 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Less is more]
[Less is more]

![]() 1. New York Times Health section 기사 스크랩
1. New York Times Health section 기사 스크랩
암에 대한 개념이 바뀌고 있습니다. 암에 걸리면 무조건 죽는 것이고, 이를 막기 위해서 조기진단이 최선이라는 생각. 너무나 당연한 상식같지만 꼭 옳은 것은 아닙니다. 암진단 후 적절히 치료하면 장기생존이 가능한 예가 얼마든지 있습니다. 조기진단을 위한 지나친 screening의 해악도 무시할 수 없습니다. 무슨 이유인지 국내에서는 잘 논의되지 않고 있습니다. 그러나 New York Times에서는 적어도 1주일에 한번 이에 대한 기사가 실립니다. 누구의 관점이 옳은 것일까? 최근 기사를 일부 모아보았습니다.
[2011-10-3. New York Times] How to Steer Toward the Path of Least Treatment (link2)-"I think we don’t talk with patients enough about the fact that there is an optimum amount of medical care, and when you start giving too much, there’s definitely a risk that it’s going to be harmful" -- 논문 link
[2011-10-7. New York Times] Panel's advice on prostate test sets up battle (link2) -- 미국 정부에서는 건강한 사람의 검진 목적으로 PSA 혈액검사를 하지 말라고 권하고 있다. 우리나라에서는 생각도 할 수 없는 일이다.
[주인장의 선택] [2011-10-10. New York Times] Screening is gambling (link2)
[2011-10-13. New York Times] Cancer risk from Barrett's esophagus lower than thought
[2011-10-20. New York Times] When doing nothing is the best medicine (link2)
[2011-10-25. New York Times] Mammogram’s Role as Savior Is Tested (link2) - Even with screening, the bad cancers are still bad
[2011-10-29. New York Times] Considering When It Might Be Best Not to Know About Cancer (link2)
[2011-10-31. New York Times] Small tumors can be vicious, big ones innocuous. (link2) - Steve Jobs가 수술을 늦춘 것이 꼭 나쁜 결정은 아니었을 수도 있다. 일찍 수술했더라도 상황이 달라지지 않았을 수 있다.
[2011-11-7. New York Times] Carotid artery bypass surgery의 효과에 의문
[2011-11-14. New York Times] Active surveillance for prostate cancer
[2011-12-3. New York Times] 'Cancer' or 'Weird Cells': Which Sounds Deadlier?
[2011-12-3. New York Times] Health Official Takes Parting Shot at ‘Waste’
[주인장의 선택] [2012-2-27. New York Times] If You Feel O.K., Maybe You Are O.K.
![]() 2. Overdiagnosis and Overtreatment in Cancer (JAMA 2013-7)
2. Overdiagnosis and Overtreatment in Cancer (JAMA 2013-7)
Screening이 활발한 시대의 과잉치료에 대한 문제제기입니다. 문제 해결을 위한 몇 가지 방안이 설득력있게 제시되어 있습니다. 아래는 그 중 하나입니다. Indolent disease 진단을 줄이는 방법은 무엇일까요? 바로 효과가 낮은 검사를 줄이는 것입니다. 진단한 후 고민하기 보다는 진단하지 않는 것이 더 좋은 병도 있습니다. 모르는게 약이라는 말도 있지 않습니까?
Mitigate overdiagnosis. Strategies to reduce detection of indolent disease include reducing low-yield diagnostic evaluations appropriately, reducing frequency of screening examinations, focusing screening on high-risk populations, raising thresholds for recall and biopsy, and testing the safety and efficacy of risk-based screening approaches to improve selection of patients for cancer screening. The ultimate goal is to preferentially detect consequential cancer while avoiding detection of inconsequential disease.
