EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [위암학회 KINGCA 2015]
[위암학회 KINGCA 2015]
4월 2일부터 4일까지 제주에서 열린 KINGCA 위암학회에 다녀왔습니다. 이번에는 구연발표 하나, 심포지엄 강연 하나를 하였습니다. 조금 쑥스럽지만... 우수 구연상을 받았습니다.^^

중문해수욕장 새벽 산책

남도의 꽃. 동백
![]() Symposium 4. Translational research for gastric cancer
Symposium 4. Translational research for gastric cancer
서울대 양한광 교수님은 'A surgeon's role' 강의에서 collaboration의 중요성을 강조했습니다. Jackson Laboratory와 함께 개발한 마우스 아바타 모델을 소개하면서 보여주신 재미있는 그림을 소개합니다.

연세대 이용찬 교수님은 Hp에서 CagA가 주입되면 GSK를 통하여 Snail을 안정화시켜 E cadherin을 down regulation하여 EMT (epithelial mesenchymal transition)에 영향을 준다는 점을 설명하셨습니다. Nature Communication 2014에 최근 발표된 내용입니다. 축하하고 존경합니다.

성균관의대 병리과 김경미 교수님은 EBV 양성 위암의 예후가 좋은 것은 종양 주변의 염증반응이 현저하기 때문이라고 설명하면서 이에 대한 기전을 연구한 결과를 보여주셨습니다. EBV 양성 위암에서 유전자 이상은 적은 편이고 대부분 염증관련 유전자에 국한되어있다고 합니다. 최근 Gastroenterology 2015에 발표된 내용입니다. 축하합니다.

![]() Symposium 10. Endoscopic Submucosal Dissection (ESD)
Symposium 10. Endoscopic Submucosal Dissection (ESD)
일본 교린 대학의 Abe 교수는 ESD와 stomach-preserving laparoscopic lymph node dissection (therapeutic harmony)에 대하여 설명했습니다. ESD 후 24명에 대하여 ESD site 주변으로 ICG를 주사한 후 laparoscopic lymph node dissection을 했다고 합니다. 환자 당 약 20개 (3-45) node dissection을 하였고 2명에서 lymph node involvement가 있었다고 합니다. 강사는 이 방법의 제한점으로 두가지를 들었습니다. (1) determination of the reasonable and minimal dissection area, (2) potential residual of cancer cells in the gastric wall. 다만 2011년 GIE 논문 후 비슷한 시술을 거의 하지 않고 있는 것 같았습니다. 이번 강의에 추가된 환자가 3명 밖에 없었습니다.
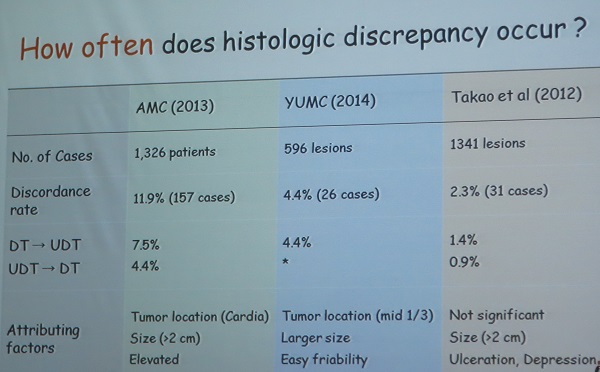
인제대 주미 주미 선생님은 histological discrepancy between endoscopic biopsy and surgical/ESD specimen을 강의하셨습니다. 수술/ESD 후 differentiate와 undifferentiated가 바뀌는 빈도는 서울아산병원 연구에서 11.9%, 연세대학교 연구에서 4.4%, 일본 Takao의 연구에서 2.3%였습니다.
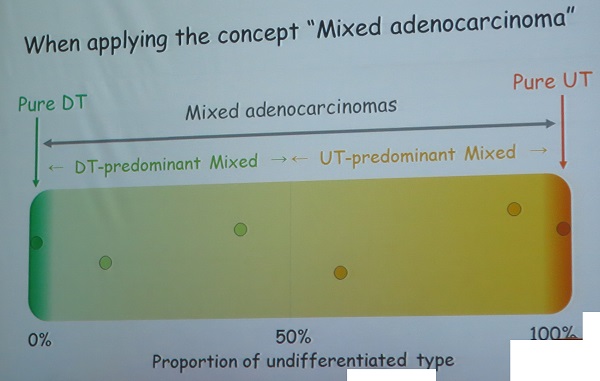
주미 선생님은 Histological heterogeneity와 mixed adenocarcinma는 다르다는 점을 지적하셨습니다. 아직 통일된 정의는 아닌 것 같지만... 그 중 mixed type의 림프절 전이가 많다는 점을 지적하셨습니다.
- Histological heterogeneity: morphologi diversity with >= 2 histologic subtypes regardless of their differentiation types
- Mixed adenocarcinoma: a mixture of differentiation type and undifferentiated type histology
(1) Mixed adenocarcinoma comprised od 10.7-44.4% of EGCs and correlated with tumor size, depth of invasion, and lymph node metastasis
(2) In particular, undifferentiated predominant mixed type is a significant risk factor for lymph node metastasis.
(3) Mixed adenocarcinoma is one of major tumor factors contributing histologic discrepancy between endoscopic biopsy and resection specimen.
Floor로부터의 질문에 대하여 삼성서울병원 병리과 김경미 선생님께서 (1) differentiated/undifferentiated 를 예측할 수 있는 면역염색이나 기타 방법은 없다, (2) histological heterogeneity는 submucosal invasion의 중요한 예측인자임을 지적하셨습니다.
![]() Symposium 11. Gastric cancer in elderly patients
Symposium 11. Gastric cancer in elderly patients
저는 screening과 ESD에 대하여 강의하였습니다. Expected survival이 10년 미만인 경우는 screening gastroscopy의 대상은 아니라는 의견을 발표했습니다. 이런 견지에서 우리나라 고령자의 expected survival 예측 모델이 필요하고, 국가암검진 프로그램의 upper age limit를 설정해야한다는 점을 언급하였습니다.
