EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [2020 KINGCA] - End of document
[2020 KINGCA] - End of document
Covid-19 pandemic 관련하여 방역 지침을 지키면서 학회가 진행되었습니다.
![]() Day 1
Day 1
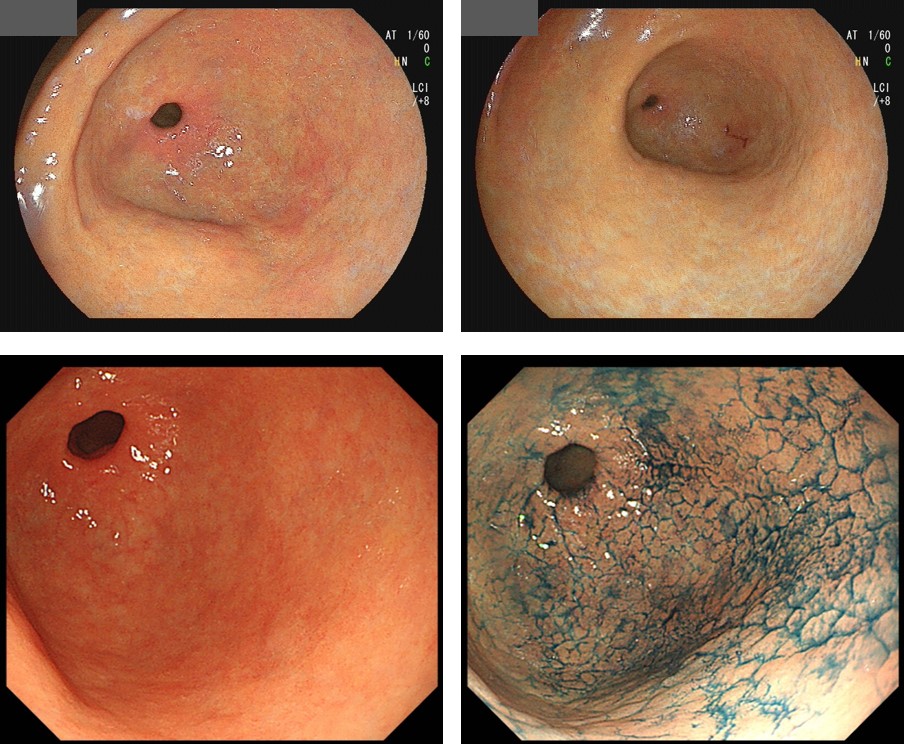
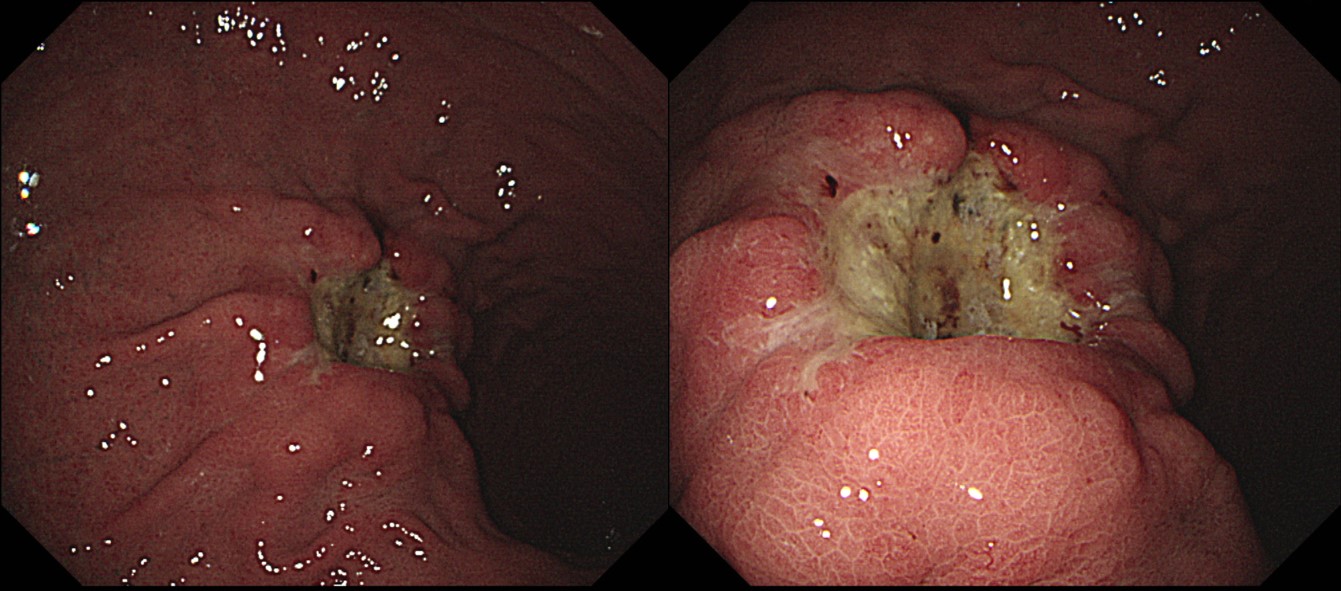
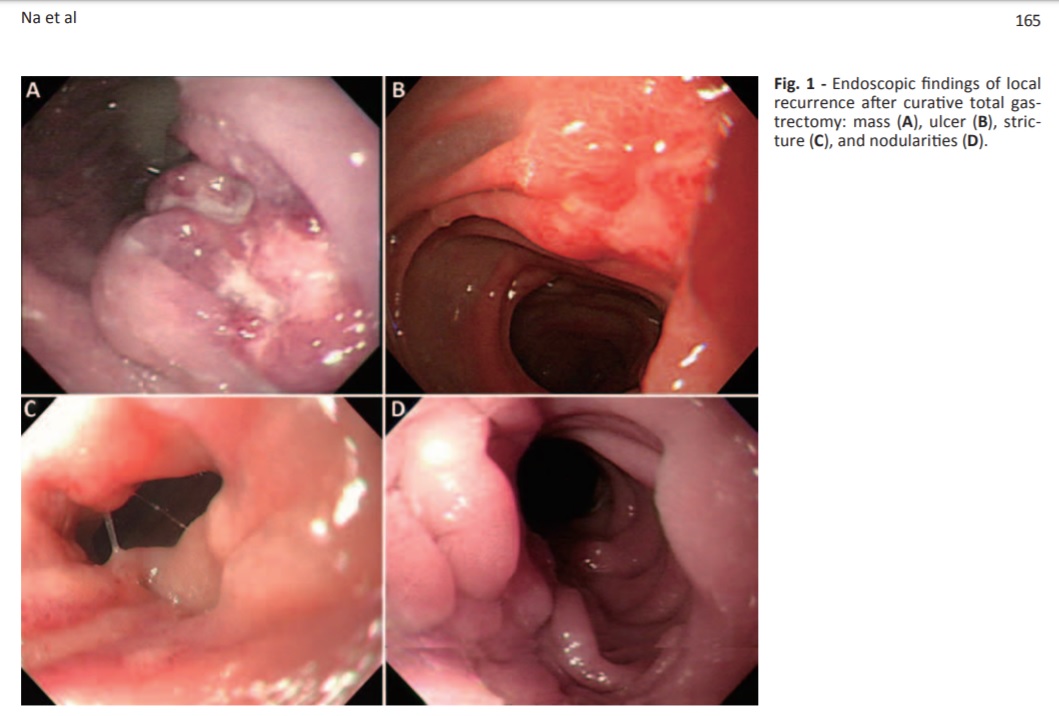
안지용 선생님은 remnant cancer 진단 tip을 소개하셨습니다.
Clinical outcomes of recurrent gastric cancer detected by upper endoscopy after curative total gastrectomy (Tumori. 2017)
Results: Of the 17 patients, 5 were resectable at the time of diagnosis of recurrence and 12 were unresectable. The median interval between total gastrectomy and diagnosis of recurrence was 20.2 months (interquartile range 12.4-42.1 months). The tumors were located in the anastomotic area in 8 patients, in the proximal part of the afferent or efferent loop in 7, and in the stump of the afferent loop in 2 patients. With regard to the endoscopic findings, a mass was found in 8 cases, an ulcer in 2, stricture in 4, and nodularities in 3. Operations were performed in 3 patients, chemotherapy in 10 (including 2 receiving adjuvant chemotherapy), and conservative management in 6. Fourteen patients died from progression of the disease and the median survival period from recurrence for all 17 patients was 5.3 months (interquartile range 1.2-7.7 months).
