EndoTODAY ГЛНУАц БГНЧ
EndoTODAY ГЛНУАц БГНЧ
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [СІ5Тї ЛяМКМПяКДПј НФЕЕОЯ НЩЦїСіОі (2016)] - №ћ
[СІ5Тї ЛяМКМПяКДПј НФЕЕОЯ НЩЦїСіОі (2016)] - №ћ
РЯНУ: 2016Гт 10Пљ 15РЯ (Хф)
РхМв: ЛяМКМПяКДПј ОЯКДПј СіЧЯ2Уў СпАДч


![]() 1. Neoadjuvant chemotherapy for locally advanced esophageal cancer: the Japanese strategy and its rationale - Harushi Udagawa (Toranomon Hospital, Tokyo)
1. Neoadjuvant chemotherapy for locally advanced esophageal cancer: the Japanese strategy and its rationale - Harushi Udagawa (Toranomon Hospital, Tokyo)
ПЌРкДТ РЯКЛРЧ АЅЖѓЦФАэНК ЧіЛѓРЛ О№БоЧЯПДНРДЯДй. ДйИЅ И№Еч ГЊЖѓПЭ РЯКЛРЬ ДйИЃДйДТ АЭРдДЯДй. ННЖѓРЬЕхРЧ СІИёРЬ "Why is Japanese treatment strategy of esophageal cancer different from rest of the world?"ПДНРДЯДй.
1) ChemoRT vs chemotherapy
МОчПЁМДТ neoadjuvant chemoRT АЁ neoadjuvant chemotherapyКИДй ПьПљЧЯДйАэ КИДТ АЭРЬ РЯЙнРћРдДЯДй. БзЗЏГЊ РЯКЛПЁМДТ neoadjuvant chemotherapy aloneРЬ ЛчПыЕЫДЯДй. ПЌРкДТ БзПЁ ДыЧб ПЊЛчРћ ЙшАцАњ ЕЅРЬХИИІ МГИэЧЯПДНРДЯДй. ЧбИЖЕ№ЗЮ "МіМњ ЙќРЇАЁ ГаРИИщ neoadjuvant chemotherapy aloneРЬ УцКаЧЯДй. МОчРК РлРК МіМњРЛ ЧЯБт ЖЇЙЎПЁ neoadjuvant chemoRTАЁ ЧЪПфЧЯДй"ДТ МГИэРдДЯДй.
"Long before the introduction of TFD (three-field lymph node dissection), Japanese surgeons first applied preoperative radiotherapy to advanced esophageal cancer in the pursuit of better survival. It was related to late diagnosis of the disease in general at that time. This strategy was denied by JCOG8201. Since then, we have concentrated our interest in postoperative chemotherapy. As a backgroud, adjuvant chemotherapy was easier to adopt in the treatment strategy including extended lymphadenectomy. JCOG9204 showed better disease free survival in 'surgery + adjuvant chemotherapy' group over 'surgery alone' group. As the concept of 'neoadjuvant threatment' was introduced and became popular, and as the safety of TFD was improved on the other hand, neoadjuvant chemotherapy became our next target. JCOG9907 clearly showed that 'neoadjuvant chemotherapy + surgery' realized better survival than 'surgery + adjuvant chemotherapy'."
2) МіМњРЧ ЙќРЇ
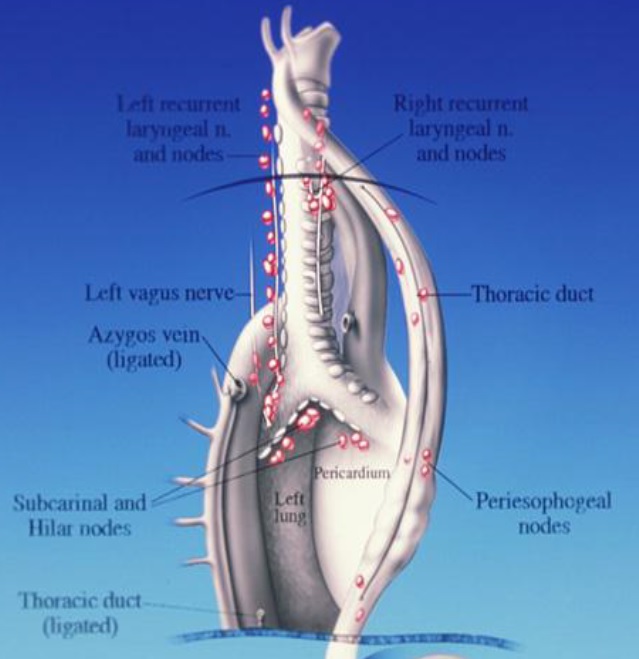
Two field lymph node dissectionПЁМ Three-field lymph node dissection (TFD)РИЗЮ МіМњ ЙќРЇАЁ ГаОюСГНРДЯДй. Ся upper mediastinal lymph nodesПЭ cervical lymph nodesБюСі БЄЙќРЇЧЯАд dissection ЧЯДТ АЭРИЗЮ, ЧіРњЧб Л§СИБтАЃРЧ ЧтЛѓРЬ РжОњНРДЯДй. РЯКЛПЁМ БЄЙќРЇЧб lymph node dissectionРЧ ИёРћ(РЯКЛПЁМ three-field lymph node sissection МіМњПЁМ Р§СІЕШ ИВЧСР§РК 100АГ РЬЛѓ)РЛ ДчПЌШї therapeuticРИЗЮ КИДТЕЅ ЙнЧЯПЉ, МОчЛчЖїЕщРК РЬИІ РЬЧиЧЯСі ИјЧЯАэ РжДТ НЧСЄРдДЯДй.

