EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Mantle cell lymphoma]
[Mantle cell lymphoma]
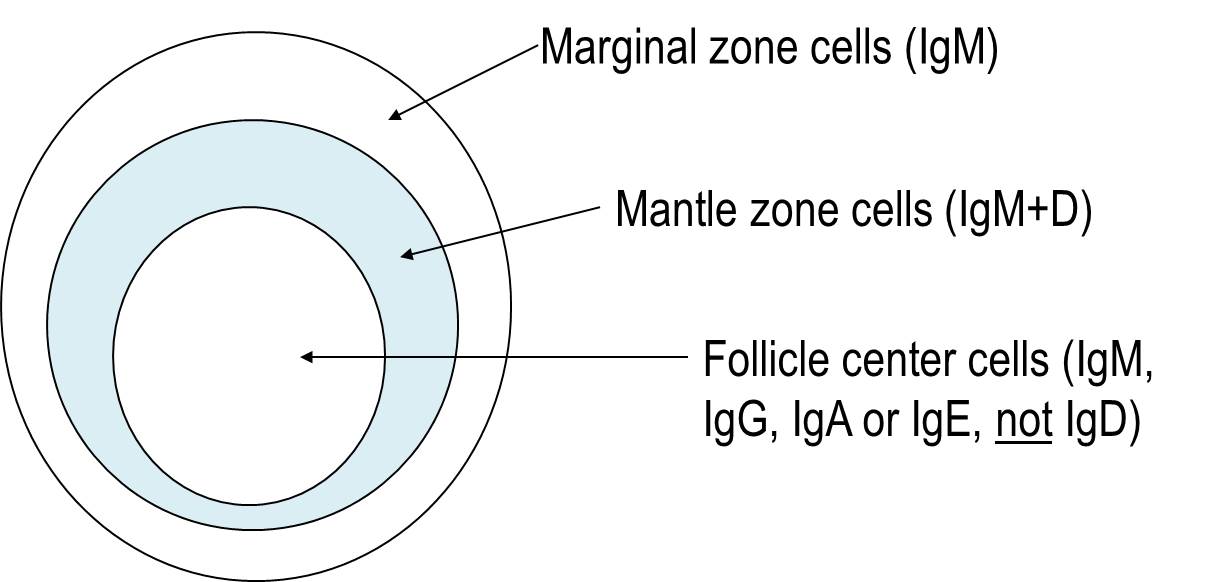
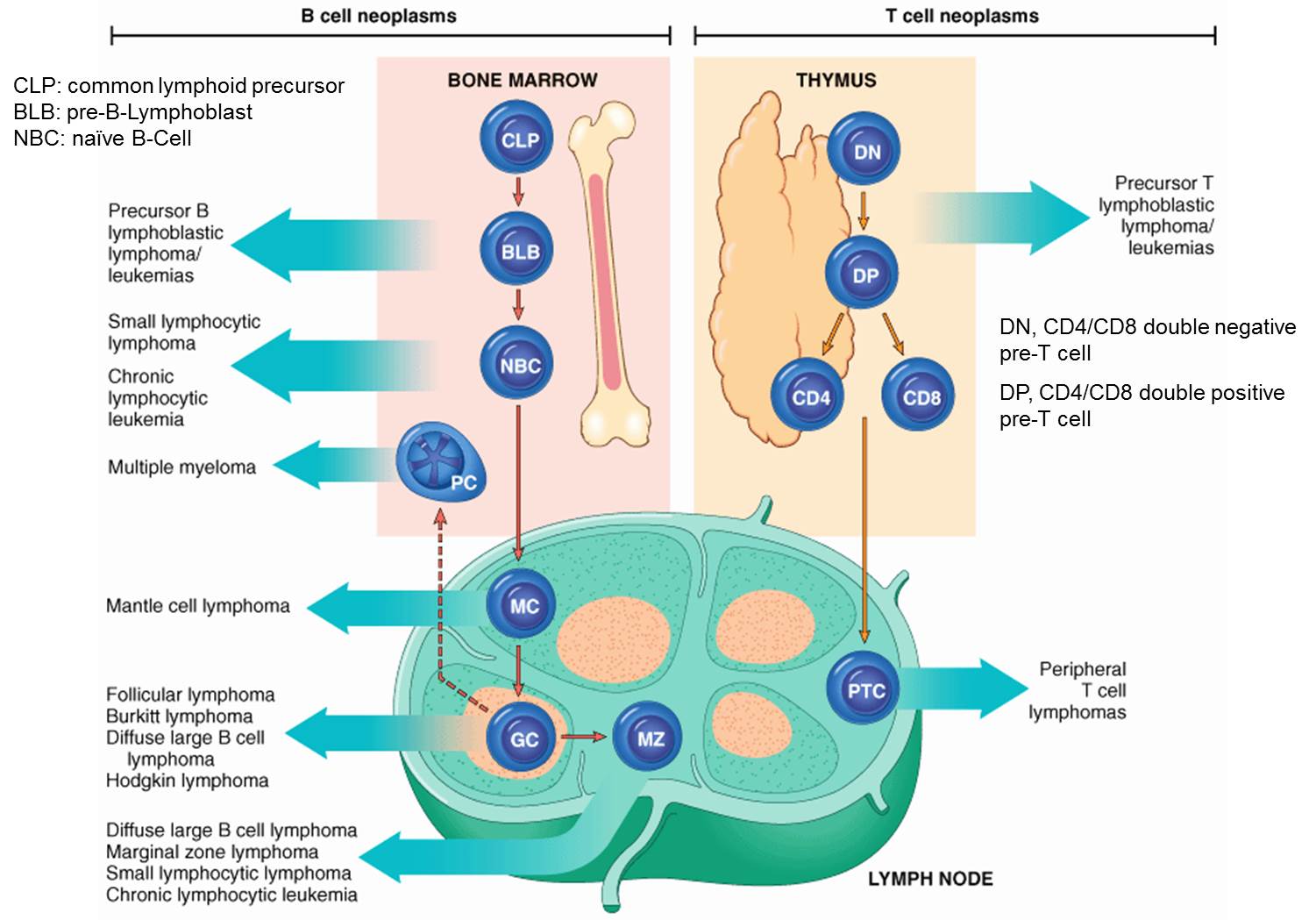
1. Mantle zone은 어디인가? Mantle cell lymphoma의 족보는?
2. Mantle cell lymphoma의 임상적 특징
3. GI involvement of nodal MCL
4. Colon involvement of MCL : lymphomatous polyposis type
5. Colon involvement of MCL : non-lymphomatous polyposis type
8. Cyclin D negative mantle cell lymphoma
9. GI mantle cell lymphoma, experiences at Samsung Medical Center
![]() 1. Mantle zone은 어디인가? Mantle cell lymphoma의 족보는?
