EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [일본위암학회 2017]
[일본위암학회 2017]
2017-3-9. 날씨마저 우중충하였습니다.
17년만에 히로시마(廣島)에 왔습니다. 사실 17년 전 목적지는 히로시마가 아니고 쿠레(吳)였습니다. 쿠레 교사이 병원의 doctor 우에무라(上村)의 내시경실에서 10일 정도 견학을 했습니다 (EndoTODAY 이준행의 좌충우돌 내시경 배우기). 군의관을 마치고 fellow 생활을 시작하기 전이었습니다. 나중에 NEJM에 헬리코박터 관련 논문(Uemura N. NEJM 2001)을 발표하여 유명해진 그 우메무라 선생님입니다.
1999년 12월 헬리코박터 학회에서 우에무라 선생님의 특강을 인상깊게 들었습니다. 자신의 외래를 찾은 환자의 내시경을 하면서 헬리코박터 관련 자료를 꾸준히 모아서 일본에서 가장 큰 데이타베이스를 만드셨다고 합니다. 동경도 아니고, 히로시마도 아니고, 쿠레라는 작은 도시(군항입니다. 우리나라로 말하면 진해 정도 됩니다. 사실 진해는 쿠레를 모델로 일본인들이 만든 도시입니다)의 그것도 가장 큰 병원도 아닌 세번째 규모의 병원에서 말입니다. '일본에는 시골 고수가 많다더니 바로 이분이구나' 생각이 들었습니다. 전화를 했습니다. 당시에는 e-mail이란 것이 없었으니... 전화로 당신네 병원을 10일 정도 방문하고 싶으니 허락해 달라고 요청했습니다. 당돌했지요. 그런데 대답은 흔쾌히 OK. 나중에 알고보니 쿠레 쿄사이 병원 내시경실을 방문한 첫번째 외국인이라고 하셨습니다. 그래서였는지, 버스 터미날까지 직접 마중을 나오셨고, 병원 숙소에 묵도록 허락해 주셨고, 선생님 댁에 초대하여 근사한 저녁 식사를 대접해주시기도 했습니다. 참 많이 배웠습니다. 환자 자료를 모으고 정리하여 그로부터 배워야 한다는 것을 우에무라 선생님으로부터 배웠습니다.
히로시마를 생각하면 제국주의 일본과 그들의 '희생자 코스프레'가 떠올라 불편합니다. 물론 일본 제국주의가 밉지 일본인 개개인을 미워하는 것은 아닙니다. 사이 좋게 지내는 일본인 의사도 여럿 있습니다. 참 좋은 사람들입니다. 그래도 히로시마에서는 기분이 좋지 않았습니다. 관광 없이 공부만 하고 돌아왔습니다. 저는 학회에서 질문하는 것을 즐기는 편입니다. 그러나 이번에는 질문을 하나도 하지 않고 조용히 듣다 왔습니다. 질문할 기분이 아니었습니다. 짧은 강의 하나가 전부였습니다.
제국주의 잔재인 히로시마의 큰 길에 평화의 길이라는 이름을 붙이다니... '참회의 길' 정도가 더 어울리지 않을까 싶습니다.
최근 일본은 아주 잘 나가고 있습니다. 경기가 너무 좋아 수습하지 못할 지경이라고 합니다. 이래저래 일본을 따라잡지 못한 것이 안타까울 뿐입니다. 그나마 탄핵이 잘 되어 다행입니다.
매우 일본적인 학회 포스터를 보았습니다. 스토푸 위암^^ 내시경을 사무라이 칼처럼 휘두르고 있습니다.
![]() 1. Inflammation and carcinogenesis (2017-3-9. 8:30am)
1. Inflammation and carcinogenesis (2017-3-9. 8:30am)
1) Role of H. pylori CagA oncoprotein in gastric carcinogensis (Masanori Hatakeyama, University of Tokyo)
WHO에서 위암의 80%가 헬리코박터 때문이라고 발표하였지만, 일본에서는 80%는 상당히 underestimation된 숫자로 생각한다. 실제로 헬리코박터 음성 위암은 매우 드물다.
Two major isoforms of the H. pylori CagA protein. (Hatakeyama. Nat Rev Cancer 2004) Western EPIYA region은 ABC로 구성 (C segment multiple일 수 있음. Single C에서는 암이 안 생기지만 multiple C에서는 암이 발생할 수 있다), Eastern EPIYA region은 ABD로 구성되어 있다 (D segment는 항상 1개).
Tyrosine phosphorylation of cytotoxin-associated antigen A (CagA) by SRC kinase occurs at the EPIYA motif. There are four different EPIYA sites, called EPIYA-A, -B, -C and -D, based on the sequence surrounding the EPIYA motif. Western strains of Helicobacter pylori express a form of CagA that contains the EPIYA-A and EPIYA-B sites, followed by 1-3 repeats of the 34-amino-acid sequence that contains the EPIYA-C site (red boxes). East-Asian strains of H. pylori express a form of CagA in which the EPIYA-C site is replaced with the EPIYA-D site (yellow box). (Hatakeyama. Nat Rev Cancer 2004)
Three dimensional structure of the H. pylori Cag A protein (Hayashi T. Cell Host Microbe 2012) - Solid region (70%, N-terminal)과 intrisically disoredered resion (30%, C-terminal tail) 으로 구성되어 있다.
The Helicobacter pylori type IV secretion effector CagA is a major bacterial virulence determinant and critical for gastric carcinogenesis. Upon delivery into gastric epithelial cells, CagA localizes to the inner face of the plasma membrane, where it acts as a pathogenic scaffold/hub that promiscuously recruits host proteins to potentiate oncogenic signaling. We find that CagA comprises a structured N-terminal region and an intrinsically disordered C-terminal region that directs versatile protein interactions. X-ray crystallographic analysis of the N-terminal CagA fragment (residues 1-876) revealed that the region has a structure comprised of three discrete domains. Domain I constitutes a mobile CagA N terminus, while Domain II tethers CagA to the plasma membrane by interacting with membrane phosphatidylserine. Domain III interacts intramolecularly with the intrinsically disordered C-terminal region, and this interaction potentiates the pathogenic scaffold/hub function of CagA. The present work provides a tertiary-structural basis for the pathophysiological/oncogenic action of H. pylori CagA. (Hayashi T. Cell Host Microbe 2012)
SHP2 is mutated in a variety of human cancers. Eastern CagA와 SHP2의 binding site가 많은데 (9개), western CagA와 SHP2와의 binding site는 적다 (4개).