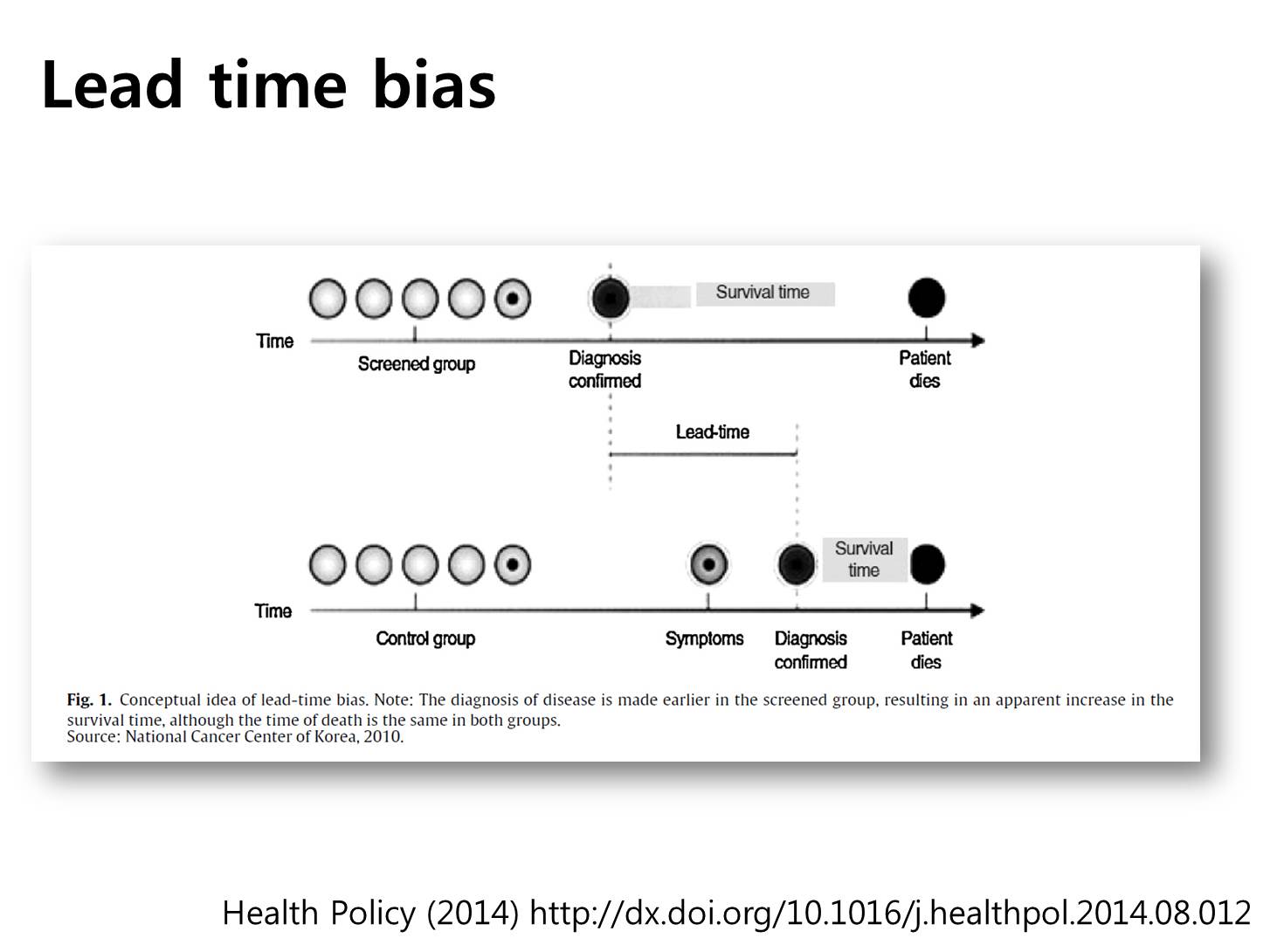
There are two important biases in the cancer screening. The first one is very famous, the lead time bias. I think all individuals in this hall already understand this type of bias. Even if we may detect cancers earlier, the overall survival gain is another issue due to the lead time bias.
The second bias is the length-time bias. It means cancers detected in the screening program may be less aggressive. This bias is especially important for the elderly population. If some cancers in the elderly people are very slow-growing, is there any reason that we need to find them?
Survival gain by the cancer screening is usually like this. At some age, the survival gain can be zero. After that point, screening can actually decrease the individual’s survival. We need to stop before that age. But, the problem here is that we don’t know exactly when to stop.
In terms of screening for cancers, we need to consider the life expectancy. Screening tests are usually recommended when the expected survival is longer than 10 years. In this regard, screening at the age of 80 is usually not recommended.
