EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [無答토론 - 다양한 위질환 011. Cascade stomach]
[無答토론 - 다양한 위질환 011. Cascade stomach]
[2019-1-11. 애독자 질문]
식도에서 위로 진입하면 화면의 좌측 fundus와 화면의 우측 high body 사이에 주로 대만에서 후벽쪽으로 긴 fold (혹은 ridge)가 보이는 환자가 있습니다.
공기를 조금 빼면 거의 사라지는 분도 있고 계속 보이는 분도 있는데요, 임상적 의의가 있는지 궁금합니다.
[2019-1-11. 이준행 답변]
종종 보는 소견이지만 임상적 의미는 없다고 생각합니다.
간혹 일본 논문에서는 cascade stomach이라고 하여 과거 barium study에서 언급하였던 category의 내시경 소견이라고 주장되는 것 같습니다 (Kusano M. J Gastroenterol 2016).
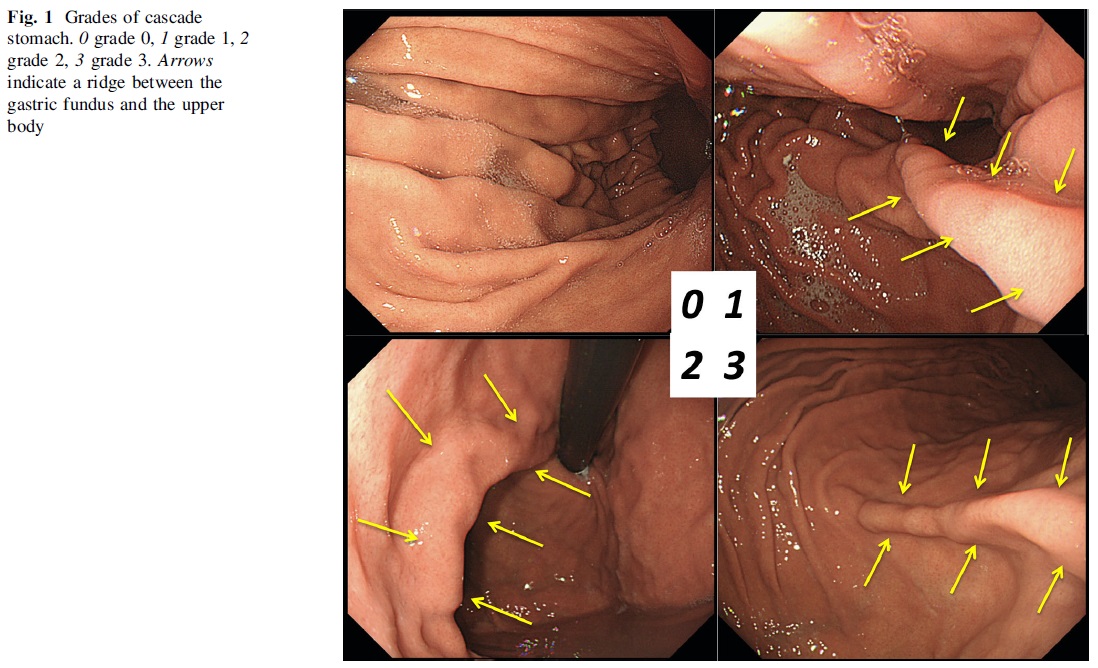
In cascade stomach (CS), the fundus of the stomach is folded backward, so detection of a ridge between the gastric fundus and upper body can be used to make a diagnosis of CS. The ridge runs from the posterior wall of the cardia toward the anterior wall of the stomach, crossing the greater curvature. It is easily observed by endoscopy when viewing from the cardia, especially when the stomach is empty and contains only a small amount of air, and it becomes less prominent when the stomach is distended by air inflation. We hypothesized that disappearance/persistence of the ridge after inflation of the stomach was related to the extent of CS. Therefore, we classified CS into four grades based on the increments of gastric inflation during endoscopic examination. Grade 0 is no detection of a ridge when viewing from the cardia at first insertion of the endoscope into the stomach. Grade 1 means that a ridge running between the fundus and upper body is observed from the cardia at first insertion of the endoscope. Grade 2 means that the ridge is also seen by retroflexed observation (J turn) of the posterior wall of the upper body of the stomach. Grade 3 means that the ridge is still detected at the end of observation after full inflation of the stomach with air.
