 EndoTODAY ГЛНУАц БГНЧ
EndoTODAY ГЛНУАц БГНЧ
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Asian Young Endoscopist Forum]
[Asian Young Endoscopist Forum]
НУАЃ: 2016Гт 6Пљ 24РЯ ПРШФ
РхМв: БзЗЃЕх ШњЦА ШЃХк

ОЦНУОЦ АЂБЙРЧ РўРК РЧЛчЕщРЬ ПьИЎГЊЖѓ ПЉЗЏКДПјПЁМ 2СжАЃРЧ trainingРЛ ЙоДТ ЧСЗЮБзЗЅРЬОњНРДЯДй. АЂРк ТЊРК presentationРЛ ЧЯПДНРДЯДй. РњДТ УЙЙјТА МММЧРЧ discussantЗЮ ТќПЉЧЯПДНРДЯДй. ШяЙЬЗЮПќДј ЙпЧЅ Ию АГИІ ПфОрЧеДЯДй.

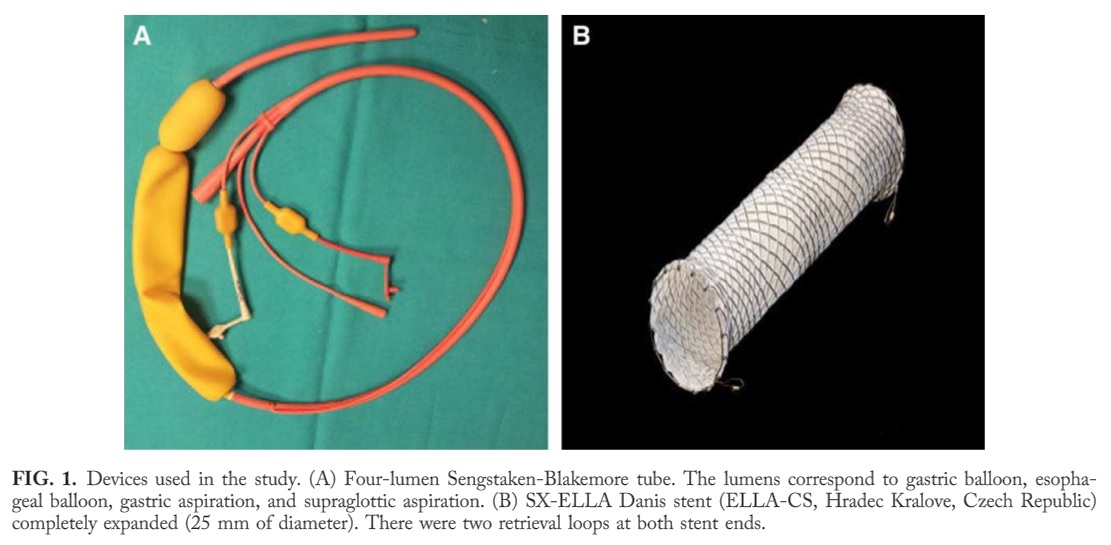
![]() 1. The use of self-expanding metal stent for refractory variceal haemorrhage. Chinmay Bera (India)
1. The use of self-expanding metal stent for refractory variceal haemorrhage. Chinmay Bera (India)
СжЗЮ EVL ШФ ЙпЛ§Чб EVL ulcerЗЮ РЮЧб refractory esophageal bleedingРЛ self-expandable esophageal covered metal stent (SX-Ella DANIS stent, Czech Republic)ЗЮ ФЁЗсЧб АцЧшРЛ ЙпЧЅЧЯПДНРДЯДй.
ИЖФЇ ААРК stent СІЧАРЛ ЛчПыЧб ПЌБИАЁ 2016Гт 6Пљ HepatologyСіПЁ ЙпЧЅЕЧОњНРДЯДй (Escorsell A. Hepatology 2016).
Results: Twenty-eight patients were randomized to Sengstaken-Blakemore tube (n = 15) or SX-ELLA Danis stent (n=13). Patients were comparable in severity of liver failure, active bleeding at endoscopy, and initial therapy. Success of therapy was more frequent in the esophageal stent than in balloon tamponade group (66% vs. 20%; P=0.025). Moreover, control of bleeding was higher (85% vs. 47%; P=0.037) and transfusional requirements (2 vs 6 PRBC; P=0.08) and SAEs lower (15% vs. 47%; P=0.077) in the esophageal stent group. TIPS was used more frequently in the tamponade group (4 vs. 10; P=0.12). There were no significant differences in 6-week survival (54% vs. 40%; P = 0.46).
