 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [EsoTODAY 063 - Pyriform sinus pouch/diverticulum] - 終
[EsoTODAY 063 - Pyriform sinus pouch/diverticulum] - 終
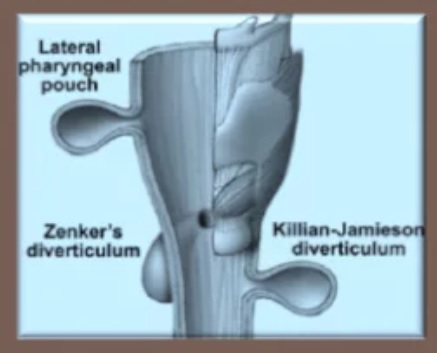
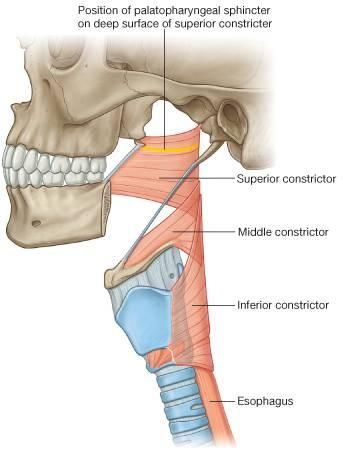
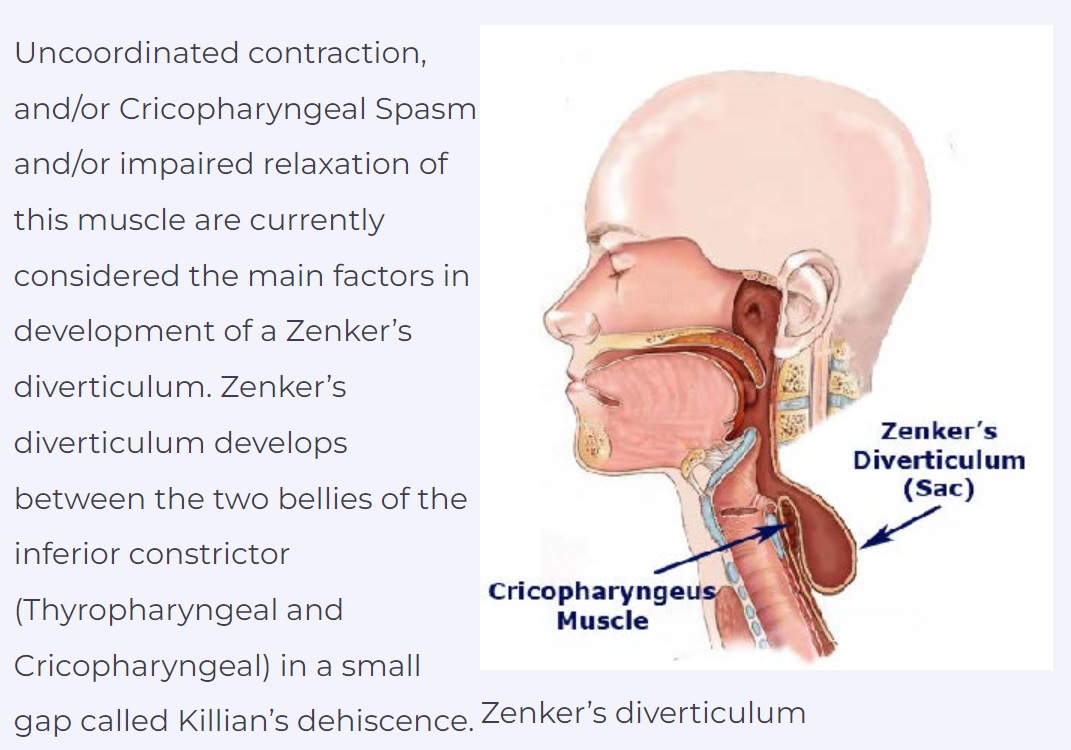
바쁜 분을 위한 요약: 인후부, 상부식도 게실 중 (1) 가장 위쪽이 pyriform sinus diverticulum (= lateral pharyngeal diverticulum)이며 middle constricture와 inferior constrictor 사이에서 옆으로 발생합니다. (2) 중간이 Zenker diverticum이며 inferior constricture의 중간, 즉 위쪽의 thyropharyngeal muscle과 아래의 cricopharyngeal muscle 사이에서 뒤로 발생합니다. (3) 가장 아래가 Killian-Jamieson 게실이며 cricopharyngeal muscle 아래에서 옆으로 발생합니다.