EBV는 epigenetic silencing으로 good guy인 SHP1을 줄인다. Bacteria와 virus가 human body에서 질병발생에 collaboration하는 첫번째 모델이다. (Saju P. Nat Microbiol 2016)
2) Gastric cancer promotion by innate immunity and chronic inflammation (Masnobu Oshima, Kanazawa University)
PGE2/NKFB/STAT3 in intestinal tumorigenesis. (Oshima H. J Gastroenterol 2012)
Inflammatory microenvironment가 carcinogenesis를 촉진시킨다. WNT + PGE2 + bacteria = carcinogenesis
The interaction of the cyclooxygenase-2 (COX-2)/prostaglandin E2 (PGE2), tumor necrosis factor-α (TNF-α)/nuclear factor-κB (NF-κB), and interleukin-6 (IL-6)/gp130/Stat3 pathways in the inflammatory environment. cAMP cyclic AMP, IKK inhibitor of κB kinase, IκB inhibitor of κB, NSAIDs non-steroidal anti-inflammatory drugs (Oshima H. J Gastroenterol 2012)
NOX-1이 stemness 유지에 기여한다.
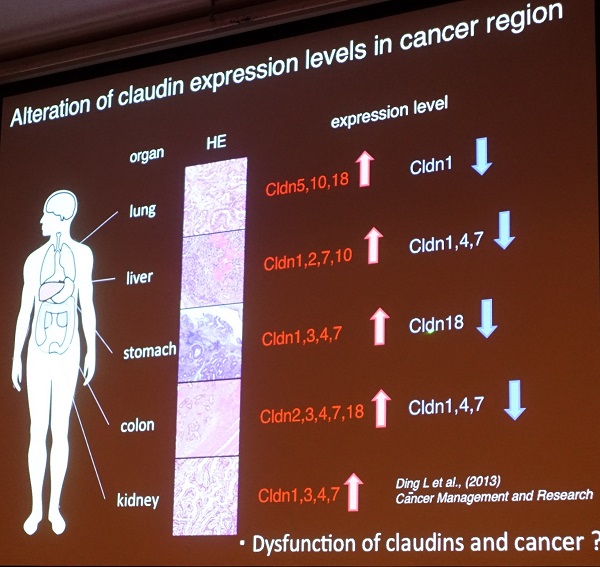
3) Defects in the paracellular barrier function of tight junctions in cancer (Sachiko Tsukita, Osaka University)
Claudins (= TJ adhesion molecule) are classified as (mostly) barrier-type and channel-type. (Suzuki H. Science 2014)
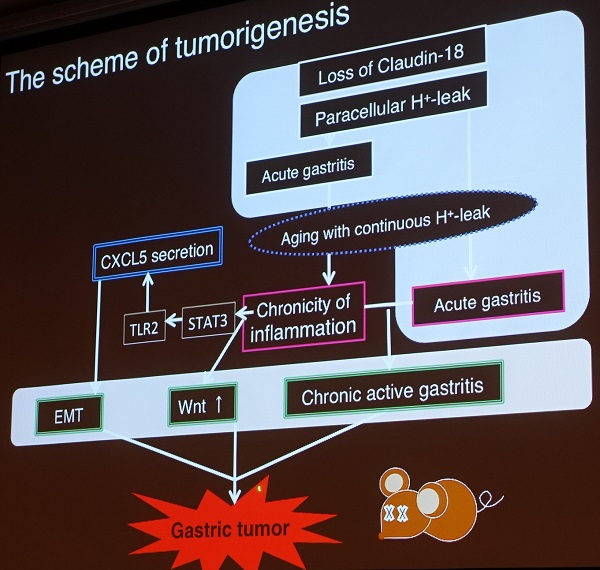
Claudin는 24 종류가 있는데 Claudins-18 이 stomach에 specific하다. stCld18-/- mice에서 고령에 만성염증이 발생한다. 이 과정에서 CXCL5가 중요한 역할을 한다.
![]() 2. Oral presentation session: EGC (2017-3-9. 10:30am, chairperson H ono, 한상욱)
2. Oral presentation session: EGC (2017-3-9. 10:30am, chairperson H ono, 한상욱)
1) OE3-1. ESD using a diode laser system with 3-D printer endoscopic clip (조주영): 새롭게 개발된 laser device를 이용한 ESD를 멋지게 보여주셨습니다. Circumferential cutting, submucosal dissection, bleeding control을 한 catheter를 이용하여 시행할 수 있었습니다. Laser system으로는 submucosal fibrosis가 있는 부분은 ablation을 할 수 있다고 합니다.
조주영 교수님께서 직접 발표하셨습니다. 수고 많으셨습니다.
2) OE3-2. Gastrectomy after ESD (Jaymei Ramos Castilio, Kyushu University) : ESD 후 수술 한 환자 45명. 평균 크기 2.13 cm. 평균 36 림프절을 박리함. Residual tumor는 22% 였음 (3명에서 lymph node 전이가 있었음).
3) OE3-2. Efficacy and safety of gastric endoscopic submucosal dissection under general anesthesia (Tstsuya Ueo, Oita University) : General anesthesia를 적용한 기준 3개를 보여주었습니다.
4) OE3-4. Effect of hospital volume on outcome after ESD (Dohi. Kyoto Preferctural University): 19 institutions, 2526명 (1년에 ESD 100개 이하면 low volume, 100-200을 high volume, 200 이상의 very high volume이라고 정의). Lymphatic invasion은 high volume center에서 많았지만, overall survival은 low volume center에서 좋지 못했습니다. (좌장 Ono 선생님은 "작은 병원에서 overall survival이 나쁜 것은 over-treatment 아닌가?"라고 comment 하였습니다.)
