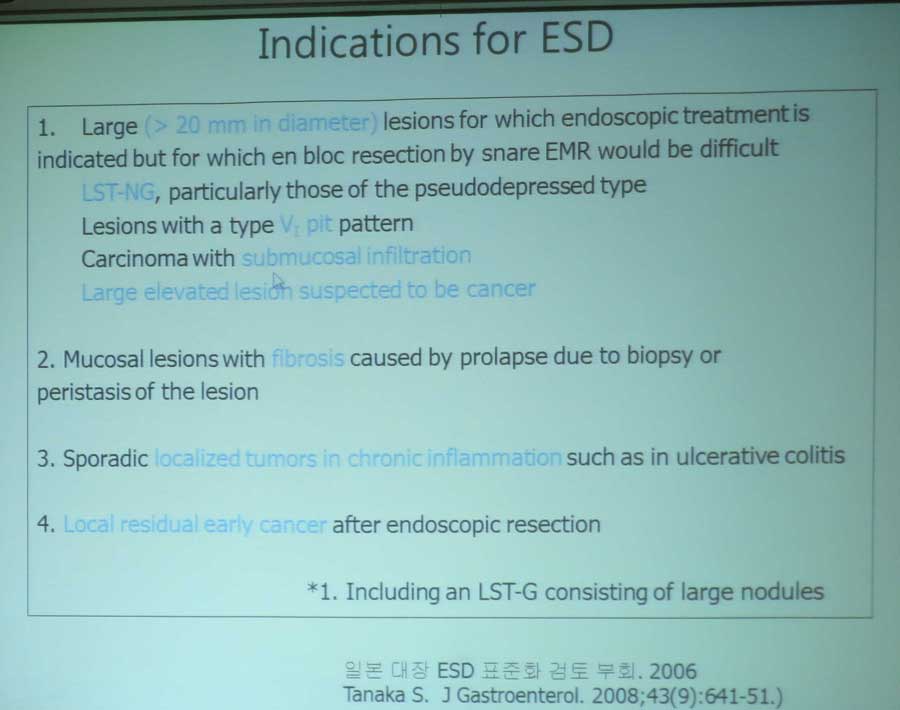
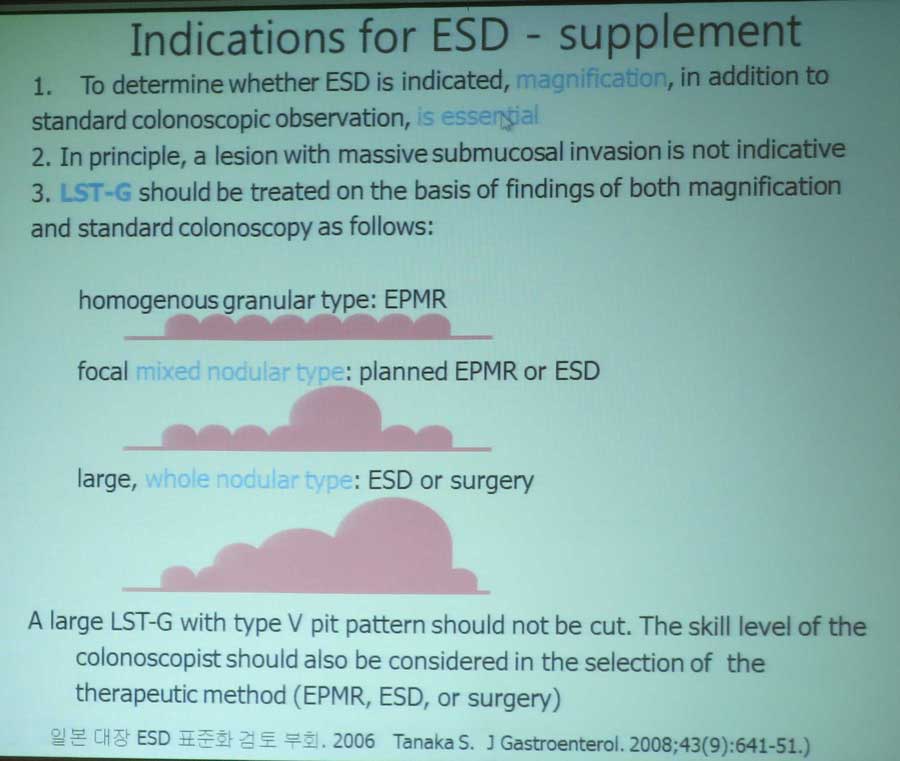
4. 조기대장암 ESD (성균관대 장동경 교수님)
상하부의 관점이 다른 것 같습니다. 위암의 내시경 치료는 대부분 ESD로 이루어지지만, 대장암 내시경 치료는 simple polypectomy, EMR과 ESD가 모두 사용되고 있습니다. 대장에서는 curability의 관점보다는 어떤 병소에서 ESD를 할 것인가의 관점이 중요합니다. 즉 piecemeal resection 필요성과 합병증 위험성이 중요합니다. 재발률은 EMR 10%, ESD 1% 정도로 추정됩니다.
