 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [ColonTODAY 095 - Solitary rectal ulcer syndrome]
[ColonTODAY 095 - Solitary rectal ulcer syndrome]
![]() 1. Introduction to solitary rectal ulcer syndrome (SRUS)
1. Introduction to solitary rectal ulcer syndrome (SRUS)
Solitary rectal ulcer syndrome(SRUS)은 이상한 병입니다. 이름과 달리 solitary 하지 않은 경우도 많고 ulcer가 아닌 경우도 있습니다. 원인은 불명확한데 straining 등이 중요하고, 내시경 소견은 다양합니다. 조직검사에서 비교적 특징적인 소견이 보입니다.
최근에는 mucosal prolapse syndrome으로 이름을 바꿨다고 합니다. (2026-7-8)

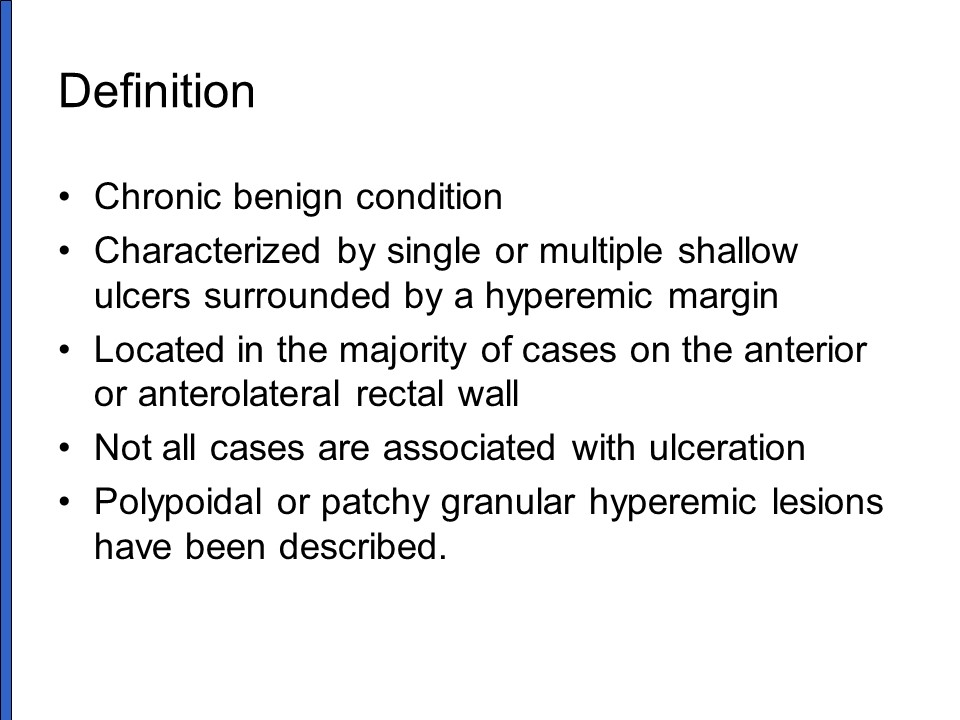
Solitary라는 이름과 달리 multiple한 경우가 25%, ulcer syndrome이라는 이름과 달리 ulcer가 아니라 protruded lesion인 경우가 25%입니다.
![]() 2. Cases of SRUS
2. Cases of SRUS
2년 전부터 straining 하는 습관이 있던 분
술 많이 드시는 당뇨환자의 혈변
Ulcer syndrome이라는 이름과 달리 융기부와 함몰부가 혼재되었던 SRUS 증례
아래는 대항병원의 최용성 선생님께서 애독자 증례 편지 19로 보내주셨던 증례입니다.
30대 여성. 배변 시 출혈을 주소로 내원. 평소 변비가 심하고 하루 30분 정도 화장실에 앉아 있음. 치핵 및 치열로 수술한 병력 (+). 변은 마려운데 안 나오고 가스가 많이 참.
