EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [KDDW 2017]
[KDDW 2017]

일시: 2017년 11월 23일 (목) - 11월 25일 (토)
장소: 그랜드 힐튼 호텔 (홍은동)
Yamamoto 선생님과 함께 (Breakfast session)


![]() 1. Meet the professor 11월 24일 금요일 7:30-8:30
1. Meet the professor 11월 24일 금요일 7:30-8:30
아침 6시에 지하철을 타고 가까스로 시간에 맞추어 도착하였습니다. 오기를 잘했다 싶었습니다. 변정식 교수님의 강의가 너~~~~~무 좋았기 때문입니다. 감사합니다.
변정식 교수님의 강의를 들으면서 강의 point 메모를 써 보았습니다.
![]() 2. 11월 24일 금요일 9:00-10:30 (Grand Ballroom BC) [우리말 심포지엄 1] 표준화된 위내시경 교육을 위하여 (Standardization of endoscopic procedure and education)
2. 11월 24일 금요일 9:00-10:30 (Grand Ballroom BC) [우리말 심포지엄 1] 표준화된 위내시경 교육을 위하여 (Standardization of endoscopic procedure and education)
1. 새로운 시대의 새로운 내시경 내시경 교육. 실무 경험을 중심으로 (New endoscopic education in a new era. Focusing on practical experience). 성균관대학교 이준행
강의 시작할 무렵 청중은 7명 밖에 없었지만... 강의는 즐거웠습니다. 세션 끝난 후 연자 및 좌장 선생님들과
오늘은 내시경 교육에 대하여 '누구를 가르칠 것인가'와 '어떻게 가르칠 것인가'를 중심으로 제 생각과 경험을 말씀드리겠습니다.
먼저 '누구를 가르칠 것인가'입니다.
내시경을 '누가 할 것인가, 누가 할 수 있는가'부터 생각해 보겠습니다. 당연한 일이지만, 내시경 진단에 대한 전문 훈련을 받은 의사가 시행하는 것이 가장 좋겠습니다. 그러나 의사면 누구나 할 수 있고, 또 누구나 하고 있는 것이 현실입니다.
그렇다면 누구를 가르쳐야 하겠습니까? 전문 훈련 과정을 밟고 있는 사람만 가르칠 수 있습니다. 예를 들면 소화기내과 fellow입니다. 반대로 원하면 누구나 가르친다는 전략도 가능합니다.
누구냐는 누구이겠습니까? 좁게는 소화기내과 fellow, 조금 넓히면 내과 전공의, 아주 넓히면 가정의학과 의사, 외과 의사 등 모든 의사가 해당합니다. 저는 원하면 누구나 가르쳐야 한다고 생각합니다.
제가 '원하면 누구나 가르쳐야 한다'고 생각하는 이유는 단순합니다. 안 가르쳐도, 못 배워도 다들 하고 있기 때문입니다. '안 가르치면 안하냐'는 것입니다. '못 배웠으면 하지 못하게 할 방도가 있느냐'는 것입니다. 국민에게 미안할 뿐이지요. 그러서 저는 원하면 누구나 가르쳐야 한다고 생각합니다.
발등의 불은 내과 전공의입니다. 전공의 과정이 4년에서 3년으로 단축되었기 때문입니다. 교수님들은 '4 plus 1'이 '3 plus 2'가 되기를 희망하고 있습니다. 그러나 fellow 2년이 당연하다는 교수님들의 희망은 이루어질까요?
혹시 이렇게 되지 않을까 걱정입니다. '3 plus 1'입니다.
아니면 이렇게 될 수도 있습니다. Fellow가 없어지는 것입니다. 제가 이런 걱정을 하는 것은 3년 코스 내과를 선택하는 젊은 의사들의 성향이 짧은 수련을 선호하는 것 같기 때문입니다.
내과 전공의 교육과정을 보면 '내시경 검사 참여 50건'이 명시되어 있습니다.
요컨데, 정규 내시경 교육을 받지 못한 시술자에 의한 내시경 검사가 광범위하게 이루어지고 있습니다. 그러나 저희 전문가들이 타 분야 의사들에게 내시경을 가르치지 않는다고 그들이 내시경 시술을 포기하지는 않습니다. 따라서 교육 대상 확대에 대한 허심탄회한 논의가 필요합니다. 내과 전공의들은 분과와 무관하게 내시경 교육을 받아야 합니다. 내시경 교육이 recruit의 핵심 경쟁력이 되고 있다는 점도 고려하시기 바랍니다.