같은 저자(Kusano)는 내시경 소견을 보고하기 몇 년 전 barium study 소견에서 보이는 cascade stomach과 증상과의 관련성을 보고한 바 있습니다 (Kusano M. NM 2012) 일본 사람들이 생각하는 cascade stomach의 개념이 잘 나타나 있어서 조금 길게 인용합니다.
Cascade stomach (CS) is diagnosed from the characteristic appearance of the stomach on barium studies. Cascade stomach was once called ‘cup and spill’, and is generally regarded as a variant of the normal stomach. In persons with CS, swallowed barium initially pools in the retroflexed gastric fundus and fills it, after which barium ‘cascades’ into the body of the stomach.
Barium study in the right anterior oblique standing view. Left: Finding that indicates a diagnosis of cascade stomach. Right: Normal stomach.
The mechanisms underlying CS include (i) extragastric compression by other viscera (especially the transverse colon, which is known as splenic flexure syndrome), (ii) swallowing of air (aerophagia), (iii) congenital CS, (iv) peptic or malignant ulcer in the upper body of the stomach, (v) perigastric adhesions, and (vi) carcinoma of the pancreas or retroperitoneal tumors.
The 2nd edition of Bockus Gastroenterology states: ‘cascade stomach, although comparatively rare, is often associated with dyspeptic symptoms. The deformity per se seldom causes symptoms but predisposes toward gastric distress if for any reason functional gastrospasm, aerophagia, or colonic dysfunction should occur’. However, this mention of CS was deleted from the next edition and it has been almost forgotten as a potential cause of dyspeptic symptoms. After endoscopy became popular, the use of radiographic examination declined. Most physicians and researchers have concentrated on endoscopic procedures because these can detect and display organic lesions more precisely than radiographic studies. In Japan, radiographic examination is still used for mass screening, but is followed by endoscopy for more detailed examination of lesions such as peptic ulcer and gastric cancer. Therefore, the relation between symptoms and gastric morphology has not attracted attention in Japan for many years. In the United States and Europe, abnormalities of gastric emptying and accommodation are considered to have a role in the pathophysiology of dyspepsia along with Helicobacter pylori infection, so there is no perceived need for barium studies in these countries. Accordingly, there have been few reports about the relationship between CS and upper GI symptoms over the past several decades.
With regard to functional dyspepsia (FD), it was recently reported that postprandial symptoms, especially postprandial fullness, are more severe in patients who report aggravation of their symptoms by meals. In patients with gastroesophageal reflux disease (GERD), heartburn characteristically occurs during the postprandial period. In persons with CS, ingested food, and fluid or swallowed air would initially collect in the fundus. After filling the fundus, the food/fluid would flow rapidly into the gastric body, and this process could be related to upper GI symptoms. As transient lower esophageal sphincter relaxation (TLESR) is triggered by distension of the gastric fundus to allow excretion of air by belching, gastric morphology might be related with upper GI symptoms, especially reflux symptoms. We hypothesized that CS could be a cause of upper GI symptoms, so we investigated the connection between CS and upper GI symptoms.