Udagawa МБЛ§ДдРК "We should find out the way to survive, ourselves!"ЖѓДТ РЮЛѓРћРЮ ЙЎБИЗЮ АРЧИІ ИЖУЦНРДЯДй.
* МПяДыЧаБГ СЖМЎБт МБЛ§Дд comment: (1) Extensive surgery ШФПЁДТ ШИКЙРЬ ДЪБт ИЖЗУРЬЙЧЗЮ ШЏРк ИИСЗЕЕАЁ ЖГОюСњ Мі РжНРДЯДй. ДыЧбЙЮБЙ СЄКЮПЁМДТ hospital lengthИІ СйРЬЗСДТ ГыЗТРЛ ЧЯАэ РжНРДЯДй. (2) МПяДыЧаБГПЁМЕЕ chemoRTРЧ УЪБт МКРћРЬ СССі ОЪОвНРДЯДй. РЬШФ АцЧшРЬ НзРЬИщМ МКРћРЬ ССОЦСГНРДЯДй. РЯКЛАњ МОчРЧ СЂБйЙ§РЛ КёБГЧв ЖЇ РЬЗЏЧб СЁРЬ АэЗСЕЧОюОп Чв АЭ ААНРДЯДй.
* Christopher Hayden Crane МБЛ§Дд (Memorial Sloan Kettering Cancer Cancer)comment: МОчРЧ РгЛѓПЌБИПЁМ surgical specimenРЧ margin positive rate 40%, local recurrence 30%РдДЯДй. РЯКЛРК ОюЖВАЁПф?
→ Udagawa МБЛ§Дд ДфКЏ: РЯКЛПЁМ margin positive rateДТ 5%РдДЯДй. Radial margin positiveДТ preoperative diagnosisАЁ РпИјЕШ АЭРЬСіПф.
![]() 2. Indication of neoadjuvant treatment (МПяОЦЛъКДПј СООчГЛАњ ЙкМїЗУ)
2. Indication of neoadjuvant treatment (МПяОЦЛъКДПј СООчГЛАњ ЙкМїЗУ)
НФЕЕОЯРК ПЉРќШї ФЁИэРћРЮ СњКДРдДЯДй. 2011Гт ПьИЎГЊЖѓ РкЗсПЁ РЧЧЯИщ ЛѕЗЮ ЙпЛ§Чб ШЏРк ДыКё ЛчИСРк КёРВРК 67%РдДЯДй.
