EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Situs inversus. 자리바뀜. 내장역위증.] - 終
[Situs inversus. 자리바뀜. 내장역위증.] - 終
![]() 1. 애독자의 질문과 이준행의 답변
1. 애독자의 질문과 이준행의 답변
[2013-6-18. 애독자 질문]
몇달전 sinus inversus totalis인 분이 와서 information없이 들어갔다가 pyloric ring을 겨우 찾고 2nd portion을 겨우 넘은 적이 있습니다.
Supine position등 검사 중 체위변화를 하니까 2nd portion으로 진입이 되었습니다. 선생님의 tip이 혹시 있으신지요?
[이준행 답변]
좋은 질문 감사합니다. 저도 답은 없습니다. 그러나 한 가지 말씀드리고 싶은 것이 있습니다. 내시경이 위로 들어간 후 방향을 잡을 수 없을 때 생각해야 할 상황이 세가지입니다. (1) 내시경의 기계적 이상입니다. 즉 공기가 잘 들어가지 않으면 위가 펴지지 않으면서 방향을 찾을 수 없게 됩니다. 50 ml syringe로 공기를 몇 번 넣어보면 금방 해결됩니다. (2) 보만 4형 진행성위암입니다. 잘 펴지지 않는 것이 중요한 특징이니까요. (3) Situs inversus입니다. 방향이 이상한 환자이므로 내시경의사가 당황하게 됩니다.
[애독자 comment]
제가 경험했던 환자는 처음에는 아무말도 하지 않고 비수면으로 내시경을 받고, 고생끝에 끝나고 나가면서 자기 내시경을 성공시킨 의사는 제가 처음이라며 다음에도 오겠다고 하며 떠났습니다.^^; 미리 얘기를 해주었다면 좋았을텐데요. 의사를 테스트하는 검진자도 있는 것 같아요.
[2013-6-19. C대 교수님 comment]
제 경험으로는 situs inversus의 경우 right down decubitus position으로 자세를 취하고 환자의 머리를 검사자 좌측에 위치한 내시경 본체에 가깝게 하여 시행하면 편하게 할 수 있음을 몇번 경험하였습니다. ESD 등에도 도움이 될 것 같습니다. 그래서 다음번에 혹시 ERCP할 일이 있으면 그렇게 해보려고 하는데 아직 기회가 없었습니다.
[이준행 답장]
좋은 의견 감사합니다. 다만 내시경실의 배치 관계로 실제로 그런 방향에서 시행하는 것이 쉽지는 않을 것 같습니다. 저도 나중에 situs inversus 환자를 만나서 내시경이 잘 되지 않으면 꼭 한번 시도해 보겠습니다.
[2013-6-20. 애독자 3의 의견. S대 교수]
사진이 없어 객관적인 증거를 보여드리긴 어려운데요... 말 그대로 정상인과 반대 방향으로 삽입하면 보는데는 문제가 없었습니다. 단 ESD와 같은 시술을 할때는 blind spot이 많아져 좀 어렵기는 합니다. 정확히 반대방향으로 접근하면 딱 맞았습니다.