Classification of gastric morphology
Barium studies were performed with 165 mL of 180 w/v % barium sulfate (Kaigen Co., Tokyo, Japan) and 6 g of effervescent salts (Kaigen Co.). To prevent gastric contraction, scopolamine butylbromide (20 mg i.m.) was given to each subject, except for those >65 years of age; those with a history of heart disease, diabetes mellitus, glaucoma, or prostate disease; and those who refused it. After esophagography, the first filling view of the stomach containing the entire 165 mL of barium was used to classify the gastric morphology. Cascade stomach and gastroptosis were diagnosed by a single author (MK) who has more than 25 years of experience with reading barium X-ray films. Cascade stomach was diagnosed in the right-anterior standing position by detecting retention of barium in the fundus and an air-fluid level. Gastroptosis was defined as existing if the lesser curvature of the angle was located below a horizontal line connecting the bilateral iliac spines in the frontal standing position. Subsequently, seven series of X-ray films were taken with the double-contrast and compression techniques for diagnosis of organic diseases. All X-ray data were stored in a digital recording system (Digital Radiography DSTATION ARD-100A, Toshiba Co., Tokyo, Japan), and were displayed on a viewer (519 × 519 pixels, Toshiba) for reading.그리고 이 논문(Kusano M. NM 2012)의 결론은 아래 그림과 같이 요약되었습니다. Reflux나 dyspepsia가 있는 사람에서 cascade stomach이 많다는 것입니다. 거의 믿거나 말거나 수준의 논문인데요......
KEY RESULTS: BMI was significantly higher in men with CS than in controls, and also in women with CS than in controls. Upper GI symptoms were significantly more frequent in the CS group than the controls among both men and women, especially reflux symptoms. In men, logistic regression analysis identified CS as an independent risk factor for upper GI symptoms (odds ratio = 1.771, P = 0.005) and for reflux symptoms (odds ratio = 2.07, P = 0.009). In women, CS was also significantly related to upper GI symptoms (odds ratio = 2.544, P = 0.020). The prevalence of CS was significantly higher (P < 0.0001) among symptomatic men than among those with no symptoms.