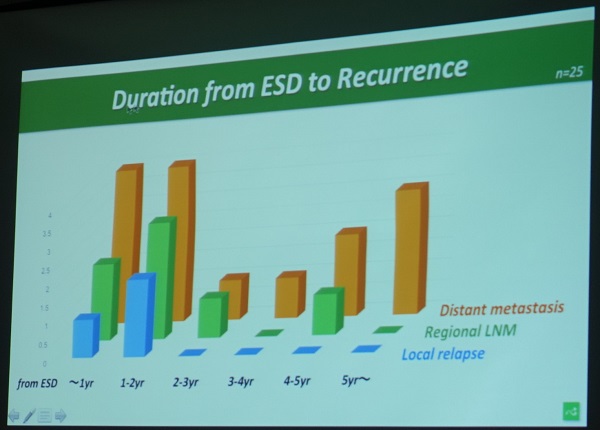
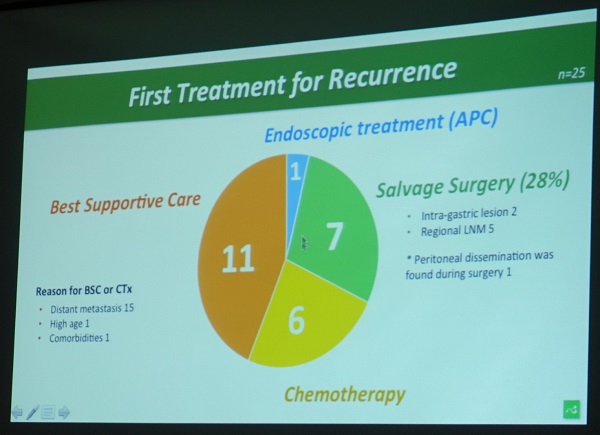
5) OE3-5. Can be the patient with non-curative ESD for gastric cancer rescued by surgery after recurrence? (Kohei Takizawa): 905명 중 60%를 평균 64개월 동안 추적관찰하였을 때 27명이 재발하였는데 60%는 원격전이였습니다. 5명을 수술할 수 있었는데 1명만 longterm survival이 가능하였습니다.
6) OE3-6. Effect of steroid use to prevent stenosis after widespread ESD (Kishida. Shizuoka Cancer Center). Steroid 사용 group에서 stenosis가 약간 늦게 발생하였기는 하지만 전체적인 발생률은 차이가 없었습니다.
![]() 3. Diagnosis and treatment of EG junction cancer (14:00-16:30)
3. Diagnosis and treatment of EG junction cancer (14:00-16:30)
흥미로웠습니다. 몇 년 전 동일 주제로 열렸던 심포지엄에 비하여 훨씬 심도있는 발표와 토론이었습니다. 많은 multicenter study, prospective study가 있었기 때문으로 보입니다.
1) Detection of early EGJ cancer and indications for endoscopic therapy (Junko Fujisaki, Cancer Institute Hospital)
ESD로 치료한 85 cardia cancer와 61 Barrett adenocarcinoma를 분석하였습니다 (Osumi H. Gastric Cancer 2016). Barrett adenocarcinoma는 elevated lesion인 경우가 더 많았습니다.
2) Nationwide retrospective study of lymphadenectomy for EGJ cancer (Hiroharu Yamashita, University of Tokyo)
일본에서는 Siewart 분류 대신 Nishi 분류가 사용됩니다. EG junction 부터 상방 2cm와 하방 2cm까지만을 EG junction cancer라고 부릅니다.
Nishi 분류에 의한 EG junction cancer라고 하면 그 위치는 같은데 SCC와 adenocarcinoma의 림프절 전이가 다른가?
Esophagus predominant cancer와 stomach predominent cancer로 나누고 SCC와 adenocarcinoma로 나누어 분석하였습니다. 그러나 실제 임상 례들을 분석해보면 Esophagectomy, proximal gastrectomy, total gastrectomy로 나누어집니다. (Yamashita H. Gastric cancer 2017)

연자는 4 cm 이하의 EGJ cancer에 대해서는 total gastrectomy는 필요하지 않을 것 같다. 그러나 lymph node dissection은 열심히 해야 한다고 주장하였습니다. (참고: Rates of lymph node metastasis at each station according to esophaguspredominant cancer (a) and stomach-predominant cancer (b))
3) Nationwide prospective study to investigate the metastatic rates of lymph nodes in EGJ cancer (Yukinori Kurokawa, Osaka University)
식도 침윤이 3cm 미만인 adenocarcinoma를 transhiatal approach와 thoracic approcah를 하였던 연구의 Final analysis : Kurokawa. Br J Surg 2015
Kaplan-Meier curves of overall survival in patients with a Siewert type II and b Siewert type III tumours by treatment group. TH, transhiatal approach; LTA, left thoracoabdominal approach. a Hazard ratio (HR) 1·19 (95 per cent c.i. 0.72 to 1.95; P=0.496, 2-sided log rank test); b HR 1·67 (0·90 to 3.11; P=0.102, 2-sided log rank test) (Kurokawa. Br J Surg 2015)
Squamous cell cariconoma의 경우는 length of esophageal invasion이 별 영향을 주지 않지만 adenocarcinoma의 경우 length of esophageal invasion이 중요하였습니다. 3 cm가 넘으면 upper mediastinal node 전이가 급격히 증가하였습니다.
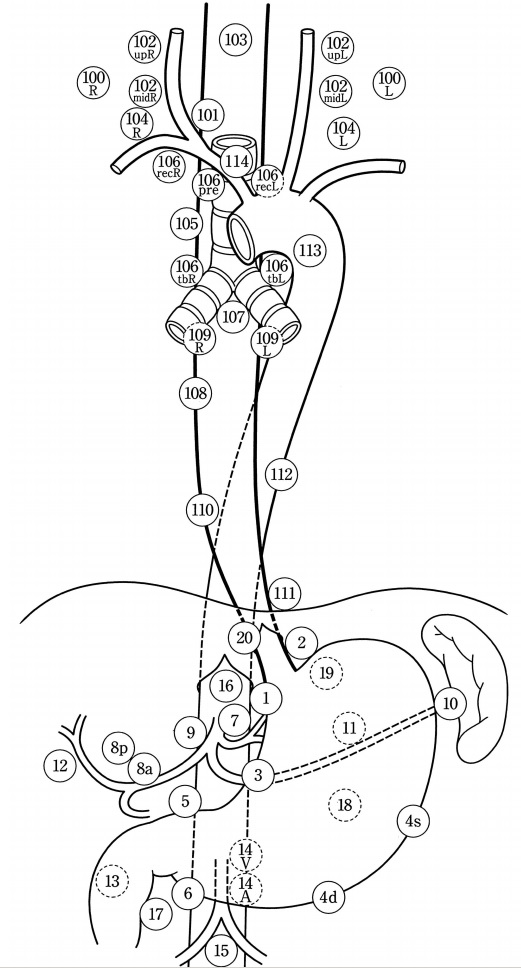
일본 식도질환학회 림프절 명명법 (Esophagus 2004;1:61-88)
[Panel discussion]
좌장이신 Yasuyuki Seto 선생님은 EG junction adenocarcinoma는 다른 곳의 gastric cancer와 상당히 다른데 비하여, SCC는 EG junction에 위치하더라도 다른 곳에 위치한 SCC와 비슷하므로 EG junction cancer에서 SCC는 빠지는 것이 어떠한가 의견을 냈습니다.