1. Mantle zone은 어디인가? Mantle cell lymphoma의 족보는?
Small B-Cell Lymphomas - Rebecca L. King MD, Paul J. Kurtin MD, in Hematopathology (Third Edition), 2018
Mantle cell lymphoma cells express pan B-lymphocyte antigens such as CD19, CD20, CD79a, CD79b, and PAX-5. They are positive for IgM or IgM plus IgD and exhibit immunoglobulin light chain restriction. More MCL cases express lambda immunoglobulin light chain than kappa immunoglobulin light chain. Greater than 95% are positive for CD5 but negative for other T-cell antigens, such as CD3, and most either completely lack CD23 expression or show weak CD23 marking in a subset of the tumor cells. They typically lack or have low-intensity expression of CD200 and are most often LEF1-negative, both of which may aid in the distinction from CLL/SLL. They are usually also negative for CD10 and BCL6. Exceptions to this typical phenotype exist. CD5- MCL cases have been described. They can be recognized on the basis of typical morphologic features and expression of cyclin D1 and will have the classic t(11;14)(q13;q32) CCND1/IGH as described below. A very small number of MCLs is positive for the follicle center cell marker BCL6, and MCL is one of the types of B-cell lymphomas that can co-express both CD5 and CD10. As a consequence of the t(11;14)(q13;q32) (see below), the nuclei of the majority of MCLs are positive for cyclin D1, a marker demonstrated best by paraffin section immunohistochemistry. More recently, cyclinD1-negative MCLs have been described, which can pose a diagnostic challenge to the pathologist. Expression of SOX11 by immunohistochemistry is seen in a high proportion (>90%) of MCL and appears useful in recognition of cyclin D1 negative MCL. Interestingly, SOX11-negative cases seem to represent a subtype of MCL, which has a more indolent course, leukemic/non-nodal involvement, and mutated IGHV. SOX11 is not expressed in other small B-cell lymphomas or DLBCL (including CD5+ DLBCL). It can be expressed in some cases of Burkitt lymphoma and lymphoblastic lymphoma, but these entities are not typically in the differential diagnosis of MCL.
![]() 2. Mantle cell lymphoma의 임상적 특징
2. Mantle cell lymphoma의 임상적 특징
가장 중요한 특징은 처음 발견시 systemic disease인 경우가 대부분이라는 것입니다. 위장관도 대부분의 경우에 이미 침윤되어 있다고 합니다 (World J Gastroenterol. 2010).
1) Subtype of B cell NHL
2) Typically present with widespread adenopathy and frequently have bone marrow and extranodal involvement (Lymph nodes > 90%, Bone marrow 70-80%, Spleen 60%, Liver 30%, GI tract 20-30%), Peripheral blood (lymphocytosis) 20-30%)
3) GI tract involvement: 과거에는 10-20% 정도로 생각하였으나 최근에는 80-90%로 보고 있음
4) Most common type in GI tract: lymphomatous polyposis
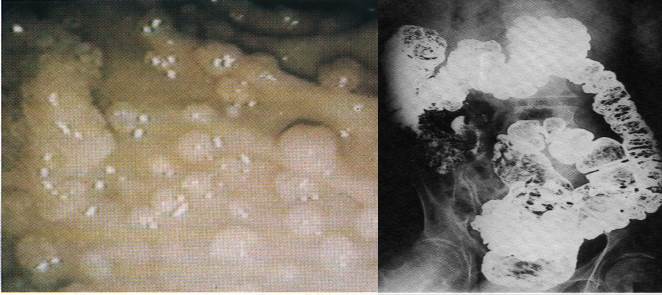
좌측 사진을 보십시오. 지금까지 제가 본 증례 중 가장 전형적인 lymphomatous polyposis 형태의 mantle cell lymphoma입니다.
5) Pathologically low-grade, clinically high-grade
6) 3-10% of all lymphoma cases
7) Mean age at presentation: 60 years
8) M:F = 3:1
9) Stage III-IV at presentation (70-80% of cases)
10) Poor prognosis: 5 years OS ≤ 30%
11) Best treatment modality: uncertain
[한 oncologist의 설명]
Mantle cell lymphoma 는 기본적으로 t(11;14)에 의해서 cyclin D1 이 양성이고, 양성이 아닌 경우는 cyclin D2 or 3가 양성일 것으로 생각합니다. 대개 두가지 타입으로 나눕니다.
1) Nodal type
이 경우는 oncogenic transcription factor 인 SOX11 양성이고 일반적으로 전신 다발성 림프절 비대를 보이며 임상적으로는 Follicular lymphoma 와 DLBCL의 중간 정도되는 공격성을 보입니다. 따라서 임상적인 모습은 mantle cell은 그렇게 빠르게 증식하고 공격성을 처음부터 보이지는 않습니다. 과거 mantle cell을 low grade로 분류했던 것도 이런 이유이지요. 하지만 재발을 반복하면서 공격적으로 변해가기 때문에 (다발 골수종 처럼) 처음부터 적극적인 치료를 합니다. 증상이 많이 심하지 않아도...
2) Leukemic non-nodal type
이 경우는 memory-like B cell orgin으로 SOX11 음성이고 이 경우는 주로 CLL 처럼 말초 혈액에 비정상세포가 많습니다. 그런데 대개 indolent 해서 치료를 하지 않고 경과를 많이 봅니다. 물론 이 경우도 치료가 필요한 경우에는 합니다. CLL처럼 matnle cel 대표적으로 위장관 multiple polyp 을 보이는 경우가 많은데 대부분 1)에서 그렇고 이것 여부가 예후자체에 미치는 영향은 크지 않습니다.
