 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [APNM2016]
[APNM2016]
APNM에 다녀왔습니다. "선생님, 안녕하세요? 엔도투데이 잘 보고 있습니다. 오늘 취재하러 오셨어요?"라는 인사를 받았습니다. 종종 EndoTODAY에 학회를 소개하다보니 이제 공부하러 가는 것인지, 취재하러 가는 것인지 저도 모르겠습니다. 마침내 제가 교수출신 의학전문기자가 되었습니다. 하하하...^^
APNM은 놀라운 학회였습니다. 국제적 대가가 엄청 모였습니다. IBS 분야는 더욱 그러했습니다.
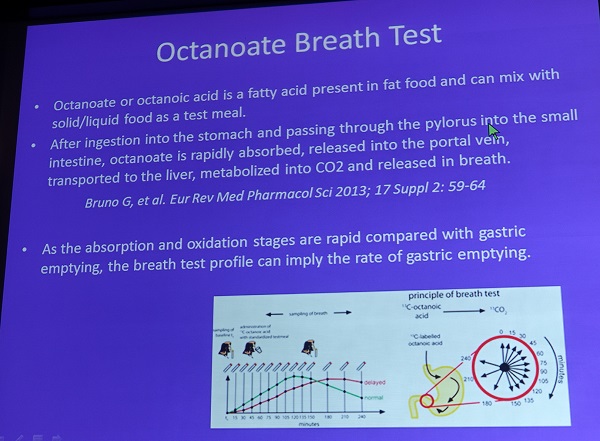
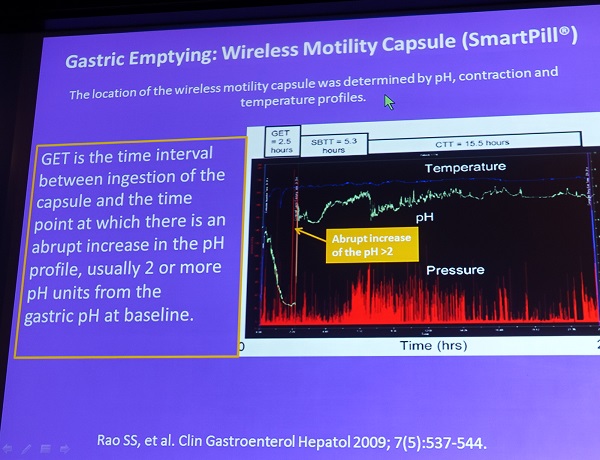
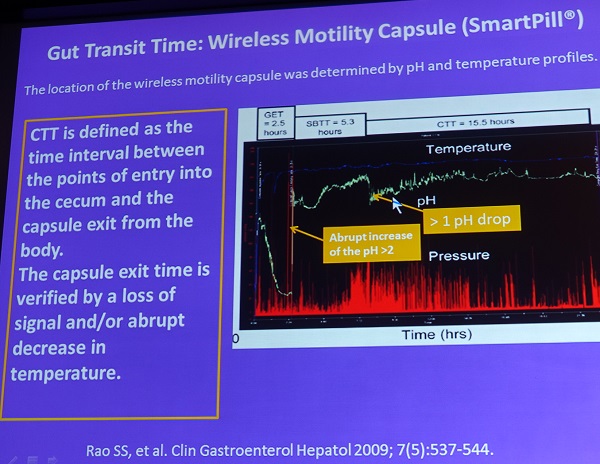
![]() 1. Gastric emptying and colonic transit (Sutep, Thailand)
1. Gastric emptying and colonic transit (Sutep, Thailand)
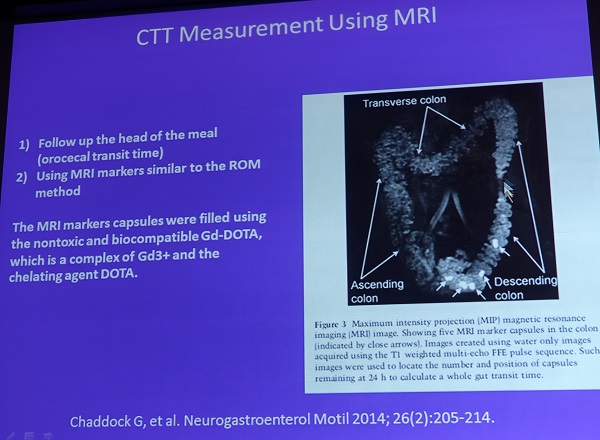
Gastric transit과 colonic transit 검사 중 smart pill 과 MRI가 주로 소개되었습니다. MRI를 이용한 transit 검사는 자세가 다르기 때문에 결과가 조금 다르게 나올 수 있다고 합니다.
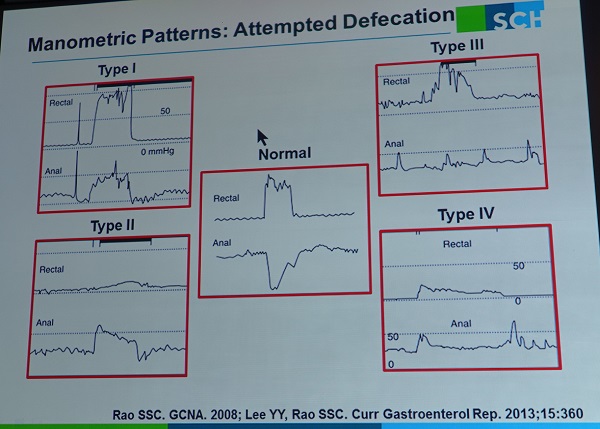
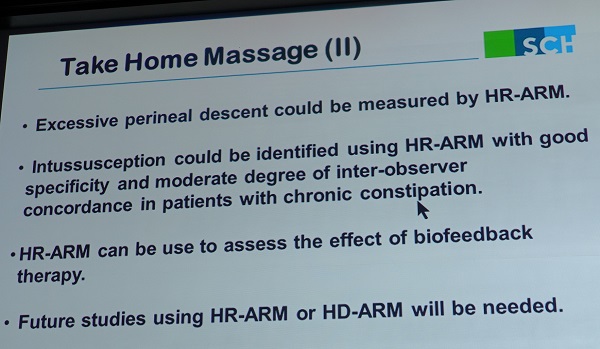
![]() 2. High resolution manometry in constipation (순천향대학교 이준성)
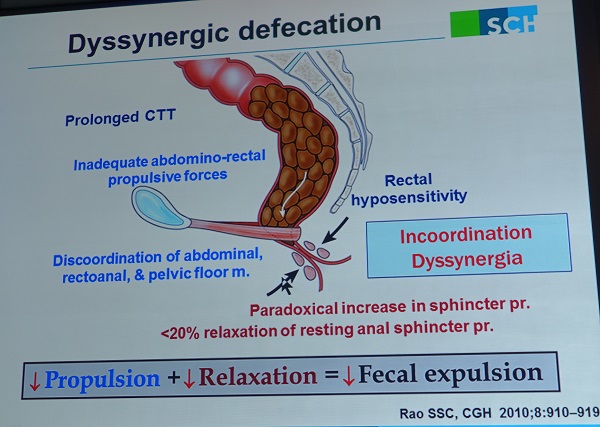
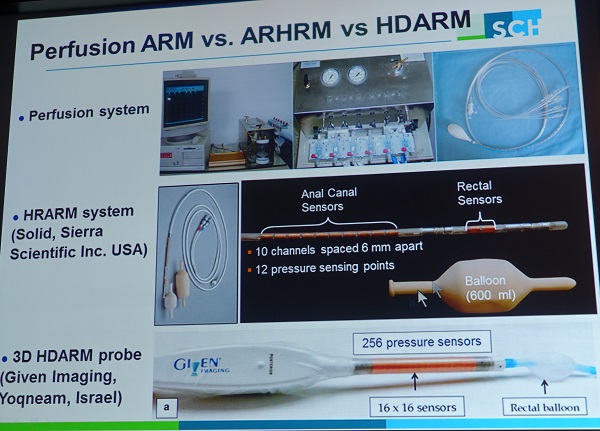
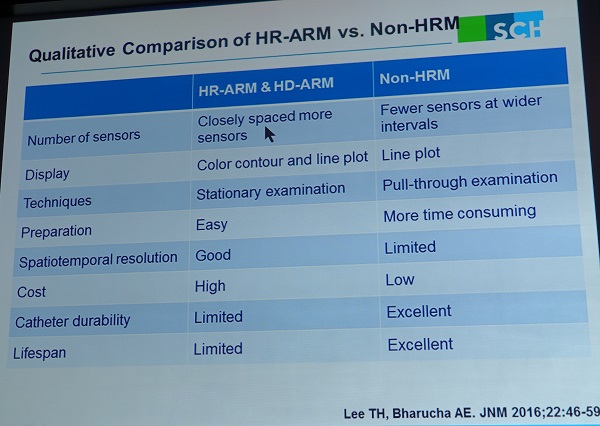
2. High resolution manometry in constipation (순천향대학교 이준성)