Yamashita 선생님은 jejunal interposition과 double tract reconstruction이라는 두 가지 방법이 있는데 어떤 것이 더 좋을지 논의가 있었습니다. 술기 면에서는 jejunal interposition이 더 어려운 모양입니다. Floor에서 어떤 선생님이 술기의 선택은 의사의 철학에 달렸다고 말하였습니다. 모든 음식이 위를 지나가야 한다고 생각하면 jejunal interposition을 선택하는 것이고 그렇지 않다면 double tract reconstruction을 하는 것이라고 하십니다.
마침 포스터 중 jejunal interposition 도해가 있어서 옮깁니다.
Floor에서 박도준 선생님은 total gastrectomy 후 double tract reconstruction을 할 때에도 중력때문에 당겨져서 문제가 발생하는데, 식도에서 anastomosis를 하고 double tract reconstruction을 하면 tension이 더 문제가 될 수 있다고 comment 하셨습니다. Kurokawa 선생님은 stomach을 right crus에 fixation 시킨다고 답하였습니다.
Kurokawa 선생님은 proximal gastrectomy를 하면서 anastomosis site가 흉강이면 double tract reconstruction을 선호하고 anastomosis site가 복강이면 anti-reflux surgery를 추가한다고 합니다.
![]() 4. [3월 10일 금요일 8:30-11:00] Diagnosis and treatment of early gastric cancer - Present and future
4. [3월 10일 금요일 8:30-11:00] Diagnosis and treatment of early gastric cancer - Present and future
1. Progress of diagnostic endoscopy for early gastric carcinoma: 3-D imaging provides precise depth of invasion. Endocytoscopy는 조직검사를 하지 않고 진단할 수 있는 장점이 있습니다.
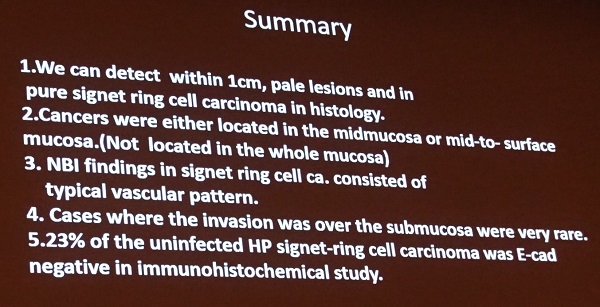
2. Undifferentiated type early gastric cancer during decreasing H. pylori infection. (Junko Fujisaki. Cancer Institute Hospital): 모든 검사 항목을 모두 적용하면 Hp (-) 위암은 0.42% 밖에 되지 않습니다 (Ono. Digestion 2012). Hp (-) 위암은 (1) undifferentiated type adenocarcinoma, (2) fundic gland type adenocarcinoma, (3) hereditary diffuse gastric cancer (HDGC)이 특징입니다. NBI 확대 소견을 이용하면 undifferentiated type adenocarcinoma의 암 분포를 추정할 수있습니다.
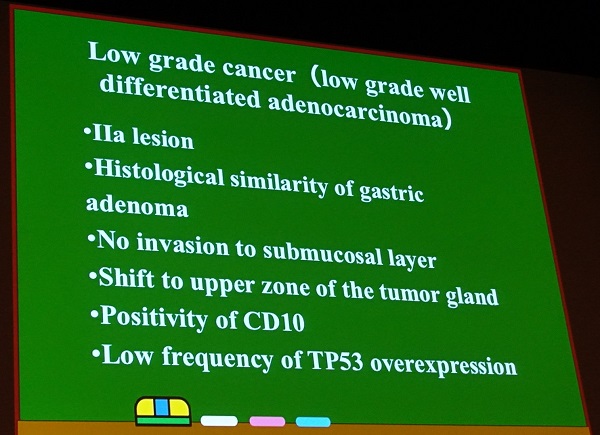
3. Association of endoscopic findings with histological features. Low grade adenocarcinoma는 제 눈으로는 HGD로 보였습니다. 연자도 선종과 low grade adenocarcinoma의 구분은 어렵고 일본 병리의사들 사이에서도 견해차가 있는 영역으로서 molecular finding이 도움될 것이라는 의견을 말했습니다. Hand-shake type gastric cancer라는 생소한 category를 소개하여 주셨습니다.
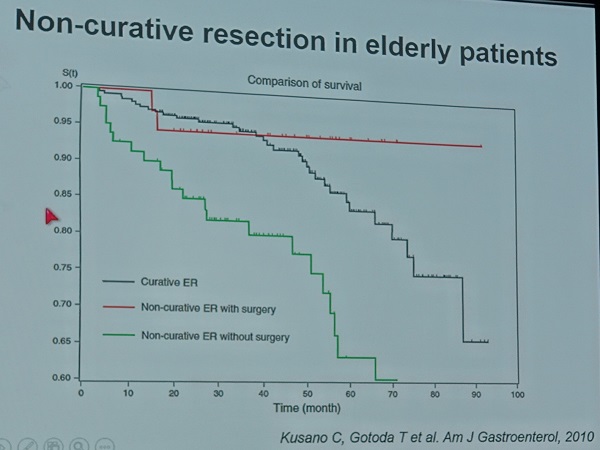
4. Stratified concept of curability after ESD in graying Japanese society. 10년 후에는 위암 환자의 평균 연령이 80은 될 것이라고 합니다. Non-curative ESD 후 수술 받은 환자의 survival은 매우 좋은데 이는 외과의사가 strong한 환자를 잘 선택하였기 때문일 것입니다. Hatta. Am J Gastroenterology (in press) 연자는 고령환자에서 여러 이슈를 모두 가이드라인에 담기 어렵기때문에 자료를 보여주고 환자가 결정할 수 밖에 없을 것 같다고 말했습니다.