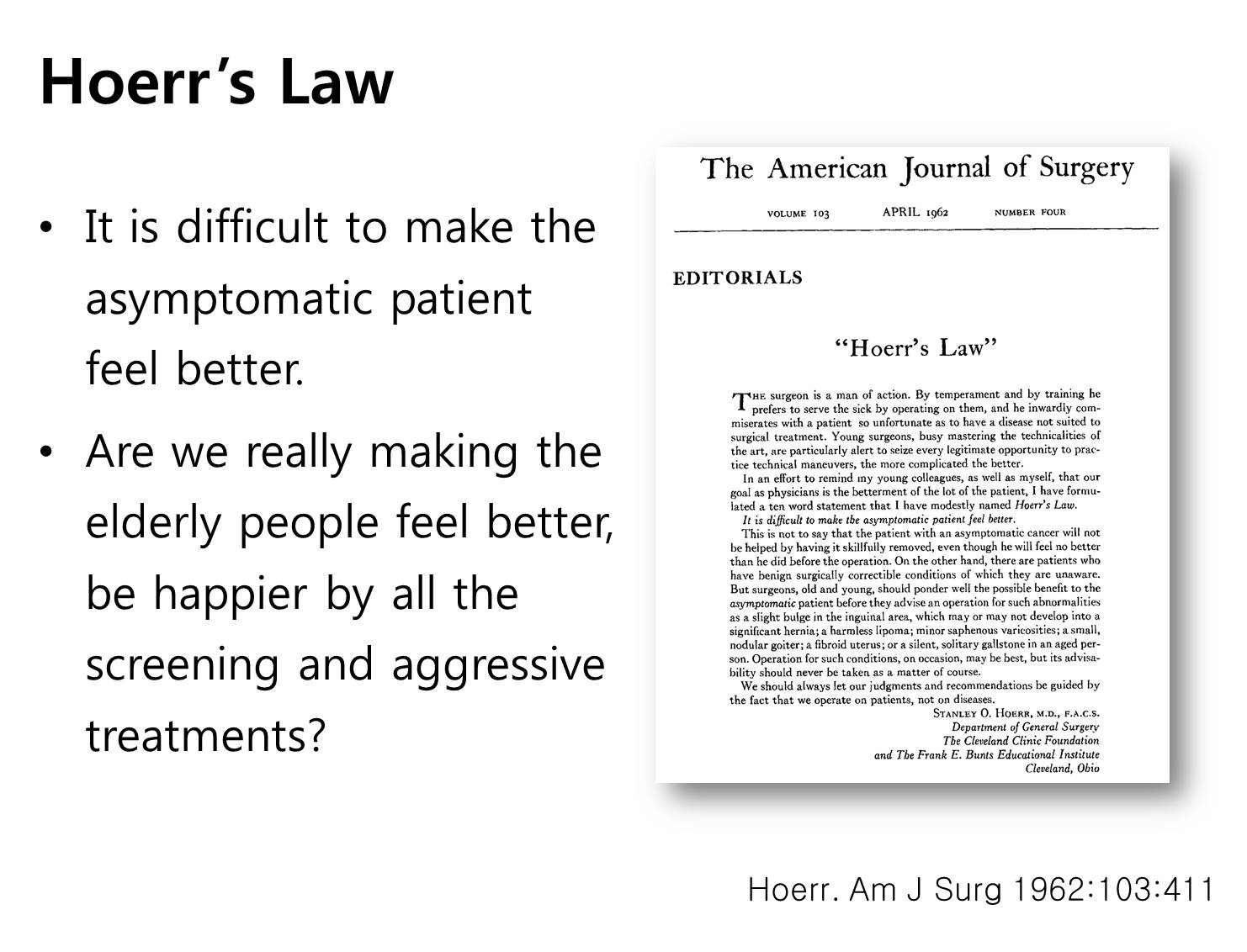
Do you know the Hoerr’s law? It means it is difficult to make the asymptomatic patient feel better. Regarding the screening in the elderly population, we need to ask to ourselves. We are really making the elderly people feel better, be happier by all the screening and aggressive treatment?
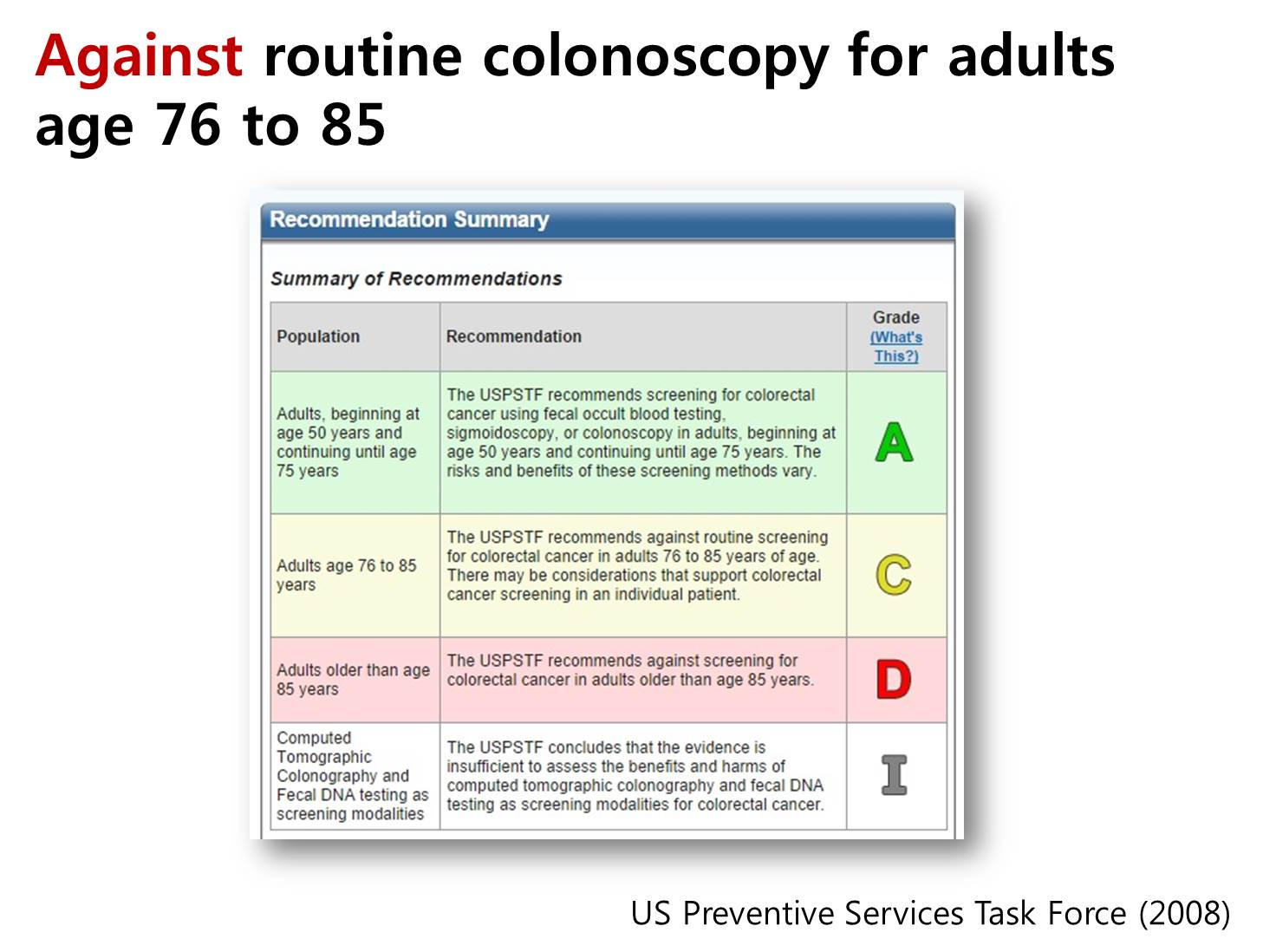
A few years ago, US preventive services task force recommended against routine colonoscopy for adults with ages 76 to 85.