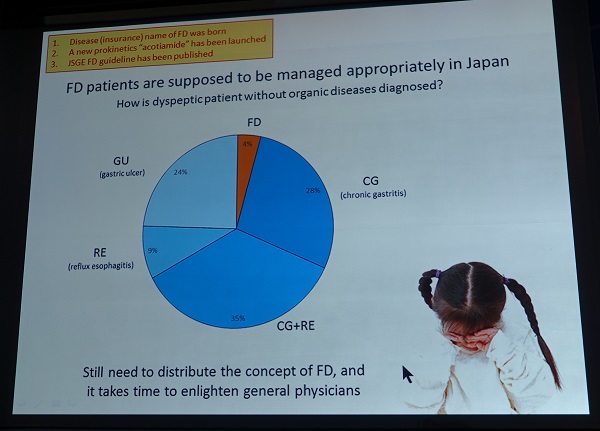
![]() 3. Functional dyspepsia (Miwa, Hogo College of Medicine)
3. Functional dyspepsia (Miwa, Hogo College of Medicine)
Dr. Miwa는 functional dyspepsia 분야는 일본이 one step 앞서 가고 있다고 자신있게 말했습니다 (국제 학회에서 이런 태도로 강의하는 사람은 처음보았습니다. 대가라도 겸손해 하는게 보통인데... 기분이 살짝 나빠지더군요). (1) 보험에서 functional dyspepsia라는 용어를 사용했고, (2) acotiamide라는 prokinetics가 일찍 도입되었고, (3) 근거 기반 가이드라인이 2014년에 발표되었기 때문이랍니다.


Functional dyspepsia가 chronic dyspepsia보다 훨씬 적다는 것이 특이했습니다. H. pylori 가 없는 경우만 FD로 간주해야 한다고 생각하는 일본인이 많은 것 같습니다. 이런 입장은 Kyoto global consensus에 반영되었습니다.

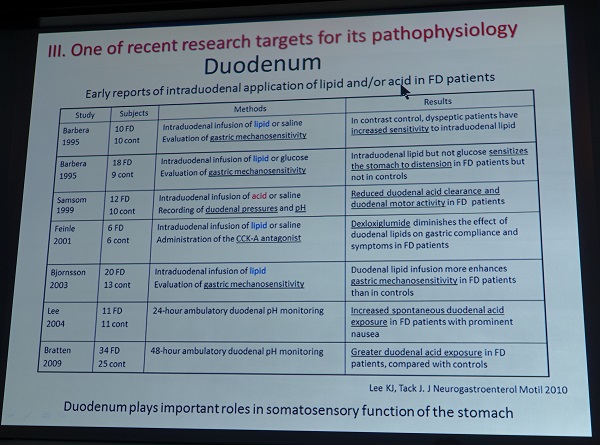
십이지장은 새로운 연구영역입니다. 예를 들어 Postinfectious FD 환자에서 십이지장 면역세포의 변화가 있다는 보고가 있습니다.

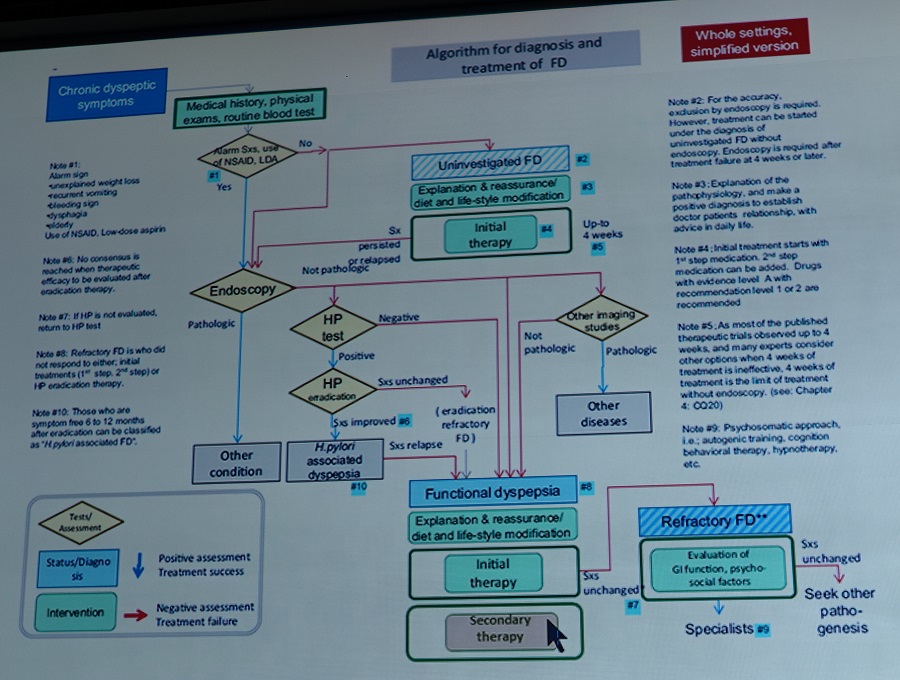
![]() 4. Treatment of FD (아주대학교 이광재)
4. Treatment of FD (아주대학교 이광재)
Rome III 의 증상기간이 practical 하지 않습니다. 한달전 시작한 증세로 찾아온 환자는 어찌 되는 것일까요?
이광재 교수님은 H pylori 양성 FD는 치료해야 한다는 의견을 말씀했습니다. "Patients whose dyspeptic symptoms are improved by H. pylori eradication,may be labled as H. pylori-associated dyspepsia." H pylori 양성자는 FD로 간주되지 말아야 한다는 의견인 것 같습니다. 저는 50% 동의합니다.
[2016-4-2. 이광재 교수님 편지]
이광재 교수님께서 제가 정확히 이해하지 못한 부분을 짚어주셨습니다. 제가 어제 'H pylori 양성자는 FD로 간주되지 말아야 한다'고 요약한 부분은 실수였습니다 (영어 hearing 실력이 부족하여). 감사합니다.
"교토 콘센서스에서 나온 H. pylori-associated dyspepsia의 개념에 동의한다는 것입니다. H. pylori 양성이라고 H. pylori-associated dyspepsia로 간주하는 것은 아닙니다. 교토 콘센서스에서는 초기 약물치료에 안 들으면 H. pylori test and treat를 해보고 호전이 있으면 의심해보고 6-12개월을 기다리자는 것입니다, H. pylori 치료로 완치가 될 수 있는 소수의 사람을 배려하는 개념인데요. 그런 부류의 환자 입장에서는 맞는 말이고요. 다만 그 진단 정의에 대해서는 더 많은 콘센서스가 필요하다는 말을 하였습니다. 저는 H. pylori 치료로 완치가 되는 사람을 기능성 소화불량증으로 진단되어서는 안된다는 개념에 동의한다고 하였습니다. H. pylori 양성을 FD로 간주해서는 안된다는 것은 아닙니다. 여전히 그 중 대부분은 FD이기 때문입니다.
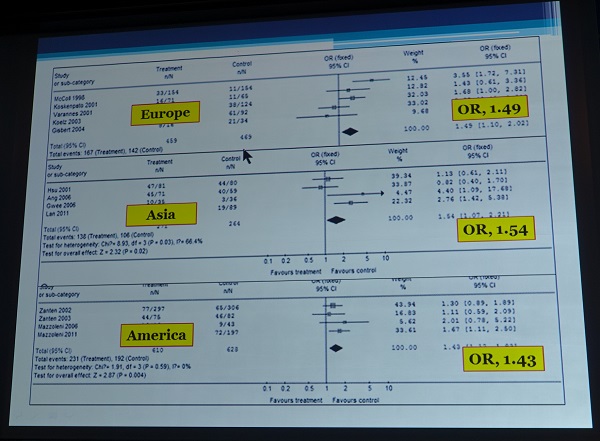
최근 메타연구에 의하면 H pylori 치료 효과는 지역에 따라 차이가 없었습니다.
Rome III의 EPS, PDS subgroup의 PPI response는 차이가 없는 것 같습니다. Rome III subgroup은 heterogenous합니다.

