EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [애독자 증례 편지 41 - 다양한 증례]
[애독자 증례 편지 41 - 다양한 증례]
[2019-12-23. 애독자 편지]
교수님 안녕하세요! 송년회 때 뵈어서 반갑고 즐거웠습니다. EndoTODAY는 여전히 잘 받아보고 있으며, 여전히 급할 때 레퍼런스로서 늘 도움을 받고 있습니다.
올해가 벌써 지나가고 있습니다... 로컬에서 10개월 가까이 적응하고 또 많은 수의 내시경과 진료를 하다 보니 로컬 나름의 재밌는 케이스가 있어서 우리 후배들과, 교수님과 공유해보고자 자료를 보내드립니다.
사실 저희 병원에서도 한 달에 한 번 내시경 집담회를 하는지라, 그거 준비하면서 혼자 보기에 아깝다 싶어서 공유해봅니다 ^^ 삼성으로 전원시킨 환자들도 다수 있어, 나와서도 교수님들을 믿고 의지하게 되는구나 싶습니다.
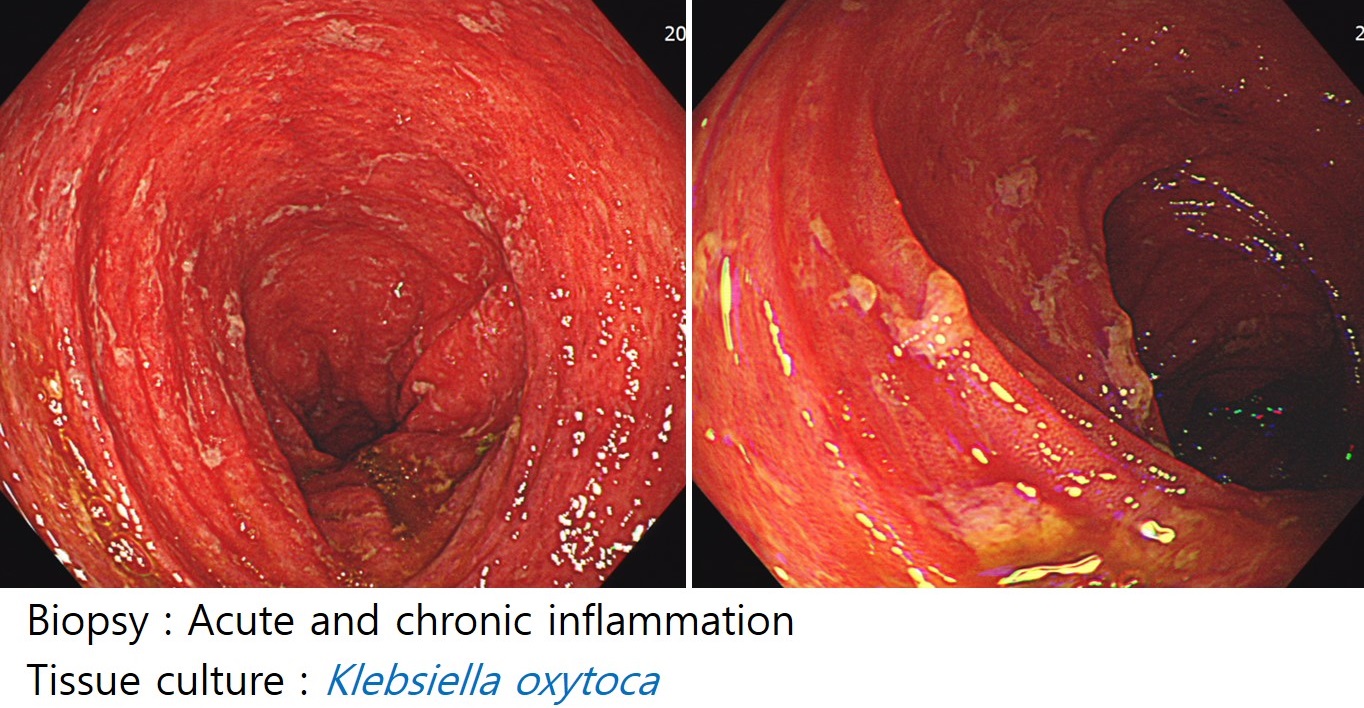
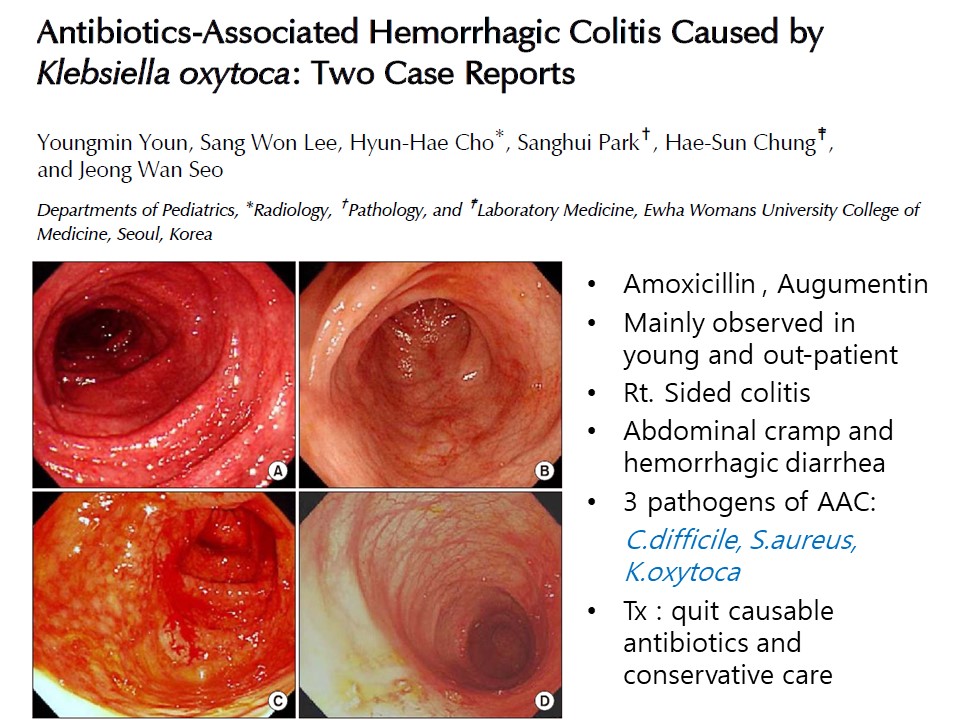
![]() 1. 젊은 여성에서의 혈성 설사와 복통 - Klebsiella oxytoca colitis (r/o antibiotics-associated)
1. 젊은 여성에서의 혈성 설사와 복통 - Klebsiella oxytoca colitis (r/o antibiotics-associated)
[이준행 comment] Tissue culture를 통하여 원인균까지 밝혔다니 정말 훌륭한 일을 하셨습니다. 비슷한 증례가 보고된 것이 있어서 아래에 옮깁니다.
Antibiotic-associated hemorrhagic colitis caused by cytotoxin-producing Klebsiella oxytoca
Klebsiella oxytoca was recently described as the causative organism for antibiotic-associated hemorrhagic colitis (AAHC). It is currently not known if this novel gastrointestinal infection exists in children. AAHC is usually preceded by antibiotic treatment with penicillins, which are frequently prescribed for pediatric patients. In contrast to colitis caused by Clostridium difficile, colitis caused by K oxytoca is usually segmental and located predominantly in the right colon. Patients with AAHC typically present with abdominal pain and almost always bloody diarrhea. We present here the case of an adolescent patient who developed acute abdominal pain and bloody diarrhea after antibiotic treatment for acute urinary infection with amoxicillin-clavulanate. Right-sided colitis was verified by abdominal sonography. Stool culture tested negative for common gastrointestinal pathogens but yielded K oxytoca. Toxin production of the isolated strain was verified in a cell-culture assay. Cessation of the causative antibiotic treatment led to rapid improvement and cessation of bloody diarrhea within 3 days. We report here the first (to our knowledge) pediatric case of K oxytoca infection causing AAHC. Establishing the diagnosis of AAHC by culturing K oxytoca and demonstrating right-sided colitis with noninvasive imaging studies might prevent unnecessary invasive procedures in children with bloody diarrhea.
![]() 2. Amebic colitis 몇 증례
2. Amebic colitis 몇 증례
3달 전부터 시작된 배변시 출혈, 잦은 배변과 설과, 복통. 외부병원에서 궤양성 대장염 의심하여 치료
최근 하루 5회의 혈성 점액변. 해외 여행 여러 차례, 최근 중국 여행
무증상 건진 내시경. 여행력 없음. 텃밭 가지고 계신 분. 복부 초음파는 정상
7개월 전부터 혈변, 점액변, tenesmus. 외부병원서 nonspecific proctitis, ulcerative proctitis 의심하에 치료받은 바 있음.
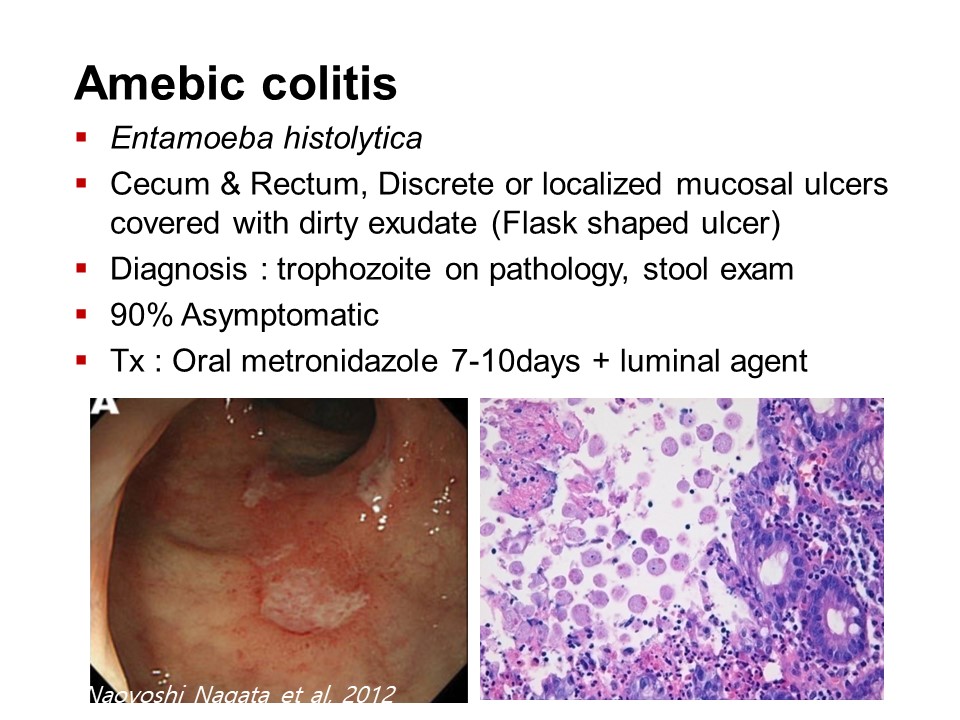
* 참고: EndoTODAY 이질아메바
![]() 3. CMV colitis
3. CMV colitis
전립선암 환자로 FU CT 에서 대장암 의심된다 하여 시행한 colonoscopy 결과임. 증상 없었음.
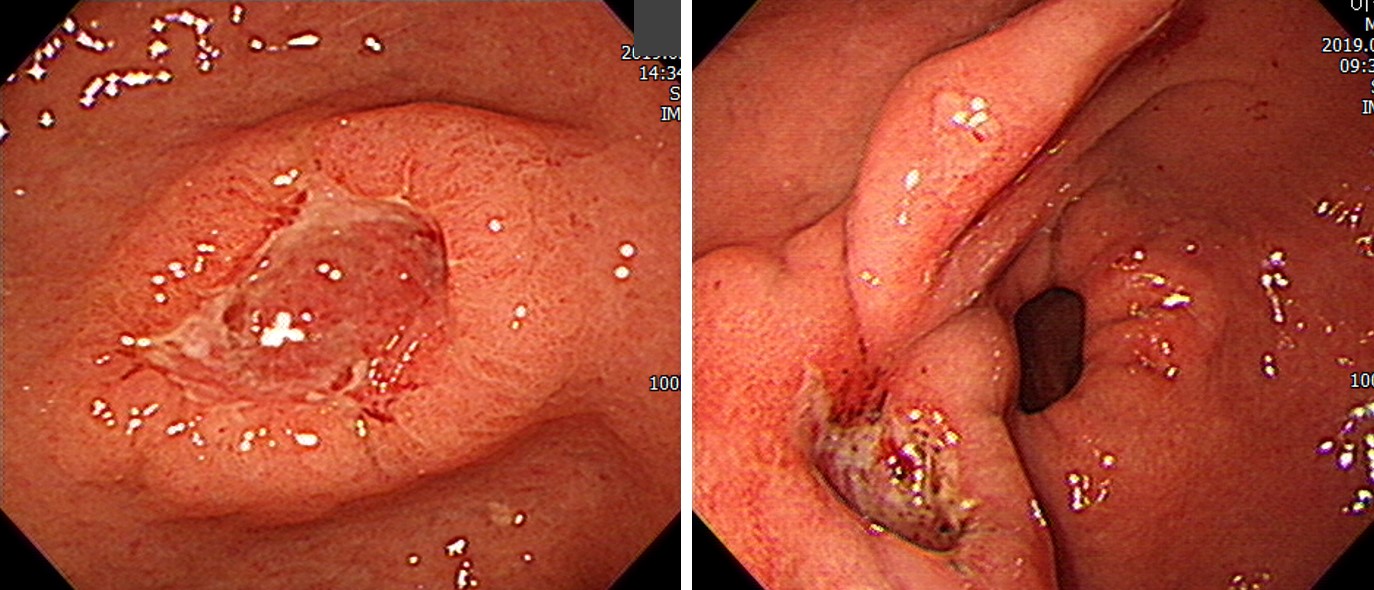
![]() 4. AGC versus BGU
4. AGC versus BGU
어느 쪽이 위암일까요?
.
.
.
.
.
.
.
.
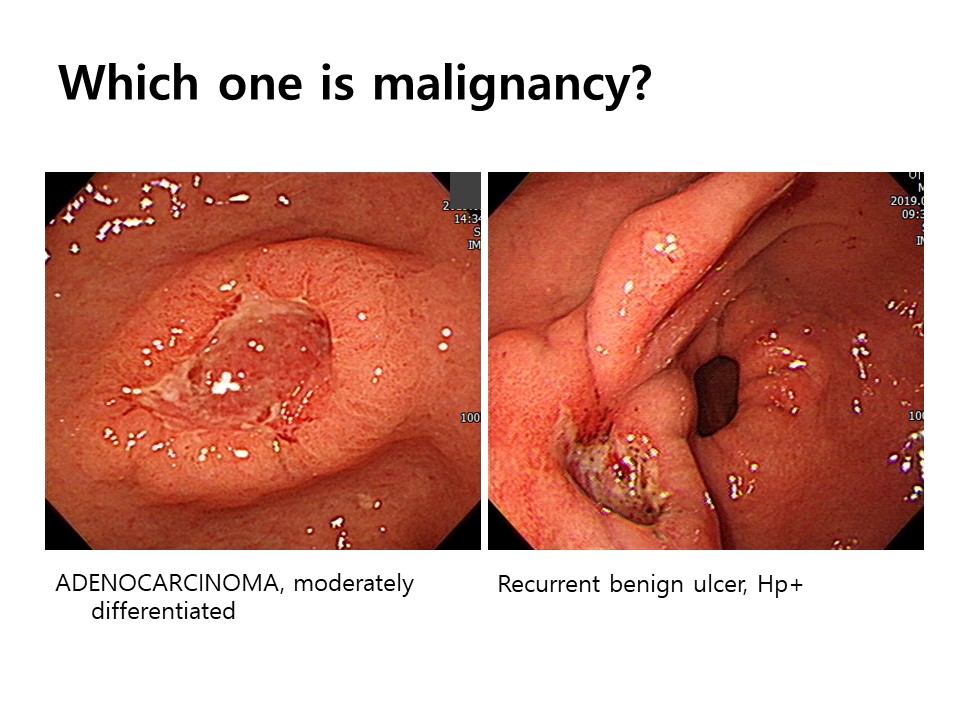
[이준행 comment] 좌측 증례가 암이라는 것은 금방 알 수 있습니다. 전형적인 보만 2형으로서 궤양부 주변의 비교적 균일한 1cm 정도의 heaped up bank 같은 모양이면 다소 불규칙한 표면 구조를 보이고 있습니다. 궤양부 edge는 일부는 sharp하지만 6시부터 9시까지와 12시 방향은 blurred되면서 일부분에서 삼각형 모양의 overriding도 보입니다. 문제는 우측인데요... 궤양부는 작지만 깊으며 edge는 blurred 되어 있습니다. 함몰부 주변의 heaped up bank 부분은 두께가 균일하지 않고 무엇보다도 1시 방향에서 몇 개의 fold가 끌려오면서 궤양부로 converging 하는 모습입니다. 게다가 1시 방향에서 끌려오는 fold의 표면에는 erosion도 있습니다. 이러한 소견은 recurrent ulcer의 scar 중앙부에서 궤양이 재발한 것으로 해석되는 소견입니다. 조직검사도 이에 합당하게 나왔다니 진단에는 무리가 없을 것 같습니다.
![]() 5. 위암
5. 위암
F/90. 수 주 이상 지속된 명치 통증 소화불량 등을 주소로 내원. 처음부터 내시경 검사를 하지는 않았고 약간의 투약에도 불구하고 호전되지 않아 초음파를 시행한 결과 위내에 음식물이 많이 남아있는 것으로 미루어 antral lesion이 의심된다고 보고됨. 내시경에서는 전정부의 ulceroinfiltrative cancer였으며 십이지장으로는 진입할 수 있었음. 병리결과: TUBULAR ADENOCARCINOMA, moderately differentiated
F/62. 위체부 후벽 병소로 하바터면 miss할 뻔 하였습니다.
F/80. 무증상 건진. 전정부 소만을 거의 다 차지하는 깊은 궤양을 동반한 종양이었는데도 환자는 전혀 증상이 없었습니다.
M/84. Adenocarcinoma, moderately differentiated. 마지막 내시경 4년 전
M/70. Adenocarcinoma, poorly differentiated with signet ring cell carcinomas
M/74. Poorly cohesive carcinoma
F/56. Signet ring cell carcinoma
M/57. Signet ring cell carcinoma
F/61. Poorly cohesive carcinoma, signet ring cell type
![]() 6. 식도암
6. 식도암
M/72. 35-37cm from UI, squamous cell carcinoma, moderately differentiated → Ivor-Lewis 수술을 받으셨고 최종 병기는 T1bN0M0
M/72. 30cm from UI, squamous cell carcinoma, moderately differentiated
![]() [References]
[References]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.