이보인: 우리나라에서 경험이 많은 시술자의 경우 대장 ESD가 생각보다 위험하지 않습니다. EPMR의 국소재발률이 10%보다 작겠지만, 그 경우 ESD를 하는 것은 무척 어렵기때문에 ESD를 조금 적극적으로 해볼 수 있다고 생각합니다.
![]() 5. 인후부, 분문부, 유문부, 십이지장 ESD (경북대 전성우 교수님)
5. 인후부, 분문부, 유문부, 십이지장 ESD (경북대 전성우 교수님)
Hypopharyngeal tumor
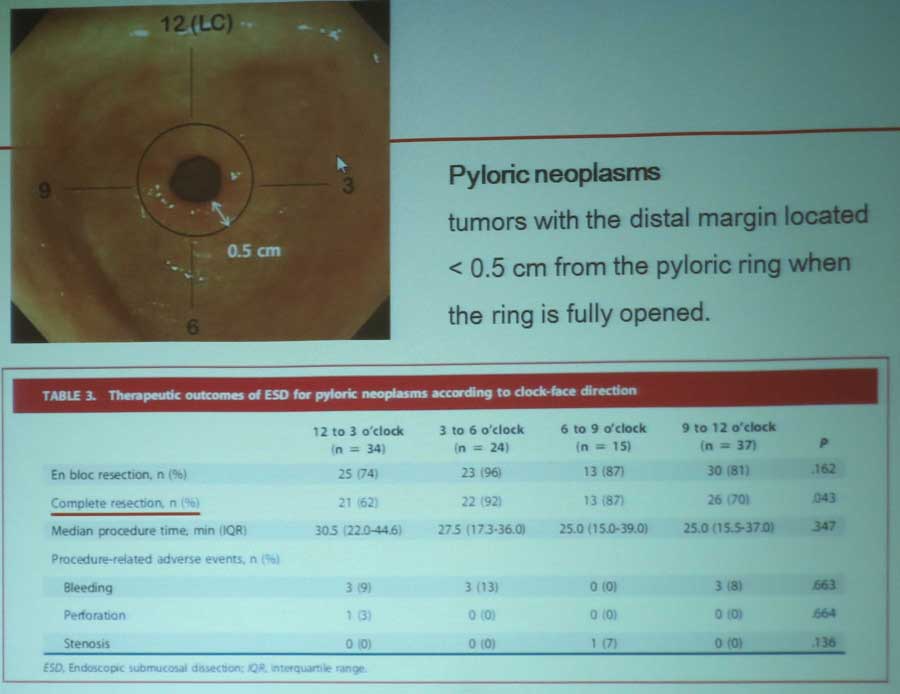
Pyloric ring ESD. 2015년 부산대 논문을 참고하시기 바랍니다. Pyloric ring cancer의 경우 12시 - 3시 방향의 성공률이 낮다는 것이 흥미롭습니다.
Duodenal ESD 후 delayed perforation으로 장기 치료가 필요한 경우가 있습니다. Submucosal injection 후 snare resection으로 해결하거나 laparoscopy endoscopy cooperative surgery를 시도할 수 있었습니다.
1) Technically difficult due to insufficient mucosal elevation and poor mucosal contraction.
2) Abundant blood vessels in the submucosal layer and thin muscle layer pose a serious risk of bleeding and perforation.
3) Minimaize thermal injury to the muscle layer to avoid delayed perforation.
* 여러 교수님들의 comments
- 박종재 교수님 comment: 절제 이후 bleeding control하면서 천공이 발생하는 경우가 있습니다.
- 박재명 교수님 comment: APC도 유용합니다.
- 조광범 교수님 comment: 병소가 작으면 EMR-L 비슷하게 band ligation만 해 주면 저절로 떨어지는 경우도 있습니다.
- 송경호 교수님 comment: 작은 병소는 injection 후 cold snaring으로 치료할 수 있습니다.
- 이준행 comment: 송경호 교수님 의견에 공감합니다. 과거 local에서 십이지장 용종절제술 후 천공으로 의뢰되어 surgical repair가 불가능하여 6개월간 금식하였던 환자를 본 적이 있습니다.
십이지장 용종절제술 후 천공으로 항생제, somatostatin 등을 쓰면서 6개월을 기다렸던 환자.
- 윤영훈 교수님 comment: 수술장에서 내시경 의사가 표시를 해주면 외과의사가 복강경으로 절제하는 방법도 유용합니다.
![]() 6. 상피하종양 (가천의대 김경오 교수님)
6. 상피하종양 (가천의대 김경오 교수님)
2013년 한림대 병원 논문을 참고하시기 바랍니다.

Possible appropriate indication of endoscopic resection
박종재 교수님 comment: Schwannoma는 50%에서 천공이 있습니다.