![]() 5. Response of PPI in Korean GERD patients (원광대학교 김용성)
5. Response of PPI in Korean GERD patients (원광대학교 김용성)
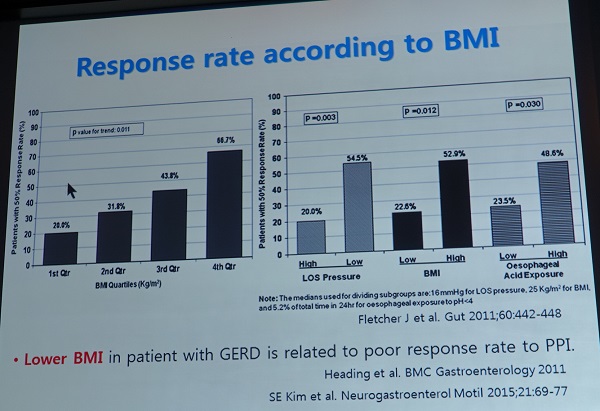
BMI가 높을 수로 GERD가 흔합니다. 그러나 BMI가 높으면 PPI response는 좋습니다.

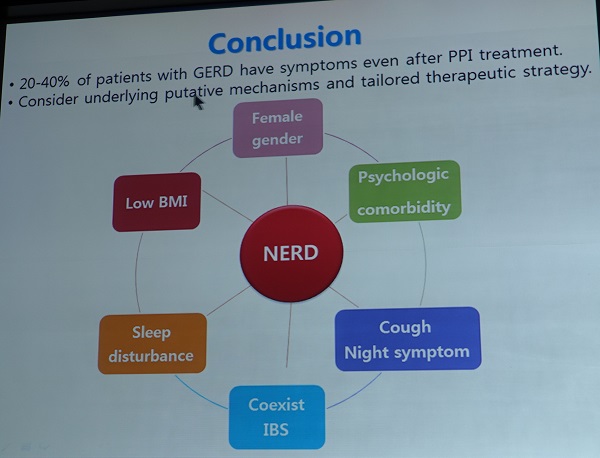
![]() 6. Options for GERD (Ronnie Fass)
6. Options for GERD (Ronnie Fass)
Satellite symposium 초대장에 Dr. Fass의 abstract가 있었습니다.
1) Refractory GERD is very common affecting up to 40% of the patients receiving PPI once daily.
2) The best initial approach is to optimize PPI treatment.
3) Evaluate for overlapping contributing factors for PPI failure.
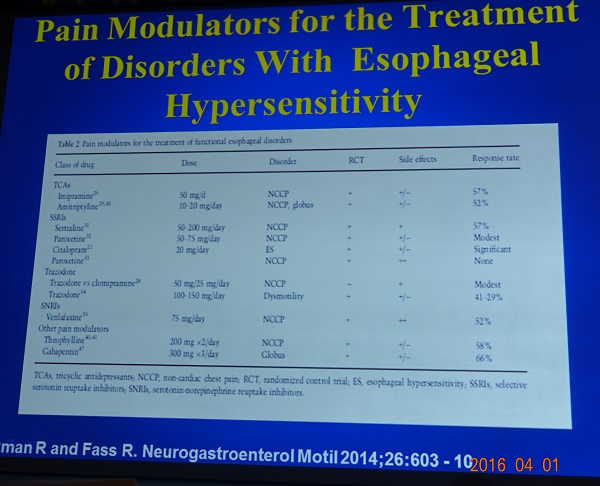
4) Pain modulators are an integral part of any therapeutic approach regardless if patients have functional heartburn or weakly acidic reflux.
5) Endoscopic and surgical treatment should be considered in a carefully selected patients.
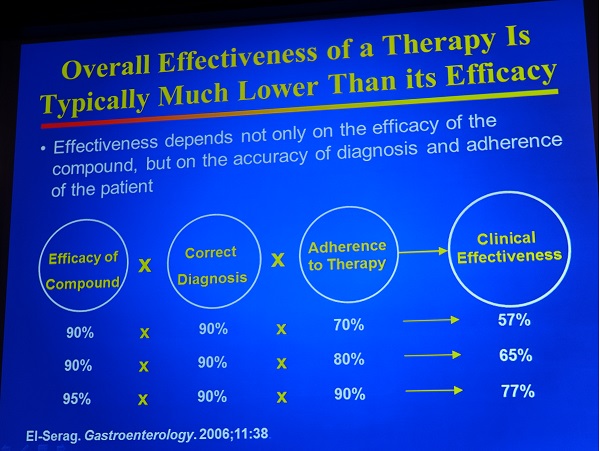
Refractory GERD는 "The current face of GERD inclinical practice"라는 말로 강의를 시작했습니다. 과거의 의사와 현재의 의사는 매우 다른 임상경험을 하고 있다는 것입니다.
Effectiveness와 efficacy에 대하여 상세히 설명하였습니다. 아래 두 슬라이드는 매우 중요할 것 같습니다.

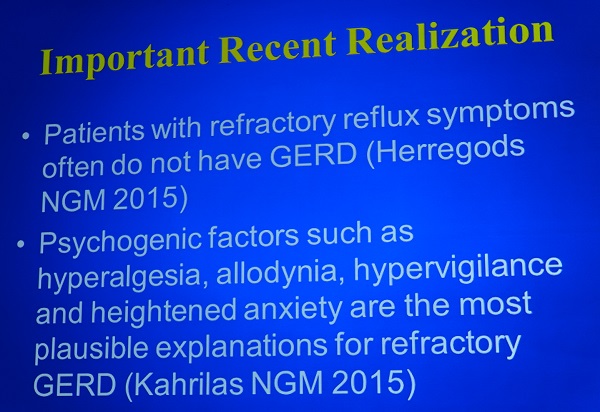
Important recent realization !!! (과거부터 다 알고 있던 것인데 세삼스럽게 recent realization이라는 제목을 붙였네요...)
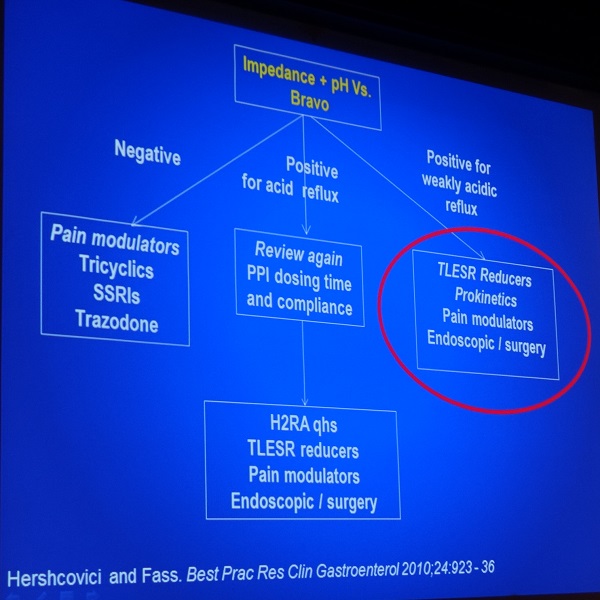
아래 슬라이드는 매우 재미있었습니다. PPI once daily에 반응이 없으면 셋 중 하나이고, PPI twice daily에 반응하지 않으면 둘 중 하나라고 합니다. 매우 단순하고 유용한 설명이라고 생각되었습니다.