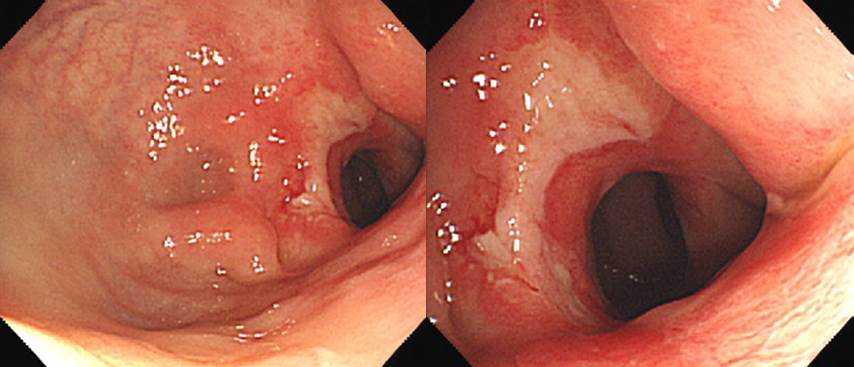

내시경 조직검사: ulcerative granulation tissue with inflammatory exudate
![]() 3. Gut and Liver 2018에 실린 멋진 리뷰(Update on the Pathophysiology and Management of Anorectal Disorders)의 SRUS 해당 부분
3. Gut and Liver 2018에 실린 멋진 리뷰(Update on the Pathophysiology and Management of Anorectal Disorders)의 SRUS 해당 부분
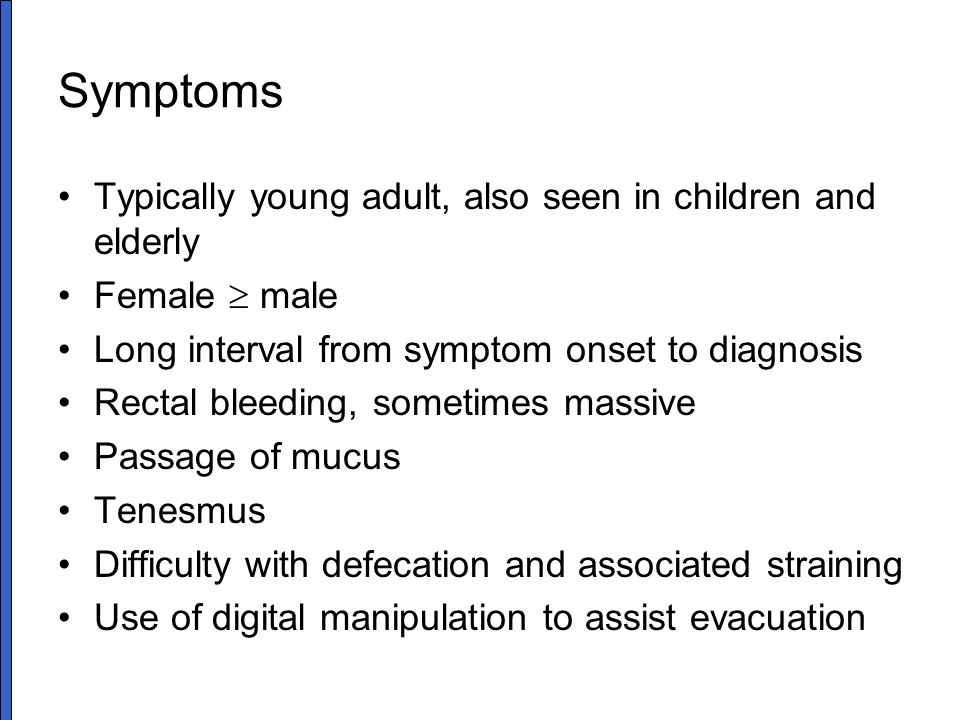
Solitary rectal ulcer syndrome (SRUS) is characterized by either erythema or ulceration in the rectum. It is not necessarily solitary or ulcerated as multiple ulcers can be found in 30% of patients. It occurs commonly in the third or fourth decade with a slightly higher prevalence in females. The most accepted pathophysiology of SRUS is either direct trauma or local ischemia to the rectal mucosa. Ulceration is thought to occur during repeated forceful straining against an immobile pelvic floor leading to mucosal prolapse and/or direct trauma from digital manipulations. This may lead to venous congestion, poor blood flow, and edema in the rectal mucosa and ischemic changes with resulting in ulceration. Patients usually present with rectal bleeding, tenesmus, mucus discharge, straining, and a feeling of incomplete evacuation. Majority use digital maneuvers but rarely admit. About 20% to 40% have diarrhea, and 25% are misdiagnosed or treated as inflammatory bowel disease. In some patients, an underlying psychologic disorder, such as obsessive compulsive disorder may be present. Anorectal manometry studies demonstrated dyssynergic defecation together with delayed balloon expulsion time in 25% to 82% of patients with SRUS. Also, SRUS patients exhibited rectal hypersensitivity, high anal pressure and paradoxical puborectalis contraction during straining.
