EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [2015년 대한상부위장관헬리코박터학회 추계학술대회]
[2015년 대한상부위장관헬리코박터학회 추계학술대회]

2015년 12월 12일 여의도 콘래드 호텔에서 추계학술대회가 열렸습니다. 이번 학술대회의 모토는 'Find the way to the reliable Helicobacter eradication therapy'였습니다. 여의도 광장의 가을이 저물어가고 있었습니다. 아직 겨울 느낌은 아니었습니다. 콘래드 호텔 앞 Parc1 공사장은 3년째 그대로였습니다. 자본주의의 추한 구석입니다.

연세대 이상길 교수님의 멋진 발표였습니다. 그러나 저는 내용을 이해할 수 없었습니다. 그냥 non-coding RNA가 숨어서 뭔가 복잡한 일을 꾸미고 있다는 느낌 정도... 2007년 Seattle 연수 시절 공부한 후 이 분야를 follow up 하지 않은 결과입니다. 이젠 공부 좀 해야 할 듯.
여러 학회에서 커피를 마셔보았지만 오늘 커피가 Best 였습니다. Acidic 풍미가 살짝 담겨있어 좋았습니다. 커피 수백잔을 준비하면서 이 정도 맛을 내기는 쉽지 않습니다.
EndoTODAY 애독자들에게 설문한 결과를 학회지에 발표한 바 있는데 금일 우수논문상을 받았습니다.

오후 5시 30분에 촬영하였습니다. 마지막까지 자리를 지켜주신 회원 여러분들을 존경합니다.


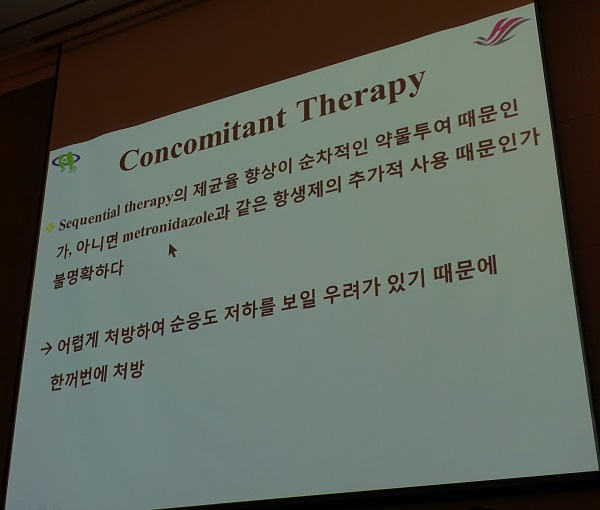
![]() 1. 제균치료 구연 세션 - sequential therapy와 concomitant therapy에 대한 발표가 많았습니다.
1. 제균치료 구연 세션 - sequential therapy와 concomitant therapy에 대한 발표가 많았습니다.
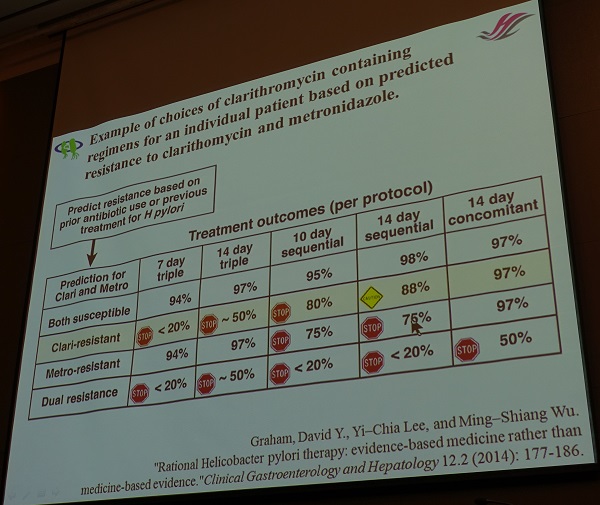
김승영 (OS-1). Clarithromycin 내성이 있는 경우 동시 치료가 순차 치료에 비하여 더 높은 제균율을 보였다.
중앙대학교 김재규 교수님 comment. Clarithromycin 내성과 관련된 point mutation의 종류가 다양하므로 몇 가지 point mutation만 측정하는 PCR kit가 clarithromycin 내성 전체를 반영하지 못합니다. Clarithromycin 내성에 대한 보다 적극적인 검사가 필요합니다.
정성민 (OS-3).
울산대학교 정훈용 교수님 comment. Compliance가 중요할 것 같습니다. Sequential therapy의 경우 첫 5일간은 부작용이 거의 없다가 두번째 5일간 classic triple therapy의 부작용이 나타납니다. Concomitant therapy는 처음부터 약제가 많기 때문에 초기에 부작용이 발생할 수 있습니다.
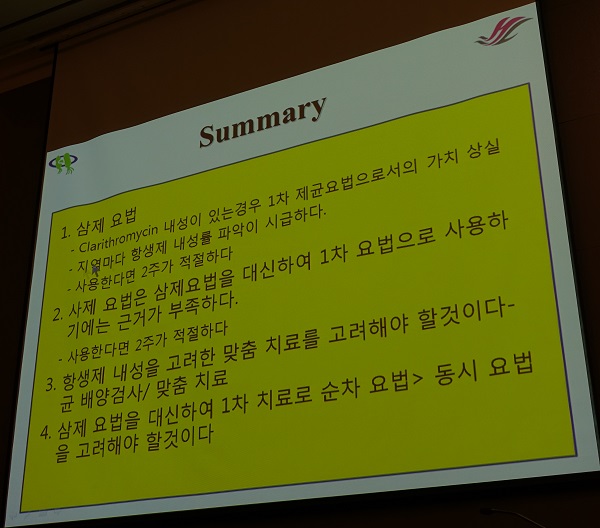
![]() 2. Best strategy of Hp eradication regimen (한림대학교 백광호 교수님 강의)
2. Best strategy of Hp eradication regimen (한림대학교 백광호 교수님 강의)
| Sequential therapy | 1-5일: amoxicillin 1g + PPI (bid) |