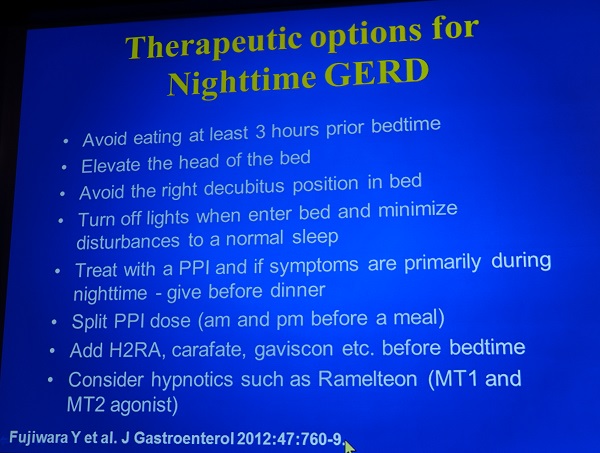
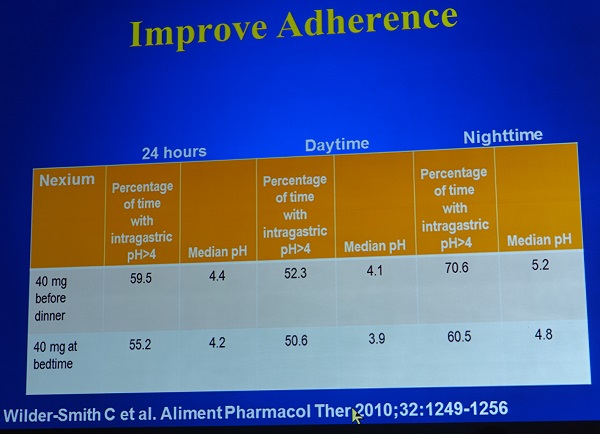
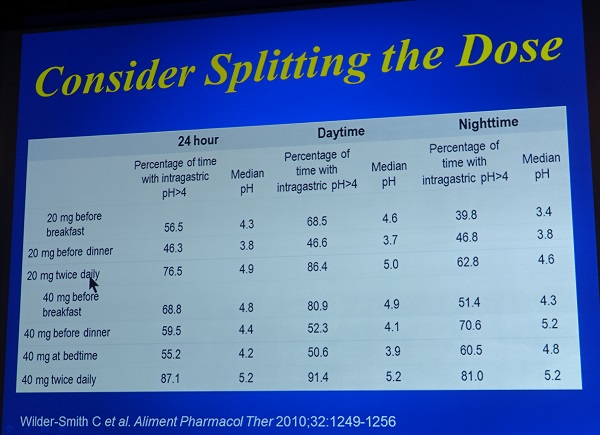
Nighttime GERD에 대한 아래 슬라이드 중 (1) 불을 꺼라, (2) 저녁 식사 전에 PPI를 주라, (3) Split 하라는 점은 인상적이었습니다.
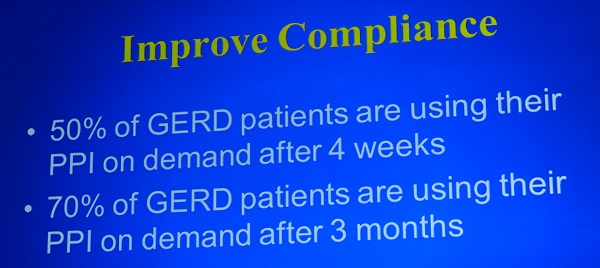
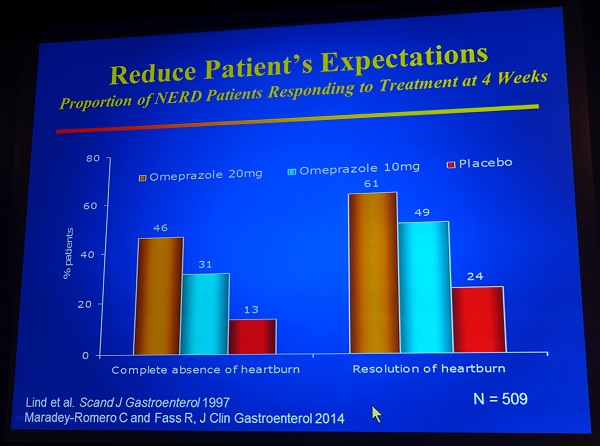
환자의 기대수준을 낮춰라!
GERD 내시경 치료가 간단히 언급되었는데, 효과보다는 가격과 부작용이 강조되었습니다. 아마 Fass 선생은 내시경 치료에 대하여 부정적인 시각을 가지고 있는 모양입니다.

저는 아래와 같은 질문 겸 comment를 했습니다. (저는 Fass 선생의 답변을 알아듣지 못했습니다. 주러리 주저리 말을 흘려서...^^)
"Very impressive lecture. Avialibility of PPI may be important. PPIs are prescription drug in Korea, but most PPIs are over the counter medication in your country. What's the influence of the over the counter PPIs in the diagnosis and management of GERD patients in your clinic?"
Compliance에 대한 질의 응답이 있었습니다. 환자들이 부작용을 우려한다고 합니다. PPI는 GERD의 원인을 고치지 않고 consequence를 바꿀 뿐입니다.
![]() [APNM2016 - 토요일 프로그램]
[APNM2016 - 토요일 프로그램]
화창한 날씨, 벚꽃이 한창인 워커힐 호텔. 깜깜한 지하에서 공부하는 것은 쉽지 않은 일이었습니다. 워커힐 호텔에서는 다음 주에 벚꽃 축제가 열린다고 합니다.
아침 7시 10분 조찬 세션부터 점심 세션까지 쉬지 않고 공부했더니 체력이 동났습니다. 아무래도 어제 저녁 fellow 들과 한잔 한 것의 여파가...... 병원으로 돌아와 quick하게 회진하고 집으로 갑니다. 일원동 병원에는 살구꽃이 한창이더군요. 꽃 피는 계절에는 학술모임 만들지 맙시다. 하하하...

![]() 8. Evidence-based recommendation for GERD treatment (Fass)
8. Evidence-based recommendation for GERD treatment (Fass)
 기대치를 높이지 말라는 점이 계속 강조되고 있습니다.
기대치를 높이지 말라는 점이 계속 강조되고 있습니다.
적절한 clinical endpoint 선정이 중요하다고 합니다. 너무 strict한 endpoint를 사용하면 차이가 없어 보이지만, loose한 endpoint를 사용하면 차이가 있을 수 있습니다.
Nighttime GERD는 흔하고 PPI로 충분히 조절되지 않는 경우가 많습니다. GERD와 sleep은 bidirectional effect가 있습니다. Fass 선생은 (1) PPI로 GERD가 호전되면 sleep이 좋아질 수 있고, 반대로 (2) hypnotic effect를 가지고 있는 melatonin-1,2 agonist로 sleep quality가 좋아지면 nighttime GERD가 좋아질 수 있다는 자료를 보여주었습니다.