사실 stage I/II mantle cell lymphoma는 매우 희귀합니다. 증상이 없어서 진단시에 대개 4기입니다.
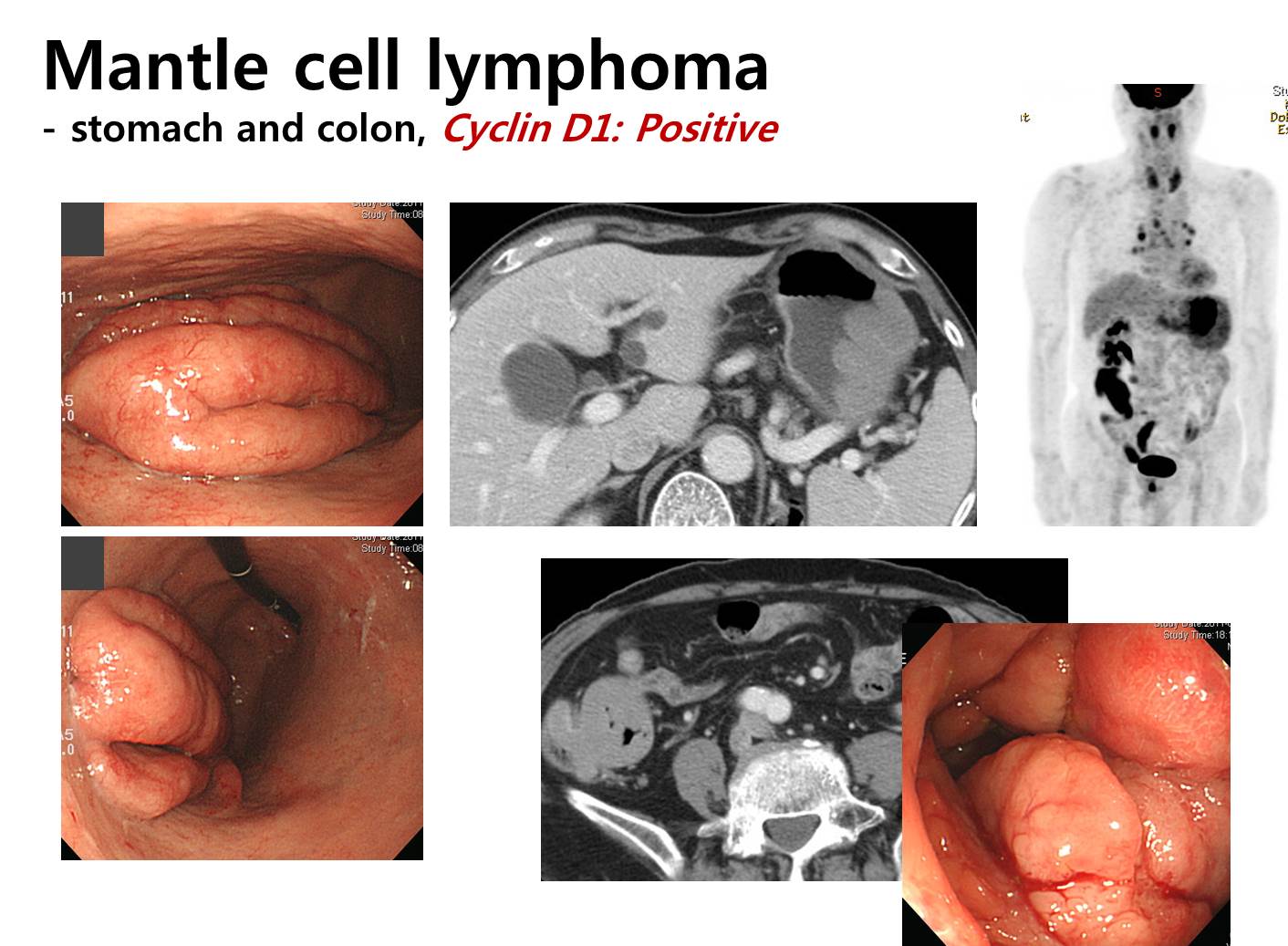
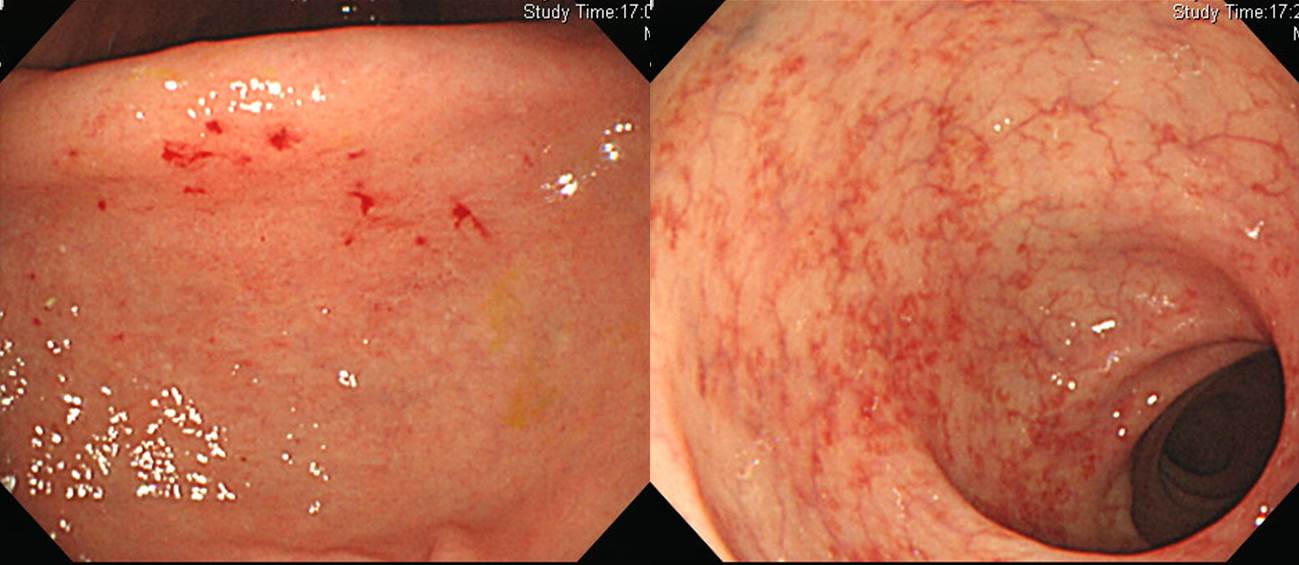
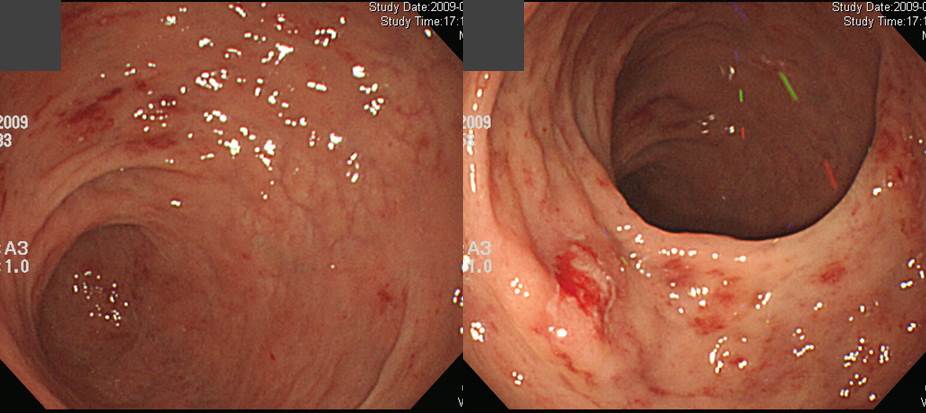
![]() 3. GI involvement of nodal MCL (Salar A. Am J Surg Pathol 2006;30(10):1274-80)
3. GI involvement of nodal MCL (Salar A. Am J Surg Pathol 2006;30(10):1274-80)
1) Only 26% of patients presented with GI symptoms at the time of diagnosis.
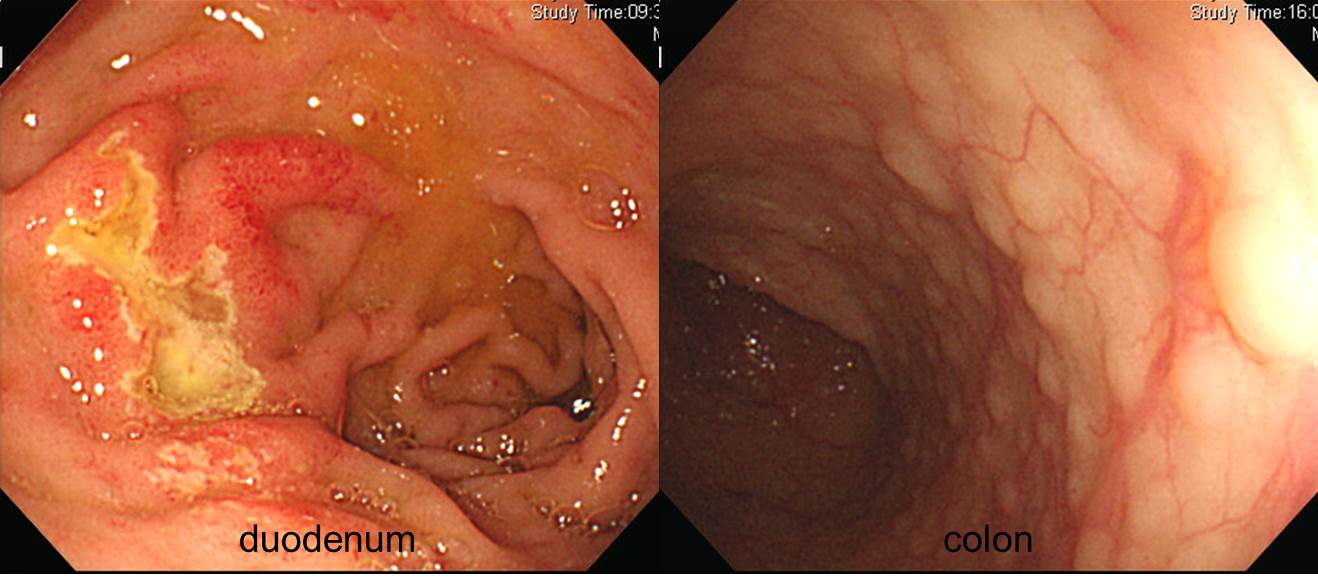
2) MCL was present histologically in the lower GI tract of 53 of 60 patient (88%) and in the upper GI tract of 28 of 58 patients (43%).
3) Microscopic evidence of MCL was found in 84% of patients with normal visual (macroscopic) findings by lower endoscopy and in 45% of patients with macroscopically normal findings by upper endoscopy.
4) Abnormal mucosa was identified in 38% of cases by upper endoscopy (mainly mild nonspecific gastritis) and in 54% of cases by lower endoscopy (mostly micropolyps).
Duodenum, stomach and colon involvement of MCL
5) Histologically, infiltration by MCL was demonstrated in the stomach in 77% of cases and in the colon in 77% of cases.
6) As a whole, 92% of patients showed upper or lower GI tract infiltration by MCL.