| 6-10일: clarithromycin 500 mg + metronidazole 500 mg + PPI (bid) | |
| Concomitant therapy | amoxicillin 1 g + clarithromycin 500 mg + metronidazole 500 mg (bid) 7일 |
| 백광호 교수님의 제안 | |
| PCR이나 배양검사가 불가능한 경우 | 삼제요법 14일 |
| PCR positive인 경우 | 1) Clarithromycin을 metronidazole로 변경한 삼제요법 2) Quadruple therapy 3) Sequential therapy, Concomitant therapy |
| Culture 검사가 가능한 경우 | Tailored therapy |
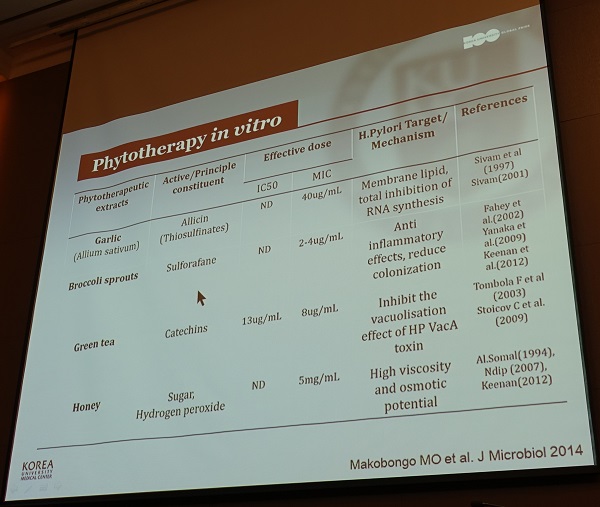
![]() 3. 헬리코박터 제균치료를 위항 새로운 무기 - 새로운 약물과 신무기 (고려대학교 정성우 교수님)
3. 헬리코박터 제균치료를 위항 새로운 무기 - 새로운 약물과 신무기 (고려대학교 정성우 교수님)
1) 항생제 - levofloxacin, moxifloxacin, sitafloxacin, rifabutin, fosfomycin, moenomycin A
2) 생균제 (probiotics)
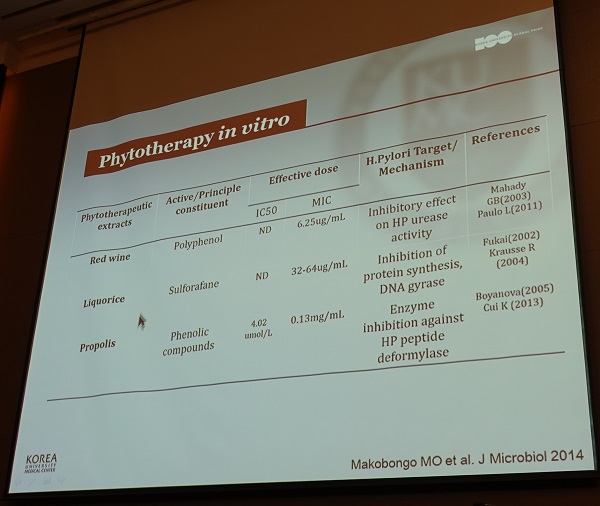
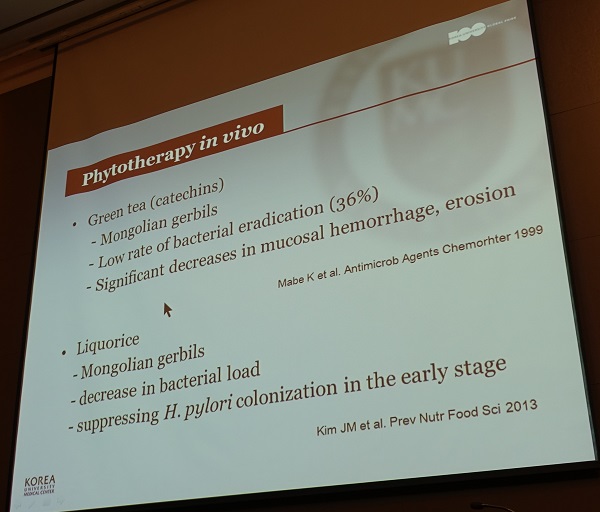
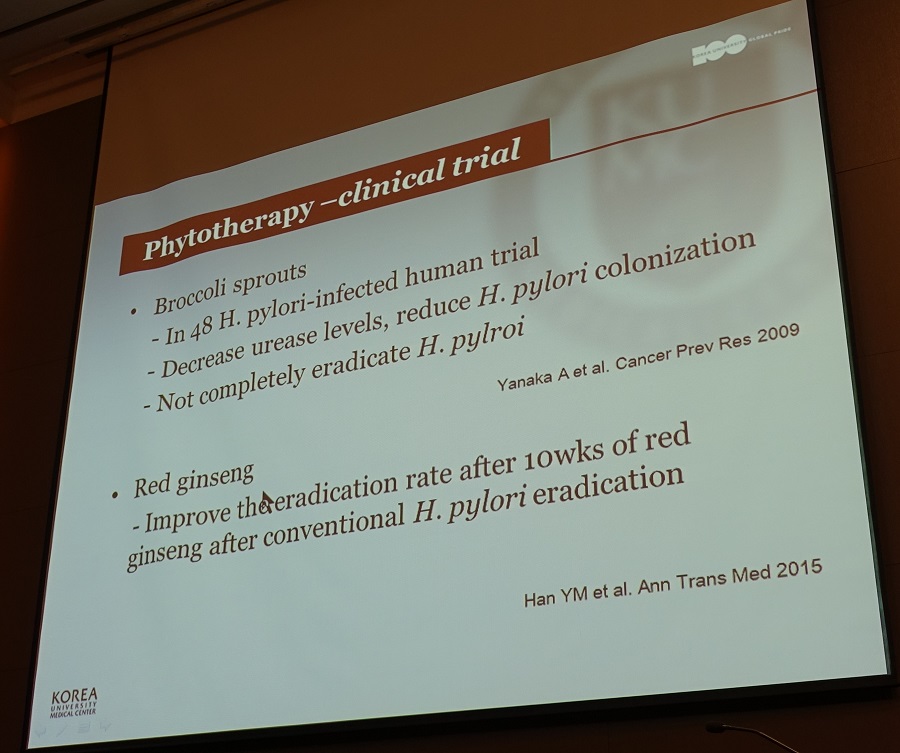
3) 식물요법 (phytotherapy)
4) 항균펩타이드
5) 저분자 억제제 (small molecule inhibitor)
6) 지방산 (fatty acid) - 지방산은 세포막을 구성하는 중요한 요소로 지방으로부터 분해되어 세포 내 여러 가지 생물학적 기능을 갖는 물질로 광범위한 균주에 대한 직접적인 살균작용과 성장을 억제하는 작용이 있다. 그러나 polyunsaturated fatty acid 섭취를 통한 H. pylori 제균에 대한 임상 연구들의 결과는 실망적이었다. 지방산은 경구로 투여시 esterification이나 oxidation되어 활성을 잃을 수 있고 지방이나 단백질 등과 결합하여 점막 내로의 전달이 어려울 수 있는 점이 임상연구에서 좋은 결과를 얻지 못하는 이유로 생각된다.
![]() 4. Selected oral presentations
4. Selected oral presentations
표정의 (PL-2). A risk model based on LN metastasis in P/D intramucosal cancer
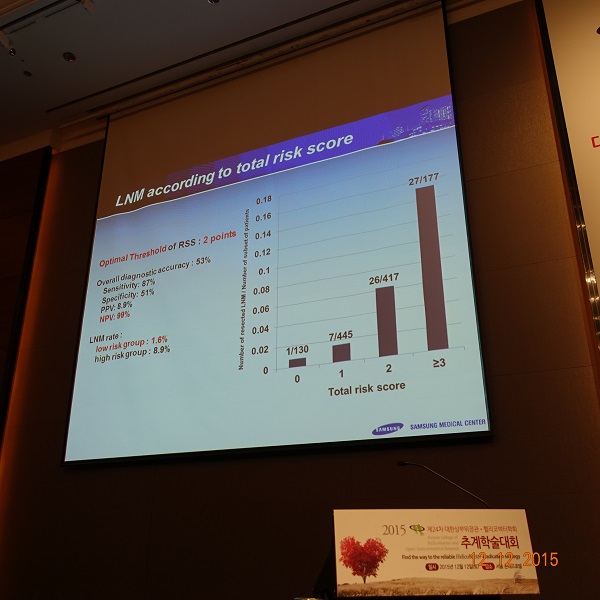
연세대 이용찬 교수님 comment: external validation이 필요할 것 같습니다.
부산대 김광하 교수님 comment: P/D 중 type I (solid)와 typd II (non-solid)를 비교해보면 좋을 것 같습니다.
박성민 (PL-4). Comparison of 4 scoring systems
연세대학교 박효진 교수님 comment: 비슷한 연구를 시행한 바 있습니다. 당시에는 '치료내시경 시행의의 만족도'가 중요했습니다. 내시경 의사가 충분하고 완벽하게 치료했다고 생각하는 경우 outcome이 좋았습니다.