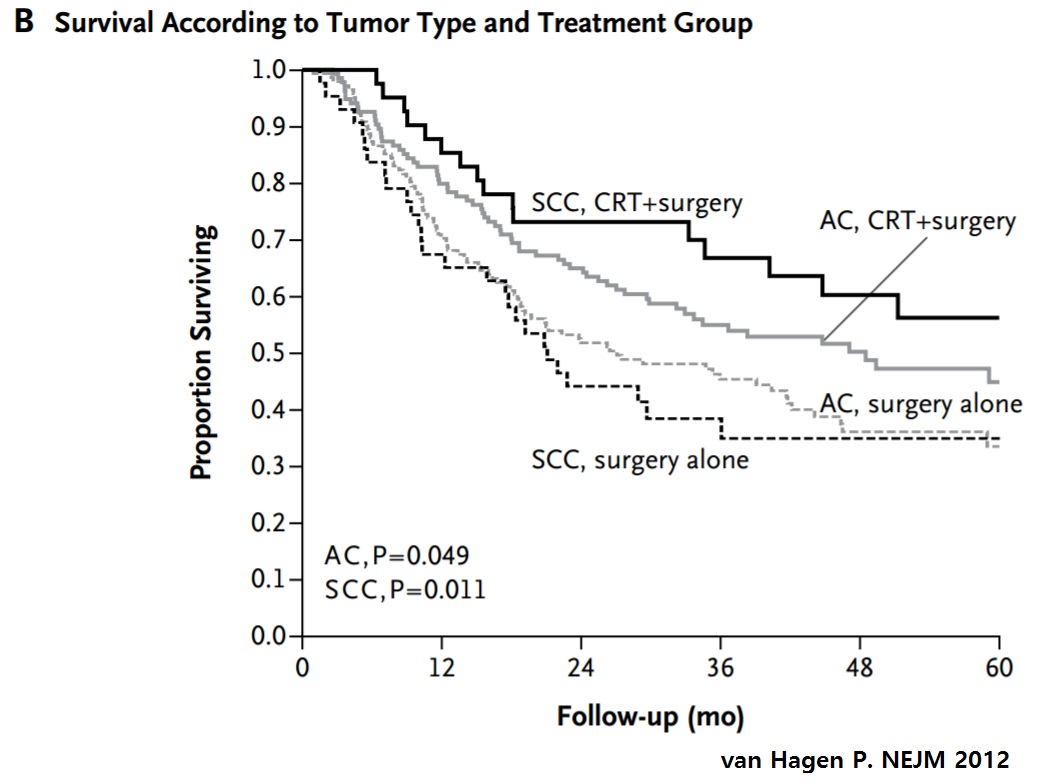
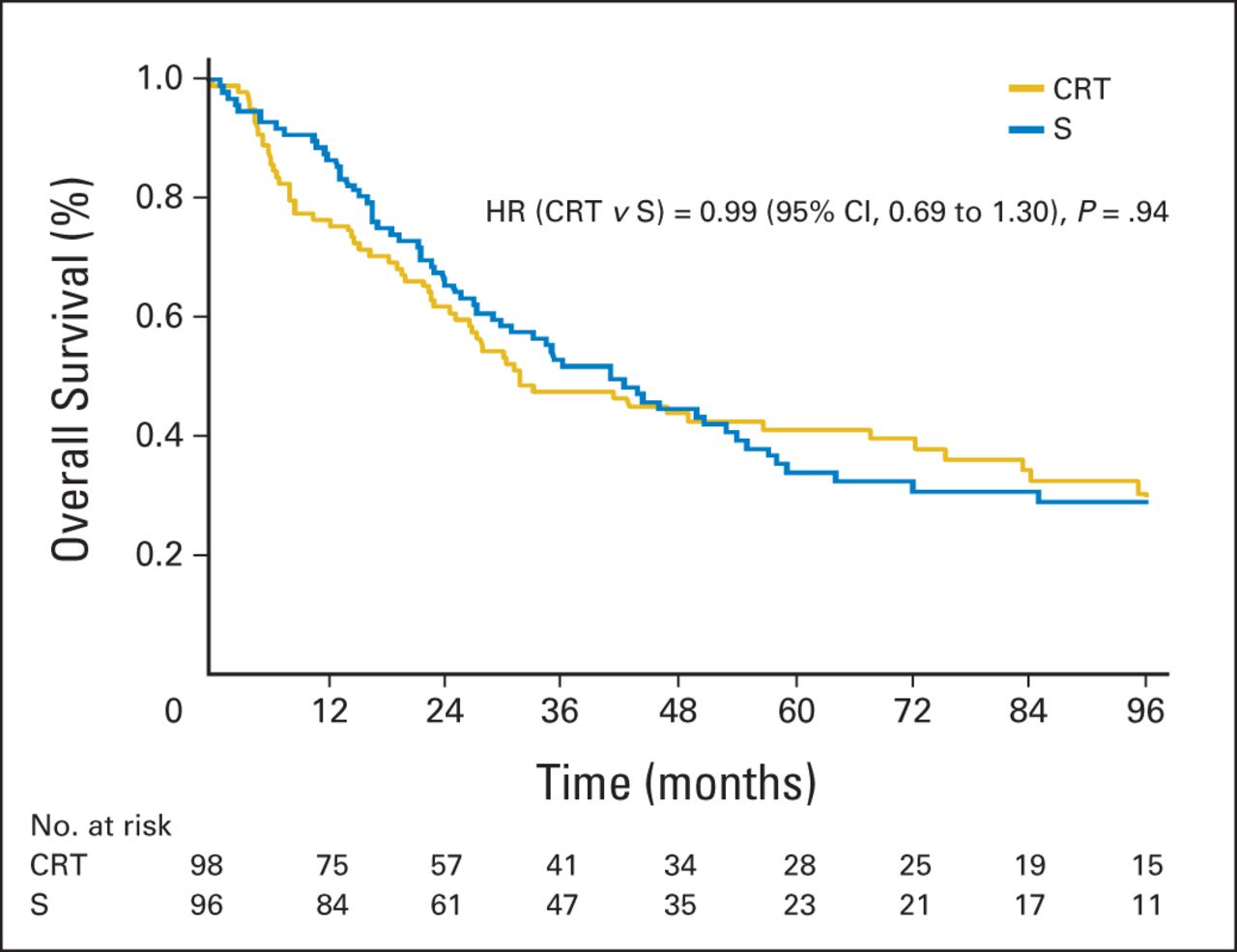
Neoadjuvant chemoRTРЧ ШПАњ: КИДй advanced stage ШЏРкИІ ДыЛѓРИЗЮ Чб CROSS ПЌБИДТ neoadjuvant stageПЁ ДыЧб positive resultИІ КИПДНРДЯДй (van Hagen P. NEJM 2012). ЛѓДыРћРИЗЮ less advanced stage ШЏРкИІ ДыЛѓРИЗЮ Чб FFCD 9901 ПЌБИ (Mariette. JCO 2014)ДТ negative resultИІ КИПДНРДЯДй.