CONCLUSIONS & INFERENCES: Gastric morphology is related to upper GI symptoms in both men and women. Cascade stomach should be reconsidered as a pathophysiological factor associated with upper GI symptoms.위와 장 (2017 증간호 52(5)권 563쪽)에는 瀑狀胃 (폭상위, 폭포 모양 위)라는 이름으로 아래과 같이 소개되어 있었습니다. Barium study 소견이고 내시경에 대한 언급은 없습니다.
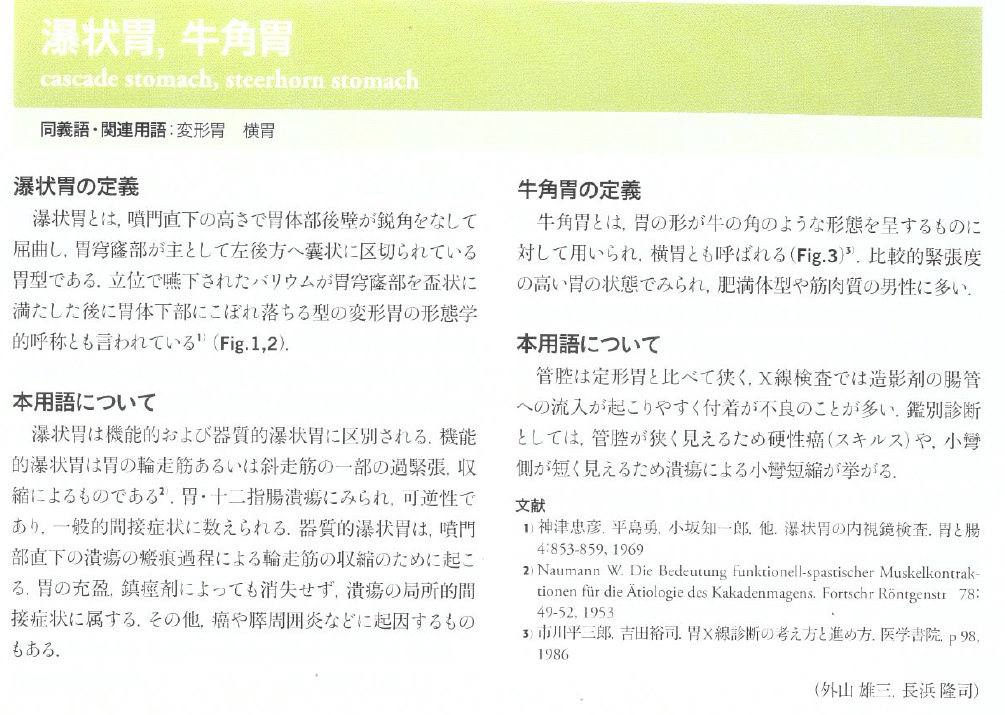
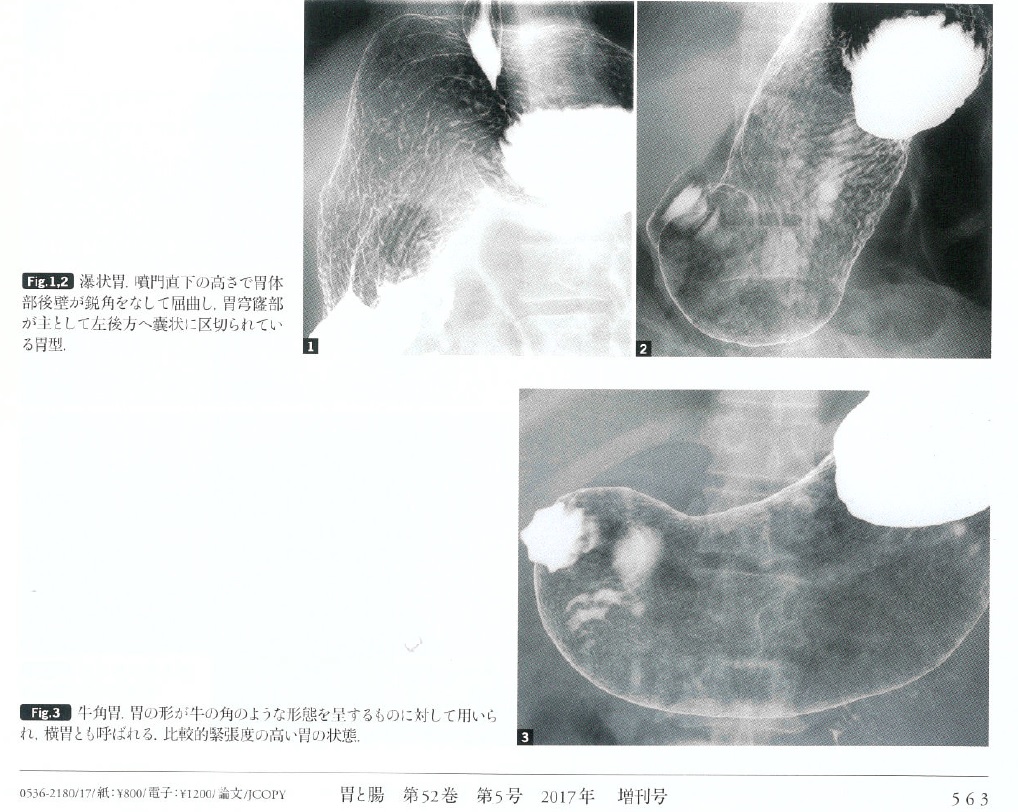
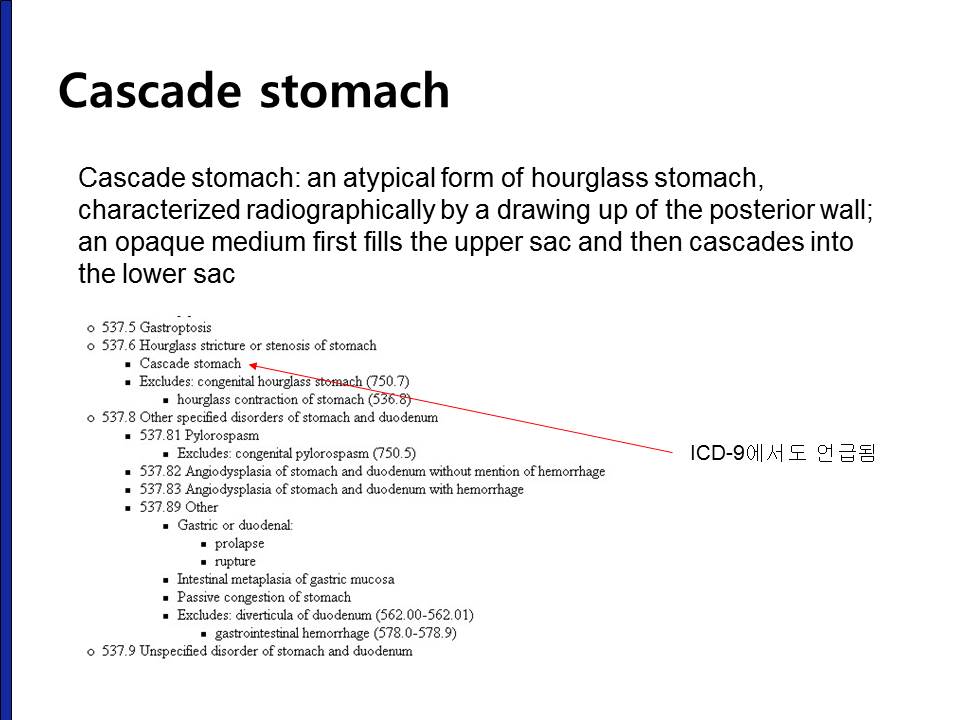
'Cascade stomach'이라는 용어는 국제질병분류에서도 언급된 적이 있고 오래된 책에서 기술된 바 있으나 실제 임상적 의의는 불명확합니다.
Cascade stomach과 약간 다르지만 barium study에서 보이는 또 다른 category로 hourglass stomach이라는 것이 있습니다. 의미는 모르겠습니다.
요컨데, cascade stomach은 barium study에서 fluid가 fundus에 유난히 많이 고이는 경우를 지칭하는 용어로서 일본에서는 가끔 임상적 의의가 있다고 주장되고 있으나 국제적으로 널리 받아들여지고 있지 않는 개념입니다. 내시경으로 위 fundus와 cardia 직하부 주름의 모양을 보고 casecase stomach을 평가하려는 시도도 있으나 너무 주관적이므로 진단명으로 사용하기 어렵다고 생각합니다. Cascade stomach처럼 소수의 내시경 의사가 연구하고 있을뿐 명확히 정립되지 않은 생소한 진단명을 내시경 impression에 적는 것은 바람직하지 않다고 생각합니다.