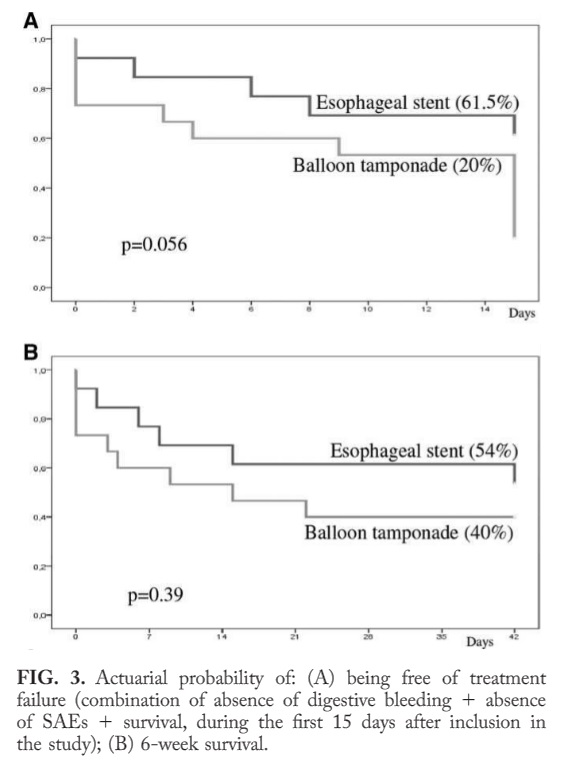
HepatologyПЁ НЧИА РлРК БдИ№РЧ ПЌБИПДСіИИ АсАњДТ РЮЛѓРћРдДЯДй. Refractory variceal bleedingРК ИХПь ЧшЧб ЛѓШВРдДЯДй. Survival graphРЧ dimensionРЬ 6СжПДНРДЯДй. 6 week survival rate!!!
ГэЙЎРЧ discussionПЁМ РЯКЮИІ ПХБщДЯДй. "These better results are owing to both a greater hemostatic effect and a lower rate of SAE, especially of aspiration pneumonia, with the use of esophageal stents. Because esophageal stents can be left safely in place for over 5 days, this procedure would be specially valuable for centers with-out facilities for early TIPS." TIPSИІ ЛЁИЎ Чв Мі РжДйИщ СяНУ TIPSИІ НУЧрЧЯДТ АЭРК ОюЖВАЁ Л§АЂЧи КИОвНРДЯДй.
* ТќАэ: EndoTODAY СЄИЦЗљ ФЁЗс (АПјМЎ БГМіДд АРЧ)
![]() 2. GIST presenting as gastroduodenal intussuscption (Eric Yasay, Philippines)
2. GIST presenting as gastroduodenal intussuscption (Eric Yasay, Philippines)
Dr. Yasay ЙпЧЅПЭ КёНСЧб СѕЗЪИІ РњГЮПЁМ УЃОвНРДЯДй (Yildiz. J Gastric Cancer 2016).
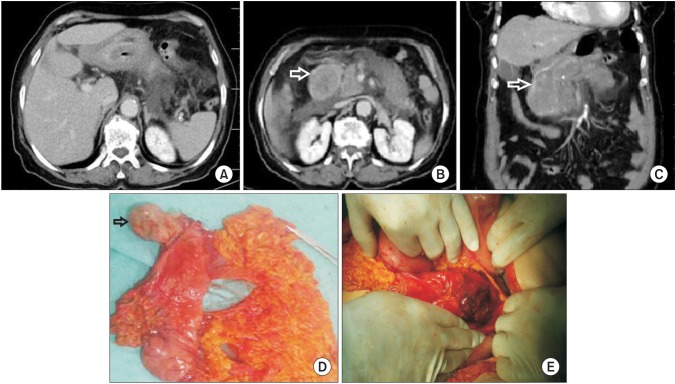 (A) Gastroduedonal intussusception. (B, C) The mass protruding to the duedonum and causing obstruction (arrows). Also visible are stranding of the peripancreatic fat and fluid accumulation around heterogenously ehancing pancreas, a sign of early necrosis. (D) Macroscopic view of the mass arising from gastric corpus (arrow). (E) Perioperative view of pancreas. Please note relatively dark portion of the pankreas corresponding to pancreatic necrosis.