Gotoda 선생님의 발표 내용은 2017년 초 Am J Gastroenterol에 발표되었습니다 (Hatta. Am J Gastroenterol 2017).
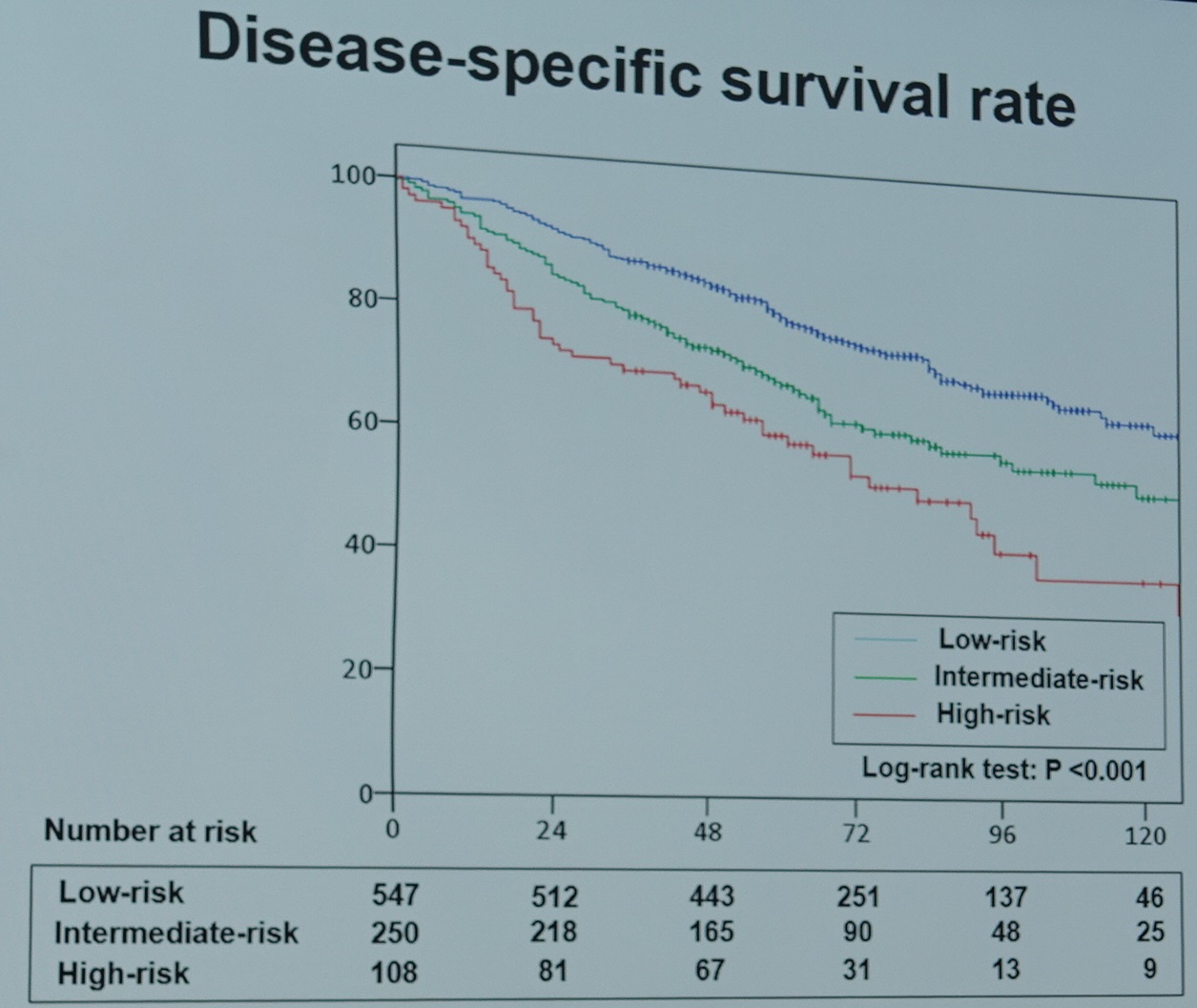
5. Current status of indications for endoscopic resection of EGC. 지금까지 동경암센터에서 10,821 환자를 치료하였고 출혈 4.2%, intraoperative 천공 2.1%, delayed perforation 46 (0.4%), curative resction 82%였습니다. 일본의 registry에 등록된 환자의 최근 결과가 발표되었습니다 (Tanabe. Gastric cancer 2017). 문제는 5년 추적률이 70% 정도라는 것입니다. 2,806명 중 8명 (0.2%)이 위암으로 죽었는데 6명이 metachronous gastric cancer로 사망하였습니다.
Overall survival (Tanabe. Gastric cancer 2017)
Disease specific survival (Tanabe. Gastric cancer 2017)
6. NEWS from U Tokyo
7. Current status of gastric ESD in Korea (Lee Jun Haeng)
![]() 5. Current status of gastric ESD in Korea (Jun Haeng Lee)
5. Current status of gastric ESD in Korea (Jun Haeng Lee)
Thank you chairman for your nice introduction. It’s a great honor for me to talk in this prestigious meeting today.
Topics of my presentation will include various issues of ESD in Korea.
I’d like to start with brief history of gastric ESD in Korea.
As you know, gastric cancer is the most common malignancy in Korea. Recently, the age-adjusted incidence of gastric cancer is slightly decreasing.
One of the most unique aspect of the gastric cancer diagnosis in Korea is that we are doing national screening program since 1999. Starting at the age of 40, all Koreans are recommended to do the biennial gastric cancer screening with endoscopy or barium study. The compliance is slowly increasing, and in a recent review, more than 70% of Koreans are doing gastric cancer screening by the national guideline. The screening modality is endoscopy in 63%.
In the screening program, gastric cancers are usually found in 2 or 3 out of 1,000 endoscopic examinations. 75% of them are early gastric cancers.
Because small EGCs are found more frequently, we are doing more and more endoscopic treatments of EGCs. This is the first small clinical report on endoscopic treatment of early gastric cancer in Korea in 1996. Professor 정현채 performed all the procedures, and I was the first author of that report. At that time, I was a senior resident at Seoul National University Hospital.
After that report, the number of endoscopic resection of EGC increased, so we stated EMR symposium and live demonstration in the year 2006. The picture in the left hand side is the first EMR symposium in Tokyo, Japan, and the right-hand side is the first EMR symposium in Seoul, Korea.