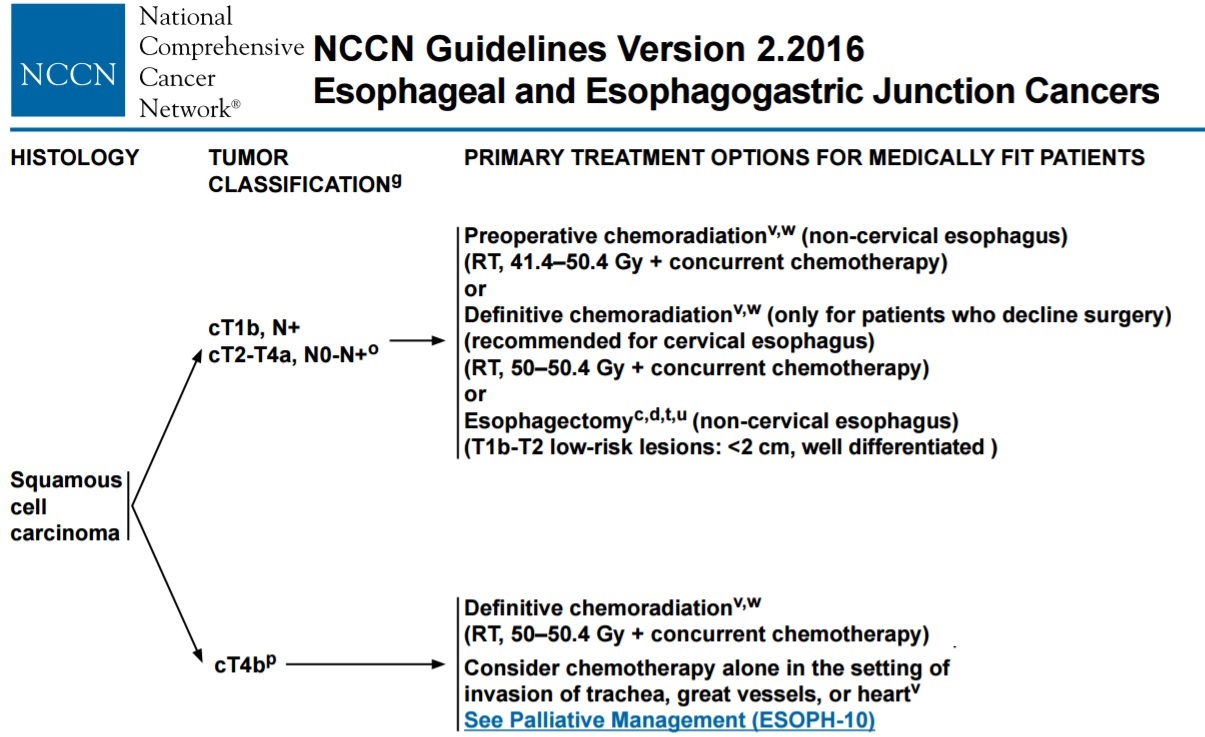
NCCN guideline 2016ПЁДТ cT1bN+M0 ЖЧДТ cT2-T4aN0N+M0ПЁМ preoperative chemoRTИІ БЧЧЯАэ РжНРДЯДй. Ся submucosal cancerПЁМ LNОчМКРЮ АцПьПЭ LNПЭ ЙЋАќЧЯАд НЩДоЕЕАЁ proper muscle РЬЛѓРЮ АцПьДТ preoperative chemoRTИІ БЧЧбДйДТ АЭРдДЯДй.