가톨릭대학교 최명규 교수님 comment: 재출혈이나 사망률이 매우 낮았습니다. 국제적으로 유래가 없는데요 혹시 cohort에 문제가 있는 것은 아닙니까?
부산대학교 하동우 (PL-5). Patient-positioning device (EZ-FIX) for ESD

이준행 comment: Procedure time은 EX-FIX 군과 대조군에서 각각 28분, 20분이었고, midazolam은 각각 5.6 mg, 5.7 mg 투여되었습니다. 비교적 짧은 procedure time에 비하여 midazolam이 많았기 때문에 fixing device가 필요하지 않았을까 생각됩니다. Midazolam을 조금 적게 사용할 것을 제안합니다.
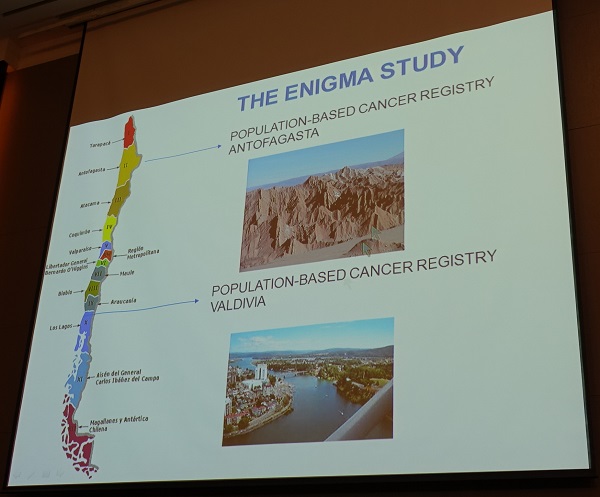
![]() 5. 특강: 라틴아메리카의 헬리코박터와 위암 임상과 연구 현황 (Catterina Ferreccio. Pontificia Universidad Catolica de Chile)
5. 특강: 라틴아메리카의 헬리코박터와 위암 임상과 연구 현황 (Catterina Ferreccio. Pontificia Universidad Catolica de Chile)
라틴아메리카인의 기원에 대한 슬라이드로 시작하여 African Enigma, 아시아와 칠레의 유사점 및 차이점에 대한 흥미로운 강의였습니다.
H. pylori prevalence is similarly high in some areas in Latin Ameria with large GC differentials, similar to the so-colled "African Enigma". The best studied of these enigmas is in Colombia, where coastal populations with African ancestry have very low GC in contrast with moutain counties of Amerindian (American Indian) ancestry. The Colombian case has been explained by co-evolution of H. pylori and its host; that is individuals of African ancestry infected with Africn HP will not present damage in the gastric niche, whereas people of Ameridian ancestry infected with African Hp are at increased risk of GC (Gastric cancer incidence and mortality is associated with altitude in the mountainous regions of Pacific Latin America. Cancer Causes Control 2013;24:249).
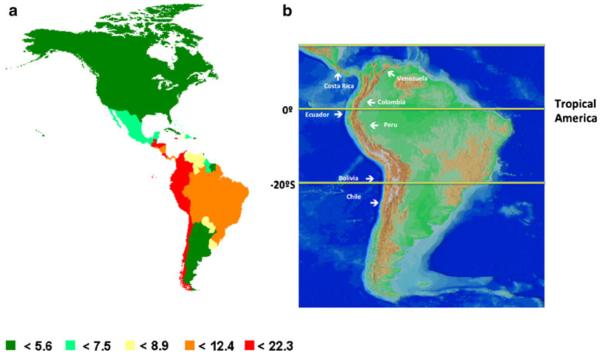 (A) Estimated age-standardized gastric cancer mortality rate per 100,000 in the Americas, (B) map showing that the countries with the higher GC mortality rates follow the Andes mountains and the Sierra Madre in Central America (Cancer Causes Control 2013).
(A) Estimated age-standardized gastric cancer mortality rate per 100,000 in the Americas, (B) map showing that the countries with the higher GC mortality rates follow the Andes mountains and the Sierra Madre in Central America (Cancer Causes Control 2013).
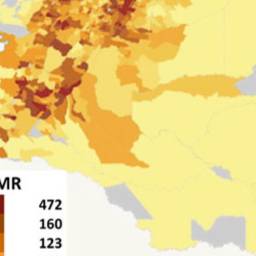 Maps of Colombia showing in a the distribution of the Andes Cordillera and in b the distribution of gastric cancer mortality rates in the different districts of the country (Cancer Causes Control 2013).
Maps of Colombia showing in a the distribution of the Andes Cordillera and in b the distribution of gastric cancer mortality rates in the different districts of the country (Cancer Causes Control 2013).
![]() 6. 위암학회와 합동 심포지엄
6. 위암학회와 합동 심포지엄
1) Longterm outcomes of ESD for EGC (성균관의대 이준행)

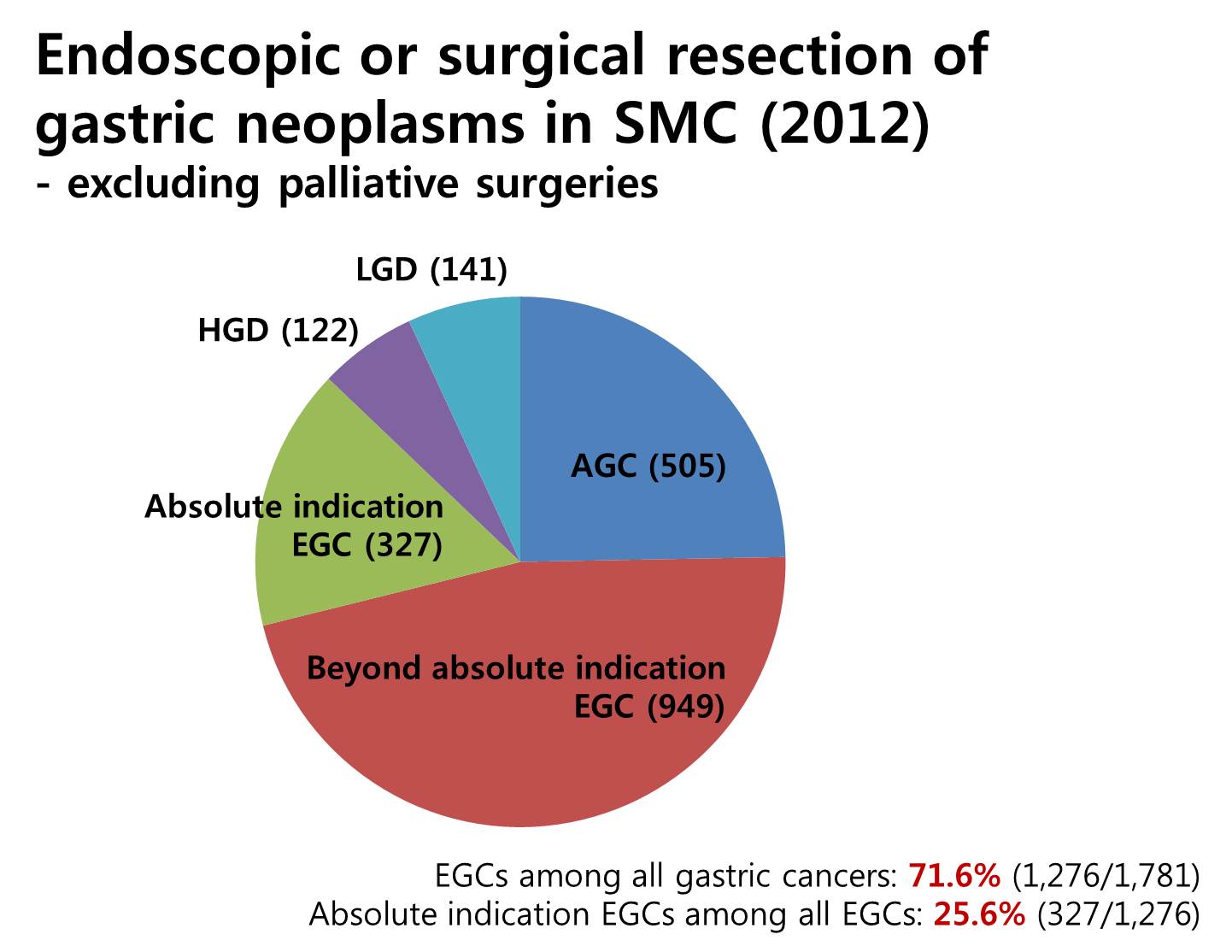
As you know, the proportion of early gastric cancer is increasing. This is how we are doing in my institution. Excluding palliative surgeries, we have endoscopically or surgically treated more than seventeen hundred gastric cancers in 2012. Among them, 72% were early gastric cancers. In early gastric cancers, cases within absolute indications were 25%. So the role of ESD for the treatment of gastric cancer is getting bigger and bigger.