Pyriform sinus diverticulum(이상동 게실, 이상와 게실, = lateral pharyngeal diverticulum)은 식후 이물감과 목이 옆으로 튀어나오는 것이 특징이며 내시경 검사에서 발견하지 못하는 경우가 많고 간혹 fistula opening처럼 보일 수 있습니다. Barium study로 확진할 수 있습니다.
60세 남성이 갈치 반찬과 함께 식사 후 왼쪽 목에 이물감있어 인근에서 이비인후과 진찰 및 상부위장관내시경 검사 후 특이소견이 없다고 들었으나 왼쪽 목 통증이 지속되어 외래 방문하였다. 내시경 재검에서 이물은 없었으나 왼쪽 이상와(pyriform sinus)에 fistula 의심 소견이 발견되었다 (좌측 사진). 목까지 포함한 chest CT 검사를 하였고 이물이나 free air는 없었다. 이후 증세는 저절로 사라졌다. 식도조영술을 시행하였고 왼쪽 이상와에서 약 1 cm 크기의 게실이 발견되었다 (우측 사진). 외래에서 다시 병력을 확인하였다. 환자는 20년 전부터 1년에 한 두 번 목에 이물이 걸렸고, 그때마다 고개를 좌우로 끝까지 돌리면 걸린 것이 톡 튀어나올 때가 있었다. 간혹 수 일 동안 증상이 지속되기도 하였다. 수술 및 경과관찰에 대하여 상의하였고 환자는 현재 증상이 없으므로 일단 경과관찰을 선택하였다.
![]() [증례]
[증례]
출처: https://www.eurorad.org/case/2320
A 32-year-old male farmer presented with dysphagia and regurgitation and a history of a sensation of intermittent bilateral neck masses during swallowing since early childhood. In the patient’s history, a sensation of bilateral intermittent neck masses during swallowing since early childhood (as far as he could remember) was mentioned.
Imaging findings: During the intradeglutitive phase, in the frontal view, two round symmetric air-filled cystic structures were noted that communicated through narrow ducts with the upper lateral pyriform sinus walls, at the valleculae level (Fig. 1).
Simultaneously, the hypopharynx appeared to be generally distorted, more obviously on performing the modified Valsalva maneuver, with lateral pyriform sinus pouch formation and the presence of a diverticulum arising from the lateral wall of the left pyriform sinus apex (Fig. 2).