다음은 '어떻게 가르칠 것인가'입니다.
과거에는 이렇게 배웠습니다. 두 글자 입니다. '해 봐.' 조금 친절한 분은 세 글자로 가르쳤습니다. '넣어 봐.' 저의 시작도 비슷했습니다. 생각하기도 싫은 황당한 기억입니다.
누구에게 배우셨는지 물어본 적이 있습니다. 많은 분들이 '미 선생님'이라고 답했습니다. 미다졸람 선생님입니다. 환자를 푹 재워 놓고 오랫동안 이리 저리 검사하다 보니 저절로 잘 하게 되었다는 것입니다. 정말 미안한 일입니다. 이래서는 안 되겠습니다.
사실 삽입이 전부는 아닙니다.
Fellow 과정을 마치는 분의 소감을 들어본 적이 있습니다. 처음에는 위내시경 목넘기기가 어렵지만, 돌고 돌아 결국은 병변의 관찰과 조직검사가 어렵다는 것입니다. 그렇습니다. 삽입은 일부 중 일부일 뿐입니다. 아주 작은 부분에 불과합니다. 내시경 교육은 내시경 삽입술 교육이 아닙니다.
과거에는 삽입부터 배웠지만 이제는 기본 지식을 먼저 배워야 합니다. 내시경 기본 지식 없이 무조건 삽입부터 배우는 것은 더 이상 타당하지 않습니다.
과거에는 두세번 observation 후 바로 삽입이었습니다. 이제는 새로운 방법이 적용되어야 합니다. 저희 기관에서는 simulator 훈련으로 흥미를 유발시키고, 몇 개월간의 교육 훈련을 받은 후 환자에게 삽입하도록 프로그램을 개편하였습니다.
Simulator 훈련에 대하여 좀 더 자세히 말씀드리겠습니다.
왜 simulator 훈련으로 시작해야 하는 것일까요?
어느 초심자의 편지를 소개합니다. "내시경의 원리나 정상을 알지 못하는 상태에서 내시경 화면만 보는 것은 큰 곤욕이었습니다."라는 부분이 있습니다. Simulator 훈련을 하면 관찰도 즐거워집니다. 흥미가 유발됩니다. 그래서 simulator 훈련부터 시작하고 있습니다.
어떤 종류의 simulator가 좋을까요? 과거에는 computer simulator를 쓰곤 했습니다. GI mentor II입니다. 그런데 요즘은 100% box simulator만 쓰고 있습니다. Computer simulator는 전부가 가짜인 반면, box simulator는 적어도 내시경은 진짜입니다. 훨씬 real합니다. 교육효과가 전혀 다릅니다. 그래서 요즘은 box simulator만 쓰고 있습니다.
구형이 있고 신형이 있습니다.
그런데 구관이 명관입니다. 신형은 위가 작고 너무 real하여 초보자가 배우기는 어렵습니다. 위가 크고 공간이 넉넉한 구형 simulator가 훨씬 유용하게 이용되고 있습니다.
대장내시경 simulator도 사용하고 있습니다.
아직 도입하지는 못했지만 일본에서는 anchor와 스프링으로 난이도 조정이 가능한 모델까지 나왔습니다.
과거 simulator 훈련은 늘 일과 후였습니다. 왜 밤에 교육을 받아야 했을까요? 환자 진료가 끝난 내시경실에서 simulator 훈련을 했기 때문입니다.
그래서 별도의 공간을 마련하였습니다. 창고의 구석을 정리하여 마련한 '내시경 box simulator 코너'입니다. 일명 '내시경 창고 교실'입니다. 아직은 방이 아니라 코너 수준이지만 그래도 없는 것보다 낫습니다.
전용 공간 확보 후에는 언제든지, 주로 낮을 이용하여 훈련할 수 있게 되었습니다.
과거에는 이런 모습으로 가르쳤습니다. 신체 접촉이 많았습니다. 왜 이렇게 가르쳐야 했을까요? 삽입법이 표준화되지 않았기 때문입니다.
