 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [NOTES symposium 2018]
[NOTES symposium 2018]
시간: 2018년 8월 11일 (토)
장소: CHA 의과대학 차바이오컴플렉스 (지하1층 대강당)
![]() 1. POEM
1. POEM
Learning curve: Type I, II는 비교적 쉽지만, type III나 complicated achalasia는 아무리 경험이 많더라도 시술이 어려울 수 밖에 없습니다. 어려운 증례는 처음부터 (intentionally) open POEM을 하기도 합니다. (조주영 선생님)
![]() 2. Live demonstration of POEM
2. Live demonstration of POEM
매우 흥미로운 live demonstration이었습니다. POEM이 생각만큼 쉬운 시술이 아니라는 것을 잘 보여주었습니다. 합병증이 없으면 그만이지만 출혈이라는 무서운 합병증이 가능합니다. 천공도 늘상 발생합니다.
환자: EG junction outflow obstruction 환자로 Botox injection 후 6개월 정도 경과관찰하였으나 증상이 지속,악화되어 POEM을 시술
장소: 수술장
자세: supine position
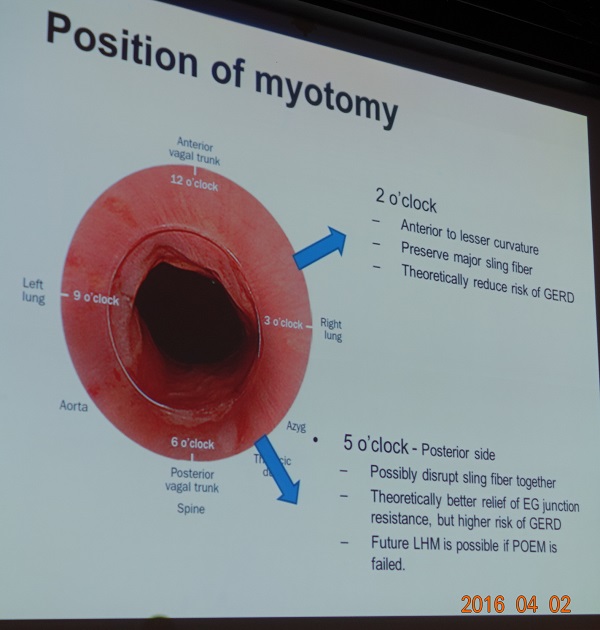
접근: posterior approach (5시 방향). Supine position에서 시술이 용이하다고 합니다.
절개도: Dual knife. 식도 submucosal tunneling 하면서 Dual knife의 needle을 내밀지 않은 상태에서 Spray Coagulation으로 시술.
내시경 cap: 3-D printing으로 prototype을 만들어 사용하던 호리병 모양의 cap을 사용. 최근 상품화되었다고 합니다.
Pneumoperitoneum이 심해 ventilator peek pressure가 높아지면 angiocath로 공기를 빼기도 합니다. "배 담당 fellow가 있다"고 합니다.^^ 홍수진 선생님께서는 (1) CO2를 사용하므로 pneumoperitoneum이 생기더라도 Angiocath로 공기를 뺀 적이 없다,(2) room air를 이용한 시술을 하면 안된다고 comment 하였습니다. 고원진 선생님은 CO2에 의한 acidosis의 위험이 있다고 comment 하였습니다.
Myotomy의 길이: Cardia에서 stomach 방향으로 2cm정도 myotomy를 하면 좋다고 합니다. 차병원에서는 nasal endoscopy를 이용하여 POEM 절제 위치를 확인하는데, 다른 병원에서는 nasal endoscopy를 사용하지 않는다고 합니다.
조주영 선생님께서 vessel anatomy를 언급하셨는데, 제가 정확히 알지 못하는 부분인지라 과거의 자료를 다시 한번 옮겨 소개합니다.