[어떤 증례]
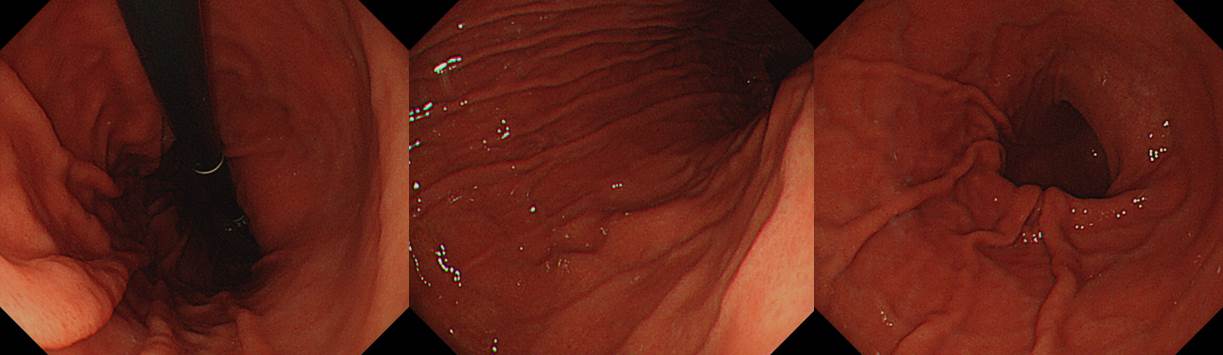
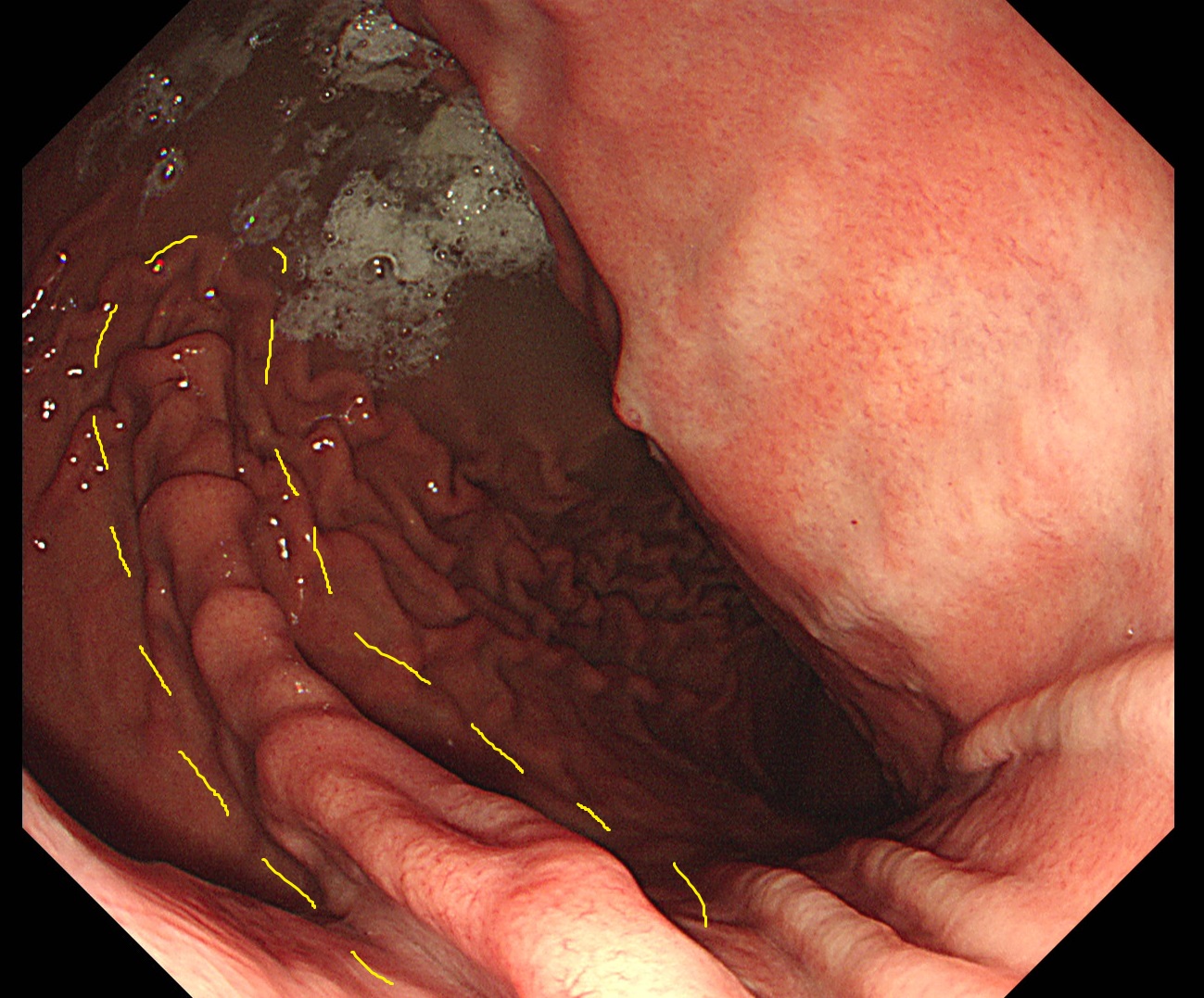
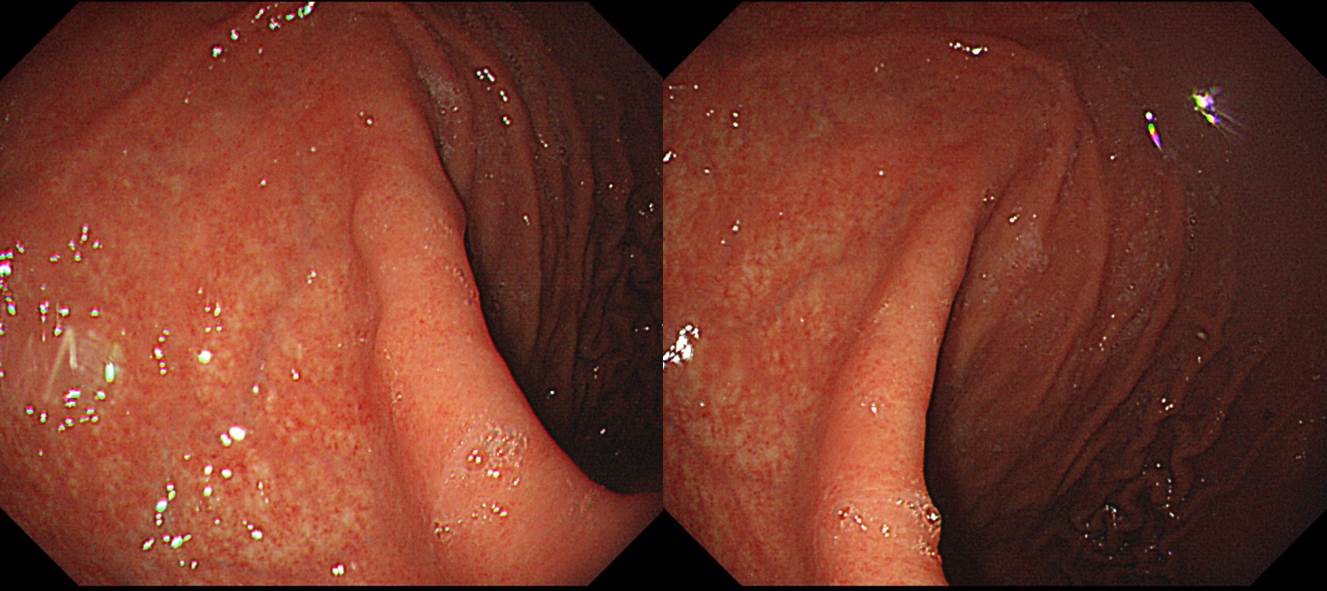
어떤 내시경 결과지에 'The upper posterior wall of the stomach was pushed forward.'라는 소견을 바탕으로 impression에 'cascade stomach'이라는 다소 생소한 용어가 적힌 것을 보았습니다.
70대 여성이셨는데 위가 다른 분에 비하여 유난히 길어 보였고 위체상부 후벽이 'pushed forward' 처럼 보여 cascade stomach이라고 쓰신 것 같습니다. 사실 내시경 사진에서 논문에 언급된 cascade stomach 사진처럼 위체상부의 ridge가 뚜렷하지도 않았습니다.
[More cases]
![]() [References]
[References]
2) EndoTODAY 위염
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (update: 2017-11-6)