그래서 표준화된 삽입법 매뉴얼을 만들었습니다. Torque rotation을 최대한 활용한 표준 삽입법 술기입니다.
새로 마련한 공간과 장비와 매뉴얼을 이용하여 지금은 여건이 허락하는 한 원하면 누구나 가르치고 있습니다.
다른 병원 의사도 가르치고 있습니다. '열린 교육'입니다.
'열린 교육'을 위하여 다른 과 동문에게 메일을 보냈더니 다양한 feedback이 있었습니다. '저는 소화기내과 의사가 아닌데 연락을 맞게 준 건가요?'라는 질문도 있습니다. 열린 교육은 아직 기대하지도 않는 모양입니다. 그래서 반응이 뜨겁습니다.
다음은 '공부 먼저 시작하는 내시경 교육'에 대하여 말씀드리겠습니다.
[책자 내용]
There has been a great advancement in the field of advanced diagnostic endoscopy and therapeutic endoscopy. However, endoscopic education for the beginners has been widely abandoned. As a result, a great proportion of endoscopic examinations are performed by suboptimally educated endoscopists. The volume of endoscopic examination is huge in Korea, so the quality control of the endoscopists is a great impact on the quality of the whole healthcase system.
At Samsung Medical Center, we have developed a basic endoscopic education course. The 3-month full-time introductory endoscopy training course is composed of following components. Most of the education materials are available on-line at http://endotoday.com/endotoday/endoscopy_training_2018.html.
The philosophy underlying our basic training course is that the knowledge is more important than the technique. You should have enough knowledge and desciption skills before starting technical training. It usually requires extensive training for 3 months before starting the first endoscopic examinations for the real patients.
Most of the education resources are available on-line, but the most import and unique component of our basic training course is the box simulator training with professors and the description exercise checked by the most experienced endoscopy teachers. I hope the model developed by our endoscopy unit is useful for the endoscopy beginners.
2. 내시경 교육 표준화의 필요성과 현장에서의 경험 (Necessity of standardization of endoscopic education and experiences in the real clinics). 울산대학교 정훈용
3. 진보된 진단 내시경 술기의 표준화와 교육 (Standardization and Education of Advanced Diagnostic Endoscopic Techniques). 경희대학교 장재영
4. 조기위암 내시경 치료 술기의 표준화와 교육 (Standardization and education of early gastric cancer endoscopic treatment). 서울대학교 김상균
![]() 3. 11월 24일 금요일 11:00-12:30 (Grand Ballroom BC) Symposium 11. Colorectal cancer screening modalities: How to use them strategically
3. 11월 24일 금요일 11:00-12:30 (Grand Ballroom BC) Symposium 11. Colorectal cancer screening modalities: How to use them strategically
![]() 4. 11월 24일 금요일 14:00-15:30 (Diamond Hall) Combined Session 3. Issues in neuroendocrine tumor (NET) of GI tract
4. 11월 24일 금요일 14:00-15:30 (Diamond Hall) Combined Session 3. Issues in neuroendocrine tumor (NET) of GI tract