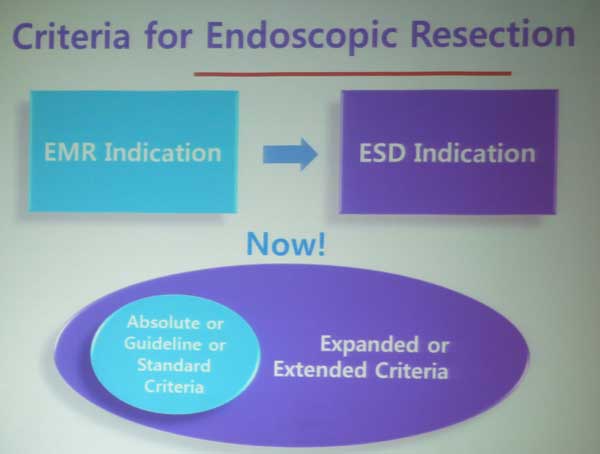
참 명료한 강의였다고 생각합니다. 장재영 교수님께서는 indication과 criteria를 명확히 구분해서 강의해 주셨습니다 (관련된 이준행 교수의 종설 및 editorial).
The second limitation can be named as 'indication/criteria issue'. We choose ESD candidates using some kind of indications. After ESD, we evaluate the resected specimen using some kind of criteria. The contents of indications and criteria may be the same. However, indications are something before ESD, and criteria are something after ESD. The 'indication/criteria issue' is related with the problem of pre- and post-resection diagnostic discrepancies. Recent clinical analysis from Samsung Medical Center has shown that about one third of pre-resection AI-EGC was shifted to post-resection beyond AI-EGC, and 42.8% of the changes were beyond EI for ESD. Another report from National Cancer Center demonstrated that 13.7% were out-of-indication at the pathological evaluation of resected specimen in pre-resection AI group, and 35.3% were post-resection out-of-indication in the clinically EI group. Until now, most data on ESD for EI-EGC are based on post-resection diagnostic groups. This means a lot of cases in reports on ESD for EI-EGC were originally considered as AI-EGCs before ESD. If we do not consider this bias carefully, patients can be exposed to unnecessary risks. (Gut Liver 2015)
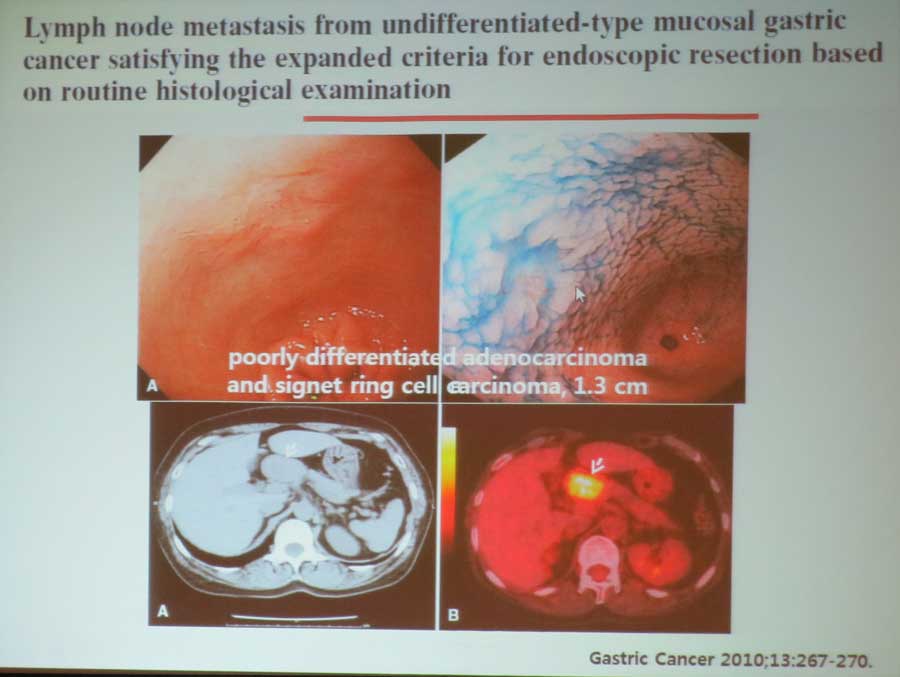
2010년 부산대 병리 논문에 의하면 Expanded indication 중 림프절 전이가 상당히 많았습니다. Lymph node metastasis from intestinal-type early gastric cancer: experience in a single institution and reassessment of the extended criteria for endoscopic submucosal dissection.
Gotoda 2010 연구에 의하면 SM2이고 1cm 미만이면 12.8%, 1-2cm 에서는 14.4%에서 림프절 전이가 있었습니다.
* 최석채 선생님 comment: 두 가지를 꼭 지키고 있는데 아직까지는 재발 예는 없었습니다. (1) 65세 이상의 undifferentiated type 조기위암은 반드시 수술을 보낸다. (2) SM2는 반드시 수술한다. 기존의 가이드라인을 엄격하게 지키면 좋은 임상 결과를 보일 수 있다고 생각합니다.
* 이준행 comment: ESD에 대한 dark side도 증례보고를 해야 할 것 같습니다.
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.
1) Tumor size: <1-3 cm ?
2) Growth pattern: intraluminal growing (submucosal growing)
3) Movability of tumor: narrow muscular connection = more movable
![]() 7. 미분화암 (경희의대 장재영)
7. 미분화암 (경희의대 장재영)
 Gotoda et al. 2000
Gotoda et al. 2000