1) Diagnosis
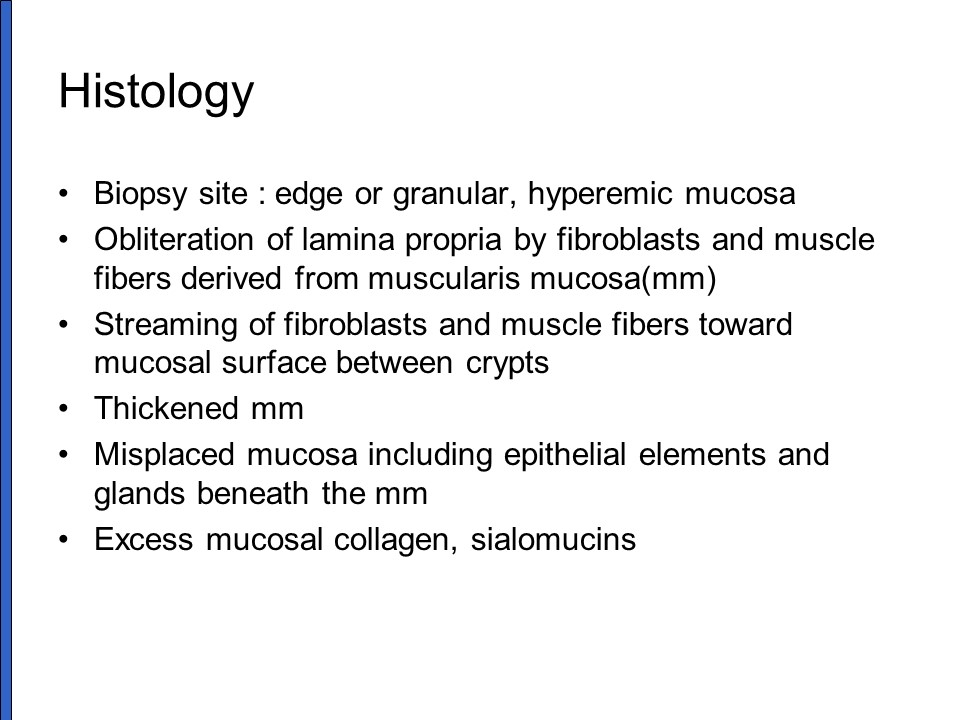
The appearances of SRUS on endoscopy may vary from hyperemic changes to established ulcers on the anterior or anterolateral wall of the rectum at about 5 to 10 cm from anal verge. Lesions are usually shallow, 1 to 1.5 cm in size, and covered by a white, grey or yellowish slough. The adjacent mucosa may appear nodular, lumpy or granular. The lesions can be multiple (30%), ulcerated (57%), polypoid (25%) or with patches of hyperemic mucosa (18%). Biopsy confirmation is important and key histological features include fibromuscular proliferation of the lamina propria, hypertrophied muscularis mucosa with extension of muscle fibers upwards between the crypts, and glandular crypt abnormalities. Presence of diffuse collagen deposition in the lamina propria is a sensitive marker for differentiating SRUS from inflammatory bowel disease. Defecography may show other abnormalities such as rectal mucosal intussusception in 45% to 80% of subjects. Endoanal ultrasonography may show marked thickening of the IAS which is highly suggestive of coexisting high grade rectal intussusception.
2) Management
Although randomized controlled trials are scarce, behavioral therapy that includes refraining from using digital maneuvers together with biofeedback therapy remain the mainstay of treatment. This treatment combination improved symptoms including straining, and bleeding in 56% to 67% of patients with significant sigmoidoscopic improvement in 30% to 55%. An increase in rectal blood flow also demonstrated after biofeedback therapy.
Topical treatments, including sucralfate, salicylate, corticosteroids, sulfasalazine, mesalazine and topical fibrin sealant, have been reported to be effective in uncontrolled studies. A recent randomized controlled study suggests that argon plasma coagulation may be useful in controlling bleeding and improving healing of ulcers better than a standard of care.
Rectopexy with or without anterior resection should be performed in highly selected cases with an advanced grade of rectal intussusception and rectal prolapse. A study of 48 patients who underwent laparoscopic ventral mesh rectopexy after biofeedback therapy reported sustained improvement in quality of life and bowel symptoms score at 2 years in the 52% who were followed up for 3 to 15 years.
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.