![]() 9. Centrally trageted pharmacotherapy for chronic abdominal pain (Douglas A. Drossman)
9. Centrally trageted pharmacotherapy for chronic abdominal pain (Douglas A. Drossman)
여러 질환의 증상 발생에 CNS가 영향을 미칩니다.
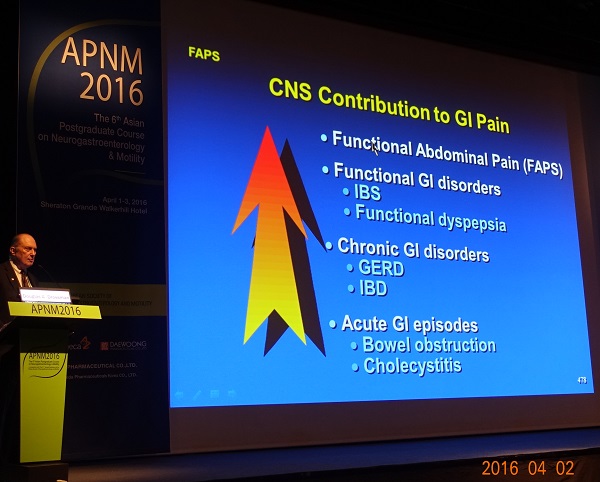
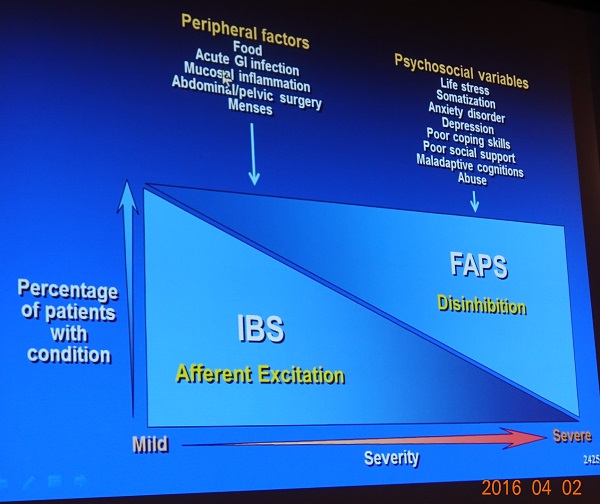
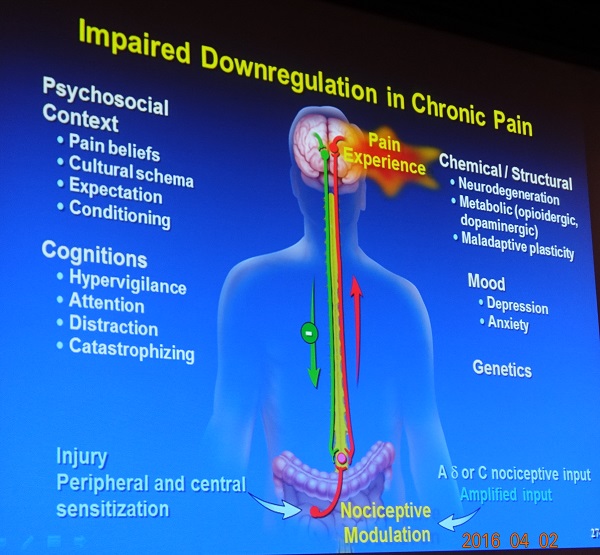
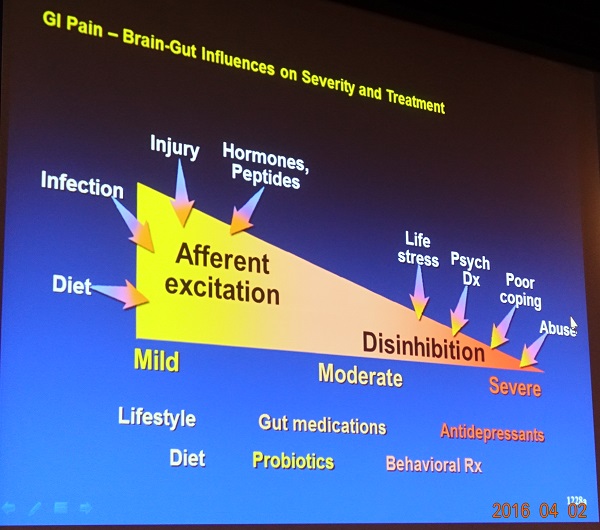
Psychopharmacological treatments provide benefit for management of chronic GI pain in several ways; (1) treatment of comorbid psychiatric disorders, (2) effects on modulating gastrointestinal motility, (3) reduction of afferent visceral nerve signaling and (4) enhancement of central downregulation pain modulation pathways. Psychopharmacological treatments may also enhance neurogenesis in the pain control areas, and this may potentially help to reverse the severity of clinical condition in general.
Dr. Drossman 자료의 특징은 각 슬라이드마다 번호가 붙어있었다는 것입니다. 자신의 모든 슬라이드에 번호를 붙이는 것 같았습니다. 고려할만 합니다.
![]() 10. Options for achalasia (연세대 윤영훈)
10. Options for achalasia (연세대 윤영훈)
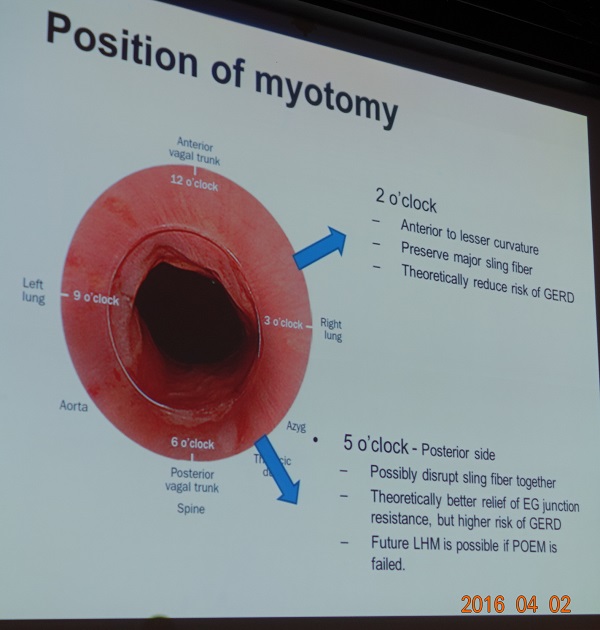
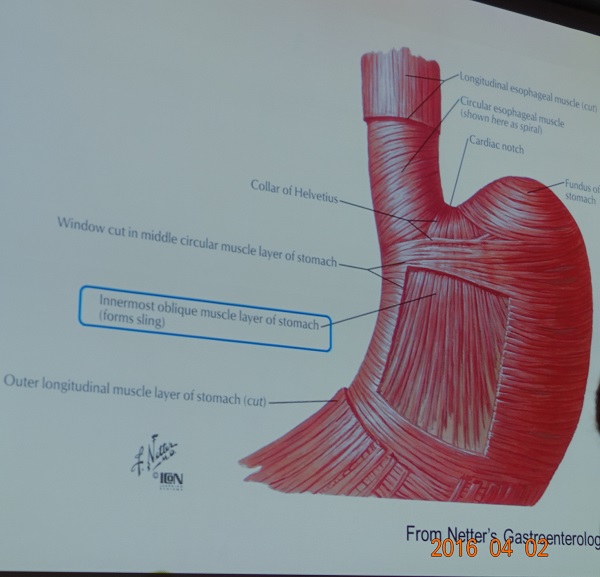
윤교수님은 myotomy 위치에 대하여 상세히 설명하셨습니다. 2시 방향은 sling fiber가 보존되므로 POEM 후 GERD가 덜 발생하고, 5시 방향은 sling fiber가 disrupt되므로 EG junction relief가 더 좋습니다. 최근에는 대부분의 시술자가 5시 방향(posterior approach)을 선호합니다. 혹자는 5시 방향으로 시술하더라도 조심스럽게 시술하면 sling fiber를 살릴 수 있다고 합니다. 내시경을 자연스럽게 잡고 가장 접근하기 쉬운 곳을 자르면 그곳이 대강 5시 방향입니다.
일본의 Dr. Inoue도 과거에는 2시 방향을 선호하다가 최근에는 5시 방향으로 시술하고 있다고 합니다. Dr Inoue의 최근 review에서 해당 부분을 옮깁니다 (Bechara R, Inoue H. Gastrointest Endosc 2016 - Epub).
The techniques used to perform a selective myotomy vary depending on the position of the mucosal incision as well as endoscopic orientation. When the muscle layer is in the 12 o’clock and the mucosa at 6 o’clock position (generally for anterior myotomy), acute tip angulation is required to hook the circular muscle layer. In contrast, when the muscle is kept in the 6 o’clock position (generally for posterior myotomy, which is our current practice), much less tip angulation is required and there is less "fling" of the knife.
Dr. Fass는 미국에서는 POEM 후 GERD가 훨씬 흔하고, stricture도 종종 발생한다고 코멘트 하셨습니다. .
Dr. Fass는 EG junction outflow obstruction도 POEM의 적응증이 되는지 질문하였고, 윤교수님은 possible future indication일 수 있지만, 아직 그 질환을 잘 알지 못하고 botox로 치료되는 경우가 많아 지금은 시술하지 않는다고 답하셨습니다.
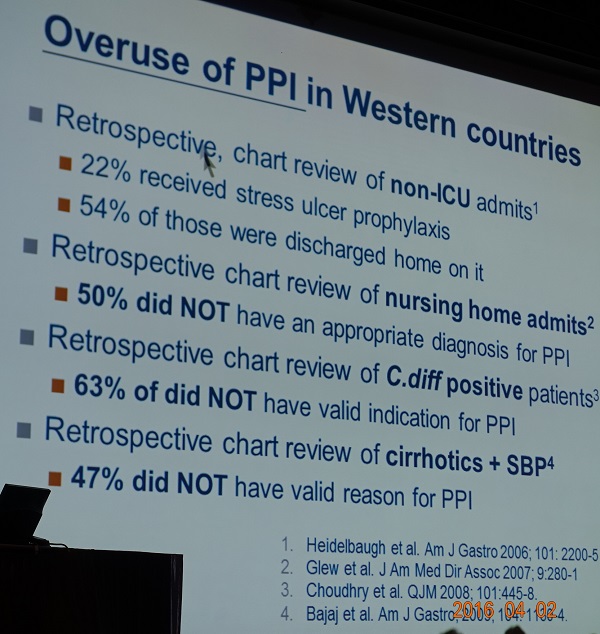
![]() 11. [런천] Optimal use of proton pump inhibitors in primary care (Ching-Liang Lu, Taiwan)
11. [런천] Optimal use of proton pump inhibitors in primary care (Ching-Liang Lu, Taiwan)
BID 투약의 시점은 아침 식전과 저녁 식전입니다.
최근 발매된 dexlansoprazole은 한 capsule에 두 가지 다른 형태의 granule이 있어서 혈중농도가 dual peak를 보이고 plasma half-life가 길다는 점이 marketing point인 것 같습니다.