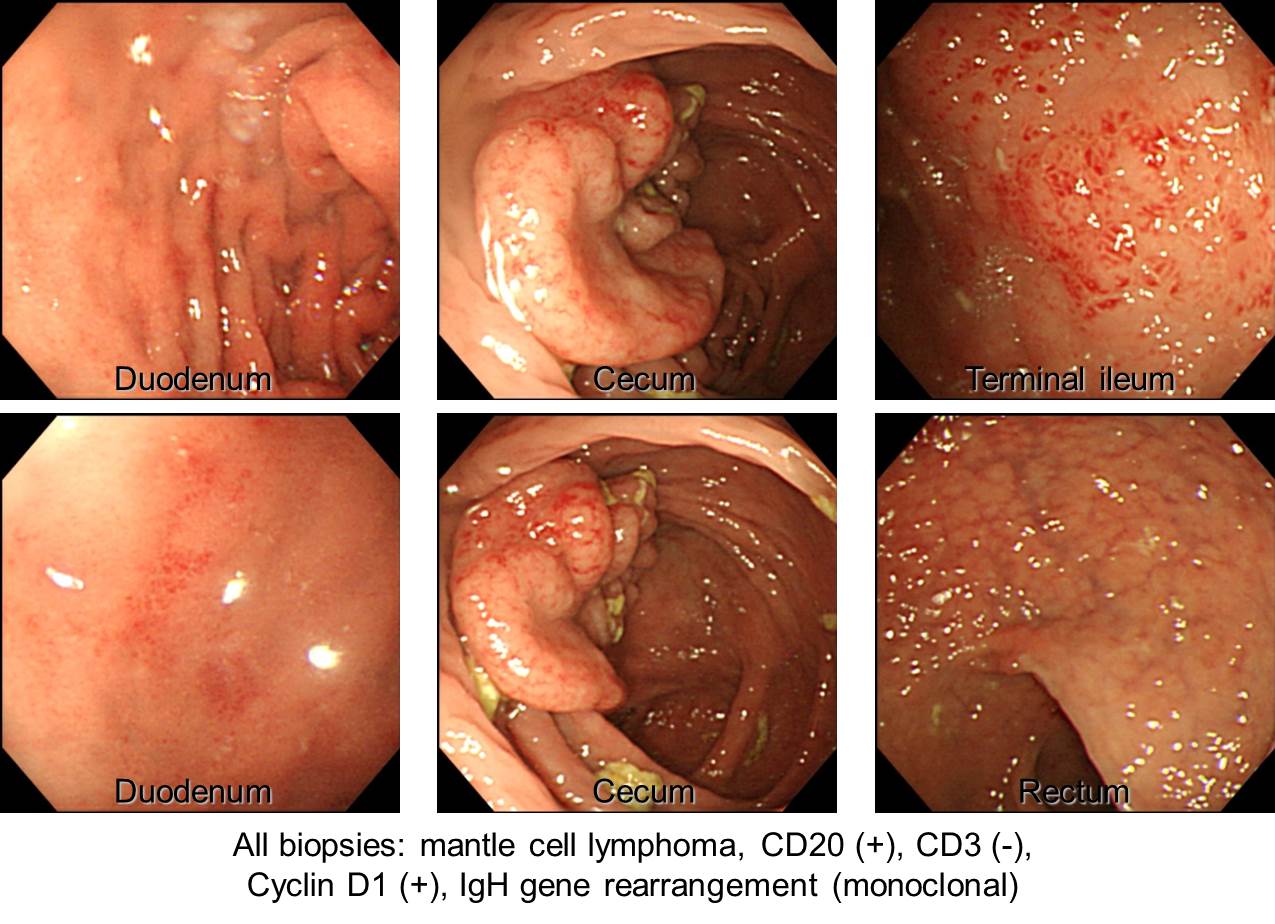
![]() 4. Colon involvement of MCL : lymphomatous polyposis type
4. Colon involvement of MCL : lymphomatous polyposis type
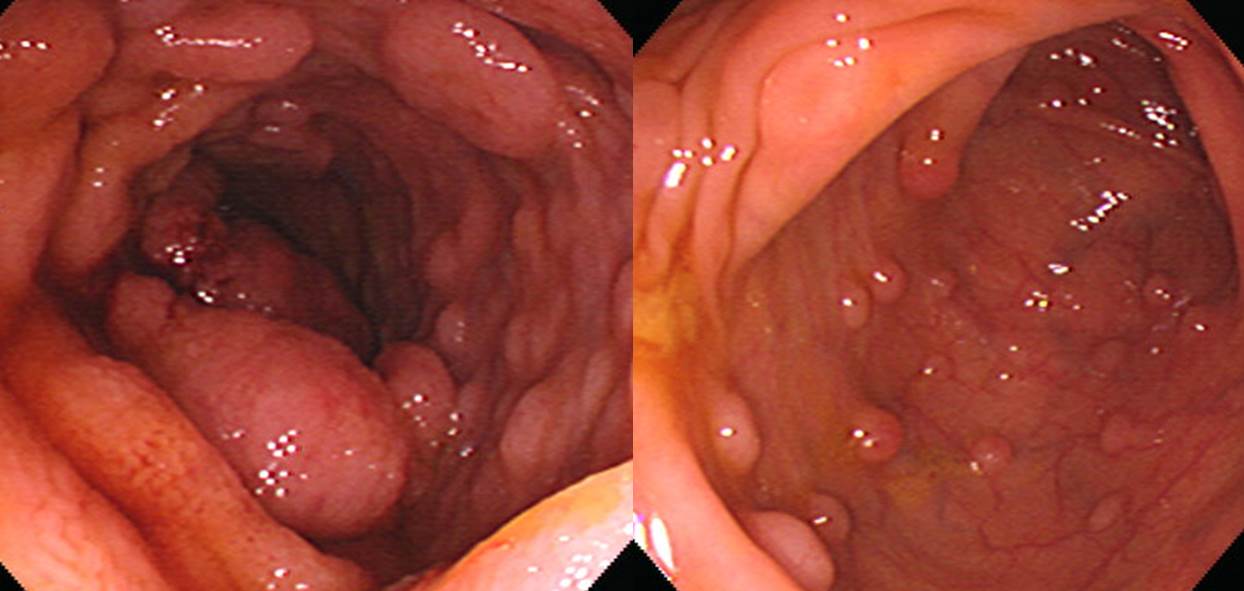
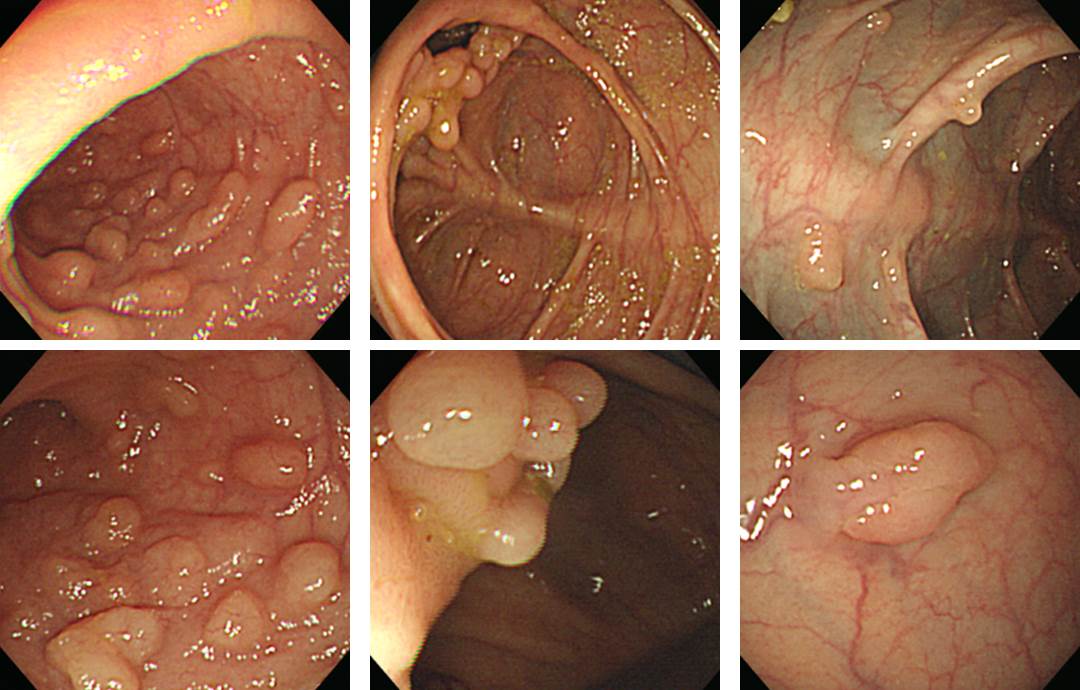

2016-9-23 내시경 집담회 서울대병원 증례. 대장 용종 EMR 후 cyclin D1 (+) mantle cell lymphoma로 진단되었으나 수 년 간 follow up loss가 되었음. 수 년 후 추적내시경에서 SMT 유사한 lymphomatous polyposis 양상이었음. 첫 임상상이 대장 용종이었고 10년 후까지 주된 병소가 대장과 mesentery였기 때문에 primary colonic mantle cell lymphoma로 판단하였음.