(A) Gastroduedonal intussusception. (B, C) The mass protruding to the duedonum and causing obstruction (arrows). Also visible are stranding of the peripancreatic fat and fluid accumulation around heterogenously ehancing pancreas, a sign of early necrosis. (D) Macroscopic view of the mass arising from gastric corpus (arrow). (E) Perioperative view of pancreas. Please note relatively dark portion of the pankreas corresponding to pancreatic necrosis.
![]() 3. Structured enteroscopy and capsule endoscopy training workshop enhanced skills and understanding of trainees
3. Structured enteroscopy and capsule endoscopy training workshop enhanced skills and understanding of trainees
Methods: The workshop was a two day even held on June 2015. The program consisted of lectures, computer workstation for capsule endoscopy (CE), ex vivo models for single balloon enteroscopy (SBE) hands-on, and an interactive live demonstration with SBE. A twenty item multiple-choice written eam was administered before and after the lectures.
РЬЦВ ЕПОШ ПНЩШї АЁИЃУЦДѕДЯ ОіУЛ ССОЦСГДйДТ АсАњПДНРДЯДй. WebpageИІ РЬПыЧЯПЉ СіМгРћРЮ БГРАЕЕ ЧдВВ СјЧрЧЯАэ РжДйАэ ЧеДЯДй. РиОюЙіИЎСі ИЛЖѓАэ...
![]() 4. A single center audit of sphincter of Oddi dysfunction managed by ERCP under propofol deep sedation. Shqan Karim (New Zealand)
4. A single center audit of sphincter of Oddi dysfunction managed by ERCP under propofol deep sedation. Shqan Karim (New Zealand)
Conclusion: SOD remains a challenging condition to treat needing recurrent procedures. High risk of management with ERCP, however our data shows low risk of pancreatitis in setting of well selected patients treated under propofol sedation by a skilled endoscopist.
ДКСњЗЃЕхПЁМ propofolРК ИЖУыАњ РЧЛчИИ ХѕПЉЧв Мі РжДйАэ ЧеДЯДй. ЙАЗа ЛѓДчЧб КёПыРЬ ЙпЛ§ЧбДйАэ ЧЯГзПф. РЯЙнРћРЮ ЛѓКЮГЛНУАцРЬГЊ ДыРхГЛНУАцРК midazolam sedationИИ ЛчПыЧЯАэ РжДйАэ ЧЯДЯ ПьИЎЕЕ ТќАэЧв ЧЪПфАЁ РжАкНРДЯДй. PropofolРК ИХПь ЙЋУД ДыДмШї ОіУЛ ГюЖіИИХ ЙЋМПю ОрРЬДЯБюПф.
* ТќАэ: EndoTODAY ГЛНУАц СјСЄ
![]() 5. Building a mentorship: Being a good mentor / Finding a good mentor. (William R. Brugge, Harvard Medical School, USA)
5. Building a mentorship: Being a good mentor / Finding a good mentor. (William R. Brugge, Harvard Medical School, USA)
Don't put blinders on. Keep your eyes open
Indentify important questions. Focus on field. Write proposals. Build a mentorship. Write manuscript. Give talks and seminars. Teach
Learn early: statistics, size calculation, data testing
Don't search for answers; create answers
Consider global health issues. Big questions.
Think about the most important questions that are unanswered in the field.
Find a question or a problem that excites or drives you.
Don't be afraid. Get out of the silo of your own community and field.
Stay up to date on journal reading.
Prioritize. Plan ahead!! Do NOT tackle everything at once.
![]() [ТќАэ РкЗс]
[ТќАэ РкЗс]
1) ГЛНУАцЧаШИ ЧаМњЧрЛч on-line СпАш
© РЯПјГЛНУАцБГНЧ ЙйИЅГЛНУАцПЌБИМв РЬСиЧр