PPI 회사가 주최하는 런천에서 PPI overuse, 부작용 등이 다뤄진 점은 긍정적입니다. 전문가 집단의 자존심 같은 것이지요.
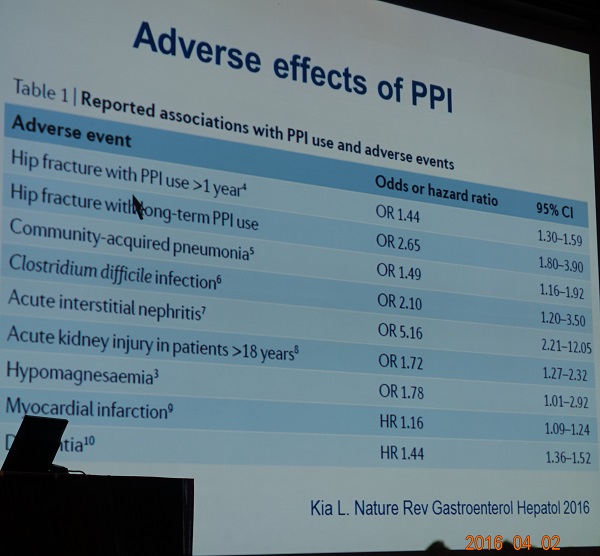
PPI가 dementia와 관련될 수 있다는 보고가 흥미로웠습니다 (Gomm W. JAMA 2016).

RESULTS: A total of 73,679 participants 75 years of age or older and free of dementia at baseline were analyzed. The patients receiving regular PPI medication had a significantly increased risk of incident dementia compared with the patients not receiving PPI medication (n=70,729; mean [SD] age, 83.0 [5.6] years; 73.6% female) (hazard ratio, 1.44).
CONCLUSIONS AND RELEVANCE: The avoidance of PPI medication may prevent the development of dementia. This finding is supported by recent pharmacoepidemiological analyses on primary data and is in line with mouse models in which the use of PPIs increased the levels of β-amyloid in the brains of mice. Randomized, prospective clinical trials are needed to examine this connection in more detail.
![]() 12. [런천] PPI in the management of GERD (고신대학교 박무인)
12. [런천] PPI in the management of GERD (고신대학교 박무인)
박무인 선생님은 hypomagnesemia를 강조하셨습니다.
EndoTODAY hypomagnesemia에서 소개한 바 있지만 아래에 다시 옮깁니다. 드물지만 매우 중요한 일이니까.
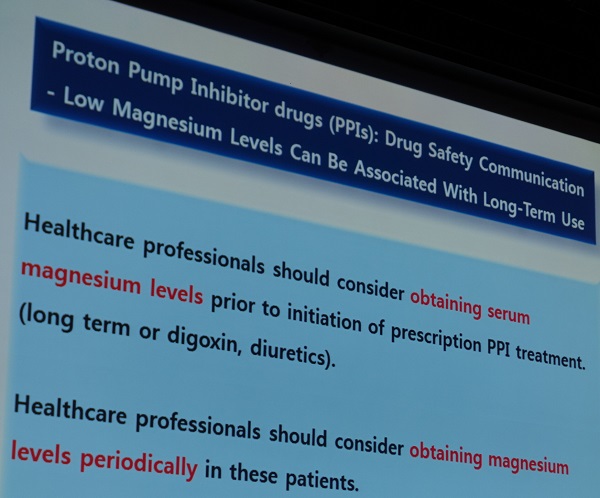
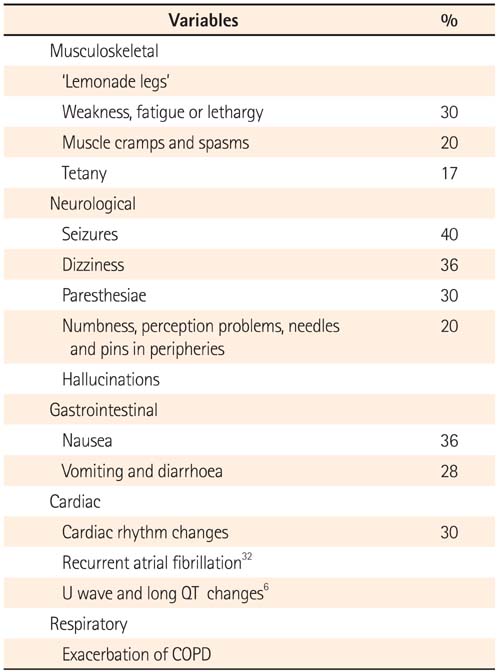
"Lemonade Legs"라는 말을 들어보셨습니까? Intestinal Research 2015년 3호에 실린 종설의 제목입니다 (Atkinson. Intest Res. 2015). PPI 사용자에서 간혹 발생하는 hypomagnesemia에 의한 근골격계 증상을 표현하는 용어라고 합니다. Weakness, fatigue, muscle cramps and spasms, tetany 등이 가능합니다. 신경증상, 소화기증상, 부정맥, COPD의 악화 등도 PPI에 의한 hypomagnasemia와 관련될 수 있습니다.
PPIs are widely used though an association with hypomagnesaemia and hypocalcaemia has only been described since 2006. Patients typically present after years of stable dosing with musculoskeletal, neurological or cardiac arrhythmic symptoms, but it is likely that many cases are under-recognised. Magnesium levels resolve rapidly on discontinuation of PPI therapy and hypomagnesaemia recurs rapidly on rechallenge with any agent in the class.
The cellular mechanisms of magnesium homeostasis are increasingly being understood, including both passive paracellular absorption through claudins and active transcellular transporters, including the transient receptor potential channels (TRPM6) identified in the intestine and nephron. PPIs may alter luminal pH by modulating pancreatic secretions, affecting non-gastric H+K+ATPase secretion, altering transporter transcription or channel function. A small reduction in intestinal absorption appears pivotal in causing cumulative deficiency. Risk factors have been associated to help identify patients at risk of this effect but clinical vigilance remains necessary for diagnosis.
Hypomagnasemia는 PPI 장기사용자에서 발생하는 경우가 많지만, 간혹 PPI 사용 2주 후에도 발생할 수 있습니다. Class effect도 있습니다. 한 PPI에 의하여 hypomagnesemia가 발생하면 다른 PPI로 바꿔도 발생한다는 것입니다. 증상은 매우 다양합니다. 부정맥도 가능합니다. Hypomagnesemia를 의심하지 못한 상태에서 갑자기 돌아가시는 분도 없지 않을 것 같습니다.
아직 PPI 사용자의 magnesium 측정 지침은 없습니다. 조금이라도 의심되면 검사해보는 수 밖에 없을 것 같습니다. 응급실에서는 더욱 중요합니다. 증상이 없더라도 PPI 장기 사용자와 이뇨제 사용자에서 고려해 볼 수 있을 것 같습니다. 다행스럽게 아주 흔한 일은 아니라고 합니다.
Histamine 2 receptor antagonist도 hypomagensemia를 일으킬 수 있습니다 (Kieboom BC. Am J Kidney Dis 2015). 그러나 그 정도는 PPI보다 덜 심한 모양입니다.
메타연구에서 PPI와 위축성 위염의 관련성은 없었습니다. 그러나 H pylori 양성자에서 PPI 장기 사용은 위축성 위염을 악화시킬 수 있다는 최근 연구가 있습니다.
![]() [APNM2016 - 일요일 프로그램]
[APNM2016 - 일요일 프로그램]
![]() 13. Plenary oral presentations
13. Plenary oral presentations
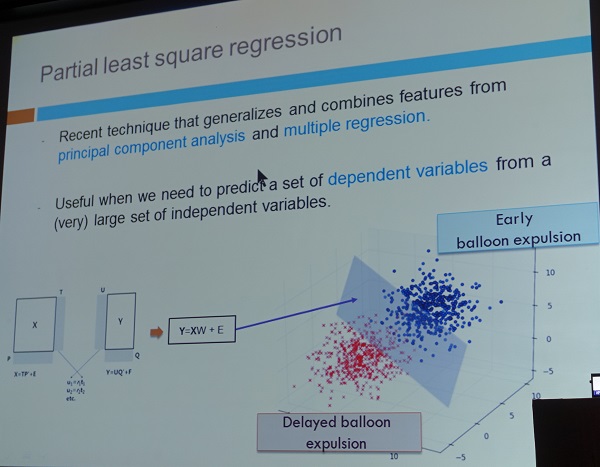
1) 서명숙 (아산병원). Balloon expulsiontest의 결과를 예측하는 high resolution anorectal manometry의 parameter를 제시했습니다. HRM만 시행하고 balloon expulsion test를 하지 않을 수 있다고 설명했습니다. Floor에서 "HRM 결과가 BET 결과가 biofeedback 효과를 더 잘 예측했는가?" 질문이 있었습니다.
Partial least square regression 개념이 소개되었습니다.
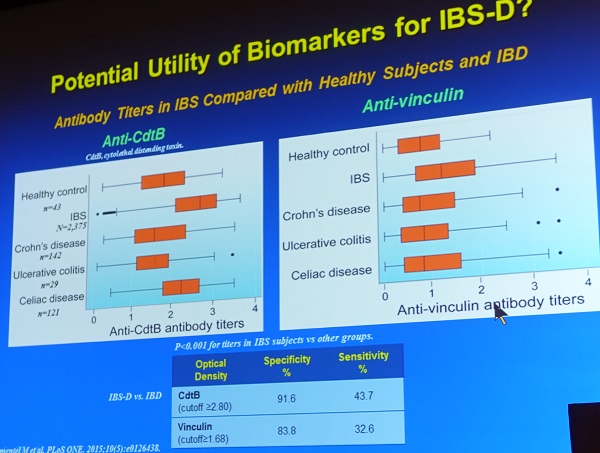
2) 김재학(동국대). Mixed type IBS의 biomarker로 anti-vinculin A antibody와 cytolethal distending toxin B antibody를 제시했습니다. Floor에서는 IBS-D와 post-infectious IBS에서 더 좋은 마커일 것 같다는 의견이 있었습니다.