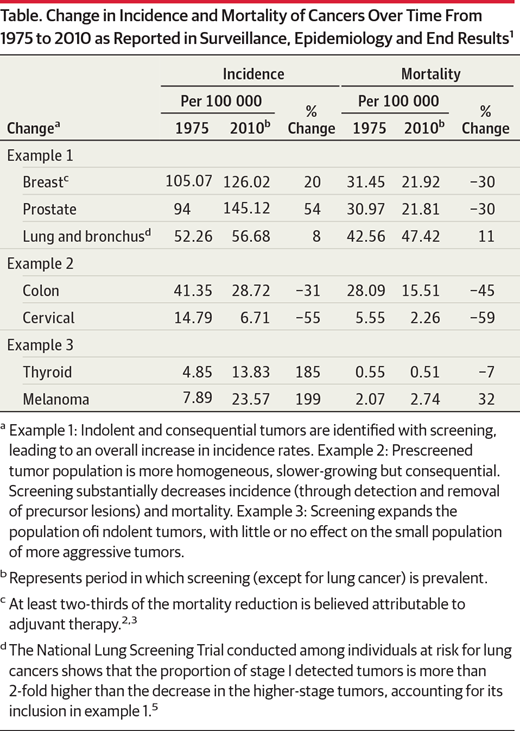
JAMA 논문에는 아래 table과 같은 흥미로운 내용도 있습니다. 모든 암이 screening을 한다고 다 좋은 결과가 오는 것은 아니라는 의미입니다. 암 진단은 많아지는데 암 사망은 줄지않는 그런 종류의 screening도 있다는 것입니다. 즉 하지 않아야 할 screening도 있다는 것입니다. 관련하여 2011년 8월 29일 EndoTODAY를 꼭 읽어보시기 바랍니다. 건강검진이 난무한 시대에 사는 의사는 확고한 철학을 가질 필요가 있습니다.
New York Times와 중앙일보 등 여러 언론에 관련 기사가 실렸습니다. 저는 90%쯤 찬성합니다. 과잉진단과 과잉치료에 넌저리가 납니다.
[2013-8-1. New York Times] Scientists Seek to Rein In Diagnoses of Cancer
A group of experts advising the nation’s premier cancer research institution has recommended changing the definition of cancer and eliminating the word from some common diagnoses as part of sweeping changes in the nation’s approach to cancer detection and treatment.
The recommendations, from a working group of the National Cancer Institute, were published on Monday in The Journal of the American Medical Association. They say, for instance, that some premalignant conditions, like one that affects the breast called ductal carcinoma in situ, which many doctors agree is not cancer, should be renamed to exclude the word carcinoma so that patients are less frightened and less likely to seek what may be unneeded and potentially harmful treatments that can include the surgical removal of the breast.
The group, which includes some of the top scientists in cancer research, also suggested that many lesions detected during breast, prostate, thyroid, lung and other cancer screenings should not be called cancer at all but should instead be reclassified as IDLE conditions, which stands for “indolent lesions of epithelial origin.”
While it is clear that some or all of the changes may not happen for years, if it all, and that some cancer experts will profoundly disagree with the group’s views, the report from such a prominent group of scientists who have the backing of the National Cancer Institute brings the discussion to a higher level and will most likely change the national conversation about cancer, its definition, its treatment and future research.
“We need a 21st-century definition of cancer instead of a 19th-century definition of cancer, which is what we’ve been using,” said Dr. Otis W. Brawley, the chief medical officer for the American Cancer Society, who was not directly involved in the report.
The impetus behind the call for change is a growing concern among doctors, scientists and patient advocates that hundreds of thousands of men and women are undergoing needless and sometimes disfiguring and harmful treatments for premalignant and cancerous lesions that are so slow growing they are unlikely to ever cause harm.
The advent of highly sensitive screening technology in recent years has increased the likelihood of finding these so-called incidentalomas ? the name given to incidental findings detected during medical scans that most likely would never cause a problem. However, once doctors and patients are aware a lesion exists, they typically feel compelled to biopsy, treat and remove it, often at great physical and psychological pain and risk to the patient. The issue is often referred to as overdiagnosis, and the resulting unnecessary procedures to which patients are subjected are called overtreatment.
Cancer researchers warned about the risk of overdiagnosis and overtreatment as a result of new recommendations from a government panel that heavy smokers be given an annual CT scan. While the policy change, announced on Monday but not yet made final, has the potential to save 20,000 lives a year, some doctors warned about the cumulative radiation risk of repeat scans as well as worries that broader use of the scans will lead to more risky and invasive medical procedures.
Officials at the National Cancer Institute say overdiagnosis is a major public health concern and a priority of the agency. “We’re still having trouble convincing people that the things that get found as a consequence of mammography and P.S.A. testing and other screening devices are not always malignancies in the classical sense that will kill you,” said Dr. Harold E. Varmus, the Nobel Prize-winning director of the National Cancer Institute. “Just as the general public is catching up to this idea, there are scientists who are catching up, too.”