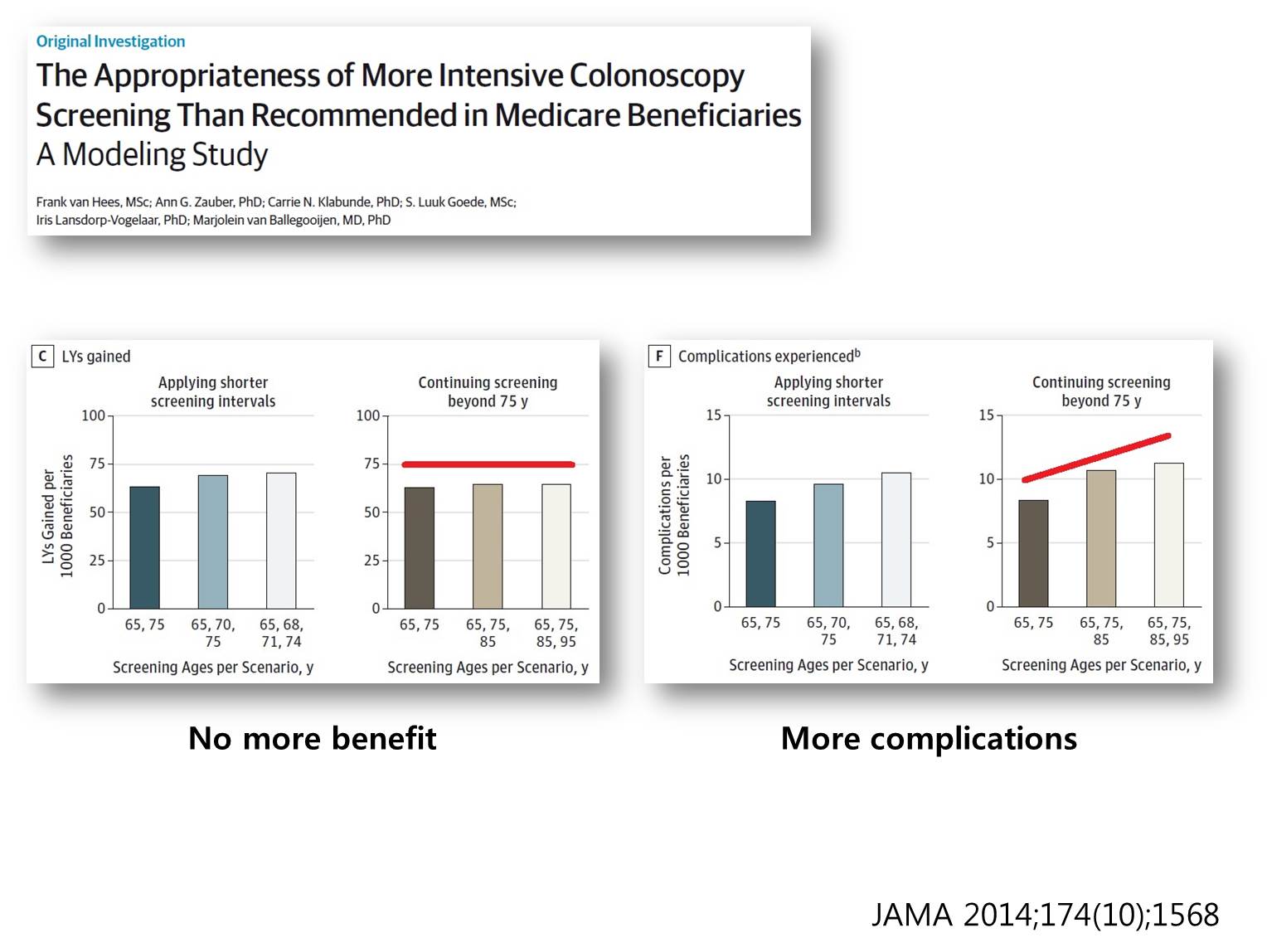
This is one of many evidences supporting the US preventive services task force recommendations. After 75 years, screening colonoscopy showed no more benefit. Actually, screening colonoscopy after 75 years makes more and more complications. 75 is a good age for stopping screening colonoscopy.
As a box summary, I can say that more is not always better, especially in the cancer screening in the elderly. Sometimes, less may be better. We need to stop at some point.
시코쿠에 위치한 Kagawa 대학의 Fujiwara 선생님은 고령 위암 수술 후 합병증 발생률 예측인자에 대하여 강의했습니다. 현재 일본 위암 수술환자의 10%가 80세 이상이라고 합니다.
경상대학교 이원섭 선생님은 고령 위암 환자의 항암치료에 대하여 설명하셨습니다. 고령환자에서는 S-1과 xelox 요법 (capecitabin + oxalipatin) 모두 효과가 약하다고 합니다. 정확히 이해하기는 어려웠으나 고령위암의 분자생물학적 특성 때문이라고 합니다. 참고자료
![]() Meet the professor session
Meet the professor session
Robotic ESD (Professor Chiu). 홍콩대학에서는 매년 gastric ESD를 20개 정도 시행하고 있고 colonic ESD는 이보다 많다고 합니다. Chiu 선생님은 외과의사인데 ESD를 하면서 countertraction이 없다는 점, 즉 one hand surgery라는 점을 가장 불편하게 느꼈던 것 같습니다. 홍콩 정부의 지원을 받아 개발하고 있는 Master라는 이름의 ESD machine에 대한 흥미로운 발표를 하셨습니다.