3) 박유미 (연세대 강남세브란스).

Methane은 peristaltic velocity는 줄이고 Amplitude를 올리고 calcium signal을 올립니다. 연구자들은 몇 가지 약물과 Calcium imaging study등을 이용하여 methane은 cholinergic pathway으로 작용하는 another gasotransmitter로 간주되어야 한다고 주장하였습니다.
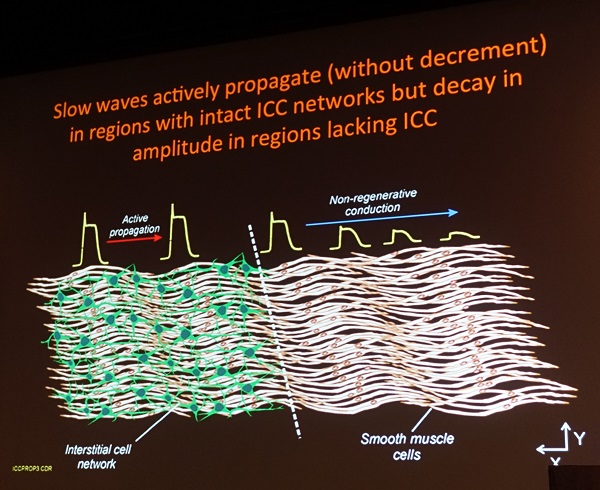
![]() 14. State of the art lecture: Significance of interstitial cells in neurogastroenterology (Kenton M. Sanders, University of Nevada)
14. State of the art lecture: Significance of interstitial cells in neurogastroenterology (Kenton M. Sanders, University of Nevada)
주로 2015년 논문(Baker. J Physiol 2015)을 중심으로 설명하셨습니다.
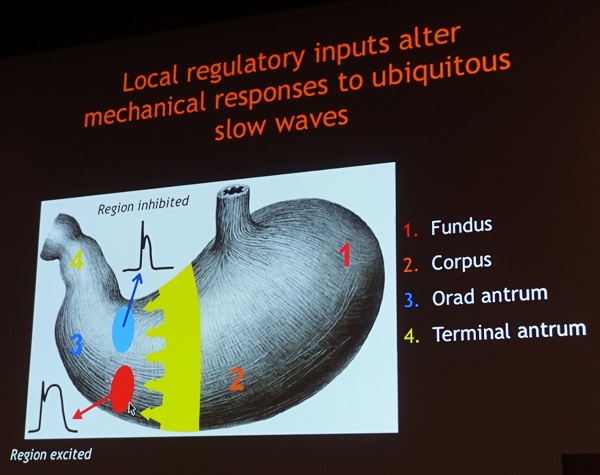
c-Kit을 ICC의 마커로 이를 이용하면 ICC의 분포를 알 수 있습니다. ICC은 위장관 벽의 여러 level에 위치합니다.

SIP syntytium (Smooth muscle cell, ICC, PDGFRalpha+ cells)
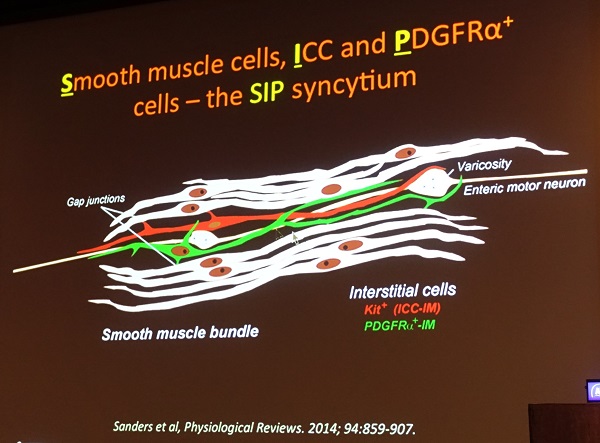

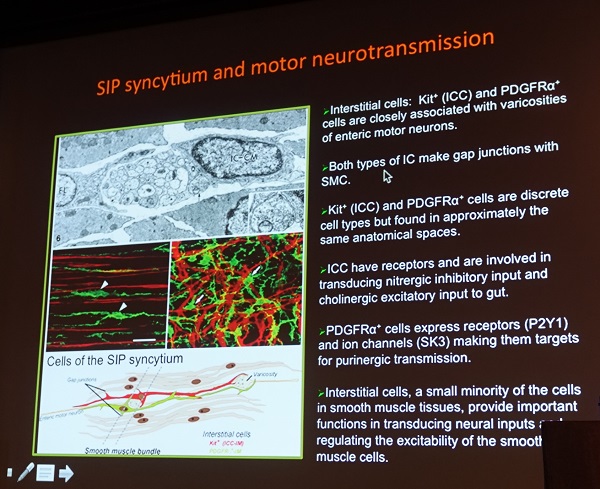
Dr. Sanders는 마지막으로 몇 가지 다른 종류의 세포들도 관여한다는 슬라이드를 보여주며 강의를 마쳤습니다. 매우 멋지고 훌륭한 강의였습니다.

![]() 15. Rome-KSNM Symposium: Rome III criteria for functional GI disorders: Is there a need forbetter definition? (William D. Chey, University of Michigan)
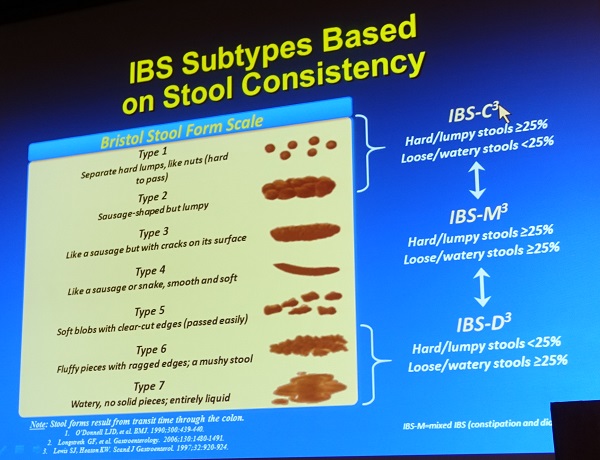
15. Rome-KSNM Symposium: Rome III criteria for functional GI disorders: Is there a need forbetter definition? (William D. Chey, University of Michigan)
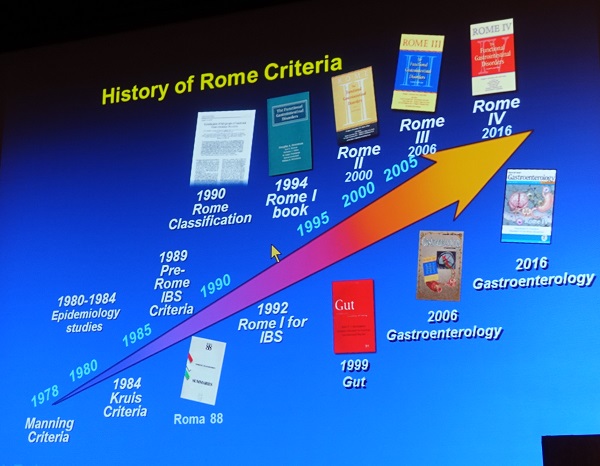
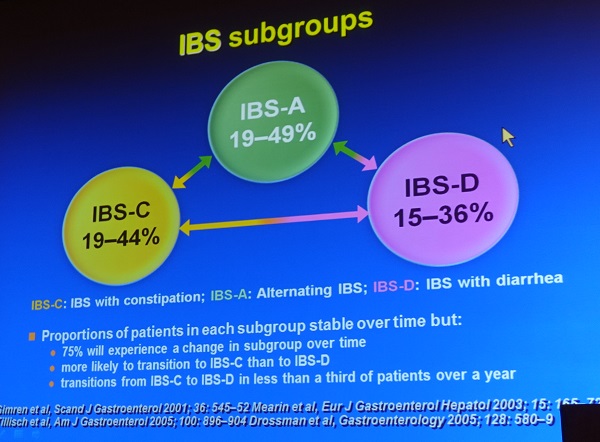
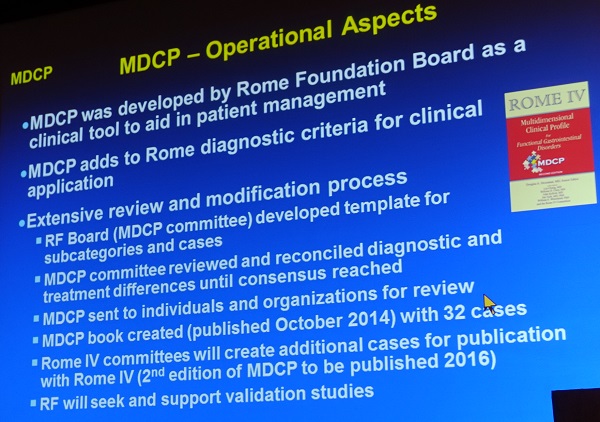
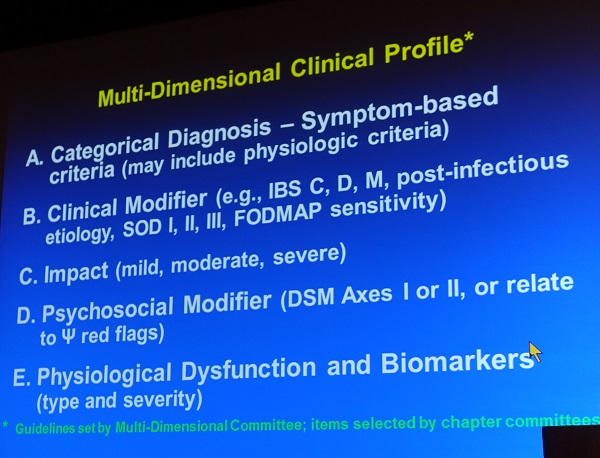
올해 발표될 예정인 Rome IV는 (1) 보다 근거 기반으로, (2) 증상 빈도를 중시하고, (3) 현실적인 subtype을 제시할 예정이라고 합니다. MDCP (multidimentional clinical profile)을 통하여 만들어지고 있는 모양입니다. 아래 예와 같이 엄청, 엄청 복잡해질 모양입니다.
Symptom-based criteria offer modest accuracy inidentifying patients with IBS. Symptoms with biomarkers and psychological markers appears to be more effective.