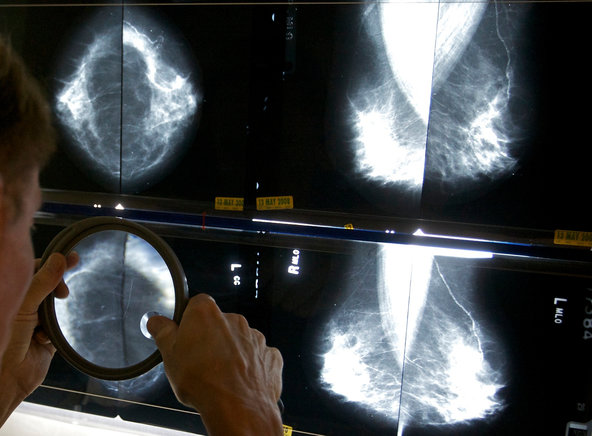
An expert panel says lesions found in some cancer screenings should not be called cancer but should instead be reclassified.
An expert panel says lesions found in some cancer screenings should not be called cancer but should instead be reclassified. One way to address the issue is to change the language used to describe lesions found through screening, said Dr. Laura J. Esserman, the lead author of the report in The Journal of the American Medical Association and the director of the Carol Franc Buck Breast Care Center at the University of California, San Francisco. In the report, Dr. Esserman and her colleagues said they would like to see a multidisciplinary panel convened to address the issue, led by pathologists, with input from surgeons, oncologists and radiologists, among others.
"Ductal carcinoma in situ is not cancer, so why are we calling it cancer?" said Dr. Esserman, who is a professor of surgery and radiology at the University of California, San Francisco.
Such proposals will not be universally embraced. Dr. Larry Norton, the medical director of the Evelyn H. Lauder Breast Center at Memorial Sloan-Kettering Cancer Center, said the larger problem is that doctors cannot tell patients with certainty which cancers will not progress and which cancers will kill them, and changing terminology does not solve that problem.
“Which cases of D.C.I.S. will turn into an aggressive cancer and which ones won’t?” he said, referring to ductal carcinoma in situ. “I wish we knew that. We don’t have very accurate ways of looking at tissue and looking at tumors under the microscope and knowing with great certainty that it is a slow-growing cancer.”
Dr. Norton, who was not part of the report, agreed that doctors do need to focus on better communication with patients about precancerous and cancerous conditions. He said he often tells patients that even though ductal carcinoma in situ may look like cancer, it will not necessarily act like cancer ? just as someone who is “dressed like a criminal” is not actually a criminal until that person breaks the law.
“The terminology is just a descriptive term, and there’s no question that has to be explained,” Dr. Norton said. “But you can’t go back and change hundreds of years of literature by suddenly changing terminology.”
But proponents of downgrading cancerous conditions with a simple name change say there is precedent for doing so. The report’s authors note that in 1998, the World Health Organization changed the name of an early-stage urinary tract tumor, removing the word “carcinoma” and calling it “papillary urothelial neoplasia of low malignant potential.” When a common Pap smear finding called “cervical intraepithelial neoplasia” was reclassified as a low-grade lesion rather than a malignancy, women were more willing to submit to observation rather than demanding treatment, Dr. Esserman said.
“Changing the language we use to diagnose various lesions is essential to give patients confidence that they don’t have to aggressively treat every finding in a scan,” she said. “The problem for the public is you hear the word cancer, and you think you will die unless you get treated. We should reserve this term, ‘cancer,’ for those things that are highly likely to cause a problem.”
The concern, however, is that since doctors do not yet have a clear way to tell the difference between benign or slow-growing tumors and aggressive diseases with many of these conditions, they treat everything as if it might become aggressive. As a result, doctors are finding and treating scores of seemingly precancerous lesions and early-stage cancers ? like ductal carcinoma in situ, a condition called Barrett’s esophagus, small thyroid tumors and early prostate cancer.
But even after years of aggressively treating those conditions, there has not been a commensurate reduction in invasive cancer, suggesting that overdiagnosis and overtreatment are occurring on a large scale.
The National Cancer Institute working group also called for a greater focus on research to identify both benign and slow-growing tumors and aggressive diseases, including the creation of patient registries to learn more about lesions that appear unlikely to become cancer.