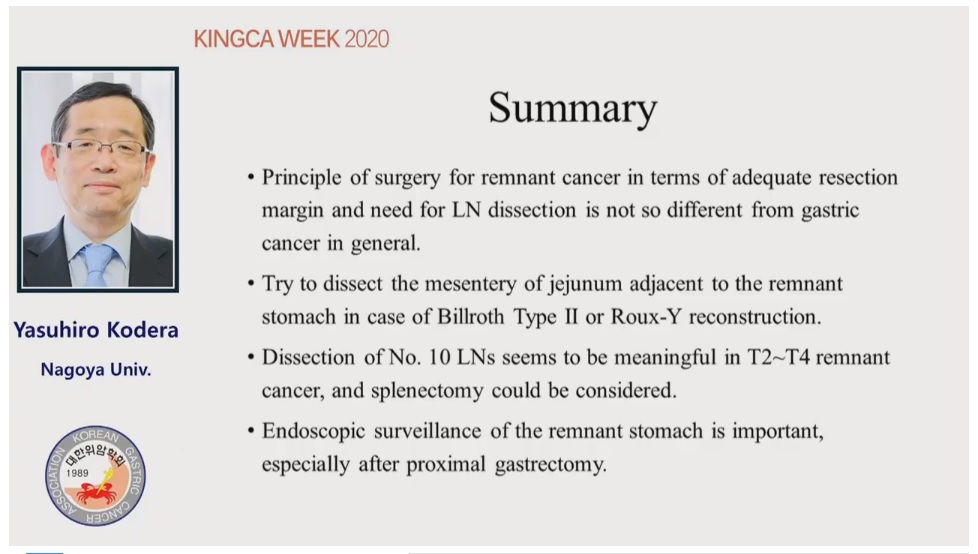
일본의 Yasuhiro Kodera 선생님께서 잔위암 수술에 대하여 말씀하셨습니다. 10번 node (splenic node)를 치료하는 것이 중요할 것 같습니다.
최일주 교수님께서 Hp treatment for gastric cancer prevention에 대한 plenary lecture를 하셨습니다. 국립암센터에서는 (1) ESD 후 위암 발생, (2) 위암 가족력 환자의 위암 발생, (3) general population에서의 위암발생을 막는데 Hp 제균치료의 효과를 분석한 연구와, (4) aspirin 사용자의 Hp 제균치료 효과를 분석한 연구를 진행하고 있다고 합니다. (1)과 (2)는 NEJM에 발표되었고 (3)은 recruitement가 끝났고 경과관찰 중이며 (4)는 현재 recruitement가 진행되고 있습니다.
우리나라 항체양성률 추이에 대해서는 Lim SH. PLos 2018 논문을 인용하셨습니다.
General population에 대한 여러 연구가 각 지역에서 진행되고 있습니다.
ESD session에서 일본 동경암센터 Abe 선생님이 보여준 자료입니다.
Digestion. 2019;99:52-58
Methods: Of 15,785 patients who underwent ESD for EGC at 19 participating institutions between January 2000 and August 2011, 1,969 failed to meet the current curative criteria after ESD. (이준행 註: 12.5%에서 noncurative resection이었습니다.) Of these, 905 patients received no additional treatment. (이준행 註: 54.0%만 수술을 받았습니다.) We evaluated the pattern of recurrence, clinical course after salvage surgery, and long-term survival rate for these patients.
Results: Over a median 64-month follow-up period, recurrence was detected in 27 patients. Two patients with missing data were excluded. Three, seven, and 15 (60%) patients showed intragastric relapse, regional lymph node metastasis, and distant metastasis, respectively. (이준행 註: 3%에서 불리한 결과가 나왔습니다.) The first line of treatment for recurrence in 1, 7, 6, and 11 patients was endoscopic treatment, salvage surgery, chemotherapy, and best supportive care, respectively. One patient survived without recurrence for 31 months after salvage surgery, one died of acute myocardial infarction 1 month after salvage surgery, and 5 showed recurrence at 0, 2, 3, 5, and 30 months after salvage surgery and eventually succumbed to the disease. The median survival times for all patients with recurrence and the 7 patients who underwent salvage surgery were 5 months after recurrence and 7 months after salvage surgery, respectively.