[Microvasculature of the esophagus and gastroesophageal junction] (World J Gastrointest Endosc 2016) - PDF
Mucosal vessels. A and C: Endoscopic images during per-oral endoscopic myotomy procedure (high magnification images); after unintentional removal of the epithelium (white layer), top half of epithelium was peeled off, and IPCLs were exposed. IPCLs appear as regularly-arranged, red dots (A: White light) or dark green spots (C: NBI); B: A schematic representation of the vascular network of esophageal mucosa: a: Branching vessels; b: SECN (Sub-epithelial capillary network); c: IPCL (Intrapapillary capillary loop)
A: Perforating vessels from the outer esophagus to the submucosal vessel; image captured during tunnelization in POEM (bottom side muscle layer, left side submucosal lifting); B: Submucosal drainage vessel (mucosal layer lifted on during ESD). These veins can become esophageal varices in portal hypertension; C: Submucosal vessels connecting the drainage veins to the mucosal branching vessels (in the lamina propria); D: Spindle veins immediately below the GEJ (in left side of the image, in blue, the submucosa and in the right side the muscle); E and F: branching vessels (seen from inside the submucosal tunnel). G: palisade vessels.
High magnifying narrow band imaging image of normal esophageal mucosa (luminal side). A: Soft pressure of the endoscope distal attachment (“hood”) onto the mucosal surface demonstrates SECN, hard pressure onto the mucosa compresses horizontal vessels, allowing clear observation of IPCLs; B: In the circle the SECN located at the top layer of lamina propria mucosae, just beneath the epithelium. The black arrows indicate the branching vessels into the lower lamina propria; white arrows indicate the IPCL located in the epithelial papilla, which is a projection of lamina propria mucosae into the epithelium.
The figure shows the histology of a non-pathologic esophageal specimen. The vessels’ wall has been colored by CD34, showing superficially the IPCLs (upper part of the lamina propria, arising the epithelium) and the SECN; deeply in the lamina propria the branching vessels. In the sumucosal layer also the drainage veins are evident. The table summarizes the vascular system observed and its own esophageal layer according to the different endoscopic procedure performed.
In the center a scheme of the submucosal view at the gastro-esophageal junction during per-oral endoscopic myotomy. At the muscle side (left endoscopic image) the spindle vein are clearly visible; at the mucosal side (seen on its backside, right endoscopic image) the palisade vessel are recognized. High magnification images.
Submucosal fibrosis가 있으면 POEM이 어려워지는데, 고원진 선생님께서는 시술 전 EUS를 하여 submucosal fibrosis 부위를 찾아보고 이를 피하여 시술한다고 하셨습니다. 홍수진 교수님께서는 (1) EUS를 보기는 하는데 fibosis를 정확히 구분하기가 어려웠다, (2) longstenting disease에서는 fibrosis가 가능하다고 생각하는 것이 좋다고 comment 하였습니다.
Myotomy: Inner circular muscle만 자르는 selective myotomy를 하고자 하였는데, 금일 증례는 근육이 얇아서인지 full thickness myotomy가 되었습니다. 홍수진 교수님께서는 (1) full thickness myotomy가 아닌 circular myotomy만으로도 충분한 것 같다, (2) EndoFLIP을 이용하여 적절한지 평가한 후 부족하면 조금 더 시술한다고 comment 하였습니다.
EG jucntion level에서는 식도에서는 perforating vessel이 굵어지고 위에서는 left gastric artery의 branch 때문에 출혈 위험이 있습니다. 혈관을 잘 관찰해야 하고, 가급적 Endocutting을 사용하지 않는 것이 좋겠습니다. Cutting의 속도도 중요합니다. (홍수진 교수님, 고원진 교수님 comment) 조주영 교수님께서는 delayed hematoma 증례가 1분 있었고, 처음에는 음식이 잘 안 내려가는 듯 했으나 hematoma가 천천히 저절로 흡수되면서 증세는 호전되었다고 합니다.