What do you think is the best way of presenting long-term outcome data? There are two types of outcome analysis - one is intention to treat analysis, and the other is per protocol analysis. Of course, data from intention to treat analysis is more realistic. In the survival analysis, the rate of follow-up loss is very important. It should be minimalized, usually less than 15 percent in prospective clinical studies.
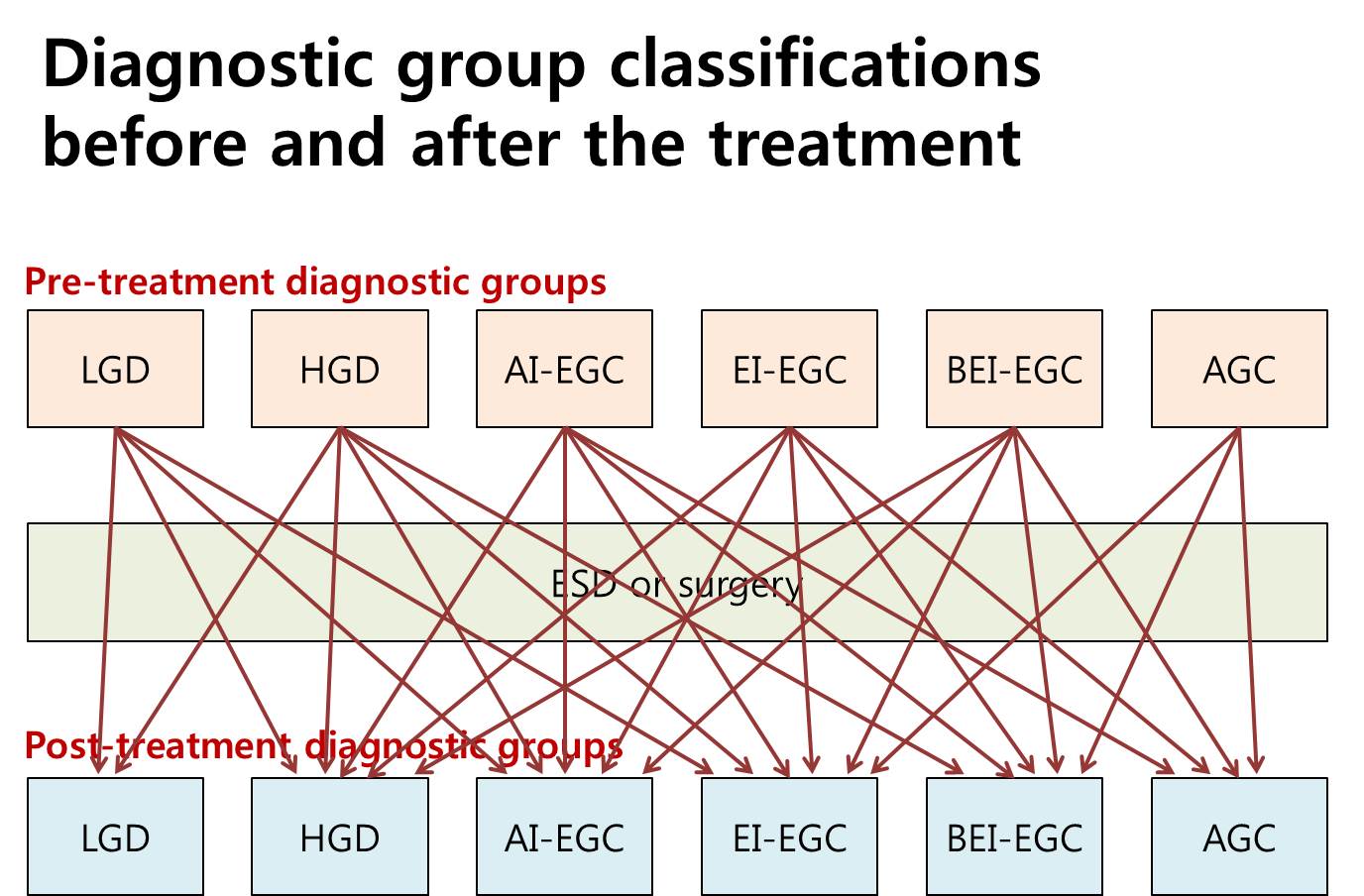
Gastric neoplastic lesions can be divided into 6 groups, such as LGD, HGD, AI-EGC, EI-EGC, BEI-EGA and AGC. Diagnostic group classifications before the treatment can be changed after the treatment. The relationship is very complex. So the outcome analysis can be based on either pretreatment diagnostic groups or posttreatment diagnostic groups.