![]() 5. 11월 24일 금요일 16:00-17:30 (Emerald Hall A) [소화기내시경학회 PG course 7 - 우리말. 상하부 합동] 증례로 배우는 위장관 질환 (Understanding Gastrointestinal Diseases Based on Cases)
5. 11월 24일 금요일 16:00-17:30 (Emerald Hall A) [소화기내시경학회 PG course 7 - 우리말. 상하부 합동] 증례로 배우는 위장관 질환 (Understanding Gastrointestinal Diseases Based on Cases)
1. 식도이완불능증의 진단과 치료의 최근 발전 (Recent developments in the diagnosis and treatment of esophageal achalasia). 가천대학교 김경오
2. 선암과 림프종을 제외한 위암의 내시경 소견 (Endoscopic findings of gastric cancers other than adenocarcinoma and lymphoma). 고려의대 정성우
3. 종양성 대장질환 감별진단 (Differential diagnosis of neoplastic colon diseases). 조선의대 이준
4. 염증성 대장질환 감별진단 (Differential diagnosis of inflammatory colon diseases). 고려의대 구자설
![]() 6. 11월 25일 토요일 7:30-8:30 Breakfast session (Meet the professor)
6. 11월 25일 토요일 7:30-8:30 Breakfast session (Meet the professor)
Clinical usefulness of image-enhanced and magnifying endoscopy in Japan. Yorimasa Yamamoto (Showa University Fujigaoka Hospital, Japan. yori-yama@med.showa-u.ac.jp)
![]() 7. 11월 25일 토요일 9:00-10:30. Image enhanced colonoscopy: pearls and pitfalls (Convention Hall C)
7. 11월 25일 토요일 9:00-10:30. Image enhanced colonoscopy: pearls and pitfalls (Convention Hall C)
![]() 8. 11월 25일 토요일 11:00-12:30. Free paper (UGI-6) (좌장: 이준행)
8. 11월 25일 토요일 11:00-12:30. Free paper (UGI-6) (좌장: 이준행)
1) Geeho Min. Efficacy and Safety of Etomidate Sedation Compared with Propofol Sedation during Gastroscopy
2) Do Il Choi. Comparison of Non-exposure Simple Suturing Endoscopic Full-thickness Resection and Laparoscopic Assist Endoscopic Full-thickness Resection for Gastric Subepithelial Tumors
3) Jihye Park. Comparison of Endoscopic Ultrosonography-guided Fine-needle Biopsy with Unroofing Biopsy for Upper Gastrointestinal Subepithelial Tumors Biopsy
4) In Rae Cho. Noninvasive Prediction Model for Diagnosis of Gastrointestinal Stromal Tumor Using Contrast-enhanced Harmonic Endoscopic Ultrasound (CEH-EUS)
5) Hyun Seok Lee. Predicting Malignancy Risk in Gastrointestinal Subepithelial Tumors with Contrast-enhanced Harmonic Endoscopic Ultrasound Using a Perfusion Analysis Software
6) Do Hoon Kim. Feasibility and Yield of a New 20-gauge Procore Needle with Coiled Sheath in EUS-guided Subepithelial Tumor Sampling: A Prospective Multicenter Study
7) Deok Yun Ju. New Method of Non-exposed Endoscopic Surgery on Patients with Gastrointestinal Tumor
8) Kyoung-Hwan Song. Single Incision Needle Knife (SINK) Biopsy: A Simple Techniques for the Tissue Sampling of Subepithelial Tumors