This is one of my early personal experiences of gastric ESDs in 2005. Because endoscopic resection of EGC was not so popular at that time, I carefully explained the difference between surgery and endoscopic resection to the patients.
The hospital stay for gastric ESD was usually 5 to 6 days, but recently it was shortened to 4 day-schedule in most hospitals.
In the year 2011, national medical insurance started to reimburse the cost of gastric ESD after a hot debate between the government and the endoscopy society. Regarding the insurance coverage, there is an important limitation that only the cases in the conventional indications, such as differentiated-type mucosal cancer less than 3 cm, are covered. We are still trying to expand the government indications.
With the increasing need of ESD training for young endoscopists, we are regularly providing hands-on training courses both by the individual institution and by the ESD study group of the Korean Society of GI Endoscopy.
Since a decade ago, some young medical companies in Korea started to develop various endoscopic instruments such as knifes, snares, needles, biopsy forceps, and so on.
ESD knives with water-jet function are also available. It makes the visual field clear during the ESD procedure. Fluid injection into the submucosa layer is also possible without exchanging the instrument.
ESD study group of the Korean Society of GI Endoscopy just started an on-line ESD registry program. Although it is just beginning, we hope this kind of registry data will produce a meaningful result in the near future.
This is the general information about the current status of ESD for EGC in Korea. From November 2011 to December 2014, number of ESD for EGC cases were more than 23 thousands. In the year 2014, 7,734 ESDs were done for Korean EGC cases. The mean age of patients were 65 years and male was 74%. Mean duration of hospital stay was 5 days. Mean medical cost in 2014 was 1,305 US dollars. Surgery was done in 6.6% within 3 months.
One unique aspect of endoscopic treatment of gastric neoplasms in Korea is that the number of gastric adenomas are very high.
This slide shows how we are doing at my institution. Excluding palliative surgeries, we have endoscopically or surgically treated more than seventeen hundred gastric cancers in the year 2012. Among them, 72% were early gastric cancers. In early gastric cancers, cases within absolute indications were 25% and more than 90% of them were treated endoscopically. In this pie graph, you can see 263 adenomas with low grade or high grade dysplasia. All of them were treated endoscopically. Patients with small adenomas, which were treated by endoscopic ablation, were not included in this graph. So, endoscopic treatment of gastric adenoma is a huge workload for Korean endoscopists.
We reviewed the discrepancy between pre-treatment diagnostic groups and post-treatment diagnostic groups in terms of histology, depth of invasion and absolute indications for ESD. As you can see in this slide, the rate of discrepancy is more than expected. When you see the cases with high grade dysplasia in the forceps biopsy, the rate of cancer in the final resected specimen is almost 34%.
I guess you know well about the inter-observer variations in the pathologic diagnosis of early gastric neoplasms. Korean pathologists and Japanese pathologists seem to have different criteria for gastric dysplasia and EGC. This issue is very complex and out of the scope of my presentation. But I want to tell you that we Korean endoscopists are treating a lot of patients with gastric adenomas, and some of them may be considered as well-differentiated gastric adenocarcinomas in Japan.
Because of the discrepancy before and after treatment, I propose the analysis based on the pretreatment diagnostic group.
Practically speaking as an endoscopist, gastric neoplastic lesions can be divided into 6 groups, such as LGD, HGD, AI-EGC, EI-EGC, BEI-EGA and AGC. Diagnostic group classifications before the treatment can be changed after the treatment. The relationship is very complex. So the outcome analysis can be based on either pretreatment diagnostic groups or posttreatment diagnostic groups.
The outcome analysis is usually based on the post-treatment diagnostic groups. In the year 2012, we can say that we performed 111 ESDs for EI-EGCs. In the beginning, however, the diagnosis was one LGD, 12 HGDs, 67 AI-EGCs and 31 EI-EGCs. So, if you analysis 111 post-treatment EI-EGCs, most of them were actually AI-EGCs before the treatment.
This analysis is based on the pre-treatment diagnostic groups. Among 396 pretreatment AI-EGCs, ESD was done for 355 cases. The final diagnoses were variable. As you can see, the post-treatment diagnosis can be actually everything.
This flow diagram shows how we handled absolute indication early gastric cancers by the pretreatment diagnostic groups. This kind of analysis is more realistic. Among 355 early gastric cancers initially treated by ESD, 120 cases, this is 34 percent, belonged to the beyond absolute indication group. Ten percent of patients in the absolute indication group were initially treated by surgery, and you can see the reason in the box at the right hand-side corner. Suspicious lymphadenopathy is the most common reason for surgery. I think this kind of analysis based on the pretreatment diagnostic group has a lot of clinical meanings in the decision making among the treatment options.
This is the treatment modalities for various gastric neoplasms by the pretreatment diagnostic groups. For early gastric cancers in the absolute indications, 90% were initially treated by ESD. Among them, additional surgeries were required in 16 percent. For early gastric cancers beyond absolute indications, 7 percent were initially treated by ESD. Among them, additional surgeries were required in 23%. In general, 20% of all gastric cancers were treated by endoscopy alone in our institution.
Next topic is indications.
Before further discussion, I’d like to make the definitions clear. Indications are different from criteria. Indication is something that we consider before the treatment. Criteria is something we consider after the treatment.
In Korea, ESD candidates are usually selected by the absolute indications. After ESD, expanded criteria is applied to determine whether the resection was curative. There are controversies about the safety of ESD for expanded indication cases. It’s partially because Korean studies consistently showed higher risk of lymph node metastasis in expanded indication cases than Japanese data. I’ll show you some examples.