Cardia의 mucosal tear가 있으면 multibend endoscopy를 이용하여 gentle하게 clipping을 해 주어야 합니다. Submucosal dissection이 된 상태의 떠있는 점막에서 천공이 된 것이므로 조심스럽게 시술하지 않으면 오히려 점막 손상이 더 심해질 수 있기 때문입니다. GENTLE하게!!
항생제 사용: 시술 직전에 1회 prophylatic antibiotics 사용하고 시술 후 2일 정도 IV로 사용한 후 경구 항생제로 변경하여 며칠 더 사용합니다.
![]() 2. GERD
2. GERD
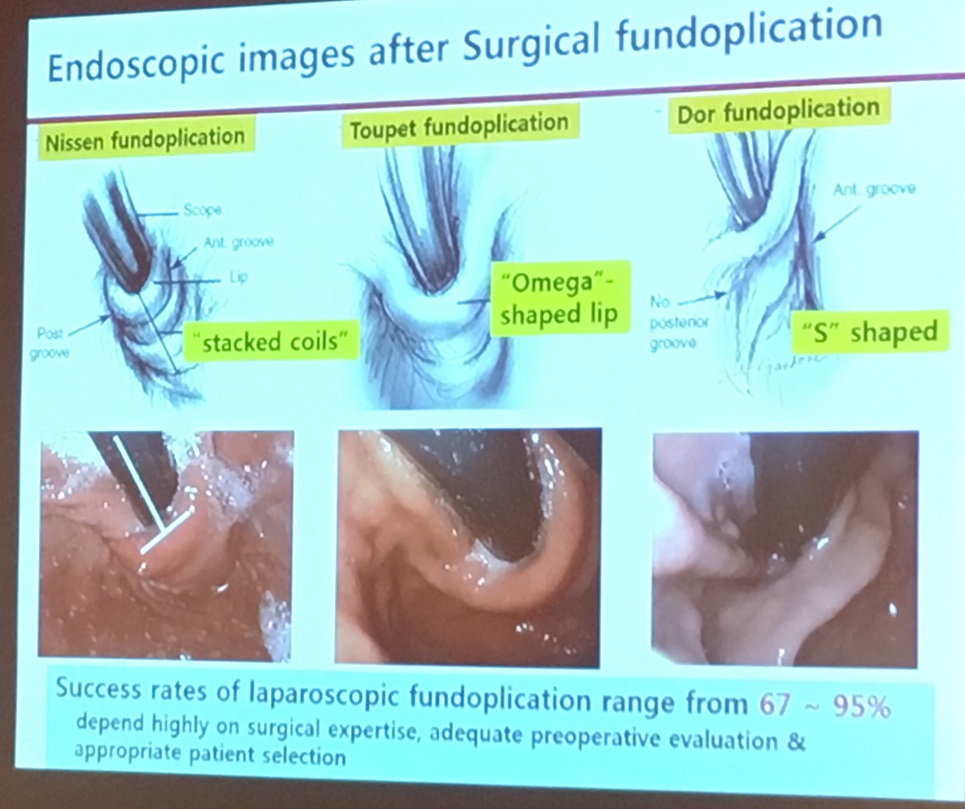
Fundoplication 후 내시경 소견은 수술의 종류에 따라 달라집니다.
문희석 교수님과 이혁 교수님께서 모두 GAP 개념을 소개하셨습니다.
Gastroenterology Report 2015;41-53
두 교수님께서 다양한 내시경 치료법을 소개해주셨습니다. 몇 주 전 삼성서울병원 임상강사 선생님께서 관련 리뷰를 리뷰한 바 있어 소개합니다.