9) Junseok Park. Endosonographic Alterations of the Resected Small Subepithelial Lesions on Upper Gastrointestinal Tract during Surveillances
![]() 9. 11월 25일 토요일 14:00-15:30 Convention Hall A [UGI. International symposium 1] Endoscopic treatment of upper gastrointestinal neoplasms. (좌장: 최명규, 이준행)
9. 11월 25일 토요일 14:00-15:30 Convention Hall A [UGI. International symposium 1] Endoscopic treatment of upper gastrointestinal neoplasms. (좌장: 최명규, 이준행)
1. Recent issues in the endoscopic treatment of early esophageal cancer. Min YW 민양원 (Sungkyunkwan University, Korea)
* 참고: 2017-1-16. 민양원 교수님 특강 - 식도암 진단과 치료의 최신 지견
2. Synchronous and metachronous gastric cancer following ESD for early gastric neoplasms. Park JM 박재명 (The Catholic University of Korea, Korea)
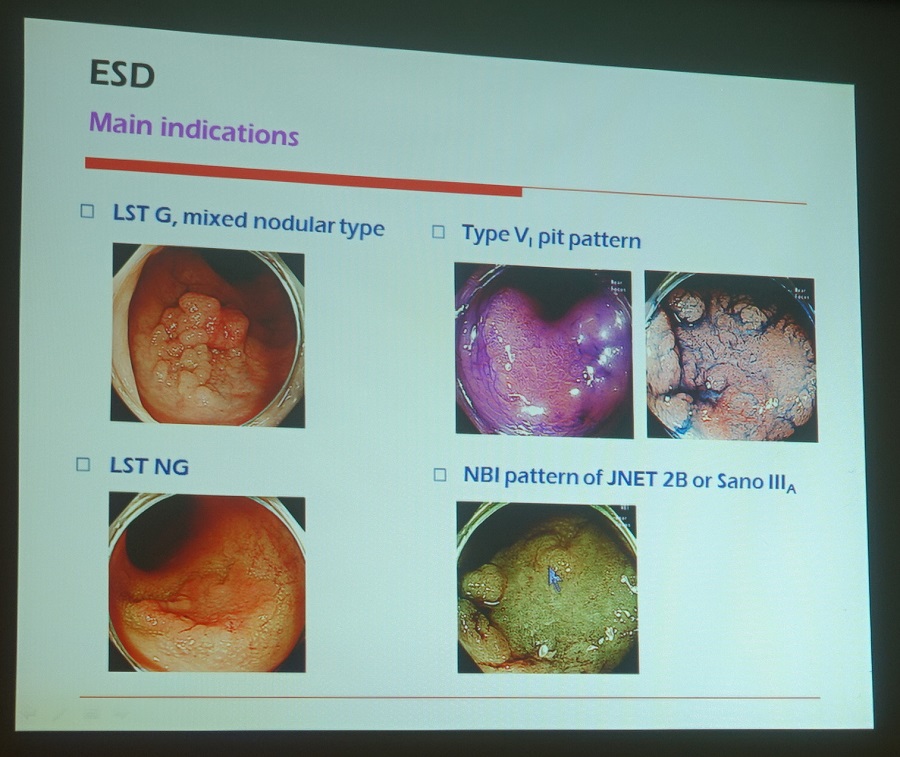
3. Indications of endoscopic treatment of EGC are still expanding? Pros and Cons. Kim GH 김광하 (Pusan University, Korea)
4. Long-term outcome after endoscopic treatment of EGC with emphasis on pathological non-curative resection. Ichiro Oda (National Caner Center, Tokyo, Japan)
Ichiro Oda 선생님에 의하면 일본 위암 가이드라인 개정판이 2017년 12월 혹은 2018년 1월에 일본어 단행본으로 발표된다고 합니다. 영어판은 좀 더 기다려야 할 것 같습니다. 그러나 내용은 이미 발표된 상태입니다.
2017년 3월 8일부터 10일까지 히로시마에서 열렸던 제89회 일본위암학회총회 소식지(News Flash)에 일본의 ESD indication 개정 방향에 대한 내용이 있어 소개합니다. 오늘 Oda 선생님이 발표하신 내용과 같았습니다. Undifferentiated type histology 위암은 absolute indication에 포함되지 않았습니다. Submucosal invasion도 마찬가지입니다. 분화조직형 점막암에 대해서만 확대되었습니다.
PDF 1.4M. 자료제공: 이선영 교수님
![]() 10. 11월 25일 토요일 16:00-17:30 Convention Hall A [UGI. International symposium 2] Gastric cancer screening and diagnosis of early gastric cancers
10. 11월 25일 토요일 16:00-17:30 Convention Hall A [UGI. International symposium 2] Gastric cancer screening and diagnosis of early gastric cancers
1. Improving quality of endoscopic examination in the setting of gastric cancer screening. Cho SJ 조수정 (National Cancer Center)
Quality of endoscopy = quality of endoscopist
차재명 교수님의 최근 분석에 따르면 우리의 quality indicator를 do not agree하거나 따를 수 없다고 답한 사람이 많았습니다.
ESGE에서는 최소한 7분 관찰하도록 하고 있습니다. Veitch A NRGH 2015에 따르면 영국에서는 최소한 8분 관찰하도록 하고 있습니다. 박재명 교수님의 연구에서도 긴 관찰시간이 중요하다고 하였습니다 (빼는 시간만 3분을 기준으로 하였지만).
일본은 double check system을 강조하고 있습니다.
내시경학회 홈페이지를 통하여 "위내시경 판독 자가 학습"이 가능합니다.
선종/암 발견율이 가장 중요한 quality indicator일 것 같습니다.
[이준행 comment] Quality of endoscopy = quality of medical system. 하루에 내시경 검사를 너무 많이들 하고 있습니다. 우리 현실에서 내시경 검사의 quality를 개선하기 위해서는 한 명의 내시경 의사가 하루에 시행하는 내시경 검사 數의 upper limit를 정할 필요가 있습니다. 이에 따른 검사 수가 조정은 당연한 일입니다.
2. Missed gastric cancer and interval gastric cancer. 한양대 박찬혁
한국과 일본에서 missed gastric cancer가 많다는 서양의 문헌은 한국와 일본에서 asymptomatic individual의 screening이 많음을 간과한 분석입니다.