Some of that research is already under way at the National Cancer Institute. Since becoming director of the institute three years ago, Dr. Varmus has set up a list of “provocative questions” aimed at encouraging scientists to focus on critical areas, including the issue of overdiagnosis and molecular tests to distinguish between slow-growing and aggressive tumors.
Another National Cancer Institute program, the Barrett’s Esophagus Translational Research Network, or Betrnet, is focused on changes in the esophageal lining that for years have been viewed as a precursor to esophageal cancer. Although patients with Barrett’s are regularly screened and sometimes treated by burning off the esophageal lining, data now increasingly suggest that most of the time, Barrett’s is benign and probably does not need to be treated at all. Researchers from various academic centers are now working together and pooling tissue samples to spur research that will determine when Barrett’s is most likely to become cancerous.
“Our investigators are not just looking for ways to detect cancer early, they are thinking about this question of when you find a cancer, what are the factors that might determine how aggressively it will behave,” Dr. Varmus said. “This is a long way from the thinking 20 years ago, when you found a cancer cell and felt you had a tremendous risk of dying.”
[2013-8-1. 중앙일보] 암입니다. 과잉 진단이 과잉 공포 불러
IHT는 암 분류를 바꿔야 한다는 요구 이면에는 연간 수십만 명이 불필요하고 때론 해롭기까지 한 암 진단 및 치료를 받고 있는 현실이 있다고 지적했다. 특히 생체 촬영 및 판독 기술이 발달하면서 놔둬도 암으로 발전하거나 전이를 일으키지 않을 종양까지 제거 및 치료 대상이 되는 게 문제라고 했다. 연구팀의 보고서도 지난 35년간 암 진단 건수가 크게 늘어난 데 비해 말기 암 진단 비율과 암 전이로 인한 사망률이 현격히 줄지 않았다고 지적했다. 암이라고 보기 모호한 초기 단계가 많이 진단됐다는 의미다.

국내에서도 논란의 중심에 있는 것이 갑상샘암이다. 갑상샘암은 생존율(5년 생존율 99.8%)이 높은 데다 대개 자라는 속도도 느리다. 그래서 ‘거북이 암’이라고 불린다. 그런데 이 갑상샘암 환자는 2000년 3288명에서 2010년 3만6021명으로 10배 이상으로 불어났다. 반면 같은 기간 전체 암 환자는 10만1772명에서 20만2053명으로 두 배로 늘어나는 데 그쳤다. 갑자기 한국인이 암에 잘 걸리게 된 걸까. 이에 대해 한국개발연구원(KDI) 윤희숙 연구위원은 “초음파 진단기기가 동네 의원까지 확대되면서 지나친 검사를 하기 때문”이라고 지적했다. 지난해 11월 ‘한국 1차 의료 발전방향의 모색’이란 보고서를 통해서다. 윤 연구위원은 “외국에선 증상이 없을 경우 초음파 검사를 하지 않는 게 일반적”이라며 한국의 과잉 진료 현실을 꼬집었다.
하지만 반론도 적지 않다. 전암 단계거나 생존율이 높다고 알려진 암일지라도 치명적으로 바뀔 수 있다는 이유에서다. 삼성서울병원 오영륜(병리학) 교수는 “유방상피내암을 제거하지 않고 그대로 두면 주변으로 퍼지는 침윤성암으로 바뀔 위험이 8~10배 높아진다고 알려져 있다”고 지적했다. 현실적인 어려움도 있다. 이진수 국립암센터 원장은 “갑상샘의 경우 사망률이 낮아 문제가 되는 측면이 있다”면서도 “의사가 놔두자고 해도 환자들은 가만 있지 않고 적극적인 치료를 요구한다”고 말했다. 국내에서도 암의 분류에 대한 논의를 시작해야 한다는 의견도 있다. 삼성서울병원 김선욱(내분비대사내과) 교수는 “현재 과학기술로는 잠재암과 진행암을 구별하기 어려운 것이 사실이지만 암의 분류에 대해 진지한 고민을 해야 한다는 보고서의 취지엔 동의한다”고 말했다.