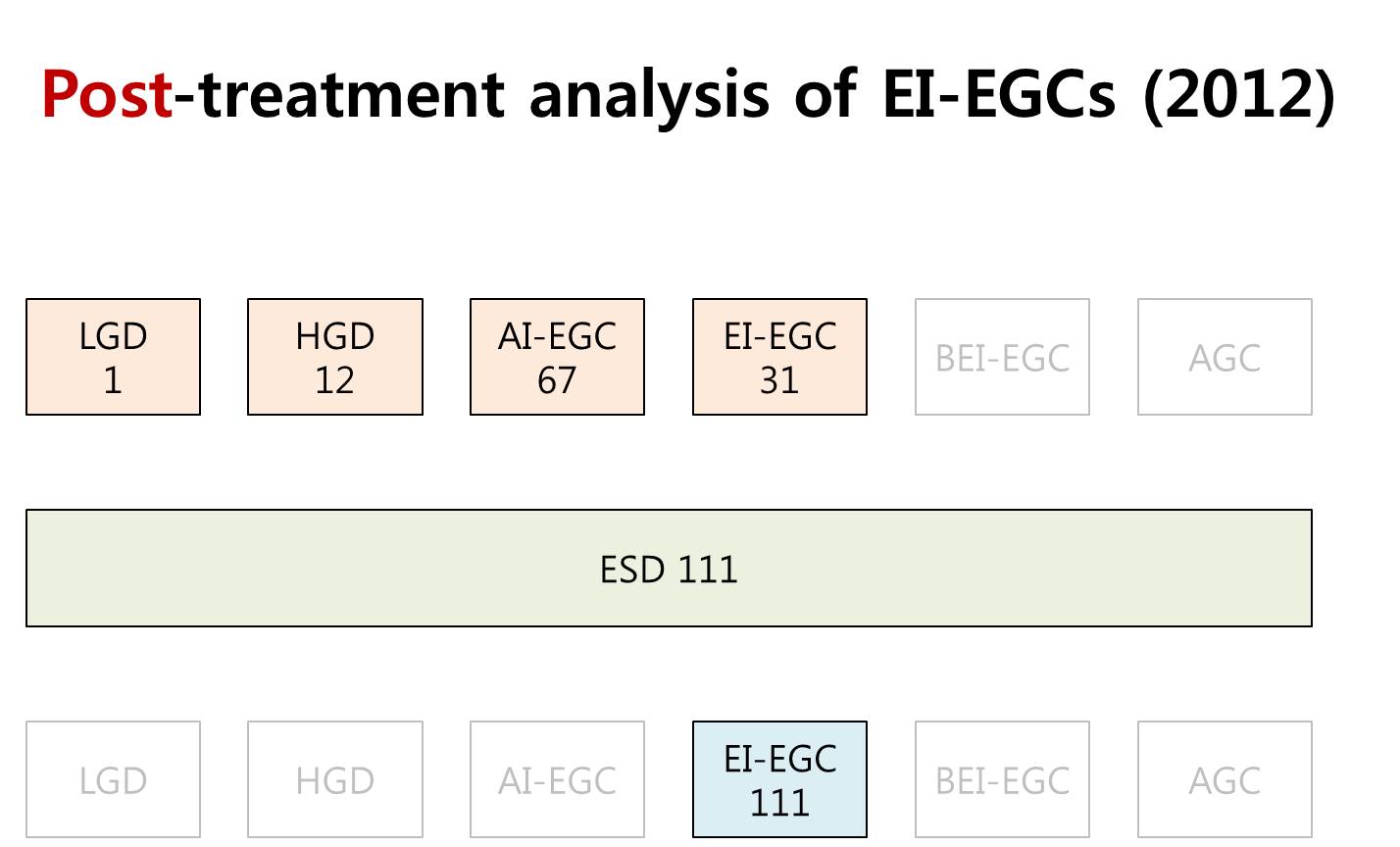
The outcome analysis is usually based on the post-treatment diagnostic groups. In the year 2012, we performed 111 ESDs for post-treatment EI-EGCs. In the beginning, however, the diagnosis was one LGD, 12 HGDs, 67 AI-EGCs and 31 EI-EGCs. So, if you analysis 111 post-treatment EI-EGCs, most of them were actually AI-EGCs before the treatment.
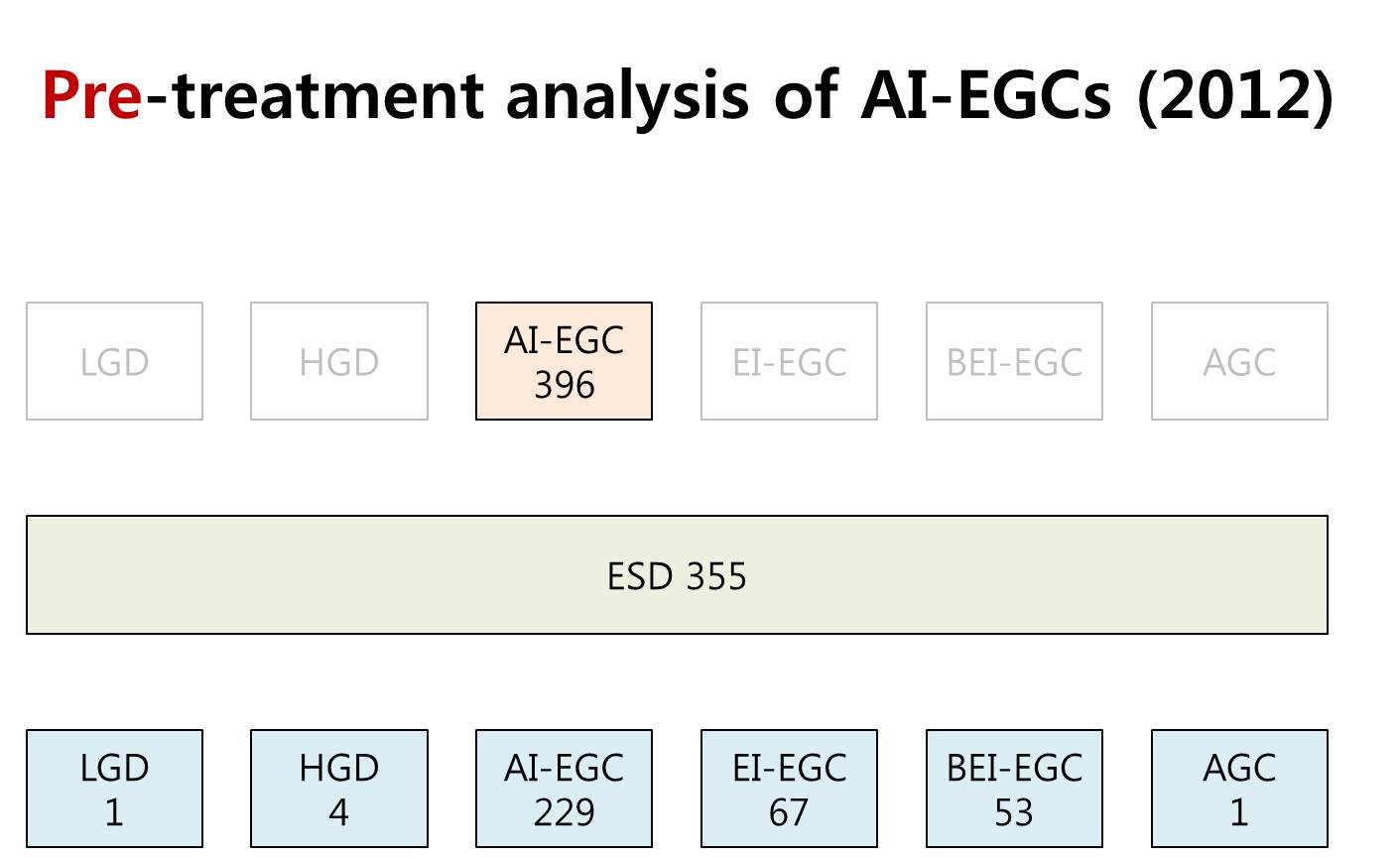
This analysis is based on the pre-treatment diagnostic groups. Among 396 pretreatment AI-EGCs, ESD was done for 355 cases. The final diagnoses were variable. As you can see, the post-treatment diagnosis can be actually everything.