Laparoscopic total gastrectomy (Hirishi Okabe, Otsu Municipal Hospital). JSES 회원 병원에서 위암 치료방법에 대하여 조사한 2013 자료에서 총 26,952명 중 Open gastrectomy가 12364 (45.8%), laparoscopic gastrectomy가 9168 (34.0%), EMR/ESD가 5420 (20.1%)였습니다. 대략 distal gastrectomy의 30%, total gastrectomy의 15%가 복강경으로 치료되고 있다고 합니다. 한가지 놀랐던 것은 아래(사진 & 참고문헌 2)와 같이 일본의 위암수술 후 사망률이 우리나라보다 결코 낮지 않은 것 같다는 점입니다. 오히려 우리나라보다 사망률이 높은 느낌입니다. Distal gastrectomy의 overall mortality가 1.07%, Total gastrectomy의 overall mortality가 2.27%라고 합니다. 제 추측에 high volume center와 그렇지 않은 병원의 차이가 큰 모양입니다.
![]() Original article presentation
Original article presentation
OP01-01. 가톨릭대학교 김욱 선생님은 CLASS-01 trial의 5년 결과를 발표하였습니다. 복강경에서 개복술에 비하여 wound complication이 적었습니다. 그러나 major intraabdominal complication과 30 day martality는 비슷하였습니다. 일본 암연구회병원의 Sano 선생님은 사망사례가 4명 발생한 점에 대하여 우려하셨습니다. 비록 0.47%라는 낮은 비율이기는 하지만, distal stomach에 위치한 stage 1 위암이였다는 점을 고려해야 한다고 따끔하게 지적했습니다.
OP01-03. 국립암센터 은방울 선생님은 National Gastric Cancer Cohort Study를 소개하였습니다. 환자 뿐만 아니라 caregiver의 삶의 질도 측정한다는 점이 특징이었습니다. Caregiver quality of life index-cancer (CQOLC)라는 35 항목의 설문지를 이용한다고 합니다. ESD 환자가 너무 적다는 점이 아쉬었습니다 (48/528 (9%) received ESD). 우리 내시경 의사들이 좀 더 분발해야겠다고 느꼈습니다.