Park (GE 2014;80;253)의 분석에 따르면 1년 간격과 2년 간격의 AGC rate는 비슷합니다. Repeated endoscopy alone cannot reduce missed gastric cancer.
박찬혁 교수님은 "Securing enough time is the best way to avoid missing lesion."을 큰 목소리고 강조하셨습니다.
3. Effectiveness of the Korean national cancer screening program in reducing gastric cancer mortality. 국제암대학원대학교 최귀선 (National Cancer Center, Korea)
우리나라의 2013년 위암 mortality/indicence ratio가 0.31로 세계에서 가장 낮았습니다.
국가 암검진 사업의 숨은 진실 (2013-1-16. 추적 60분. YouTube)
4. Detection of early EGJ cancer and indications for endoscopic therapy. Yorimasa Yamamoto (Showa University Fujigaoka Hospital, Japan)
바렛식도암 위치와 gastroesophageal reflux의 location과 관련되어 있다는 놀라운 연구 결과를 보여주셨습니다 (Omae, Fujisaki. Endosc Int Open 2016). 환자에서 acid 역류와 non-acid 역류의 방향은 대부분 일치하는데, 이 부위에서 암이 많이 발생한다니 놀라울 따름입니다. 연구의 결론("Accurate observation of the distribution of acid or non-acid reflux by pH monitoring would aid early detection of s-BEA by endoscopy.")은 다소 황당했습니다만...
The catheter used in our preliminary study had four sensors arrayed circumferentially at each of two levels. In our main study, the pH catheter had eight sensors (white arrows) arrayed circumferentially at the same level as the catheter. This catheter had a blue line on channel 1 located at the 6 o’clock position, and the eight sensors were arranged counterclockwise from that position
Distribution of the direction of s-BEA in (a) SSBE, (b) LSBE, and (c) all cases of Barrett’s esophagus.
A s-BEA case located at the 0-3 o’clock position in the lower esophagus. MTD-A and MTD-NA were detected by sensor 4 in the 0-3 o’clock position, and therefore this case was coincidental with acid and non-acid reflux.
A s-BEA case located at the 9-10 o’clock position in BE. MTD-A was detected by sensors 5-7 in the 9-0 o’clock position, and MTD-NA was detected by sensors 6-8 in the 8-10 o’clock position. Therefore this case was coincidental with both acid and non-acid reflux.
![]() [Selected posters]
[Selected posters]
2017-11-24 KDDW. CMV gastritis in heart transplantation (심형훈. 성균관의대)
2017-11-24 KDDW. 서울대병원. 첫 조직검사에서 atypical gland인 환자의 최종 결과에 대한 포스터였습니다. 병리리뷰에서 재확인된 252명 중 189명은 암으로, 26명은 선종으로 최종 확인되어 neoplasia가 무려 85.3%(215/252)였습니다. 제가 나름대로 분석해 보았습니다. (1) 859명 중 376명(43.8%)은 coexist adenoma or adenocarcinoma인데 이는 아마도 upward interobserver variation, 211명(24.5%)은 abscense of atypical glands on review인데 이는 아마도 downward interobserver variation 아닌가 생각되었습니다. 둘을 합하면 interobserver variation이 68.3%였습니다. Forceps biopsy에서 보고된 atypical gland의 interobserver variation이 엄청나다는 것을 알 수 있었습니다. (2) Upward interobserver variation 376명과, 치료 후 adenoma나 cancer로 나온 215였으므로 859명 중 적어도 68.8%(591/859)가 neoplasia였습니다.
2017-11-24 KDDW. 건국대병원. 조직검사에서 lymphofollicular gastritis로 나온 환자 중 아주 일부분만이 내시경상 nodular gastritis로 보인다는 중요한 자료입니다.
T cell lymphoma mimicking ulcerative colitis (영남대)
Acute esophageal necrosis (AEN), also known as "black esophagus" is characterized by a striking circumferential black appearance of esophageal mucosa on endoscop. AEN is a rare and is almost invariably associated with severe clinical conditions and serious comorbidities. (가톨릭대)
black esophagus (영남대)
Echinococcal cysts (전남대)
참고: EndoTODAY FUSE
Abdominal Castleman's disease
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.