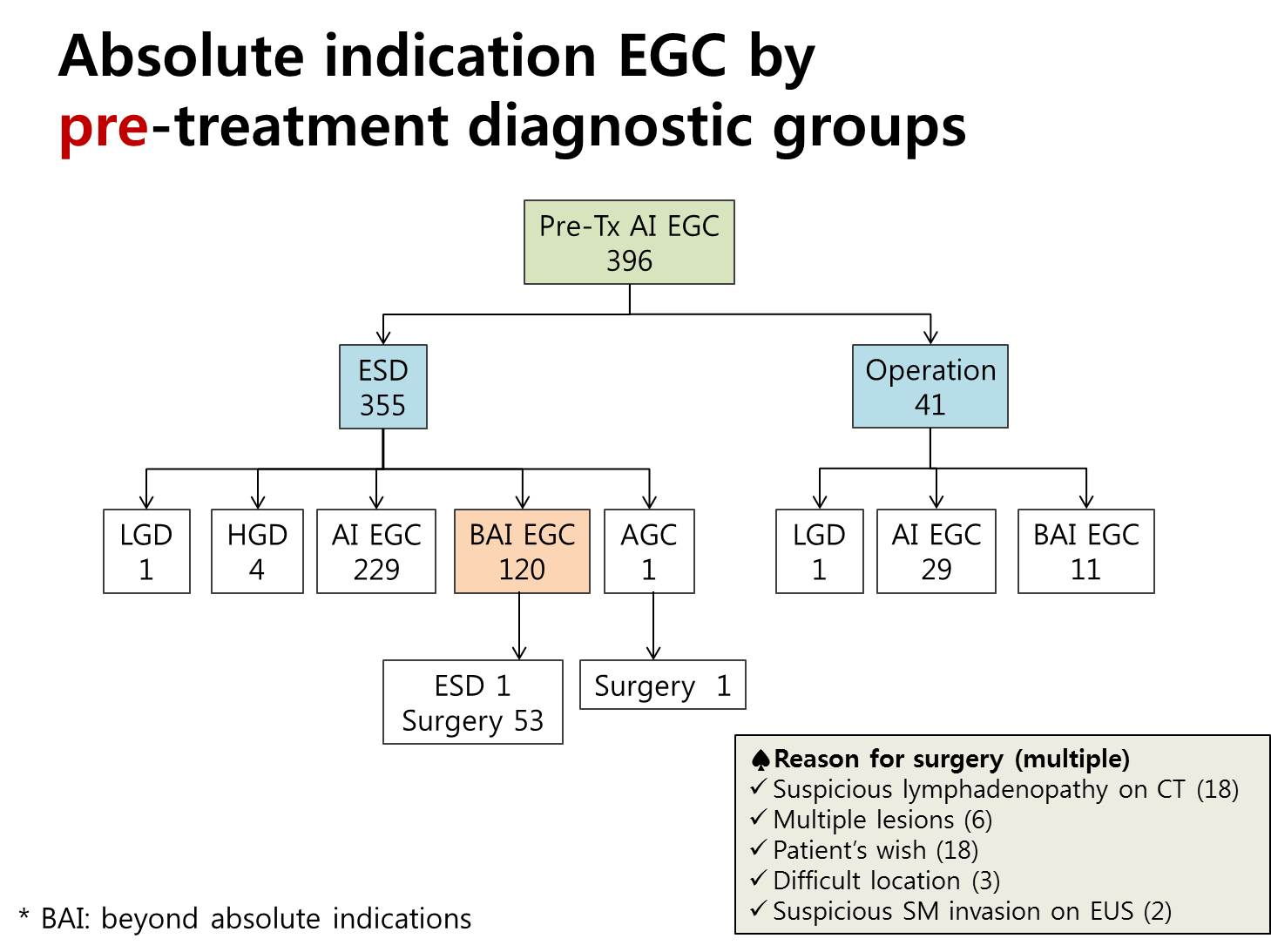
This flow diagram shows how we handled absolute indication early gastric cancers by the pretreatment diagnostic groups. Among 355 early gastric cancers initially treated by ESD, 120 cases, this is 34 percent, belonged to the beyond absolute indication group. Ten percent of patients in the absolute indication group were initially treated by surgery, and you can see the reason in the box at the right hand-side corner. Suspicious lymphadenopathy is the most common reason for surgery. I think this kind of analysis based on the pretreatment diagnostic group has a lot of clinical meanings in the decision making among the treatment options.

추적관찰이 짧았던 환자와 synchronous lesion 13명 등 제외기준을 적용한 후 1,306 환자 (조기위암 1,341 병소)에 대하여 중앙값 47 개월 동안 경과관찰하였습니다.
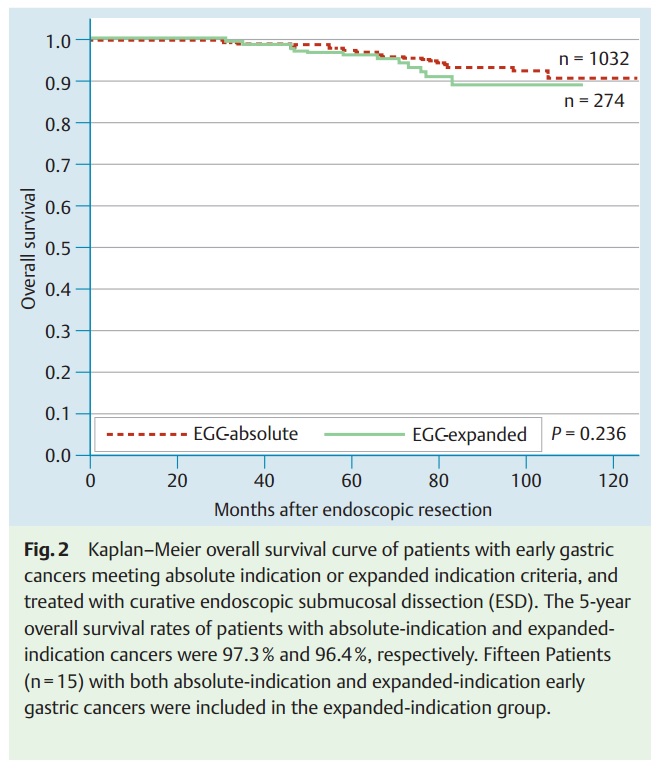
5년 생존율은 절대적응증의 경우 97.3%, 확대적응증의 경우 96.4%였습니다.
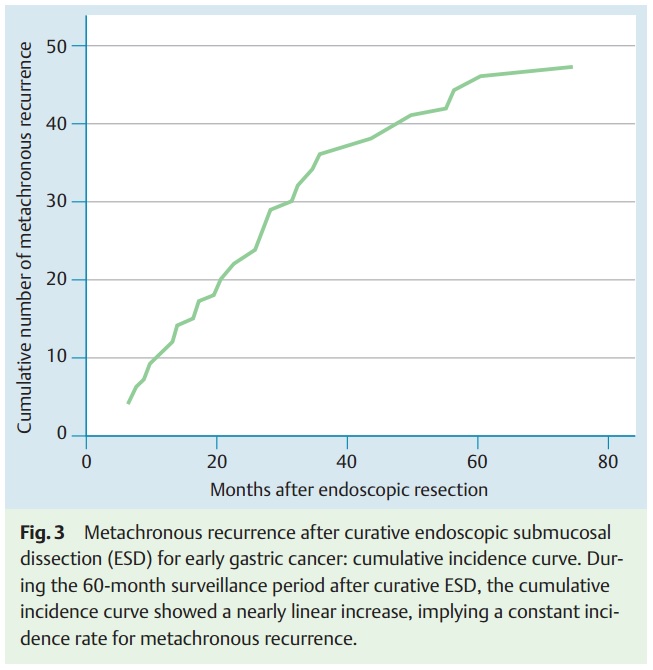
Metachronous recurrence는 47명 (3.6%, 47/1306)에서 발견되었습니다. 조기위암이 44예 (93.6%), 진행성위암이 3예였으며, 28예(60.0%)는 ESD로 19예(40.0%)는 수술로 치료하였습니다.

가장 중요한 extragastric recurrence는 절대적응증에서 1예, 확대적응증에서 1예가 있었습니다. 절대적응증 1예는 재발병소를 수술로 치료할 수 있었습니다. 그러나 확대적응증이었던 1예는 palliative surgery 밖에 할 수 없었습니다. 두 명 모두 처음 사진을 다시 보더라도 ESD를 했을 것 같은 환자입니다. 참 어렵습니다. 다행인 것은 1,306명에서 단 두 명만 extragastric recurrence를 보였다는 점이고 이는 radical subtotal gastrectomy의 일반적인 surgical mortality보다 낮은 수준이었습니다.