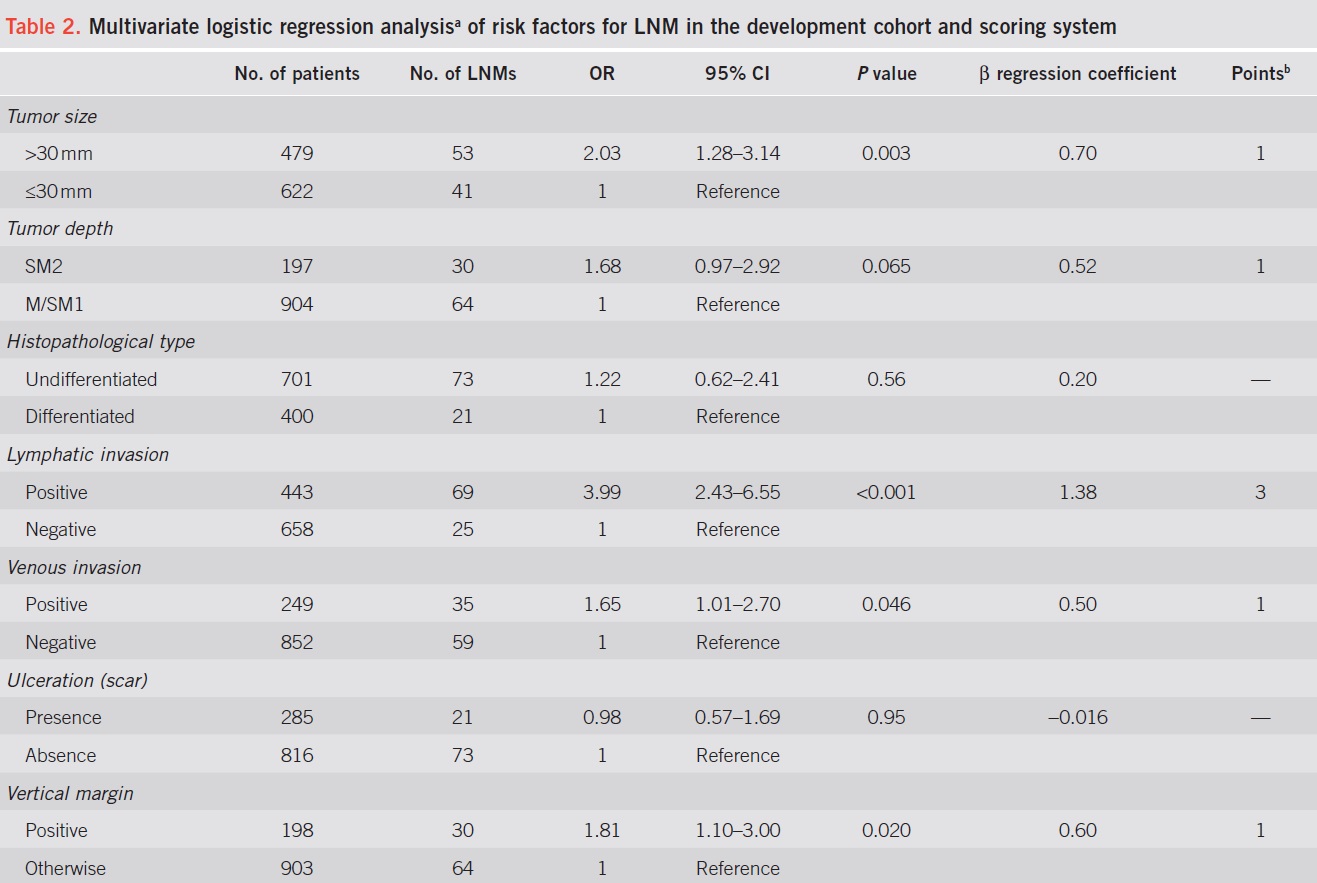
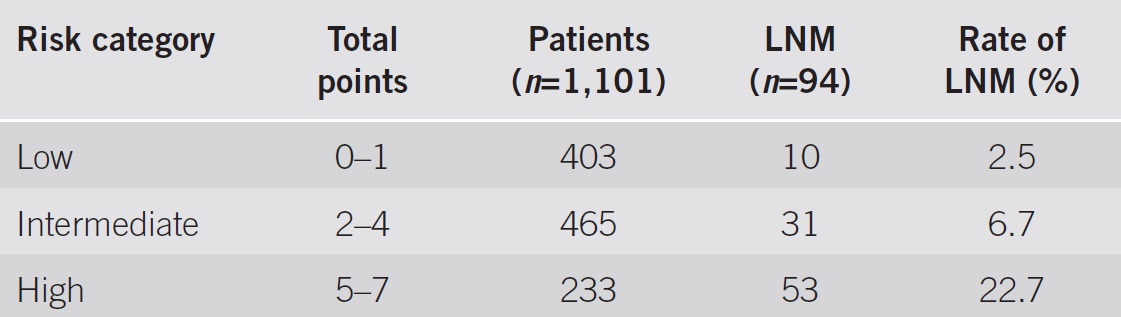
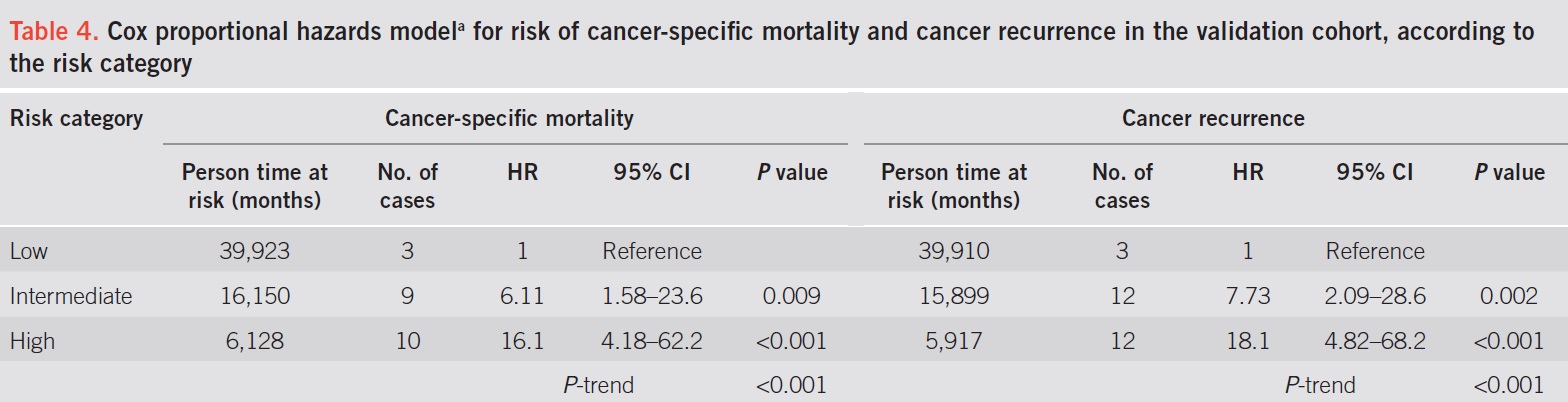
Researchers at Pusan National University examined the risk of LN metastasis in expanded indication cases. As you can see in the table, risk of lymph nod metastasis seems to be slightly higher than the risk in the famous Japanese data by Professor Gotoda.