OP01-08. 국립암센터 김영일 선생님은 수술한 점막암의 림프절 전이 위험을 분석하였습니다. Lamina propria암의 림프절 전이는 2.1% 였고 Muscularis mucosa암의 림프절 전이는 4.9% 였습니다. 저는 ESD 환자가 빠졌을 것이므로 점막암의 림프절 전이가 over-estimation된 것같다고 comment를 했습니다. 일본의 Sano 선생님은 수술한 환자에 대한 연구임에도 불구하고 ESD 적응증에 해당하는 환자가 적지 않다는 점을 지적하셨습니다.
OP05-02. 제가 삼성서울병원의 noncurative resection case를 분석한 결과를 발표하였습니다. 연세대학교 이용찬 선생님께서 disease specific survival을 보는 것이 중요한데 이 환자에서는 overall survivsl만 보았다는 것이 중요한 제한점이라고 지적하셨습니다. 타당한 comment라고 생각합니다. 고령환자에서 follow up loss가 많기 때문에 disease specific survival을 구하기 어렵다는 점을 언급하는 것으로 답변을 대신했습니다. 이 발표로 우수구연상을 받았습니다.
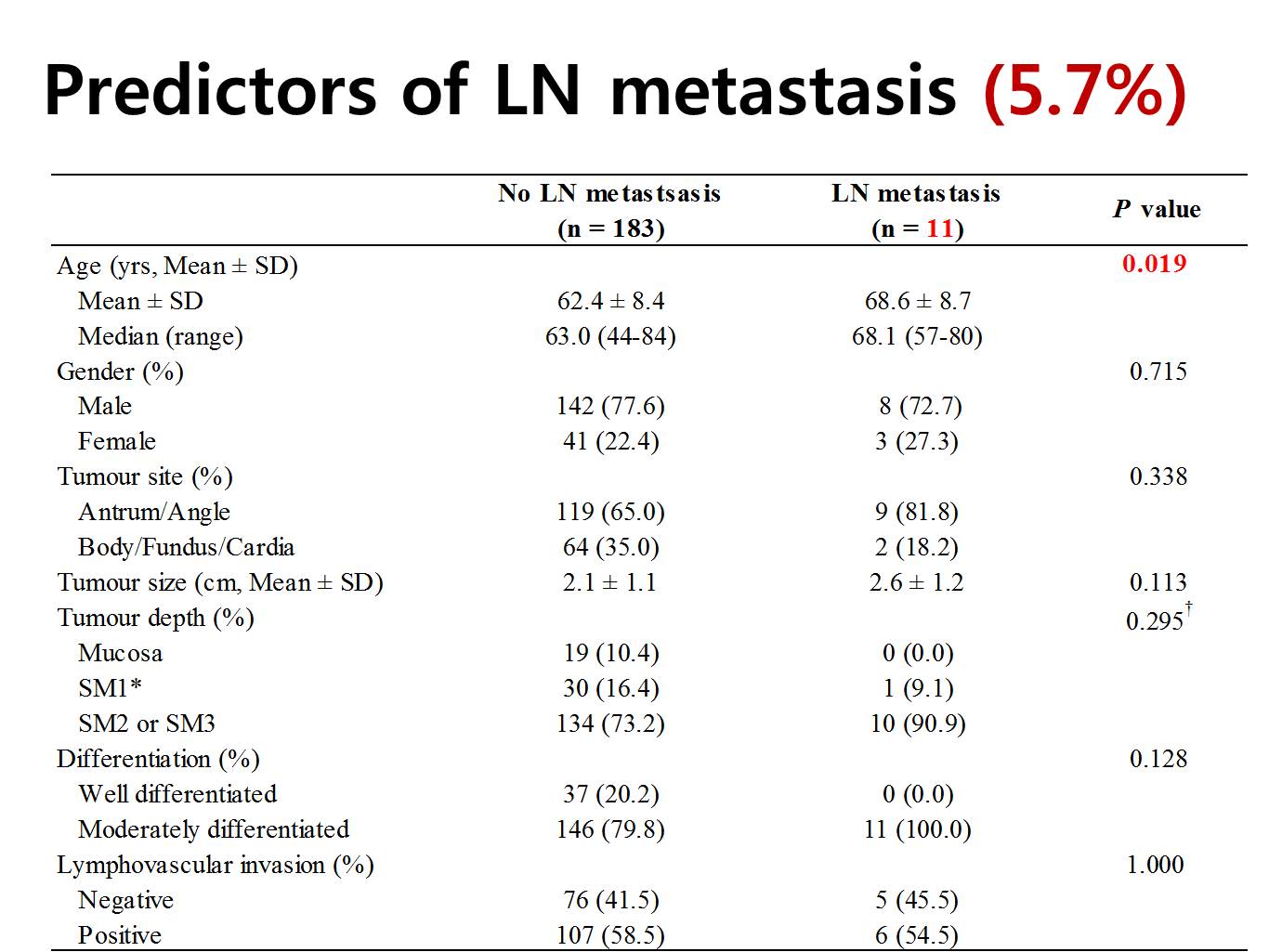
In the surgery group, 11 have lymph node metastasis, which means 5.7%. Patients with lymph node metastasis were older. To our surprise, the rate of lymph node metastasis was not different by the tumor size, depth of invasion, histological differentiation, and lymphovascular invasion in the endoscopically resected specimen. So, basically we found no predictor of lymph node metastasis in this analysis.
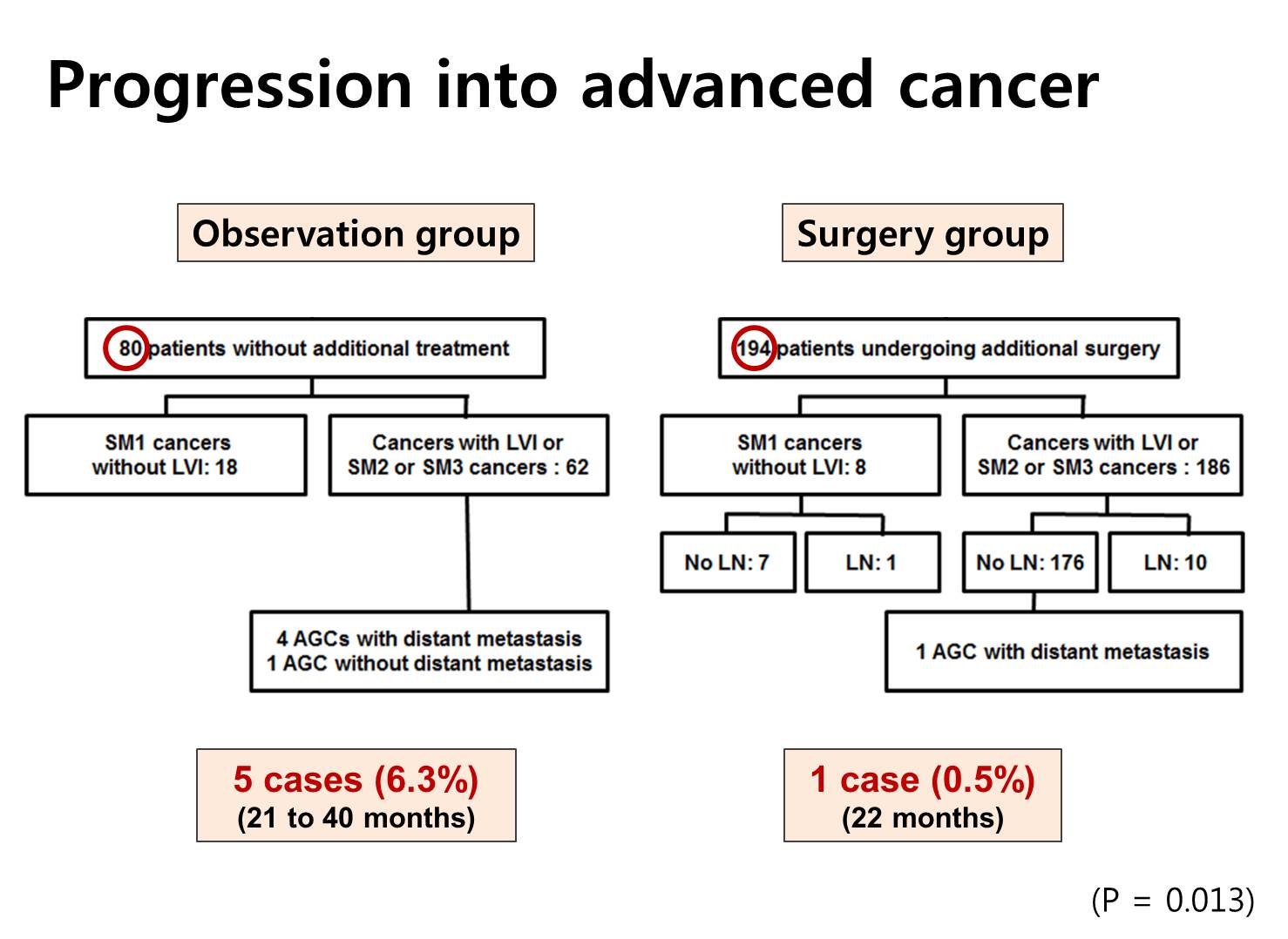
Rate of progression into the advanced cancers were different between 2 groups. Five advanced cancers were found in the observation group, and only one metastatic disease was found in the surgery group. This difference - 6.3% versus 0.5% - was statistically significant.