![]() 3. 존엄한 기다림과 고통스러운 기다림 (호스피스)
3. 존엄한 기다림과 고통스러운 기다림 (호스피스)
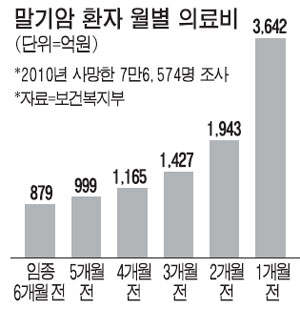
[매일경제. 2013-10-9] 말기암환자, 임종전 석달 `의료비폭탄`
[조선일보. 2013-10-10] 번호표만 뽑아주고 마냥 기다리게 하는… 말기癌 환자에게 멀고 먼 호스피스 전문
![]() 4. 기타 다양한 읽을거리
4. 기타 다양한 읽을거리
[한겨레 2012-6-5] 과잉 건강검진의 후유증, 가짜병·마음의 병·약물 남용 (link2)
[청년의사 2012-3-5] 건강검진 오남용, ‘브레이크’ 필요하다 (link2)
 "검진은 위양성과 과진단을 양산한다!" 그러나 암이라고 다 똑같은 것은 아니다. 암에는 3가지가 아니라 4가지의 놈이 있다. '빠르게 진행하는 놈', '천천히 진행하는 놈', '아주 천천히 진행하는 놈', 그리고 마지막으로 '아예 진행하지 않거나 퇴행하는 놈'이다. 조직학적인 여러 특징으로 보아 암은 분명하나, 암이 아예 진행하지 않아 그 상태로 머물러 있거나 아주 천천히 진행하여 암으로 사망하지 않고 다른 원인으로 - 예를 들어 뇌중풍으로 - 사망할 경우 '가짜병'('pseudo-disease')이라고 한다
"검진은 위양성과 과진단을 양산한다!" 그러나 암이라고 다 똑같은 것은 아니다. 암에는 3가지가 아니라 4가지의 놈이 있다. '빠르게 진행하는 놈', '천천히 진행하는 놈', '아주 천천히 진행하는 놈', 그리고 마지막으로 '아예 진행하지 않거나 퇴행하는 놈'이다. 조직학적인 여러 특징으로 보아 암은 분명하나, 암이 아예 진행하지 않아 그 상태로 머물러 있거나 아주 천천히 진행하여 암으로 사망하지 않고 다른 원인으로 - 예를 들어 뇌중풍으로 - 사망할 경우 '가짜병'('pseudo-disease')이라고 한다
[The Doctor 2012-3-9] 임종환자의 연명치료 중단과 사전의료의향서 (허대석 교수)
[한겨레 2012-3-11] 비타민제 복용할수록 독
[데일리메디 2011-10-13] 무증상 뇌동맥류' 예방적 치료 or 관망
[JAMA] Clinical inertia as a clinical safeguard
[AHQS] 20 tips to help prevent medical errors (link2) - 이런 문장이 나온다. 18번째 항목이다. "Know that "more" is not always better. It is a good idea to find out why a test or treatment is needed and how it can help you. You could be better off without it."
[The Doctor 2012-4-13] ACP·AAFP·ACC·ACNC 권고, 재고돼야 할 검사·치료, ASCO·ASN·AGA·AAAAI·ACR 권고, 재고돼야 할 검사·치료
![]() 3. Less is more는 참 다양한 의미로 쓰인다. 디자이너 김재훈이 쓴 디자인 캐리커처 (부제: 유쾌한 20세기 디자인 여행)에 less is more가 언급되어 있다.
3. Less is more는 참 다양한 의미로 쓰인다. 디자이너 김재훈이 쓴 디자인 캐리커처 (부제: 유쾌한 20세기 디자인 여행)에 less is more가 언급되어 있다.
클릭하면 그림을 크게 볼 수 있습니다.
![]() [Furor medicus]
[Furor medicus]
[2013-8-19] 근간 American Journal of Gastroenterology에 실린 Diagnostic testing in extraesophagal GERD : another case of furor medicus?라는 논평을 소개합니다. 제가 제일 싫어하는 do-somethingism에 대한 훌륭한 논평입니다. Fuor medicus는 MD consult에서는 아래와 같이 설명하고 있습니다. 애매하다고 이것 저것 검사하기보다는 한발 물러서서 천천히 생각해보자는 것입니다.
Here, the physician risks overdoing the diagnostic evaluation or instituting unneeded or harmful treatments in such patients (sometimes called furor medicus).