PPT PDF 2.9M
Network meta-analysis Richter. Gastroenterology 2018
CONCLUSIONS: In a systematic review and network meta-analysis of trials of patients with GERD, we found LNF (laparoscopic Nissen fundoplication) to have the greatest ability to improve physiologic parameters of GERD, including increased LES pressure and decreased percent time pH <4. Although TIF (transoral incisionless fundoplication) produced the largest increase in health-related quality of life, this could be due to the shorter follow-up time of patients treated with TIF vs LNF or PPIs. TIF is a minimally invasive endoscopic procedure, yet based on evaluation of benefits vs risks, we do not recommend it as a long-term alternative to PPI or LNF treatment of GERD.
문희석 선생님께서는 아래와 같은 인상적인 slide를 보여주었습니다.
| Who are not EART candidate? |
| Patients with refractory GERD who have:
large sliding hiatal hernia (> 2cm long) Very low LES pressure (LEST < 5 mmHg) No response or change of symptoms with PPI Negative pH/impedance studies and no symptom correlation with acid events |
[ARMS (anti-reflux mucosectomy)]
개인적으로 ARMS의 경험이 없어서 2017년 POEM sympotisum의 고원진 교수님 말씀을 옮깁니다.
길이 방향으로 식도는 1cm, 위 cardia는 2cm 정도 resection을 해 줍니다. 식도를 포함하지 않으면 stricture 발생은 줄겠지만 효과도 떨어지기 때문에 식도를 조금 포함시켜야 합니다.
Circumference의 50% 이하는 효과가 없고 80% 이상은 stricture가 발생하므로 60-80% 정도 절제하는 것이 좋습니다. Inoue 선생님의 경우 retroflection으로 관찰하였을 때 1cm 정도 정상 점막이 남도록 조절하고 있다고 합니다.
Hernia가 있는 경우 hernia를 다 포함해서 시술합니다. Stretta 시술은 hernia가 있거나 erosive esophagitis가 있으면 시술할 수 없는데, 그런 환자에서는 ARES가 도움이 됩니다.
Stricture가 발생하더라도 healing 과정 중간에 balloon dilatation을 하면 stricture는 쉽게 해결됩니다.
전훈재 회장님 comment: ARMS의 유용성을 학회 차원에서 평가할 전향적 연구가 필요한지 NOTES 연구회에서 진지하게 토론해 볼 것을 권합니다.
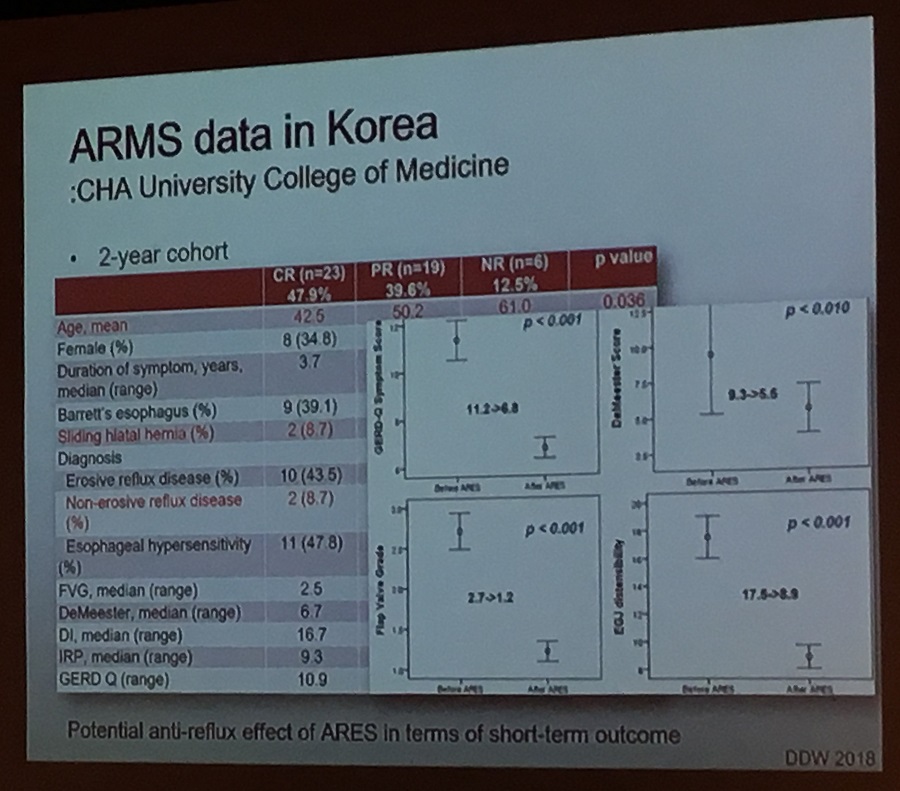
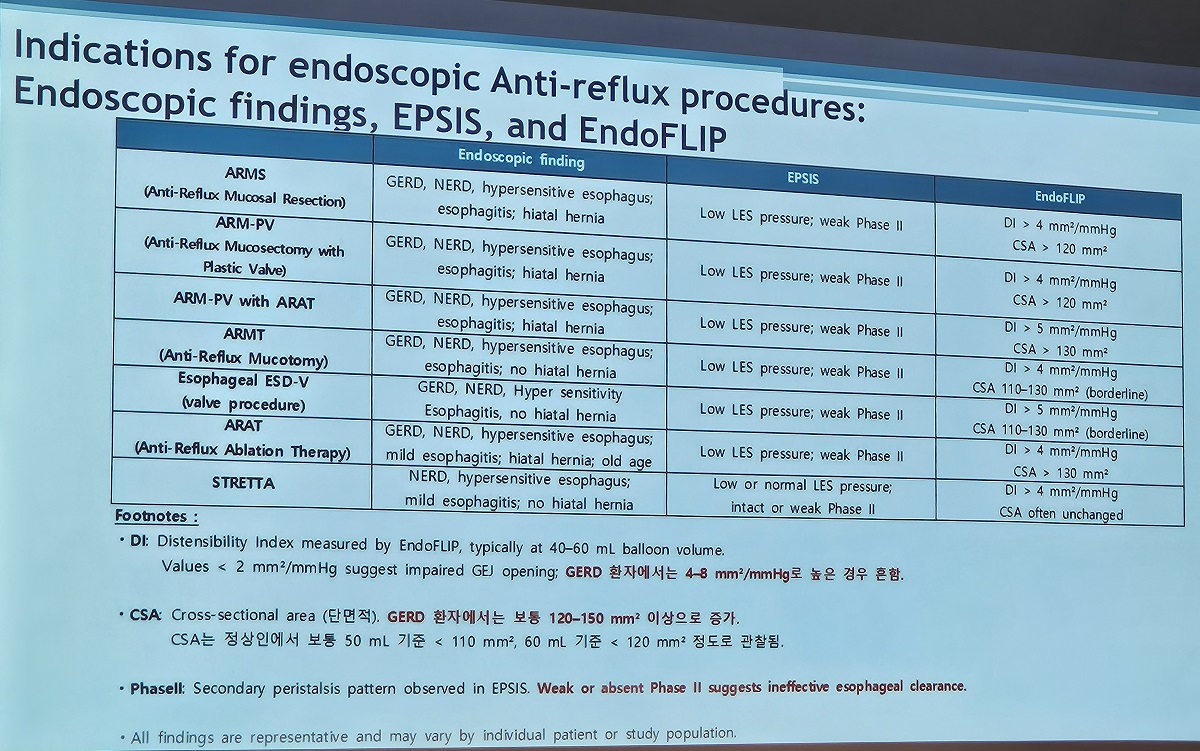
[추가] 2025년 7월 9일 내시경 학회 집담회의 차병원 발표 자료에서 ARMS (anti-reflux mucosal resection)의 institutional indication이 제시되었습니다.
![]() [References]
[References]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.
{kind=link}