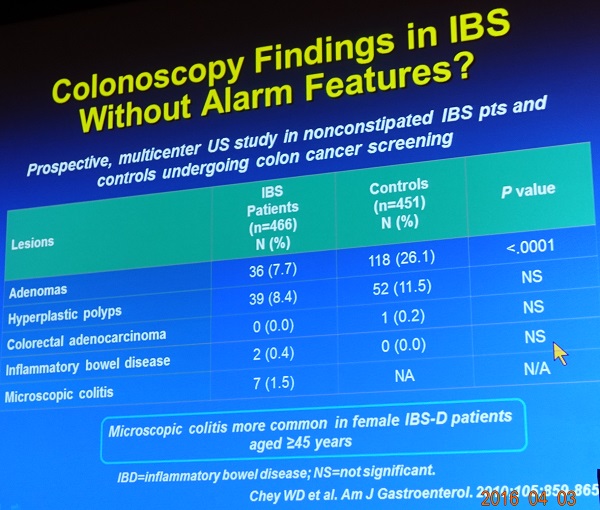
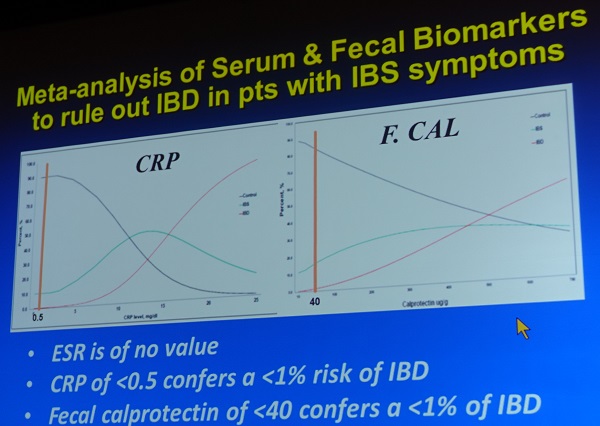
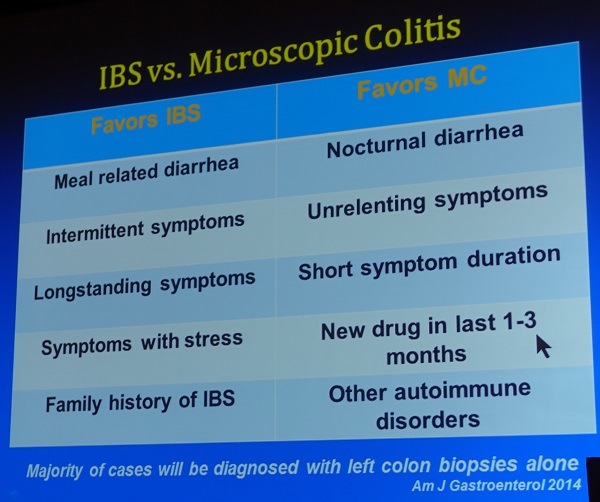
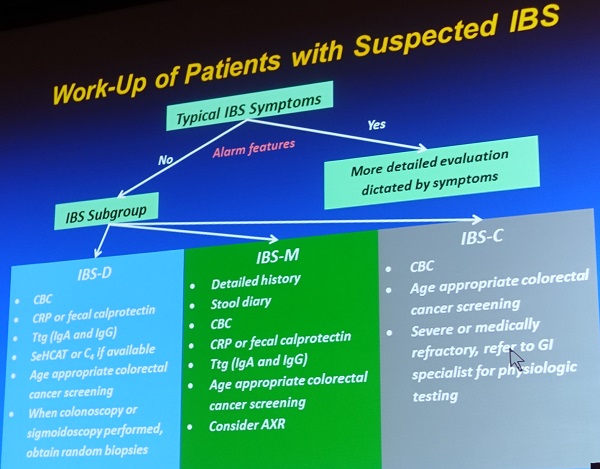
Dr Chey는 IBS 증상을 가진 사람 중 다른 질환을 가진 사람들을 골라내야 한다는 점을 강조하였습니다. Rule ou 뿐만 아니라 몇 가지 rule in biomarker (CdrB, vinculin)도 소개하였습니다.
CRP, fecal calprotectin이 낮으면 IBD 가능성이 낮습니다. IBS와 IBS 구분을 위하여 ESR은 쓰지 맙시다.
Microscopic colitis는 IBS-D 증상을 가진 사람에서 흔합니다.
Rome IV를 만들기 위한 노력이 계속되고 있는 모양입니다.
* 이준행 comment: Dr. Chey의 강의는 매우 좋았습니다. 그러나 Rome foundation은 수명을 다한 것 같습니다. 아시아, 남미, 아프리카 학자는 단 한 명도 포함되지 않은 그들만의 board of directors에서 만든 criteria를 전세계 사람들이 사용한다는 것은 도무지 맘에 들지 않습니다.

Rome criteria는 스스로의 논리에 의하여 점차 복잡해지고 있습니다. 연구 중심일 뿐, 환자는 안중에도 없어 보입니다. 아무래도 조만간 저절로 붕괴될 것 같습니다. Rome foundation은 미국 대학교수에게나 필요하지, 저같은 평범한 대한민국 의사에게는 불필요해 보입니다. 설익은 연구 결과에 의존하여 10년마다 진단기준이 바뀌었고, 그때마다 기준만 다를뿐 비슷한 내용의 연구들이 양산되었지만 도대체 뭐가 달라졌습니까? 전세계의 여러 학자들이 자신의 연구와 경험을 바탕으로 진단 기준을 제시하는 것이 옳지 않을까요? 활발한 연구와 논의를 통하여 가장 좋은 기준이 자연스럽게 선택되겠지요. Rome foundation이라는 단체에서 온갖 질환의 진단 기준을 독점하고 있다는 것 자체부터 말이 되지 않습니다. 무슨 이익단체 비슷하게 되버렸습니다.
Rome criteria 관련 공부는 이제 그만 할까 합니다. 10년마다 뻔한 공부를 반복하자니 시간이 아깝습니다.
![]() [참고자료]
[참고자료]
© 일원내시경교실 바른내시경연구소 이준행