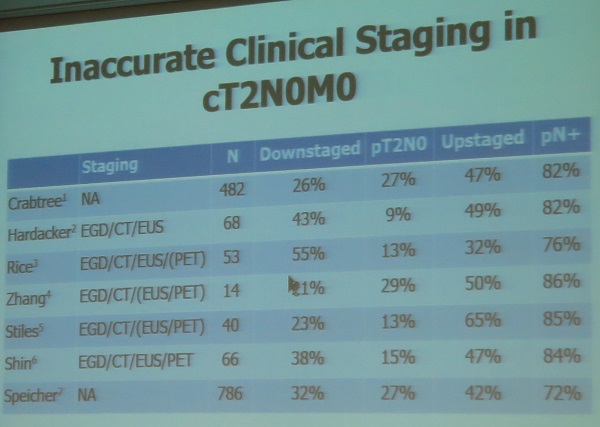
БзЗЏГЊ cT2N0M0ПЁ ДыЧб ФЁЗс ЙцФЇРК NCCN guidelineАњ ДйИЃАд СЂБйЕЧДТ АцПьАЁ ИЙНРДЯДй. cT2N0M0РЧ clinical stagingРЬ БзИЎ СЄШЎЧЯСі ОЪДйДТ СЁЕЕ ЙЎСІРдДЯДй. Understaging ЕШ ШЏРкИІ Рп АэИІ Мі РжОюОп ССРК АсАњИІ ГО Мі РжНРДЯДй.
While some sudies have advocated for the use of preoperative therapy due to a high incidence of nodal dieases detected after resection (Zhang JQ. Ann Thorac Surg 2012), other studies have questioned whether preoperative therapy improves survival (Speicher PJ. J Thorac Oncol 2014). cT2N0M0РЧ preoperative chemoRTРЧ toxicityИІ АэЗСЧв ЖЇ, cT2N0M0ДТ preoperative chemoRT ОјРЬ ЙйЗЮ МіМњРЛ НУЧрЧв Мі РжДйАэ Л§АЂЕЫДЯДй.
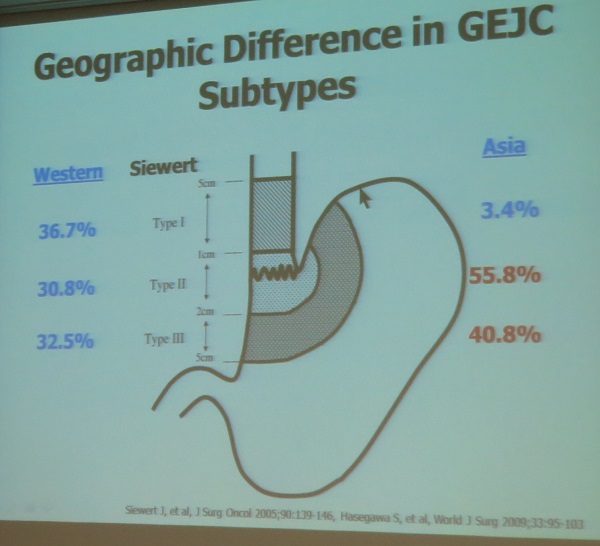
GE junction cancerИІ НФЕЕОЯУГЗГ ФЁЗсЧв АЭРЮАЁ, РЇОЯУГЗГ ФЁЗсЧв АЭРЮСі ГэЖѕРдДЯДй. ЕПМОчРЧ СЖСїЧќ ТїРЬАЁ ХЎДЯДй.
![]() 3. Pre-treatment and post-treatment staging of esophageal cancer (ЛяМКМПяКДПј ПЕЛѓРЧЧаШ БшХТСЄ)
3. Pre-treatment and post-treatment staging of esophageal cancer (ЛяМКМПяКДПј ПЕЛѓРЧЧаШ БшХТСЄ)
ЦѓОЯРК ГЛГтКЮХЭ 8ЦЧРЬ ЛчПыЕЩ ПЙСЄРЮЕЅ НФЕЕОЯРК О№СІ 8ЦЧРЬ ГЊПУСі И№ИЈДЯДй. ЕћЖѓМ НФЕЕОЯПЁМДТ ДчКаАЃ 7ЦЧРЬ ЛчПыЕЩ АЭРдДЯДй. 7ЦЧРЧ ЦЏТЁРК histologic gradingРЬ T stagingПЁ ПЕЧтРЛ СиДйДТ СЁРдДЯДй. N stagingДТ АЙМіЗЮ ДмМјЧиСГДТЕЅ, 1-2АГИщ N1, 3-4АГДТ N2РдДЯДй.