![]() 2. Endoscopic pictures of situs inversus
2. Endoscopic pictures of situs inversus
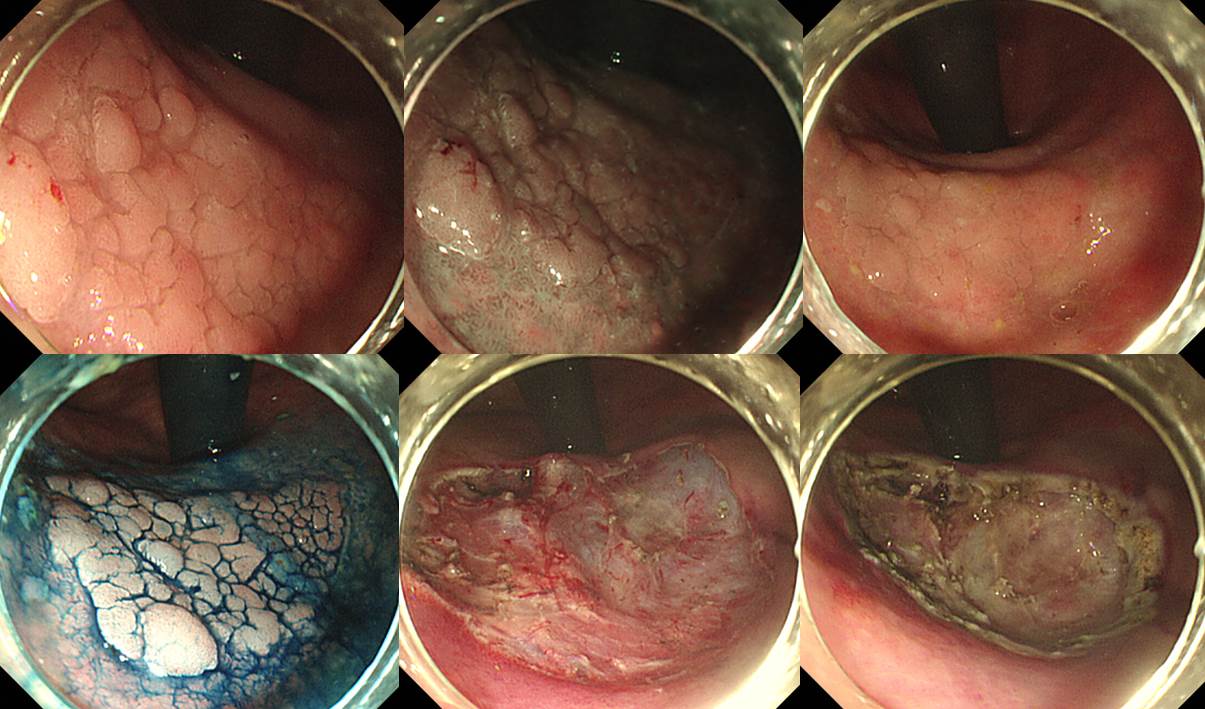
1998년 이준행이 군의관이던 시절 처음 진단한 situs inversus.
Situs inversus인줄 알고 검사하였는데도 방향을 찾는데 어려움이 있었음.
Situs inversus 환자의 위각에서 발생한 조기위암의 내시경치료. 매우 힘든 치료였다. 손목을 최대한 비틀고 내시경 knob를 많이 이용하였다. 시술 후 손목과 손가락이 아파 며칠간 고생하였던 기억이 역력하다. 내시경은 노동에 가깝다. ESD는 특히 그렇다. 중노동이다.
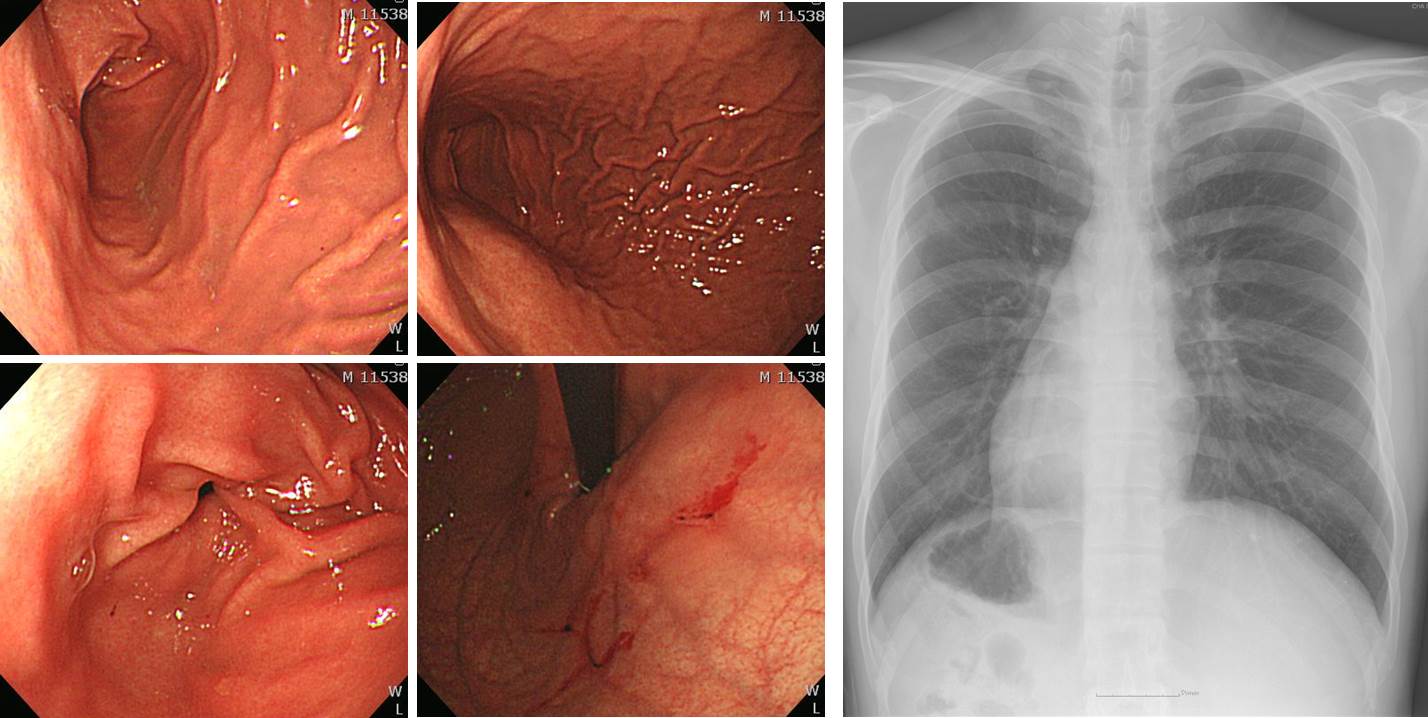
Dextrocardia 환자의 situs inversus (M/40)
![]() 3. Situs inversus에 대한 case에서 언급된 내용
3. Situs inversus에 대한 case에서 언급된 내용
Complete situs inversus is a rare congenital anomaly that results in a complete left-right inversion of the viscera. Although there is a link to various associated malformations and the immotile cilia or Kartagener syndrome, most patients with situs inversus have completely normal lives. Nevertheless, knowledge of this conditions is of paramount importance for the patient and the treating physician, as many gastrointestinal disease processes will manifest differently, ie, with pain on the "wrong" side. If an endosocpy is necessary, such as in our patient, careful attention should be paid to scope advancement.
A useful maneuver is the endoscopic "mirror technique." This technique mandates that all endoscopic maneuvers are performed inversely, as during a normal procedure. The basic principle of this technique is to perform the procedure as if the endoscopic exploration were the reflection of a standard endoscopy.1Once the cardia is reached, a left lateral deflection of the tip of the scope is followed by advancing the scope to the left instead of to the right. The "mirror" changes during scope advancement should also be paralleled by manipulation of the handle wheels, ie, the lateral and up-and-down movements of the tip of the scope should also follow a "mirror technique." This is especially important when the scope is inside the duodenal bulb.
![]() 4. 위암 385 - situs inversus 환자의 위암 및 remnant gastric adenoma의 ESD
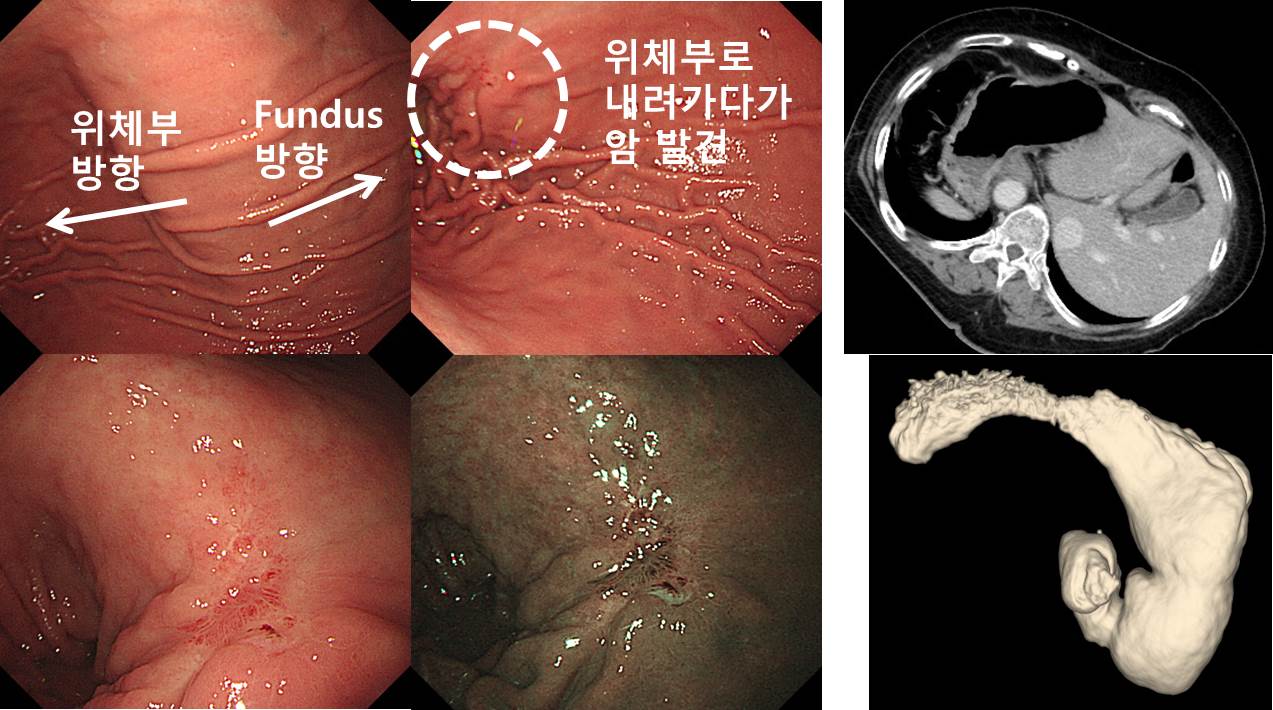
4. 위암 385 - situs inversus 환자의 위암 및 remnant gastric adenoma의 ESD
Dextrocardia 환자에서 발견된 위암입니다. 식도에서 위로 들어간 다음 평소와 같은 우측 방향이 아니라 화면의 좌측방향으로 antrum으로 가는 길이 있었습니다. 위각부 직상부에서 암이 발견되었습니다.
Stomach, subtotal gastrectomy:
Early gastric carcinoma
1. Location : middle third, Center at low body and posterior wall
2. Gross type : EGC type IIb+IIc
3. Histologic type : tubular adenocarcinoma, poorly differentiated
4. Histologic type by Lauren : diffuse
5. Size : 3.3x3 cm
6. Depth of invasion : invades mucosa (muscularis mucosae) (pT1a)
7. Resection margin: free from carcinoma
8. Lymph node metastasis : no metastasis in 38 regional lymph nodes (pN0)
9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. Peritoneal cytology : negative
13. AJCC stage by 7th edition: pT1a N0
그런데 이 환자의 remnant stomach에서 adenoma가 발견되었습니다. (1) dextrocardia, (2) remnant stomach, (3) cardia 직하부, (4) 비교적 넓은 병소인지가 상당히 어려웠지만 ESD는 가능했습니다. 엄청 힘들었습니다. Resection margin이 부족할까 싶어서 360도 circumferential APC ablation을 추가했습니다.
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.