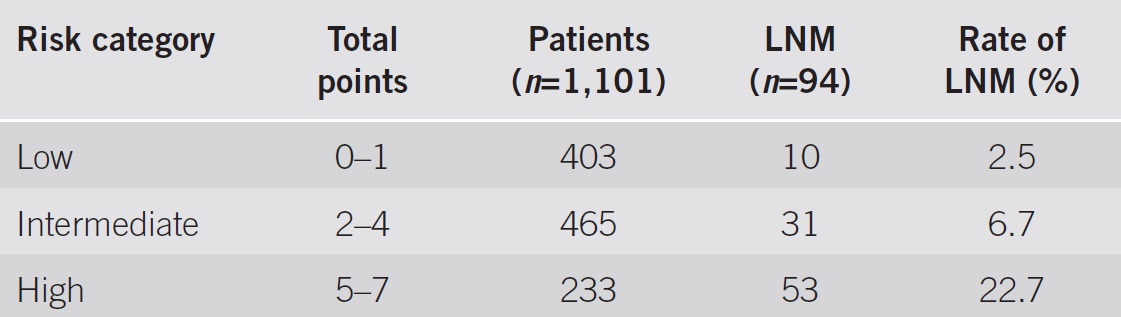
eCura system이 반복적으로 언급되었습니다.
Hatta. Am J Gastroenterol 2017
김형호 교수님 강의: Proximal gastrectomy는 남아있는 위가 50% 이상일 때 고려합니다. Peritoneum은 surgical plane으로 들어가는 gateway입니다. Mesogastrium에 대한 해부학적 개념이 D2 dissection에서 중요합니다. Dorsal mesogastrium (pancreas쪽, 9,7,8,10,11,1,2,3,4) 과 ventral mesogastrium (간쪽, 3,5,12)과 medoduodenum (6)으로 나누어집니다. 과거의 apple B 수술이 가장 완벽한 D2 dissection이지만 혈류가 너무 나빠지기 때문에 요즘은 시행하지 않는다. 그래서 dissectable layer라는 개념이 나왔습니다 (Mesogastric excision).
![]() Day 2
Day 2
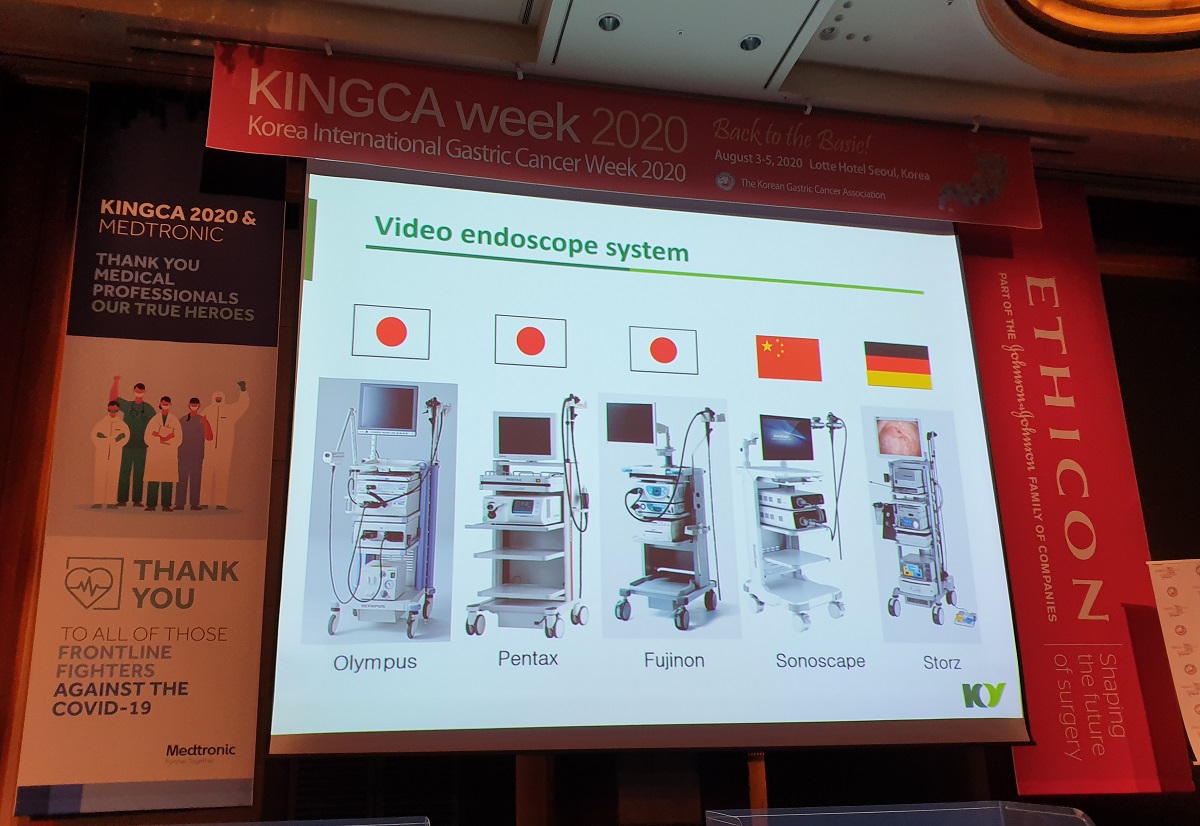
김선문 교수님께서 내시경의 구조를 설명하였습니다.
[MDT3]
64/M. signet ring cell carcinoma, IIa + IIc, 1cm (김찬규 발표)
ESD 12, Surgery 10, Hybrid approach 2
Final conclusion 1.8cm SRC SM1 lymphatic (+), LN (+, 1)
55/M SET
Carida 2.8 x 2.1
Endoscopic resection after unroofing
3.2cm 22/50 next plan
5 (Gleevec)
Patient factor and cancer factor and human factors.
Human factors include endoscopist's experience, pathologist's experience, percentage of surgery in pathologically non-curative resection cases.
Dealing with the patient is a very important factor in the discussion of ESD pathology report.
Surgeon's point of view (distal gastrectomy with D+). 외과 의사도 pretreatment diagnosed differentiated type을 명시하고 있습니다. Selection bias가 매우 크다는 점은 명백합니다.
HIRA 2017: 77% (proportion of gastric cancer in screening program)
![]() 4. Basic skills and tips for good endoscopic examination - There is a royal road to learning endoscopy. (이준행)
4. Basic skills and tips for good endoscopic examination - There is a royal road to learning endoscopy. (이준행)
사진 제공: 송교영 (서울성모병원 외과)
Thank you Mr chairman for your nice introduction. It’s a great honor for me to talk in this prestigious meeting today. I want to say that there is a royal road to learning endoscopy. It’s a simulator training.
There has been a great advancement in the fields of diagnostic and therapeutic endoscopy. However, endoscopic education for the beginners has been widely neglected. As a result, a great proportion of endoscopic examinations are performed by suboptimally educated endoscopists. The volume of endoscopic examination is huge in Korea, so the quality control of the endoscopists should have a great impact on the quality of the whole healthcare system.
Learning endoscopy is not easy. In order to become an endoscopy specialist, it usually takes two years of full-time training in a dedicated training center. However, a few months of training can be enough to learn the basic knowledge and skills for a primary clinic-level screening endoscopist. Efficient training system needs to be established.
Traditional endoscopy training means observation and do it yourself. New style endoscopy learning starts with box simulator trainings followed by description exercise.
Today, I’d like to talk about three topics.