![]() 4. Esophagectomy after neoadjuvant chemoRT (МПяОЦЛъКДПј ШфКЮПмАњ БшПыШё)
4. Esophagectomy after neoadjuvant chemoRT (МПяОЦЛъКДПј ШфКЮПмАњ БшПыШё)
ОЦЛъКДПјПЁМДТ cT1-2N0ДТ МіМњ, cT3/4N+ДТ neoadjuvant chemoRTРЛ ЧЯАэ РжНРДЯДй.
CCRTПЁ ЙнРРРЬ ССРИИщ МіМњРЛ ДѕЧЯСі ОЪАэ CCRTИІ АшМгЧЯДТ АЭРЬ ССДйДТ ПЌБИАЁ РжНРДЯДйИИ, ОЦЛъКДПјРЧ РкЗсПЁ РЧЧЯИщ CCRT ШФ МіМњЧб ШЏРкАЁ CCRT ДмЕЖКИДй survivalРЬ ССОвНРДЯДй.
Time interval of esophagectomy/CCRT: The operation is usually performed 4 to 8 weeks after CCRT when the patient has fully recoverd. Longer waiting may increase the rate of pathologic complete reponses and may improve survival.
РЬСиЧр СњЙЎ. Clinically T2N0 ЗЮ ЦђАЁЕЧОю initially surgeryИІ ЧпДј ШЏРкРЧ postop lymph node stagingРК ОюЖАЧЯПДДТСіПф?
![]() 5. Neoadjuvant therapy followed by surgery in locally advanced resectable esophageal cancer (ЛяМКМПяКДПј ПРЕПЗФ)
5. Neoadjuvant therapy followed by surgery in locally advanced resectable esophageal cancer (ЛяМКМПяКДПј ПРЕПЗФ)
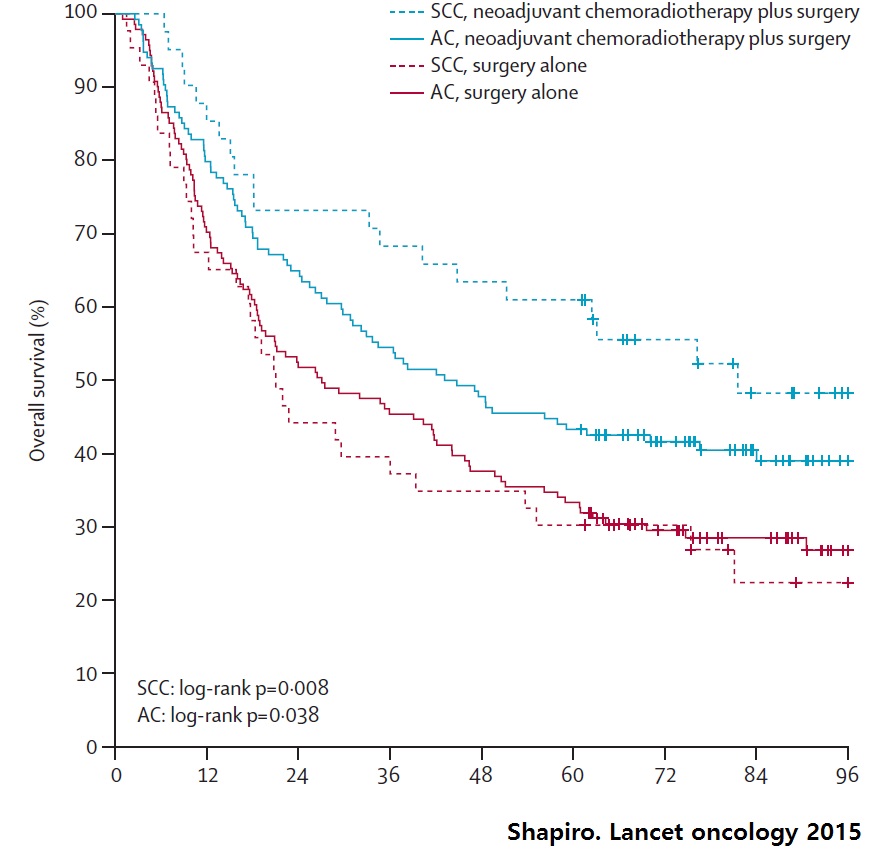
CROSS trialРЧ longterm dataАЁ 2015Гт ЙпЧЅЕЧОњДТЕЅ АњАХ РкЗсИІ ШЎРЮЧЯДТ МіСиРЬОњНРДЯДй (Shapiro. Lancet oncology 2015).