8년전 진단되었고 항암치료 후 호전되었다가 최근 재발됨. 용종 부위조직검사에서 모두 mantle cell lymphoma가 나옴.
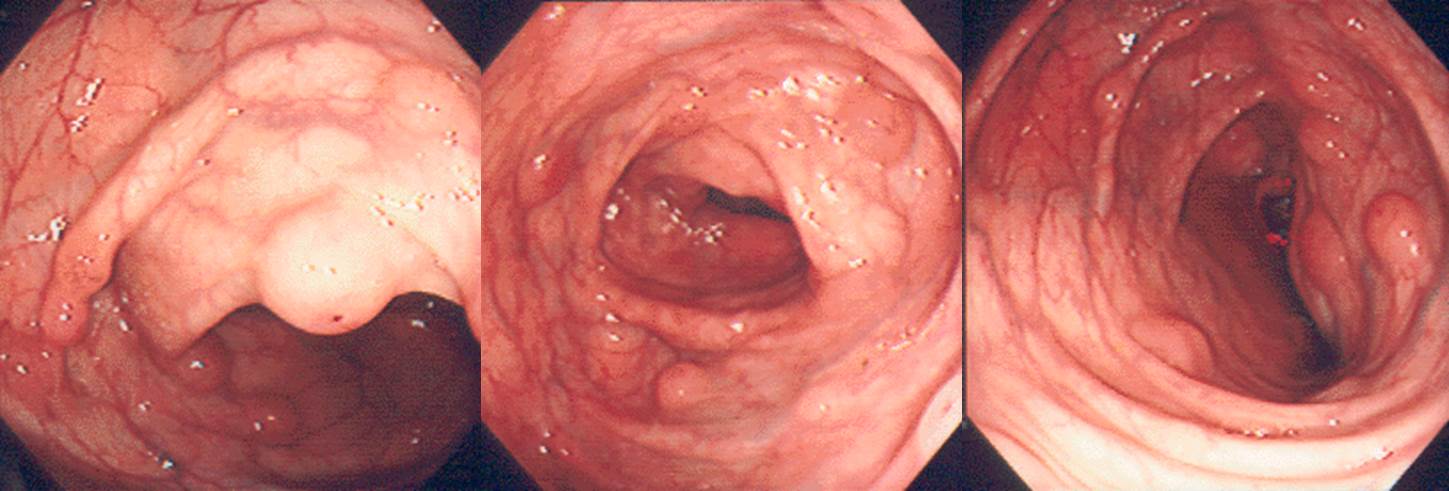
![]() 5. Colon involvement of MCL : non-lymphomatous polyposis type
5. Colon involvement of MCL : non-lymphomatous polyposis type

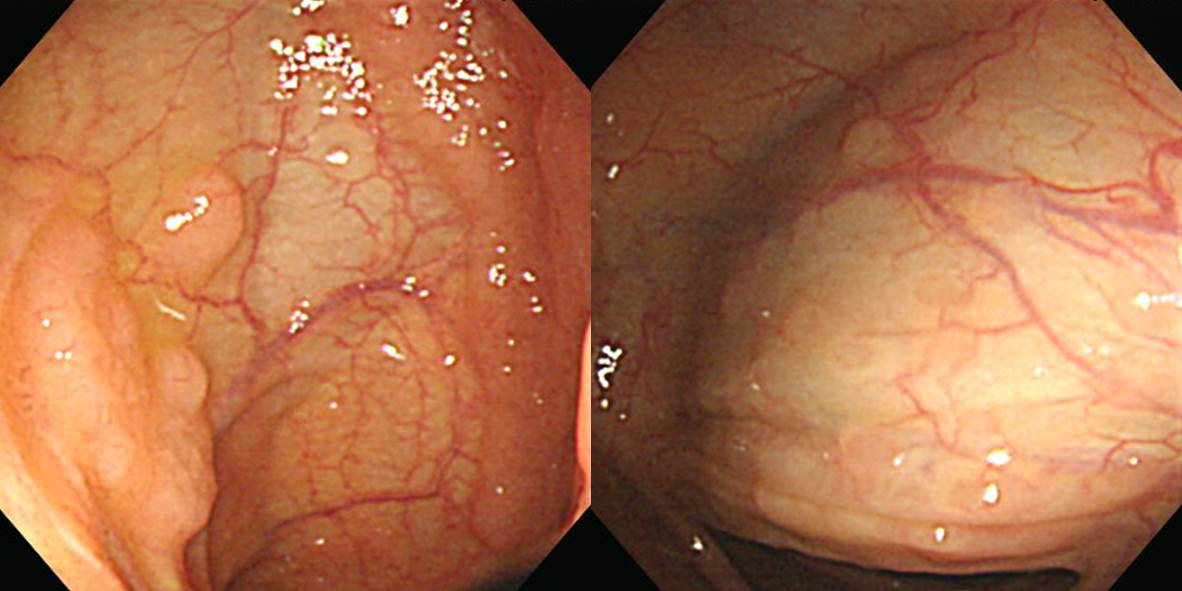
체중감소를 주소로 내원한 60대 여성의 대장내시경입니다. 조직검사에서 mantle cell lymphoma, cyclin D1 (+)가 나왔습니다. CT에서 ileum이 두꺼워 보였습니다. 경부 림프절과 골수 침윤이 있었습니다.