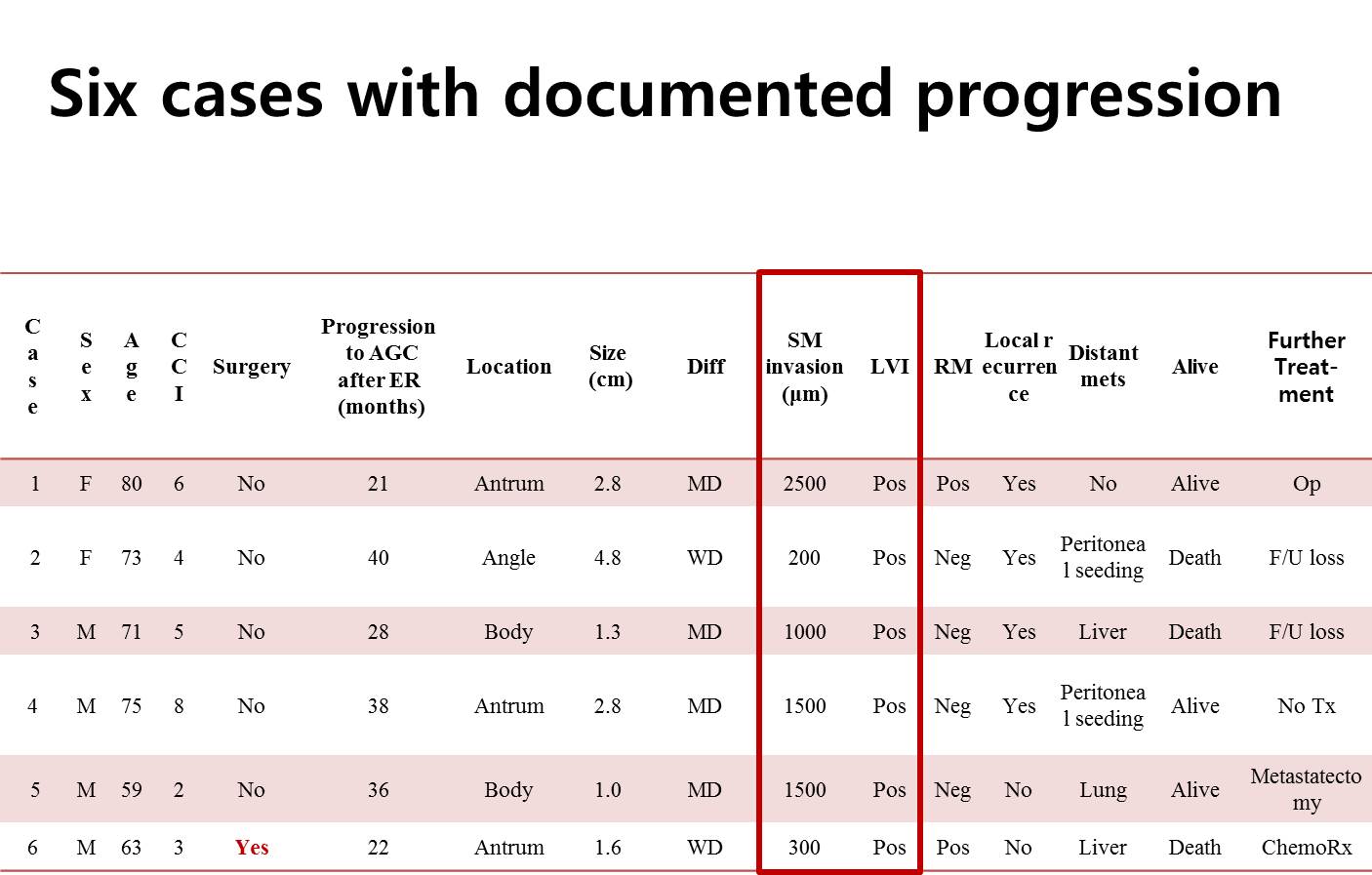
This is the summary of six cases with documented progression of gastric cancer. As you can see, all cases have submucosal invasion of more than 200 micrometer and all have evidence of endolymphatic invasion.
OP05-03. 서울아산병원 나희경 선생님은 1995년부터 2011년까지 내시경으로 치료한 margin-negative endoscopic resection 3,037명 중 국소재발을 보인 22명을 분석하였습니다. 국소재발까지의 기간은 평균 16.8개월이었습니다. 'Elevated gross morphology (both evenly and unevenly) or hyperemic change' 내시경 소견의 specifivity는 95.5%, specificity는 68.2%라는 자료를 근거로 연자는 다음과 같이 결론을 맺었습니다. Routine follow-up endoscopy shows flat mucosa without hyperemic changes at the scar especially for the en-bloc resected and differentiated EGCs.
OP05-04. 국립암센터 은방울 선생님은 ESD후 complete resection을 판정하는 submucosal invasion의 기준이 500 um가 아니라 300 um가 더 좋다는 병리분석결과를 발표하였습니다. The incidence of lymph node metastasis insubmucosal cancers meeting the expanded indication was 3.9%.
OP05-06. 연세대학교 김해원 선생님은 새로운 WHO 분류의 유용성을 분석하여 다음 결론을 냈습니다. Considering LNM and outcomes of ER, the recent WHO classification may not be helpful to perform ER for UD-EGC. 좋은 연구라고 생각되었습니다. 저는 poorly differentiated type 조기위암의 Lauren 분류에서 절반이 intestinal type, 절반이 diffuse type이라는 점이 조금 이상하다고 comment 했습니다.