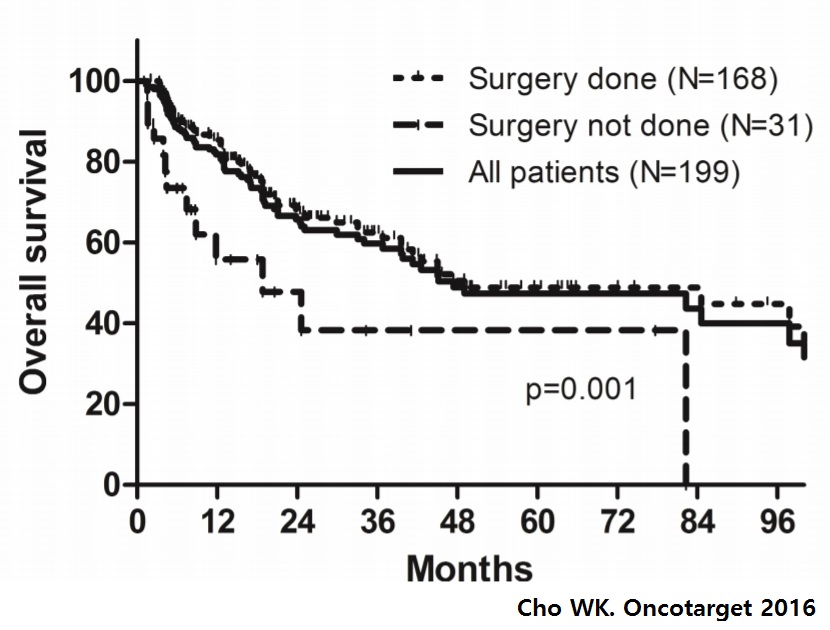
ОЦЗЁДТ neoadjuvant chemoRT ЙоРК ЛяМКМПяКДПј ШЏРкРЧ УжБй АсАњРдДЯДй (Cho WK. Oncotarget 2016). ДчПЌЧб РЬОпБтАкСіИИ МіМњЙоРК ШЏРкРЧ Л§СИРВРЬ Дѕ ССОвНРДЯДй. ЙАЗа МіМњЙоСі ОЪРК ШЏРкПЁМЕЕ РЯСЄ КЮКа longterm survival ПЙАЁ РжНРДЯДй.
ОЦСїБюСіДТ neoadjuvant chemotherapy ШФ CRРЬ ПдДѕЖѓЕЕ МіМњРЛ ЧЯДТ АЭРЬ ЧЅСиРЬЖѓАэ Л§АЂЕЫДЯДй.
![]() 5. PD-1/PD-L1 inhibitor therapy for locally advanced esophageal cancer. (ЛяМКМПяКДПј ЧїОзСООчГЛАњ МБСОЙЋ. 2000Гт МПяРЧДы СЙОї)
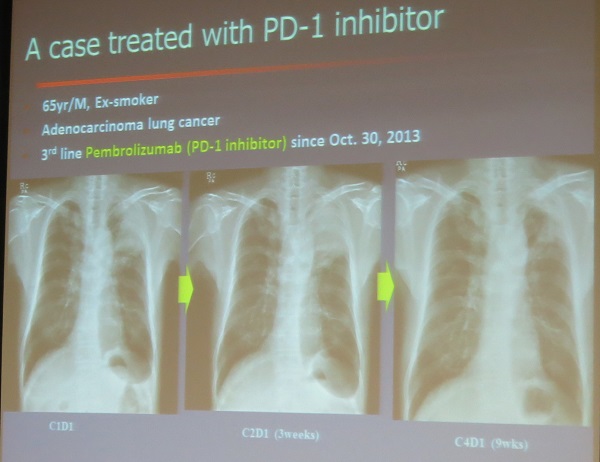
5. PD-1/PD-L1 inhibitor therapy for locally advanced esophageal cancer. (ЛяМКМПяКДПј ЧїОзСООчГЛАњ МБСОЙЋ. 2000Гт МПяРЧДы СЙОї)
Pembrolizumab (PD-1 inhibitor) ЛчПы ШФ ЧіРњШї ШЃРќЕШ ЦѓОЯ (adenocarcinoma) СѕЗЪИІ КИПЉСжОњНРДЯДй. ИХПь СЖПыЧб ФЁЗсЖѓАэ ЧЯМЬНРДЯДй. КЮРлПыРЬ АХРЧ ОјБт ЖЇЙЎРдДЯДй.