2) 로봇 위 절제술 (연세대학교 김형일)
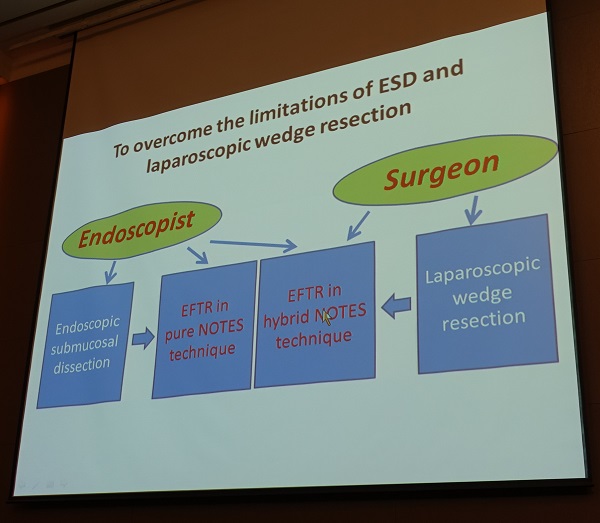
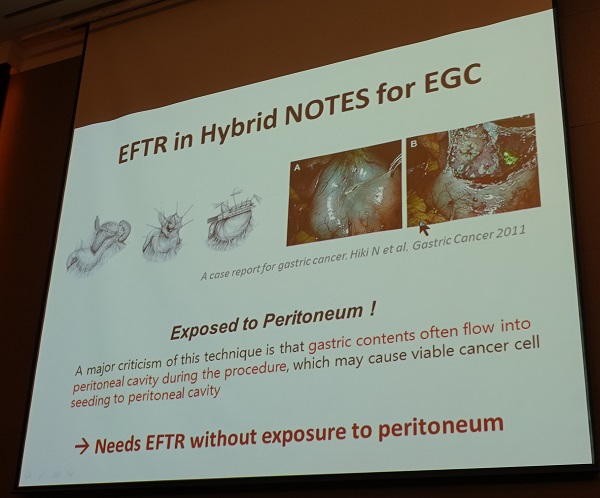
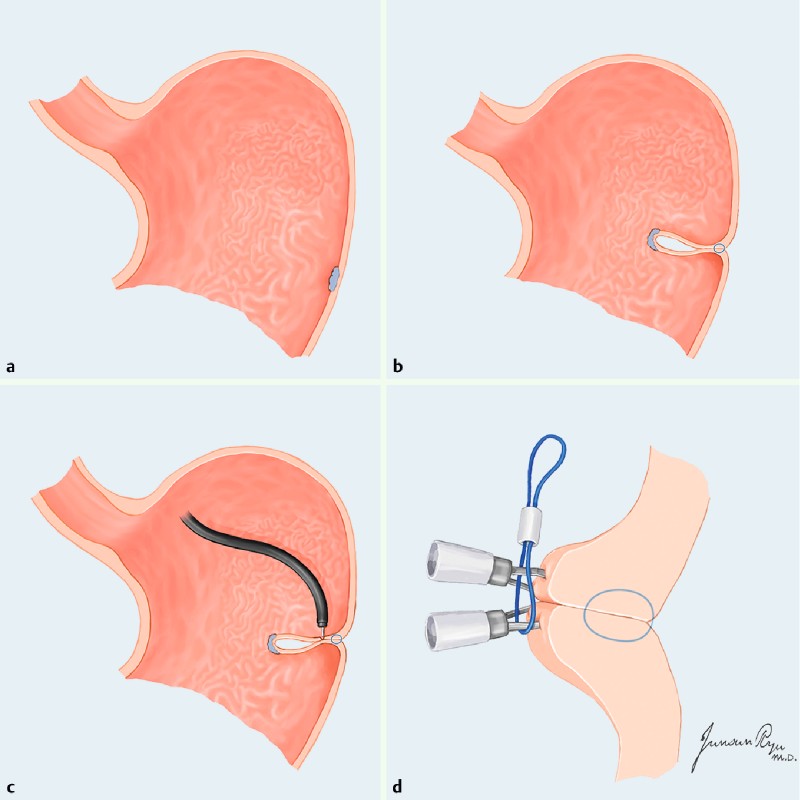
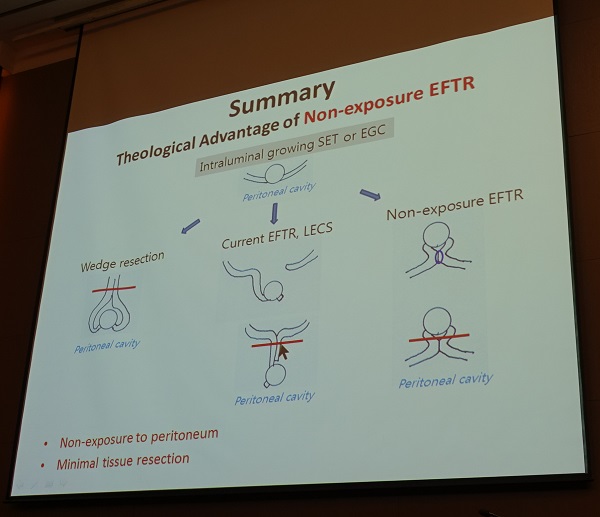
3) Endoscopic full thickness resection for EGC (국립암센터 김찬규)
국립암센터 김찬규 선생님께서는 2015년 12월 Endoscope 지에 발표한 내용을 중심으로 강의해 주셨습니다 (Kim CG. Endoscopy 2015).
기존의 Hybrid nodes법으로 시행하는 EFTR은 아래와 같은 장점이 있지만 no touch technique은 아니라는 단점이 있었습니다.
Advantage of EFTR
김찬규 선생님은 돼지를 이용하고 외과 의사의 도움을 받아 non-exposure 방법으로 full thickness resection을 하셨다고 합니다.
- No possibility of deep margin positive : full thickness resection
- Accurate resection margin evaluation : no stapler wire
- Visualization of the tumor at resection : endoscopic evaluation
4) Ongoing trials of organ-preserving surgery (서울대학교 외과 안상훈)
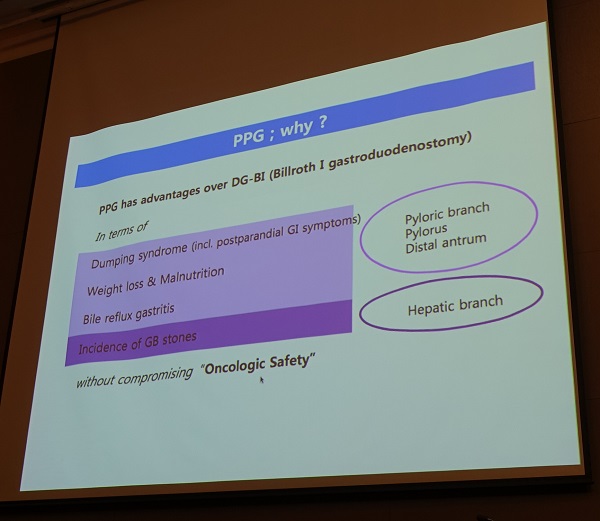
(1) Pylorus preserving gastrectomy (PPG)
일본에서는 30%가 시행되고 있는데 우리나라에서는 1% 미만에서 시행되고 있습니다. 전향적 연구가 진행되고 있습니다 (KLASS-04, PI: 서울대학교 이혁준, 간사: 분당서울대병원 안상훈, 2015년 7월 첫 환자가 enroll 되었음).
