 EndoTODAY ГЛНУАц БГНЧ
EndoTODAY ГЛНУАц БГНЧ
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [ГэЙЎ РаБт 2016Гт 2Пљ]
[ГэЙЎ РаБт 2016Гт 2Пљ]
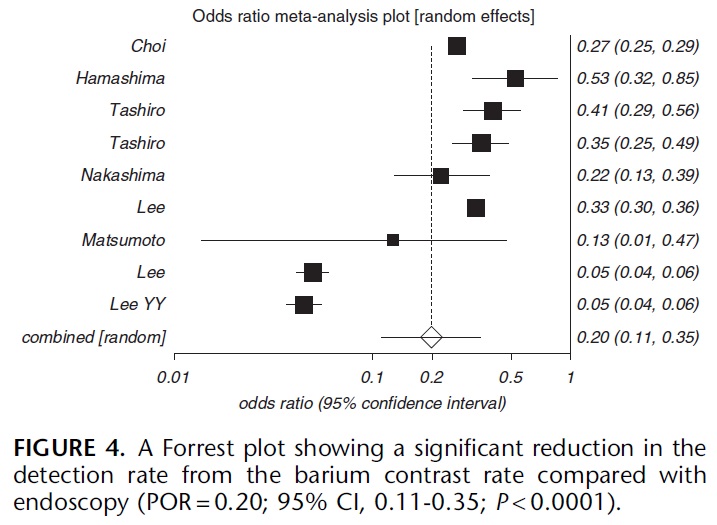
![]() Influence of gastric cancer screening on the stage at diagnosis and survival (Khanderia E. J Clin Gastroenterol 2016)
Influence of gastric cancer screening on the stage at diagnosis and survival (Khanderia E. J Clin Gastroenterol 2016)
РЇОЯ АЫСј ШПАњИІ КаМЎЧб ПЕБЙРЧ ИоХИПЌБИРдДЯДй. "About 73% of the screened patients were found to have EGC compared with 43% of the nonscreened patients."
ГЛНУАцПЁ КёЧЯПЉ ЙйЗ§ АЫЛчДТ РЇОЯРЛ 20% ЙлПЁ ЙпАпЧЯСі ИјЧбДйАэ ЧеДЯДй. РЇОЯ АЫСјПы ЙйЗ§ АЫЛчДТ КЮЕЕДіЧб РЯЗЮ АЃСжЕЧОюОп Чв АЭ ААНРДЯДй.
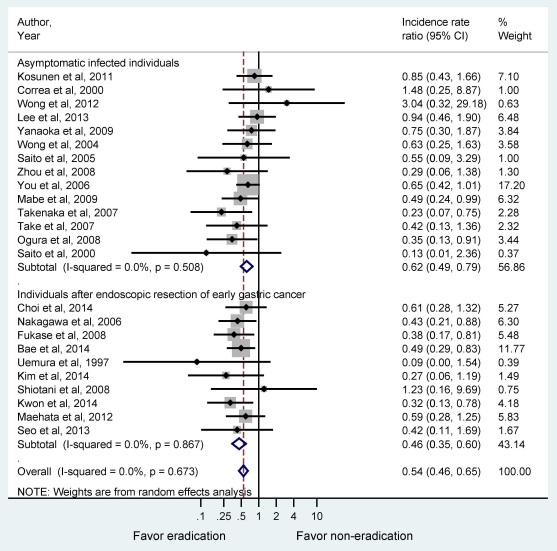
![]() Association between Helicobacter pylori eradication and gastric cancer incidence (Lee YC. Gastroenterology 2016)
Association between Helicobacter pylori eradication and gastric cancer incidence (Lee YC. Gastroenterology 2016)
РЇОЯ ПЙЙцРЛ РЇЧб СІБеФЁЗсРЧ ШПАњИІ КаМЎЧб ХИРЬПЯРЧ ИоХИПЌБИРдДЯДй. General population Йз ESD ШЏРкБК И№ЕЮПЁМ positive resultРдДЯДй. Pooled incidence rate ratioАЁ АЂАЂ 0.62, 0.46РЬОњНРДЯДй.
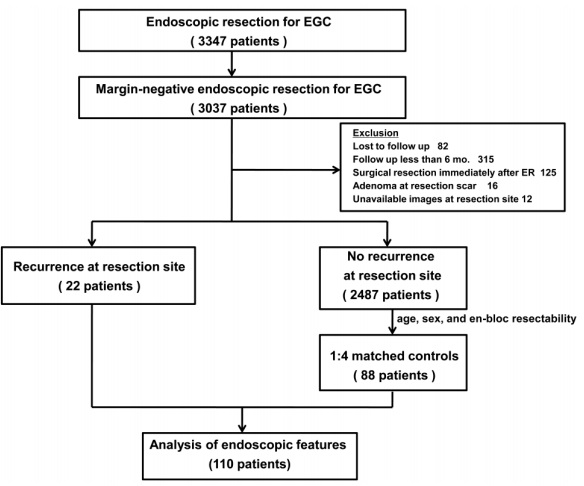
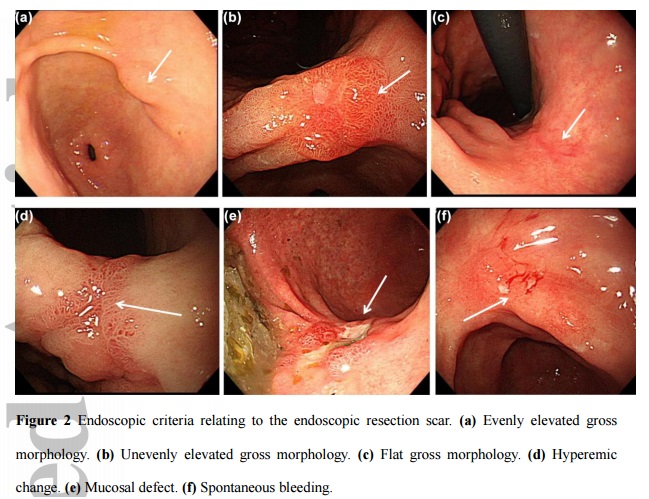
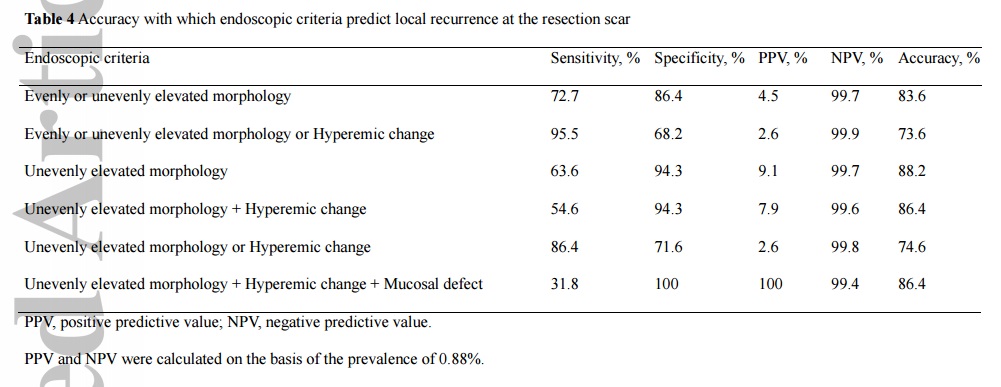
![]() Endoscopic prediction of recurrence after margin-negative endoscopic resection. (Na HK. JGH 2016)
Endoscopic prediction of recurrence after margin-negative endoscopic resection. (Na HK. JGH 2016)
МПяОЦЛъКДПј УжБтЕЗ БГМіДд ЦРПЁМ РЇОЯ ГЛНУАцФЁЗс ШФ БЙМвРчЙпРЛ КаМЎЧЯПДНРДЯДй. 1995ГтКЮГЪ 2011ГтБюСі 3,347ПЙРЧ СЖБтРЇОЯ ГЛНУАцФЁЗс Сп 3,027ПЙ(90.7%)АЁ margin-negative EGCПДНРДЯДй. 22ПЙРЧ БЙМвРчЙпАњ 4ЙшМіРЧ controlРЛ КёБГЧЯПДНРДЯДй. Differentiated type EGCРЧ en-block margin negative resection scarАЁ hyperemic change ОјРЬ flat ЧЯИщ СЖСїАЫЛчИІ Чв ЧЪПфАЁ ОјДйАэ АсЗаСўАэ РжНРДЯДй.
[РЬСиЧр comment]
СІАЁ БйЙЋЧЯДТ БтАќПЁМДТ АцЧш Йз РкЗс УрРћРЬ ЧЪПфЧЯДйАэ Л§АЂЧЯПЉ ДчКаАЃ БЙИГОЯМОХЭ Йз МПяОЦЛъКДПјПЁМ СІОШЧб АЭКИДй СЖБн tightЧЯАд АЫЛчЧЯДТ РќЗЋРЛ РЏСіЧЯАэ РжНРДЯДй. ОЦЗЁДТ 2016Гт 2Пљ ЧіРчРЧ ЙцФЇРдДЯДй.
1) СЖБтРЇОЯ EMR/ESD: 5ГтБюСі УпРћ ГЛНУАцИЖДй scarПЁМ СЖСїАЫЛч (2СЁ) → 5Гт ШФКЮХЭДТ РчЙп РЧНЩ МвАпРЬ РжРЛ ЖЇИИ СЖСїАЫЛч (Дм, СЖБтРЇОЯ EMR/ESD ШФ УЙ УпРћ ГЛНУАцПЁМДТ H. pylori СЖСїАЫЛчЕЕ ЧдВВ НУЧрЧбДй.)
2) МБСО EMR/ESD: 1ГтБюСі УпРћ ГЛНУАцИЖДй scarПЁМ СЖСїАЫЛч (2СЁ) → 1Гт ШФКЮХЭДТ РчЙп РЧНЩ МвАпРЬ РжРЛ ЖЇИИ СЖСїАЫЛч
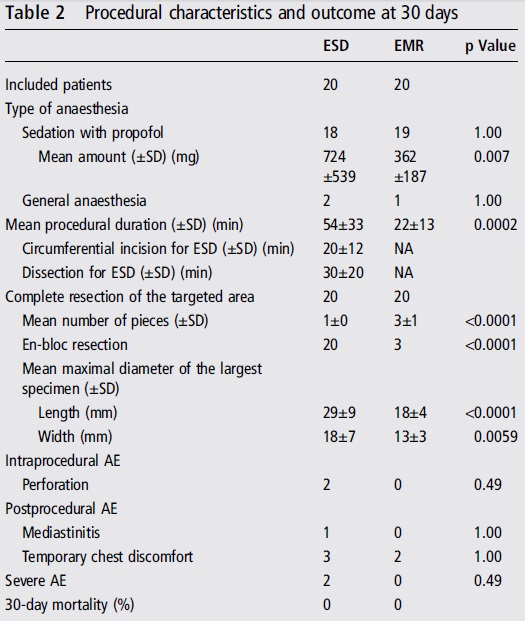
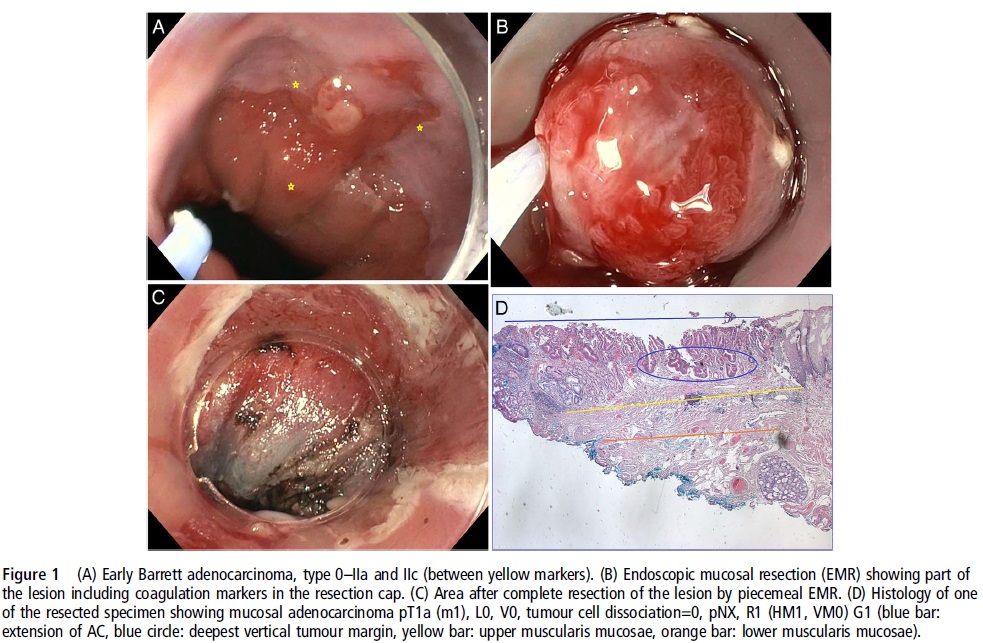
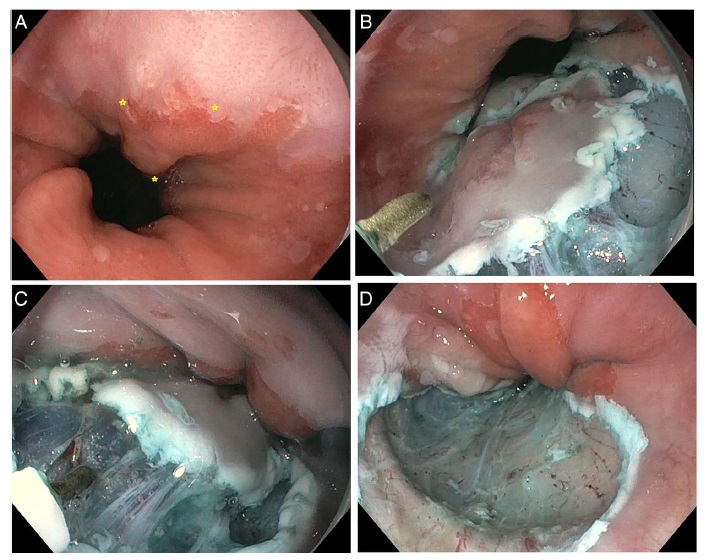
![]() A randomised trial of EMR versus ESD (Terheqqen G. Gut 2016)
A randomised trial of EMR versus ESD (Terheqqen G. Gut 2016)
ЦђБе 16mmРЧ СЖБт ЙйЗПНФЕЕОЯ ГЛНУАцФЁЗсРЧ ЕЮ ЙцЙ§(EMRАњ ESD)РЛ КёБГЧб ЕЖРЯ ПЌБИРдДЯДй. ESDДТ R0 resection rateАЁ ГєСіИИ, НУАЃРЬ ИЙРЬ АЩИЎАэ ЧеКДСѕРЬ ШчЧеДЯДй. ЕЖРЯ ПЌБИРкЕщРК ФЁЗс ШПАњАЁ КёНСЧЯДйДТ РЬРЏЗЮ ESDИІ АњМвЦђАЁЧЯАэ РжНРДЯДй. СІАЁ КИБтПЁДТ ESD МњБтИІ АЅАэ ДлОЦМ ЧеКДСѕ ОјРЬ Рп НУМњЧЯИщ АсАњАЁ ДйИІ АЭ ААНРДЯДй.
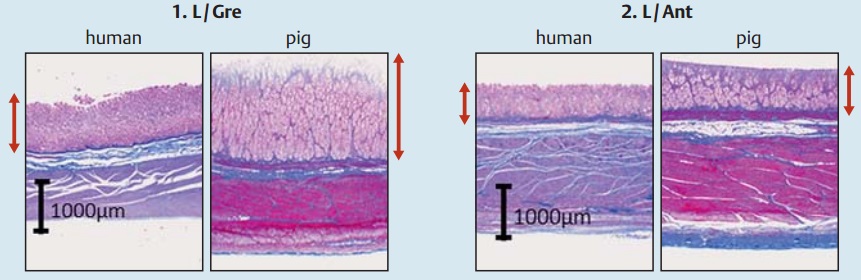
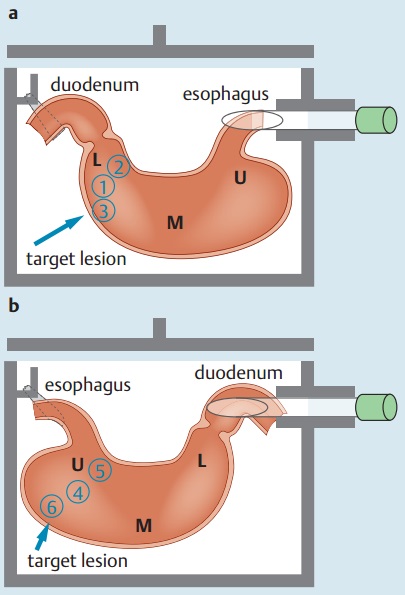
![]() Which part of a porcine stomach is suitable as
an animal training model for ESD? (Horii J. Endoscopy 2016)
Which part of a porcine stomach is suitable as
an animal training model for ESD? (Horii J. Endoscopy 2016)
УжБй ПьИЎГЊЖѓ ИюИю КДПјПЁМ ЕХСі stomachРЛ РЬПыЧб ESD hands on trainingРЬ СјЧрЕЧАэ РжРИИч, ДыЧбМвШБтГЛНУАцЧаШИ ESD ПЌБИШИПЁМЕЕ СЖИИАЃ ЕПРЯ ЧСЗЮБзЗЅРЛ openЧв ПЙСЄРдДЯДй.
 ЛяМКМПяКДПј 2016Гт 2Пљ 1РЯ
ЛяМКМПяКДПј 2016Гт 2Пљ 1РЯ
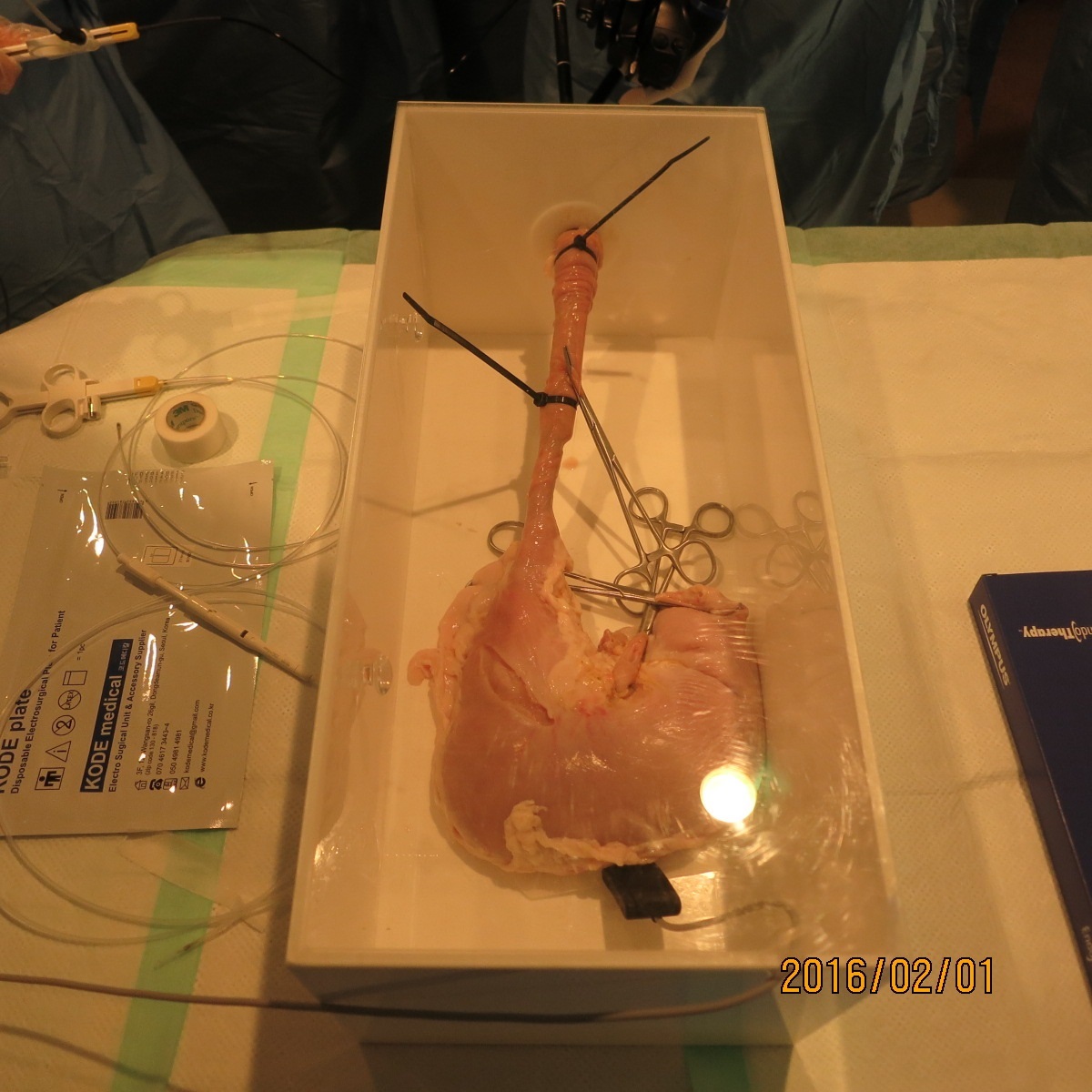

РЯКЛПЁМДТ ПРЗЁ РќКЮХЭ ЕХСі stomachРЛ РЬПыЧб ESD hands on trainingРЬ ИХПь ШАЙпЧЯАд СјЧрЕЧОњНРДЯДй. ПьИЎГЊЖѓ МБЛ§ДдЕщЕЕ РЯКЛРЧ hands on trainingПЁ АЛчЗЮ УЪКљЕЧБтЕЕ ЧЯПДНРДЯДй.
 2015Гт JDDWПЁМ РќГВДы РЬПЯНФ БГМіДдАњ РЮСІДы БшСіЧі БГМіДдВВМ hands-on trainingПЁМ ESD НУМњРЛ demonstration ЧЯДТ РхИщ
2015Гт JDDWПЁМ РќГВДы РЬПЯНФ БГМіДдАњ РЮСІДы БшСіЧі БГМіДдВВМ hands-on trainingПЁМ ESD НУМњРЛ demonstration ЧЯДТ РхИщ
РЯКЛ ПЌБИРкЕщРК ЕХСі stomachРИЗЮ ПРЗЁ ШЦЗУЧЯДйКИДЯ ОюДР КЮКаРЬ ESD ПЌНРПЁ РћЧеЧбСі БУБнЧпДј И№ОчРдДЯДй. АсЗаРћРИЗЮ greater curvatureДТ СССі ОЪАэ РќКЎАњ ШФКЎРЬ ССДйДТ РЬОпБтРдДЯДй. ОЦЗЁ ЛчСјАњ ААРЬ СТУј greater curvatureДТ ЛчЖїАњ ЕХСіАЁ ПЕ ДйИЅЕЅ ПьУј anterior wallРК ЛчЖїАњ ЕХСіАЁ КёНСЧЯДйАэ ЧеДЯДй.
Simulator boxПЁ ЕХСі stomachРЛ АХВйЗЮ РхТјЧЯИщ upper stomach РќКЎАњ ШФКЎЕЕ ESD ПЌНРПЁ ЛчПыЧв Мі РжДйДТ ОЦРЬЕ№ОюАЁ ШяЙЬЗЮПќНРДЯДй.
![]() Guidelines for endoscopic submucosal dissection and endoscopic mucosal resection for early gastric cancer (Ono H. Digest Endosc 2016)
Guidelines for endoscopic submucosal dissection and endoscopic mucosal resection for early gastric cancer (Ono H. Digest Endosc 2016)
РЯКЛМвШБтГЛНУАцЧаШИПЭ РЯКЛРЇОЯЧаШИАЁ АјЕПРИЗЮ СЖБтРЇОЯ ГЛНУАцФЁЗс АЁРЬЕхЖѓРЮРЛ ГТНРДЯДй. РЯКЛРЧ РяРяЧб ИтЙіЕщРЬ УбЕППј ЕЧОњНРДЯДй.
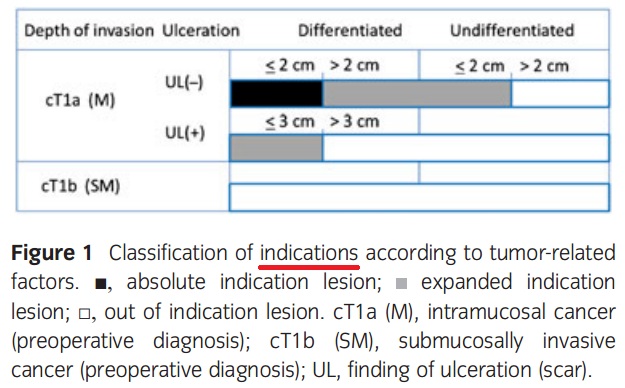
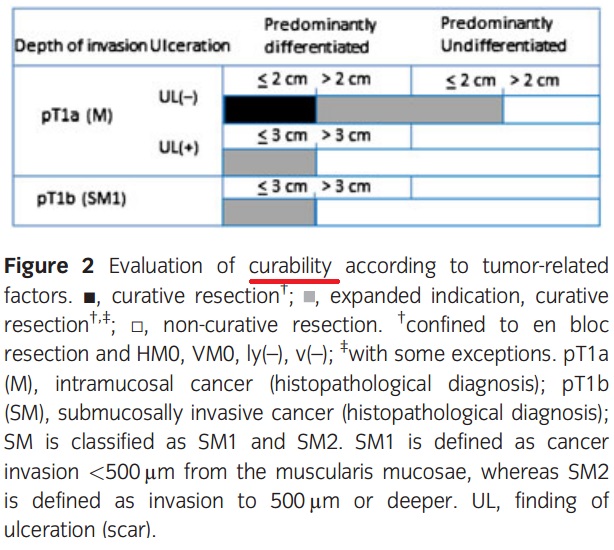
Indication tableАњ curability decision criteria tableРЛ ЕћЗЮ СІНУЧпДйДТ СЁПЁМ КИДй ИэЗсЧиСГДйАэ Л§АЂЕЫДЯДй. ScarИІ ЦїЧдЧб ulcer findingРЬ РжДТ differentiated type СЁИЗОЯ 3 cmБюСі expanded indicationПЁ ЦїЧдЕЧОю РжНРДЯДй. БзЗЏГЊ СЁИЗЧЯОЯРИЗЮ ЦЧДмЕШ АцПь(cT1b)ДТ ХЉБтПЭ ЙЋАќЧЯАд expanded indicationРЬ ОЦДЯЖѓДТ СЁПЁ РЏРЧЧеНУДй. РЇОЦЗЁ ЕЮ ЧЅИІ КёБГЧЯИщ БнЙц ОЫ Мі РжНРДЯДй.
![]() ACG Clinical Guideline: Diagnosis and Management of Barrett's Esophagus (Shaheen NJ. AJG 2016).
ACG Clinical Guideline: Diagnosis and Management of Barrett's Esophagus (Shaheen NJ. AJG 2016).
2016Гт ЙйЗПНФЕЕ АЁРЬЕхЖѓРЮРЬ ГЊПдНРДЯДй. СІАЁ ШяