EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [미분화조직형 조기위암의 림프절 전이 위험. Risk of LN metastasis in EGCs with undifferentiated-type histology] - 終
[미분화조직형 조기위암의 림프절 전이 위험. Risk of LN metastasis in EGCs with undifferentiated-type histology] - 終
| 2025-8-4. EndoTODAY 생각 |
| 하나의 기준이 있고 모두 그에 따라 진단하고 치료하면 혼선이 적을 것입니다. 위암 내시경 치료는 국제기준이라고 부르는 WHO 분류를 따르지 않는 일본에서 개발되고 발전되었습니다. 일본 의사들은 스스로 개발한 분류법(Nakamura 분류)에 따라, 스스로 개발한 적응증 (Gotoda table)에 의해 환자를 선정하고, 스스로 만든 기구(Olympus, Fujifilm 내시경과 accessory)를 이용하여, 스스로 개발한 시술(ESD)을 하고, 스스로의 결과(JCOG)에 따라 추가 치료 여부를 결정하기 때문에 비교적 일관된 ESD 서비스를 환자에게 제공하는 듯 합니다. 우리는 Nakamura 분류가 아닌 WHO 분류에 따라 진단하고, 일본에서 개발한 적응증을 약간 modify한 적응증을 정부 입맛에 따라 다시 modify한 기준에 의해 환자를 선정하고, 일제 내시경과 일제 기구를 이용하여 일제 시술(ESD)을 하고, 우리의 결과와 일본의 결과를 종합하여 추가 치료여부를 결정하고 있어서 일선 현장은 매우 혼란스럽습니다. 가장 혼란이 큰 부분이 undifferentiated histology 병소에 대한 ESD입니다. 걱정스러운 부분은 한두가지가 아닙니다. (1) 일본 연구에 비하여 우리 연구에서 일관성있게 림프절 전이가 많았습니다. (2) 내시경 의사뿐만 아니라 병리 의사의 interobserver variation이 상당합니다. (3) 체계적인 longterm 연구가 부족합니다. (4) 국민건강보험에서 ESD 적응증을 매우 좁게 제시하고 있으므로 undifferentiated histology 위암에 대한 ESD는 선별급여입니다. 즉 환자가 돈을 더 많이 내야 합니다. 불필요하게 환자를 유인하였다는 의심을 받기 쉽습니다. (5) 위암 ESD 후 수술이 필요하다고 나온 환자 중 수술을 받지 않는 환자가 제법 많습니다. (6) 학계에서 의견이 통일되지 않았습니다. 폭넓은 적응증을 가지고 있는 전문가가 해당 부분의 강의를 하는 경우가 많습니다. 특수한 상황을 일반적인 것처럼 포장하는 예도 많습니다. (7) 환자에게 informed consent를 받는 과정이 매우 형식적입니다, 등등. 이런 상황에서 undifferentiated type histology 위암에 대한 내시경 치료는 아직도 매우 조심스럽게 진행되어야 한다고 생각합니다. 아주 조금이라도 마음에 걸리는 요소가 있으면 현재의 표준치료인 수술을 권하는 것이 맞다고 생각합니다. |
![]() 1. 초기 연구
1. 초기 연구
1990년대부터 확대적응증을 언급한 작은 연구들이 있었습니다. 그러나, 확대적응증에 대한 논의가 본격화 된 것은 위암이 많았던 두 병원(동경암센터와 동경암연구회병원)의 수술 후 림프절 전이 위험 분석을 바탕으로 한 2000년 Dr. Gotoda의 제안(Gastric Cancer 2010;3:219)이 계기가 되었습니다. 여기에는 undifferentiated-type이 포함되어 있습니다.
2009년 동경 암연구회 병원의 Hirasawa는 수술을 받은 undifferentiated-type 조기위암의 병리결과를 분석하여 2000년 Gotoda 논문의 결과를 반복하였습니다. 두 연구는 두 가지 점에서 다릅니다. (1) Gotoda는 3cm를 제시한 반면, Hirasawa는 2cm를 제시하였습니다. 이후 모든 가이드라인에서는 2cm가 표준이 되었습니다. 어떤 data를 기점으로 3cm가 2cm로 좁혀졌는지는 저는 모르겠습니다. (2) Hirasawa 연구가 더 컸기 때문에 95% confidence interval이 0-0.96%로 더 좁았습니다. 한 가지 우려점을 연구 대상이 중복된 것 같다는 것입니다. 둘 다 동경암연구회 병원과 동경암센터의 자료를 모아서 분석한 것이기 때문입니다.
2011년 서울아산병원의 연구(Chung JW. JGH. 2011)에서는 점막암의 림프절 전이 위험이 분석되었습니다. 저자들이 Criteria III로 명명한 'undifferentiated less than 20 mm without ulceration'에서는 통계적을 유의한 수준의 림프절 전이 위험이 있는 것으로 분석되었습니다 (1.15%, 3/261, 95% CI, 0-2.44%).
2012년 삼성서울병원의 연구(Lee JH. Br J Surg. 2012)에서는 poorly differentiated만 따로 분석했습니다. ESD 적응증과 유사한 기준을 적용하였는데, 위험인자가 없는 124명 중 4명 (3.2%)에서 림프절 전이가 있었습니다. 여러 자료에서 singet ring cell 형보다 P/D 형이 더 위험하다는 점을 지적한 것과 같은 맥락이라고 생각됩니다.
![]() 2. 연세대학교 심충남 선생님의 멋진 종설 (2014)
2. 연세대학교 심충남 선생님의 멋진 종설 (2014)
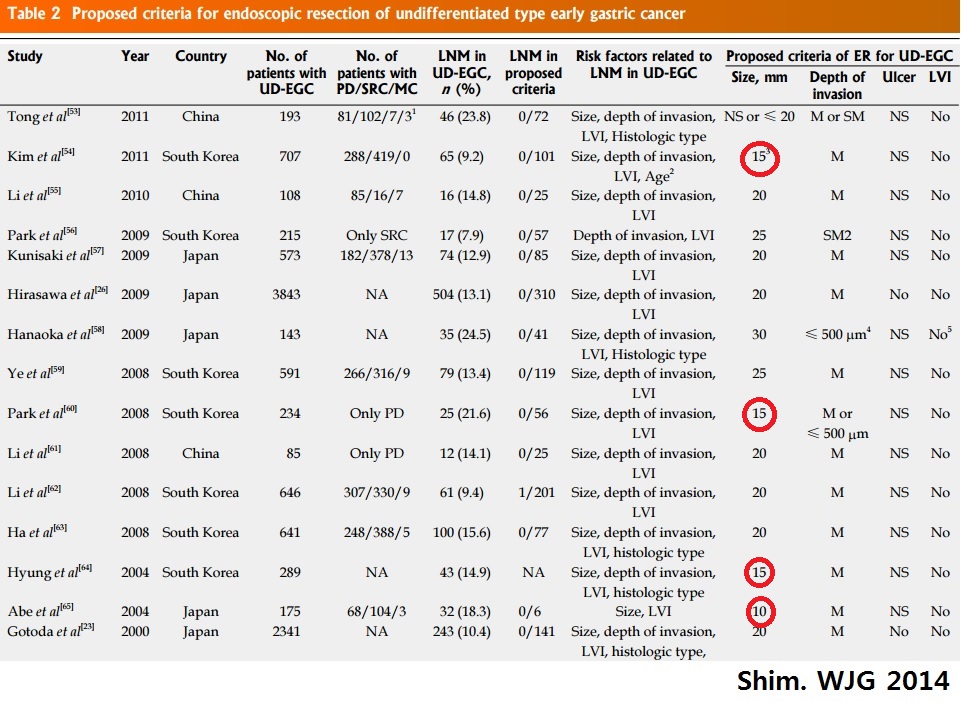
2014년 연세대학교의 심충남 선생님께서 undifferentiated-type EGC의 내시경치료에 대한 종설을 발표하였습니다 (Shim. World J Gastroenterol. 2014). 기존에 발표된 수술병리 검토 결과를 잘 요약하셨습니다. 일부 연구(붉은 색 동그라미)에서는 20m가 아니라 10-15mm를 기준으로 제시하였다는 점에 주목하시기 바랍니다.
심충남 선생님은 내시경으로 크기 측정의 오류 가능성을 잘 설명하셨습니다. 심충남 선생님께서는 size discrepancy에 대한 논문도 발표한 바 있으므로 (Shim. Surg Endosc. 2014), 이 부분에 관심이 많은 것 같습니다. 해당 부분을 옮깁니다 (WJG 2014;20:3938-3949 중 3940쪽).
Moreover, the size discrepancy between pathologic size and endoscopic size should be resolved, because we can only determine the indications of ER based on the endoscopically estimated size. While a previous study revealed that endoscopic visual estimation method was found to show reliable agreement with pathologic measurements in EGC treated with ER, other earlier ESD series showed the mean size discrepancies ranged from 5.8 mm to 6.8 mm, which are not negligible in ER for EGC. In UD-EGC, the margins of the lesion tend to be obscured compared to the differentiated histology, which was found to cause frequent margin failure of ESD in our previous report. Thus, a standard reliable measurement method is required through further prospective studies.
비슷한 시기에 연세대학교에서는 signet ring cell carcinoma에 대한 ESD에서 크기의 역할에 대하여 분석한 연구를 발표하고 있습니다 (Kim MN. Dig Liver Dis. 2014). 초록의 Results 부분이 아주 명료하게 잘 정리되어 있어서 숫자를 빼고 옮깁니다.
Multivariate analysis showed that large tumour size was the only significant factor related to incomplete resection. In addition, large tumour size was the only significant factor related to endoscopic size underestimation. The rate of endoscopic size underestimation was significantly higher in tumours with a size ≥20mm.
![]() 3. 점막에 국한된 signet ring cell carcinoma의 림프절 전이 위험
3. 점막에 국한된 signet ring cell carcinoma의 림프절 전이 위험
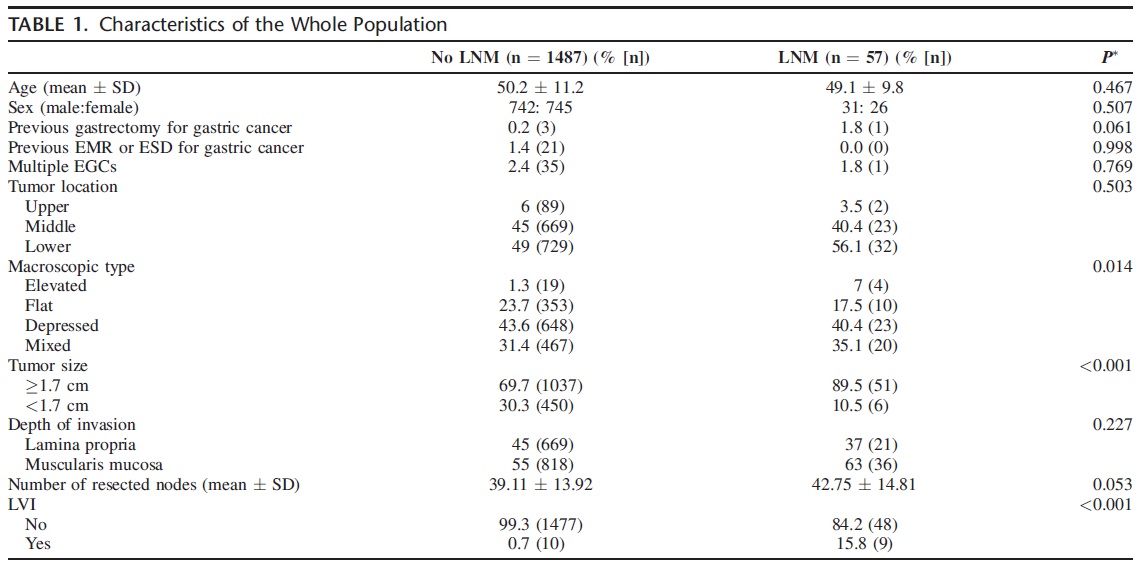
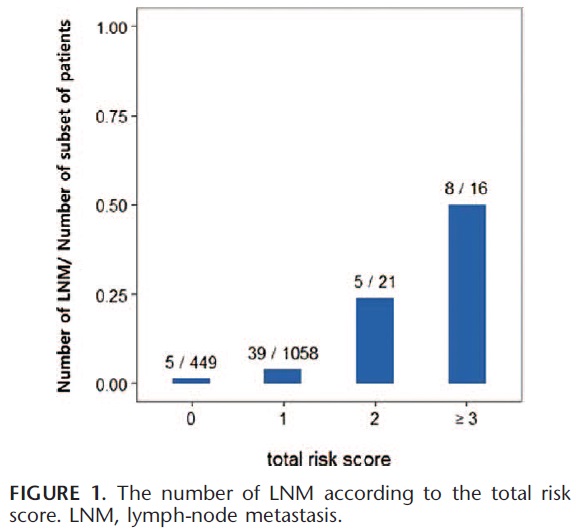
2016년 1월 Ann Surg에 점막에 국한된 signet ring cell carcinoma의 림프절 전이 위험에 대한 삼성서울병원의 분석이 발표되었습니다 (Pyo JH. Ann Surg 2016). 1,544명의 환자를 분석하였을 때 림프절 전이는 3.8%에서 발견되었습니다.
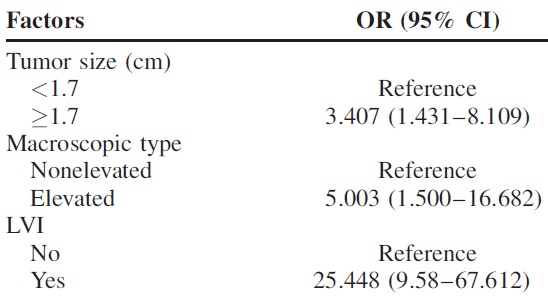
세 개의 위험인자가 확인되었습니다 ((tumor size ≥1.7 cm, tumors of elevated type, and lymphatic-vascular involvement). Non-elevated type에 비하여 elevated type이 무려 5배 위험했습니다.
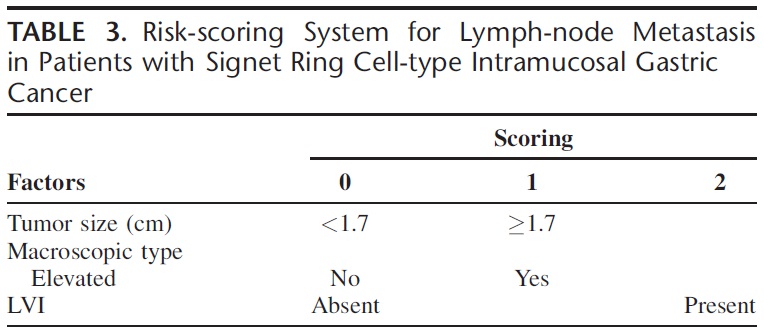
세 위험인자를 이용하여 risk scoring system이 만들어졌고 이를 적용하였을 때의 점수와 림프절 전이가 linear한 관계가 있음을 보여주었습니다.
![]() [FAQs]
[FAQs]
| 2025-8-4. EndoTODAY 생각 |
| 하나의 기준이 있고 모두 그에 따라 진단하고 치료하면 혼선이 적을 것입니다. 위암 내시경 치료는 국제기준이라고 부르는 WHO 분류를 따르지 않는 일본에서 개발되고 발전되었습니다. 일본 의사들은 스스로 개발한 분류법(Nakamura 분류)에 따라, 스스로 개발한 적응증 (Gotoda table)에 의해 환자를 선정하고, 스스로 만든 기구(Olympus, Fujifilm 내시경과 accessory)를 이용하여, 스스로 개발한 시술(ESD)을 하고, 스스로의 결과(JCOG)에 따라 추가 치료 여부를 결정하기 때문에 비교적 일관된 ESD 서비스를 환자에게 제공하는 듯 합니다. 우리는 Nakamura 분류가 아닌 WHO 분류에 따라 진단하고, 일본에서 개발한 적응증을 약간 modify한 적응증을 정부 입맛에 따라 다시 modify한 기준에 의해 환자를 선정하고, 일제 내시경과 일제 기구를 이용하여 일제 시술(ESD)을 하고, 우리의 결과와 일본의 결과를 종합하여 추가 치료여부를 결정하고 있어서 일선 현장은 매우 혼란스럽습니다. 가장 혼란이 큰 부분이 undifferentiated histology 병소에 대한 ESD입니다. 걱정스러운 부분은 한두가지가 아닙니다. (1) 일본 연구에 비하여 우리 연구에서 일관성있게 림프절 전이가 많았습니다. (2) 내시경 의사뿐만 아니라 병리 의사의 interobserver variation이 상당합니다. (3) 체계적인 longterm 연구가 부족합니다. (4) 국민건강보험에서 ESD 적응증을 매우 좁게 제시하고 있으므로 undifferentiated histology 위암에 대한 ESD는 선별급여입니다. 즉 환자가 돈을 더 많이 내야 합니다. 불필요하게 환자를 유인하였다는 의심을 받기 쉽습니다. (5) 위암 ESD 후 수술이 필요하다고 나온 환자 중 수술을 받지 않는 환자가 제법 많습니다. (6) 학계에서 의견이 통일되지 않았습니다. 폭넓은 적응증을 가지고 있는 전문가가 해당 부분의 강의를 하는 경우가 많습니다. 특수한 상황을 일반적인 것처럼 포장하는 예도 많습니다. (7) 환자에게 informed consent를 받는 과정이 매우 형식적입니다, 등등. 이런 상황에서 undifferentiated type histology 위암에 대한 내시경 치료는 아직도 매우 조심스럽게 진행되어야 한다고 생각합니다. 아주 조금이라도 마음에 걸리는 요소가 있으면 현재의 표준치료인 수술을 권하는 것이 맞다고 생각합니다. |
![]() [References]
[References]
© EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. 일원내시경교실 바른내시경연구소 이준행