DISCUSSION; Most authors refer to transient lateral pharyngeal protrusions as “pharyngeal pouches”, whereas they prefer to use the term “lateral pharyngeal diverticula” when the protrusions are permanent. Lateral pharyngeal pouches are more common than was believed in the past. They arise in weak areas of the lateral pharyngeal wall. In the hypopharynx, this area is located at the posterior lateral wall of the pyriform sinuses, between the middle and inferior constrictor muscles which fail to overlap, leaving an area of the thyrohyoid membrane with no muscular support when the intraluminal hypopharyngeal pressure rises, as with deglutition. (참고: Zenker diverticulum은 inferior constrictur muscle를 이루고 있는 위쪽의 thyropharyngeal muscle과 cricopharyngeal muslce 사이에서 발생한다)
So, with aging, lateral wall bulging may occur. At a higher level, another weak area develops at the site of the tonsillar fossae after a tonsillectomy is done, the tonsils representing the major supporting structures of this area. Lateral pharyngeal pouches are a common finding in the elderly population and can be considered as a normal variant. Acquired lateral pharyngeal diverticula are found to be rare. They occur almost exclusively through a slit-like opening in the weak area of the thyrohyoid membrane, most often distally to a lateral pharyngeal pouch as a result of repeated pharyngeal distention due to a high intraluminal pressure. They are usually unilateral and occur singly. Adults engaged in activities that repeatedly raise the intrapharyngeal pressure (e.g., playing wind musical instruments, blowing glass) are at high risk of developing lateral pharyngeal diverticula. Congenital lateral pharyngeal protrusions are rarely found and represent the remnants of pharyngeal pouches and branchial clefts, communicating with each other. Diverticula consist of branchial cleft cysts and ducts, whereas pharyngeal fistulas consist of sinus tracts, both communicating with the pharynx internally and ending blindly externally. Incomplete anomalies in the form of cysts or fistulas with an external blind end are rare. Second branchial cleft remnants communicate with the pharynx at the tonsillar fossa, which develops from the second branchial pouch. Third and fourth branchial cleft remnants communicate with the base of the pyriform sinus at the level of the valleculae and the apex of the pyriform sinus, respectively.
Pyriform sinus abnormalities develop in the left lateral neck in, approximately 95% of the cases . Clinically, pharyngeal pouches and acquired diverticula may be asymptomatic, or cause dysphagia, a lump or foreign body sensation in the throat, and aspiration, due to retention of food and delayed emptying of their contents to the valleculae and pyriform sinuses. Congenital lateral pharyngeal abnormalities usually present in the first or second decades of life. Dysphagia, aspiration, sensation of a lump or an intermittent neck mass, regurgitation of food, discomfort in the throat and neck swelling are the symptoms reported for congenital diverticula. With late presentation in adulthood, the patients typically report the onset of symptoms during childhood, which strongly indicates the congenital origin of the anomalies. In children, congenital anomalies, cysts and fistulas may also present as masses in the neck, respiratory distress, acute or recurrent inflammation, abscess formation, hoarseness and nerve palsies, with an upper airway obstruction and suppurative thyroiditis being more common in neonates.
Because it is very narrow, the internal opening of a lateral pharyngeal diverticulum or fistula can easily escape the endoscopist’s attention during a radiography examination.
참고: '세균맨'이라는 blog에서 right pyriform sinus diverticulum이 소개되었습니다.
The lesions are more easily identified on fluoroscopic examination on swallowing barium in the frontal view. Congenital lateral pharyngeal diverticula are usually unilateral, most often to the left, and occur singly. They can be seen as cystic structures connected by a narrow duct of varying lengths to the tonsillar fossa or the pyriform sinus, either to its base at the level of the vallecula, or to its apex. They may be intermittently identified, being filled with air during the pharyngeal phase of swallowing, with their walls subsequently collapsing during the post-deglutitive phase, or, more permanently, with barium retention. Common lateral pharyngeal pouches present as semi-oval, “ear-like” protrusions of the lateral pharyngeal wall, with a broad opening leading to the region of the pyriform sinuses, or, less commonly, the tonsillar fossae. They are transient findings during deglutition, disappearing in the post-deglutitive phase, usually bilateral and symmetric. Acquired lateral pharyngeal diverticulum consists of a pouch , with a usually short neck, at the apex of the pyriform sinus which fills and retains barium.
![]() [References]
[References]

2020-4-25. 순천만내시경세미나 동영상 강의
1) Pyriform sinus diverticulum
2) 식도 게실: Zenker diverticulum, Killian-Jamieson 게실, 중부식도 게실, 하부식도 게실
3) 위 게실
4) 십이지장 게실
5) Meckel 게실
6) 대장 게실과 게실염
![]() © 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (since 1999-8-23)
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (since 1999-8-23)


{kind=link}