OP05-08. 순천향병원 외과 정귀애 선생님은 고령 AGC 환자의 수술 성적을 발표하였습니다. 수술한 사람 중 morbidity의 차이가 없다는 것은 잘 알겠지만 수술하지 못하거나 거부한 사람은 없었는지 궁금했습니다. 저는 아래와 같은 질문을 했습니다. If you study this kind of topic in the retrospective manner, postoperative morbidity and mortality may be the same. My concern is that high risk patients may be observed without surgery by physicians in the medical department. The patient might have refused to be operated due to self image of poor health condition. What's your opinion on this possible bias?
OP05-09. 가톨릭대학의 서영주 선생님은 위암의 palliatve treatment로 복강경수술이 사용될 수 있다는 발표를 하였습니다. Bypass 39예, resection 10예, feeding jejunostomy 1예였습니다.
OP06-05 이서현 선생님은 leakage의 치료에 대한 아산병원의 경험을 멋진 영어로 발표하였습니다. Anastomosis site leak의 빈도는 0.7% (133/19207)로 매우 낮았습니다. 내시경 치료와 수술적 치료가 경과관찰군보다 좋았습니다. 내시경치료는 대부분 "clip + fibrin glue injection"가 적용되었다고 합니다.
OP06-06. 서울대병원의 손영길 선생님도 anastomosis site leak에 대하여 발표했습니다. 빈도는 2.4%였으며, 수술 후 10일에 발견되었습니다. Billoth II anastomosis에서 leakage가 많았는데, 이에 대하여 전남대 정오 선생님은 보통 Billoth II에서 더 적은 것이 상례인데 조금 이상하다고 comment하였습니다.
OP06-07. 동아대학교의 김기한 선생님은 위암 수술 후 재입원에 대하여 발표하였습니다. Subtotal gastrectomy에서는 delayed gastric emptying, wound infection가 흔한 원이었고, total gastrectomy에서는 esophajejunal stricture, intestinal obstruction이 재입원의 흔한 원인이었습니다.
![]() Poster presentation
Poster presentation
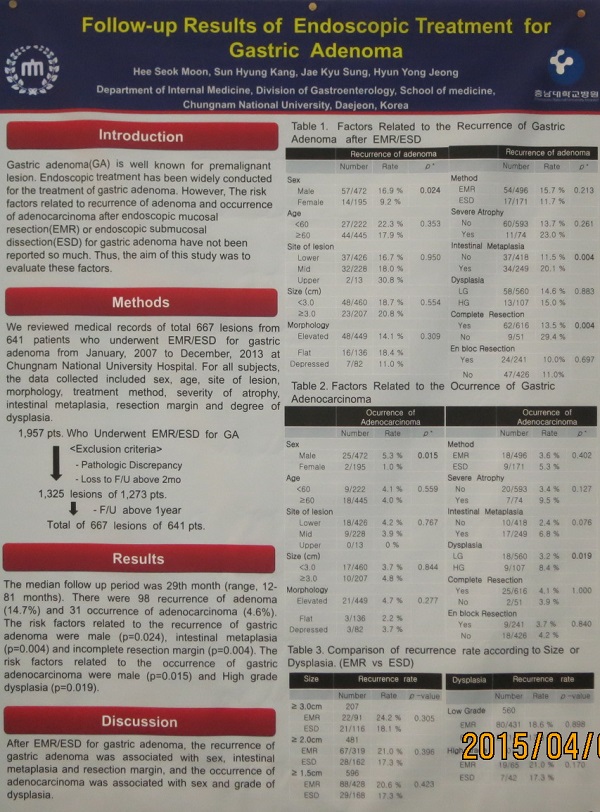
PP07-01. 충남대 문희석 선생님은 위선종 내시경 치료의 장기치료성적을 발표하였습니다. 641명을 평균 29개월간 관찰했을 때, 14.7%에서 선종이, 4.6%에서 위선암이 발생하였습니다. 조기위암 내시경 치료 후 metachronous cancer의 일반적인 발생률과 비교해도 큰 차이가 없음을 알 수 있습니다.
PP07-02. 국립암센터 최지은 선생님은 ESD specimen을 2mm 간격으로 병리검사해야하는 이유를 잘 보여주었습니다. 4mm 간격으로 관찰하면 SM invasion은 88.6-89.5%, lymphovascular invasion은 63.2-78.9%만 발견할 수 있음을 보여주었습니다. 6mm간격에서는 그 비율이 각각 75.4-84.2%, 55.3-63.2%로 더욱 떨여졌습니다. 유명한 동경암센터 연구에서 ESD의 absolute indication을 제시한 것은 2 mm cutting을 기준으로 한 것이 아니라는 좌장님의 comment가 있었습니다. Absolute indication에 따라 치료했고 병리결과도 좋은데 extragastric recurrence를 보이는 환자가 있는데, 아마도 이번 연구가 좋은 설명이 된다고 생각됩니다.
![]() [2015-4-2. 애독자 질문] EndoTODAY에 위암 환자의 내시경 사진과 함께 수술 병리 보고서를 소개해주어 도움이 됩니다. 그런데 보고서 형식이 한 가지가 아닌데 무슨 이유가 있습니까?
[2015-4-2. 애독자 질문] EndoTODAY에 위암 환자의 내시경 사진과 함께 수술 병리 보고서를 소개해주어 도움이 됩니다. 그런데 보고서 형식이 한 가지가 아닌데 무슨 이유가 있습니까?
[2015-4-2. 이준행 답변] 세 가지 이유가 있습니다. (1) 2005년 이후 위암 병리보고서 양식은 표준화되었습니다. 그 이전에는 다소 간략한 형태로 보고되었습니다. 저는 개인정보보호를 위하여 가급적 5년 보다 오래된 환자 증례를 소개하고 있습니다. 따라서 표준화 되기 전 환자가 포한되어 있어서 보고서 형식이 다양합니다. (2) 보고서 양식 표준화 이후에도 본 병원 병리과에서 몇 가지 관심있는 정보를 추가하여 보고하고 있습니다. 예를 들어 histological heterogeneity와 EBV infection status 등입니다. (3) 개인정보 보호를 위하여 간혹 일부 자료를 누락시키는 경우가 있습니다.
![]() [References]
[References]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.