![]() 6. Stomach involvement of MCL
6. Stomach involvement of MCL

명란젓처럼 생겨서 깜짝 놀랐습니다.
9년 전 tonsil의 mantle cell lymphoma로 chemotherapy + RT 받은 환자의 위 내시경입니다. 조직검사에서 mantle cell lymphoma가 나와 stomach RT를 시행하였습니다.
![]() 7. Pathology of MCL
7. Pathology of MCL
1) MCL is characterized by neoplastic expansion of the mantle zone surrounding lymph node germinal center, with a homogeneous population of small lymphoid cells displaying slightly to markedly
2) irregular nuclear outlines, small nucleoili and scant cytoplasm.
3) In contrast to follicular lymphomas, very few large cells are identified among the mantle cells. The malignant cells are intermediate in size, between those of small lymphocytic lymphoma and
4) hose of follicular small cleaved cell lymphoma.
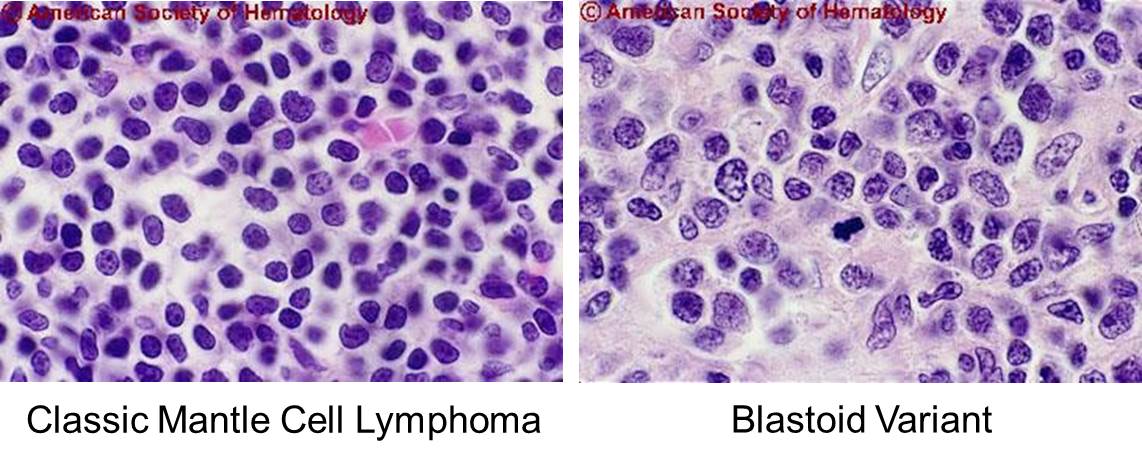
5) Small cell (small lymphocyte-like; intermediate lymphocyte) 80% of cases
6) “Blastoid” (classical/monomorphic; pleomorphic) 20% of cases
7) B marker: IgM (+) or IgD(+), CD19, CD20, CD22, CD79
8) T marker: CD10(-), CD23 (-), CD5 (weakly +)
9) Cyclin D1 (+)
10) BCL6 negative

[Genetics of MCL]
1) t(11;14)(q13;q32)
2) Immunoglobulin (H and L chains) clonal rearrangement
3) IgVH unmutated (70-80% of cases) origin from a subset of (CD5+) “naive” (pre-germinal centre) B lymphocytes
4) Conventional cytogenetics : often complex caryotype; del 6q, del 11q22, del 13q14…
5) CGH : chromosomal gains (3q26-27,…); and losses (13,Y,…)

![]() 8. Cyclin D negative mantle cell lymphoma
8. Cyclin D negative mantle cell lymphoma
Cyclin D negative MCL를 진단하기가 어렵습니다. 빈도는 2%로 추정됩니다. Cyclin D negative인 경우 SOX-11 expression이 진단하는데 도움될 수 있고 (Hematologica 2009. SOX11 mRNA and nuclear protein expression is a highly specific marker for both cyclin D1-positive and negative mantle cell lymphoma), SOX-11 expression이 음성인 경우 indolent한 경과를 보이는 경향이 있습니다 (Am J Hematol 2017 ).
(M/70, 2018)
위체부, 위전정부, 십이지장 조직검사 모두 mantle cell lymphoma로 나왔습니다. 진단 3개월 후 사망하셨습니다.