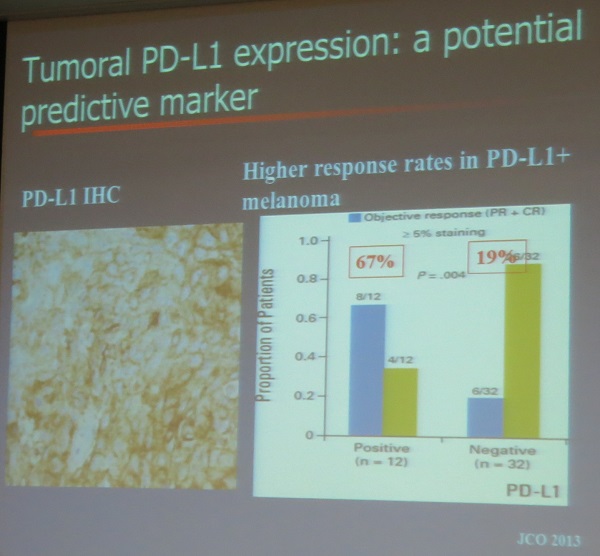
MelanomaПЁМ PD-L1 immunohistochemistry ОчМКРЬИщ response rateАЁ 67%РЮ ЙнИщ РНМКПЁМЕЕ response rateАЁ 19%РЬЙЧЗЮ АњПЌ РЬИІ predictive markerЖѓАэ Чв Мі РжРЛСі ОЦСї ГэЖѕРдДЯДй.
![]() 7. Neoadjuvant CCRT for locally advanced esophageal cancer. Christopher Haydon Crane (Memorial SLoan Kettering Cancer Center)
7. Neoadjuvant CCRT for locally advanced esophageal cancer. Christopher Haydon Crane (Memorial SLoan Kettering Cancer Center)
ChemoRTДТ margin negative resection rateИІ ПУИГДЯДй.
КДМв РЇФЁПЁ ЕћЖѓ margin positive rateПЁ ТїРЬАЁ РжНРДЯДй. ЛѓКЮНФЕЕПЁМДТ margin positive rateАЁ ГєНРДЯДй.
Cardiopulmonary complicationРЛ СйРЬБт РЇЧЯПЉ dose deliveryАЁ ССОЦОп ЧеДЯДй.
* Udagawa МБЛ§Дд СњЙЎПЁ ДыЧб ПЌРкРЧ ДфКЏ: ЙЬБЙРЧ R0 resection rateАЁ ГЗРК РЬРЏПЁ ДыЧЯПЉ ПЌРкДТ (1) ЙЬБЙПЁДТ ЧбБЙ, РЯКЛ, СпБЙАњ ААРК high volume centerАЁ ОјДйДТ СЁ, (2) ЙЬБЙ ШЏРкЕщРК obesityАЁ ИЙДйДТ СЁРЛ ЕщОњНРДЯДй. → РЬПЁ ДыЧЯПЉ СТРх ОШПыТљ МБЛ§ДдРК (3) РЯКЛ surgeonРЬ ИХПь aggressiveЧЯДйДТ СЁРЬ ХЋ ТїРЬИІ ИИЕчДйАэ comment ЧЯПДНРДЯДй.
* FloorРЧ Чб МБЛ§Дд comment: CROSS trialРК ШЏРкАЁ РўАэ АЧАЧб ЦэРЬОњНРДЯДй. ПьИЎ ШЏРкЕщАњ ЛѓДчШї ДйИЈДЯДй.
![]() 8. Esophageal cancer in Korea
8. Esophageal cancer in Korea
ПьИЎГЊЖѓПЁМ НФЕЕОЯРК И№Еч ОЯРЧ 1% СЄЕЕИІ ТїСіЧЯАэ РжНРДЯДй. ИХГт 1,400ИэРЬ НФЕЕОЯРИЗЮ ЛчИСЧеДЯДй. НФЕЕОЯ МіМњПЙДТ 2014ГтРЧ АцПь РќБЙРћРИЗЮ 414ИэРЬОњНРДЯДй (РЬ Сп 62.8%РЮ 260ИэРЬ ЛяМКМПяКДПјПЁМ МіМњРЛ ЙоОвРН).
1994ГтКЮХЭ 2014ГтБюСі ЛяМКМПяКДПјПЁМ НФЕЕОЯ МіМњРК 1,538ПЙАЁ РжОњНРДЯДй. Mean ageДТ 63.3ММ, ГВРк 93%, 2-FLND 85% & 3-FLND 10%, Median hospital stay 12РЯ, 30 day mortality 0.8%ПДНРДЯДй. Squamous cell carcinoma, primary surgery, R0 resectionРЧ АцПь 5Гт Л§СИРВРК 64.7%ПДНРДЯДй (1Бт 82.7%, 2Бт 63.5%, 3Бт 41.2%, 4Бт 46.9%).
![]() [References]
[References]
© РЯПјГЛНУАцБГНЧ ЙйИЅГЛНУАцПЌБИМв РЬСиЧр. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.