(2) Proximal gastrectom (KLASS-05, PI: 분당서울대병원 박도중, 간사: 분당서울대병원 안상훈)
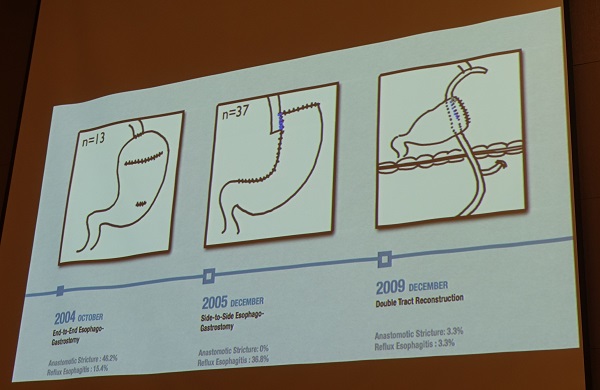
과거 proximal gastrectomy with esophagogastrostomy 후 reflux esophagitis, stricture와 같은 후기 합병증이 많아서 최근에는 total gastrectomy가 대세입니다. 외과 교과서에도 proximal gastrectomy를 추천하지 않고 있습니다. 최근 분당서울대병원에서는 근위부 조기위암에 대하여 laparoscopic proximal gastrectomy (LPG) with double tract reconstruction (DTR)을 시행하고 있습니다.
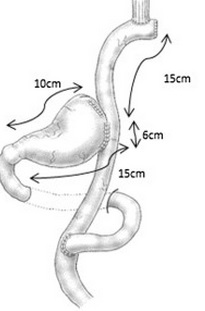
식도와 위 사이에 10-15 cm 간격을 유지하면 역류성 식도염은 큰 문제가 되지 않는 것 같습니다. 51예의 LPG with DTR 증례를 laparoscopic total gastrectomy와 후향적으로 비교해 보았는데, reflux esophagitis가 거의 발생하지 않았고 빈혈도 적었습니다. 현재 전향적 연구인 KLASS-05연구를 진행하고 있습니다.
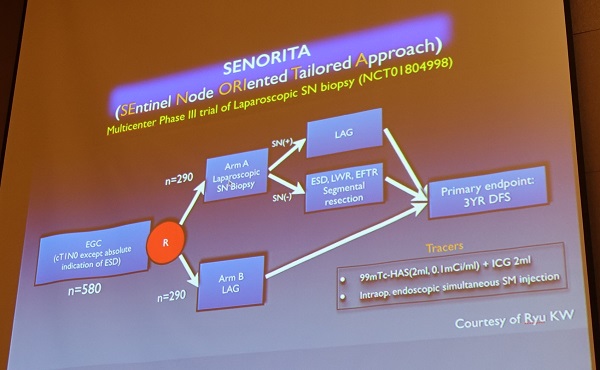
(3) Sentinel lymph node navigation surgery - 분당서울대병원에서 2상 연구, 국립암센터 주도의 다기관 3상 연구(SENORITA)가 진행되고 있습니다.
![]() 7. 오후 구연 세션
7. 오후 구연 세션
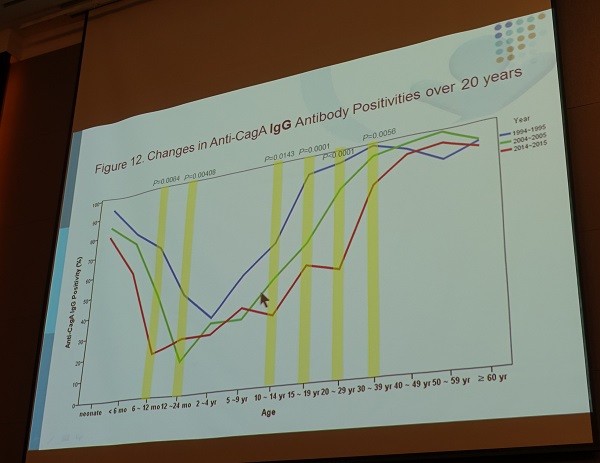
OA-1 (진주 경상대 박지숙). Immunoblot for Hp CagA in 진주
20년간 진주 지역의 anti-CagA IgG 항체 양성률의 변화 양상으로 볼 때 10년 후에는 30-39세가 50% 감염률을 유지하는 코호트 효과가 기대된다.
OA-2 (성균관대학교 강북삼성병원 양효준). Hp eradication on the promoter methylation of Wnt antagonist genes in gastric cancer
These results suggests that epigenetic silencing of SFRP and DKK family genes may mediate Hp-associated gastric carcinogenesis. Although many of them may persist even after Hp eradication once GC has been developed, methylation of DKK-3 may be reverseved by Hp eradication in GC patients.
OB-3 (경북대학교 권용한). Could we predict the metachronous gastric neoplasm after ER for EGC by using serum pepsinogen?
Persistent decreased serum PG I/II ratio (less than 3) during follow up period is a good indicator for predicting development MGN after ER for EGC and persistent Hp infectio could increase the risk of metachronous gastric neoplasm.
OC-1 (차의과대학교 차암연구소). 암예방김치 (cpKimchi = cancer preventive kimchi)
좌장 동국대학교 양창헌 교수님 comment: 식품은 식품으로 한계가 있다는 것을 잊지 말아야 한다.
OC-2 (차의과대학교 차암연구소). Plastem (placenta-derived mesenchymal stem cells)이 Hp로 인한 gastric damage에 대하여 anti-inflammatory, rejuvanating action을 한다.
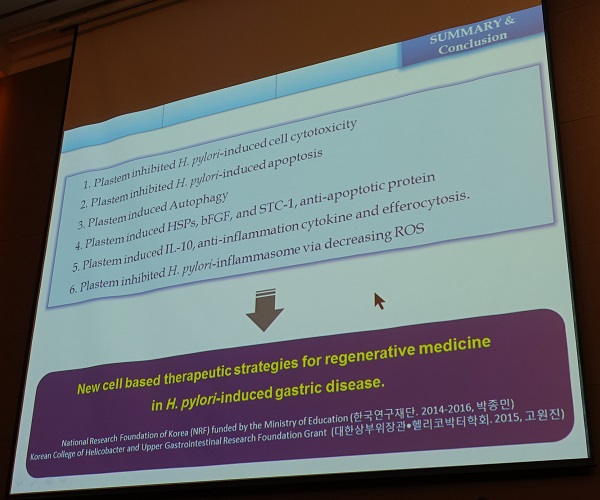
좌장 동국대학교 양창헌 교수님 comment: 효과가 있다는 것은 알겠는데, 제균치료를 하면 간단하지 않습니까?
![]() 8. 특강. Tips and cues for wonderful presentation with PowerPoint - 채종서 (PTIA 대표)
8. 특강. Tips and cues for wonderful presentation with PowerPoint - 채종서 (PTIA 대표)
메세지에 집중한다.
근거의 전달이 아니라 메세지에 집중한다. 메세지는 구체적이어야 한다. 초등학교 국어교실로 돌아가야 한다. 주어와 동사가 명확히 들어가야 한다.
메직아이는 가장 나쁜 프레젠테이션이다.
1) 전달내용 story
2) 시각자료 visual
Graphic overload에서 벗어나라. 기억나게 하기 위함이다. 단순함이 중요하다. 핵심 메세지가 3초 안에 가독되어야 한다. 대비가 중요하다. 적극적인 차이를 만들어야 한다. (1) 회색조, (2) 색, (3) 크기.
Noise를 찾아서 없앤다. 도형의 윤곽선은 사용하지 않는다. 이미지는 배경에 잠겨야 한다.
3) 전달기술 techniques
![]() [참고자료]
[참고자료]
© 일원내시경교실 바른내시경연구소 이준행