Diagnosis: B CELL LYMPHOMA with SOX11, PAX5 and CD138-positivity, suggestive of MANTLE CELL LYMPHOMA with plasma cell component
Ki-67 : Positive in 60% of tumor cells
CD 3, T-CELL : Negative in tumor cells
CD 20, L26 : Negative in tumor cells
CD 21, B-CELL : No follicular dendritic cell meshwork
SOX11 : Positive in tumor cells
CD 79a : Negative in tumor cells
Cyclin D-1 : Negative in tumor cells
Tdt : Negative in tumor cells
PAX-5 (Pan b Cell) : Weak positive in tumor cells
S-100 protein : Negative in tumor cells
CD 138, Syndecan-1 : Positive in tumor cells
Epstein-Barr virus: Negative in tumor cells
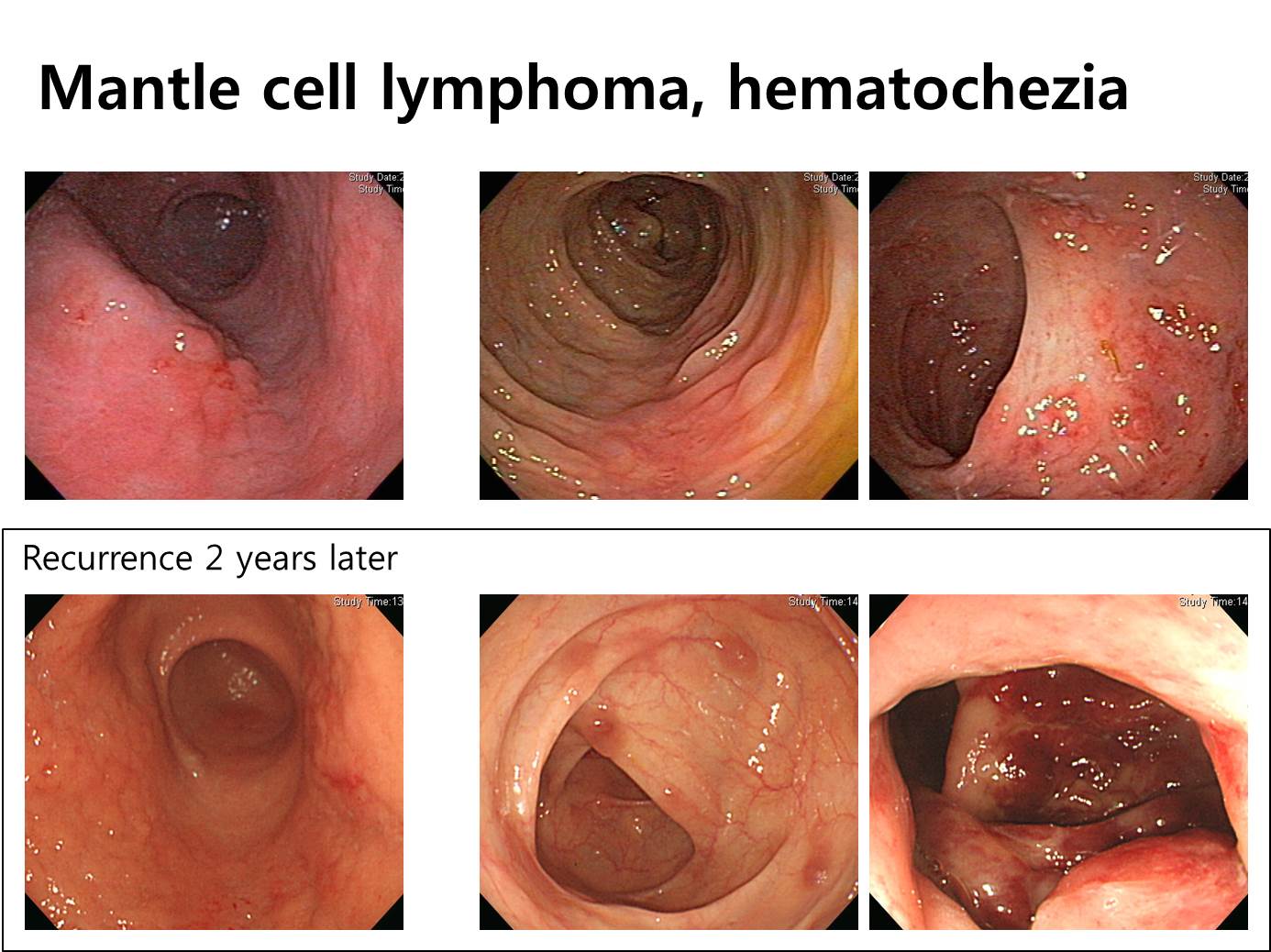
![]() 9. GI mantle cell lymphoma, experiences at Samsung Medical Center (Kim JH. Acta Haematol 2012)
9. GI mantle cell lymphoma, experiences at Samsung Medical Center (Kim JH. Acta Haematol 2012)
Endoscopic findings in mantle cell lymphoma with gastrointestinal tract involvement.
BACKGROUND AND AIMS: Mantle cell lymphoma (MCL) of the gastrointestinal (GI) tract is a rare disease with a poor prognosis. The aim of this study was to determine clinical and endoscopic characteristics of patients with GI MCL.
METHODS: Clinical features of 19 patients with GI MCL were reviewed along with the endoscopic findings on 27 anatomical lesions.
RESULTS: The initial presenting symptoms were abdominal pain (n = 7, 36.8%), GI tract bleeding (n = 5, 26.3%), dyspnea (n = 2, 10.5%), indigestion (n = 1, 5.3%), diarrhea (n = 1, 5.3%), cervical lymphadenopathy (n = 1, 5.3%), tonsilar mass (n = 1, 5.3%), and no symptoms (n = 1, 5.3%). On endoscopy, in 19 patients with 27 lesions, the anatomic locations of the lesions were: stomach, n = 2 (10.5%); stomach and colon, n = 7 (36.8%); terminal ileum and colon, n = 1 (5.3%); colon, n = 9 (47.4%). There was 1 fungating case (3.7%), 4 ulcerative cases (14.8%), 9 infiltrative cases (33.3%), and 13 polypoid cases (48.1%).
CONCLUSIONS: The endoscopic findings in GI MCL are variable, with common presenting manifestations of abdominal pain and GI bleeding.
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.