Researchers at Korean National Cancer Center examined the risk of lymph node metastasis in mucosal EGC meeting the curative resection criteria. As you can see, The risk of lymph node metastasis was about 1 percent.
In my institution, we examined the risk of lymph node metastasis in signet ring cell mucosal EGCs. Actually, the risk was not negligible.
Considering the risk of lymph node metastasis, ESD for expanded indication cases are not regarded as a standard treatment option, but selectively performed in the individual cases basis in Korea.
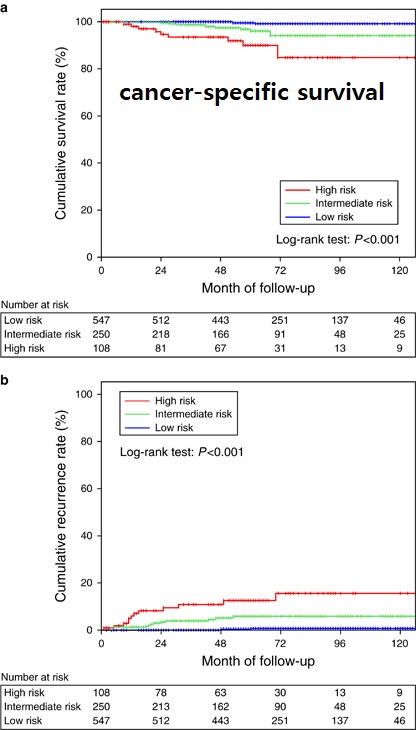
Next topic is the outcome. Although there are 4 or 5 major centers reporting similar results in Korea, I would mostly talk about our own experience at Samsung Medical Center.
Outcome of endoscopic treatment of EGC with differentiated histology is well established. We have ITT analysis such as comparison with surgery using propensity score matching. We also have PP analysis such as long-term follow-up data after curative resection or non-curative resection.
At my institution, we performed a propensity score-matching analysis between the two groups, endoscopic resection or surgery for differentiated type EGCs.
In the propensity score matched cases, about 60 percent were absolute indication cases. Others are expanded or beyond.
The rate of R0 resection was 82% in the endoscopic resection group
The overall survival was almost the same in the two groups. Because of the metachronous recurrences, disease free survival and recurrence free survival is better in the surgery group. However, there was no difference in the disease specific survival.
Next evidence is the PP analysis. It’s a single-arm long-term follow-up data for curatively resected differentiated-type EGCs.
Excluding metachronous recurrences, we experienced only one case of local recurrence, and 2 cases of extragastric recurrences.
This is the overall survival. There was no statistical difference between absolute indication and expanded indication.
There are the pictures of the two extragastric recurrences in our series. The top case belonged to the absolute indication group, and the lower case belonged to the expanded indication group.
Many centers recently reported longterm outcome after ESD in Korea. The rate of extra-gastric recurrence is usually less than 0.2%.
This is another PP analysis for non-curatively resected differentiated type EGCs. In cases with risk of lymph node metastasis, 70% were operated, and 30% were observed without surgery.
In the surgery group, 11 have lymph node metastasis, which means 5.7%. Patients with lymph node metastasis were older. To our surprise, the rate of lymph node metastasis was not different by the tumor size, depth of invasion, histological differentiation, and lymphovascular invasion in the endoscopically resected specimen. So, basically we found no predictor of lymph node metastasis in this analysis.
Rate of progression into the advanced cancers were different between 2 groups. Five advanced cancers were found in the observation group, and only one metastatic disease was found in the surgery group.
In terms of the overall survival, additional surgery was related with better outcome.
Survival benefit of additional surgery after non-curative resection was shown in a propensity matched study by doctor Eom at Korean National Cancer Center. As you can see at the right-hand side picture, the overall mortality of observation group was higher than that of the matched initial standard surgery patients.
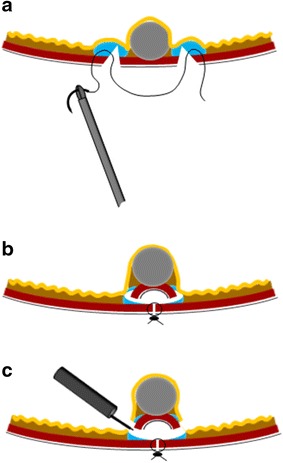
Final topic is future directions. I’ll briefly talk about non-exposure endoscopic full thickness resection and insights from genetic studies.
It seems to be similar technique shown in the previous presentation by professor Fujishiro. Doctor 김찬규 at Korean National Cancer Center developed a new simple non-exposure endoscopic full-thickness resection technique with laparoscopic seromuscular suturing.
This is the procedures.
They performed a randomized comparative animal study.
As you can see in this slide, the success rate was just comparable.
And the size of resected tissue was significantly smaller in the endoscopic full-thickness resection group. Clinical trial of non-exposure EFTR is now ongoing in Korean National Cancer Center for patients with subepithelial tumor.
As I mentioned earlier, treatment of gastric adenoma is very important in Korea. It is unclear whether all adenomas should be endoscopically resected. Professor Min of my institution investigated the genomic and transcriptomic landscape of adenoma with LGD, adenoma with HGD, and EGC. Because several genetic changes have been identified in advanced gastric cancer, but the genetic alterations associated with early gastric carcinogenesis remain unclear.
He found that the expression pattern clearly divided into normal, LGD, and EGC, whereas those of HGD overlapped with LGD or EGC. RNF 43 mutation were present only in HGD and EGC.
This is the adenoma-carcinoma model of gastric multistep carcinogenesis by professor Min. The red text indicates new genetic alterations found in the present study. We guess or hope that, some day in the future, further genetic information can help us select ESD candidates from patients with low grade or high grade dysplasia.
Ladies and gentlemen, I’d like to conclude my presentation by saying that ESD is widely performed for EGCs in the absolute indication in Korea. Annually, its more than 7,000 cases. We are still very careful about expanded indication cases. It’s done usually for flat SRCs less than 1 cm. Strategies for non-curative resection cases are still under investigation. Thank you for your attention.
![]() [References]
[References]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.