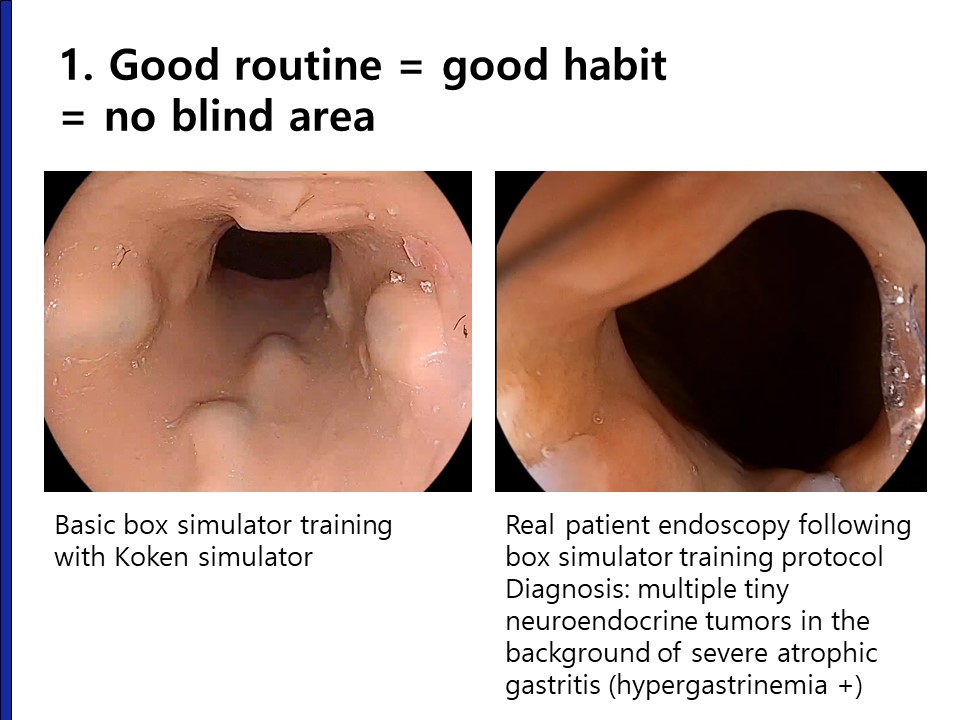
You can have a good examination routine by simulator hands-on training. What’s the meaning of a good examination routine?
It means good habit and no blind area. Left-hand side is a Koken simulator endoscopy and you can compare with the real patient endoscopy. As you can see, it is quite similar. Beginners can learn a lot of technical tips with gastroscopy simulator training.
For the box simulator training, BOXIM, we need simulators, endoscopes and training programs.
I found a box gastroscopy simulator at the Olympus booth in 2005.
I bought the simulator immediately, and started BOXIM training at my center.
What kind of simulator is the best for the beginners? Do you think the computer simulator is better? No. Box simulator is much more useful for the endoscopy beginners.
Professor Jin Hyuck Lee developed a new gastroscopy simulator using a 3D printing technology. It is more realistic than the Koken simulators, but a little bit difficult for the beginners. So, I use the Korean simulator only in the final stage of the hands-on training.
Regarding endoscopes, Olympus, Fujifilm, and Pentax are dominant players in Korean endoscopy market. All three vendors are providing state-of-the-art endoscopes. At Samsung Medical Center, we are using endoscopes from all three vendors for endoscopy training. I think every endoscopist should be familiar with all three vendors.
We are using the Olympus system at SMC clinical simulation center. We call it “the retirement home of the old endoscopes.”
We also use the Fujifilm systems at the small simulator training room in the endoscopy unit. It’s my main playground.
I am using the Pentax endoscopy system for the therapeutic endoscopy training. Pictures in the right hand side is an EndoGEL docking station that I developed with the Pentax company.
For the biopsy training, home-made simulator box and baskets are used.
Endoscopy training should be stepwise. We start with torque rotation exercise and than the simulator training and so on.
BOXIM workshops at SMC clinical simulation center are open to anyone who want to learn endoscopy. It’s not only for physicians. Surgeons, OK. Family medicine doctors, OK. Pathologists, OK. Medical students, OK. Everyone is welcome here.
During the KINGCA2019 Master Class, we had a special BOXIM training for foreign surgeons.
We also support BOXIM training at local hospitals. I performed 12 BOXIM workshops outside my hospital in the year 2019.
I have a great interest in the collaboration with surgeons. This is a symposium organized by Korean Surgical Endoscopy Study Group, KSESG. Some surgeons are also visiting my training room for the personal endoscopy training.
This is a typical program for 2-day BOXIM workshop for foreign doctors. Basic and intermediate course is 4 hours each. We also have one day program for busy Korean doctors.
In order to become a good endoscopists, you need to learn from patients. Case studies are really important.
There are three types of case studies. Off-line things are very important during the COVID-19 pandemic.
We have regular endoscopy conference every Thursday. Before COVID-19, lunch boxes are prepared. These days, we have conferences after the lunch.
On-line endoscopy conferences can be done in various platforms. I use either Zoom or YouTube. EndoTODAY on Air, EoA, is a personal YouTube live streaming lecture program. I do it at 8pm every Monday. During the live lecture, I get text questions. You can find the VOD in my YouTube channel 바른내시경연구소.
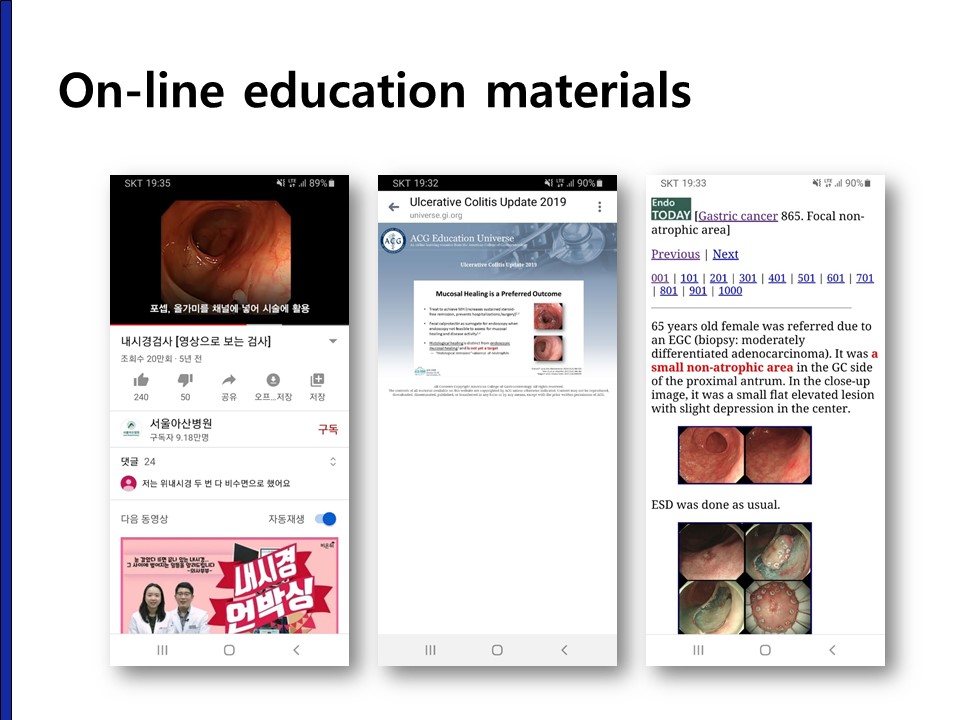
You can find a lot of education materials in the Internet. Left hand side is a YouTube patient education material from Asan Medical Center. The second is a Facebook VOD lecture from American College of Gastroenterology. Right hand side is my personal homepage EndoTODAY
Let’s briefly review an interesting case. A 58 years old lady was referred with the pathology result of poorly differentiated adenocarcinoma. At first, I think it is a surgical case, because the border of the lesion was not clear and the pathology was undifferentiated type histology.
So, repeated endoscopy was done very carefully
Unexpectedly, the outside slide review and the repeated biopsy at my institution was moderately differentiated adenocarcinoma.
I had a long patient interview and discussed the treatment options. It was an expanded indication lesion, but the patient wanted an endoscopic treatment.
ESD was done as usual.
The pathology was 22mm sized moderately differentiated type cancer limited in the lamina propria. The conclusion was curative resection.
Final topic is the examination time.
Minimum examination time should be 5 minutes.
This is an AGC.
It was not found in the previous endoscopy 39 days ago.
When I reviewed the pictures, I found that air inflation was not enough and GC side of the fundus was not examined.
And the examination time was very short.
It is clear that longer observation time is the most import quality indicator. The minimum is 5 minutes. Please do it slowly. Slow endoscopy means good endoscopy.
Ladies and gentleman, I’d like to conclude my discussion by showing this webpage. You can find information about box simulator training here.
I hope you stay trained. Thank you for your attention.
![]() [References]
[References]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.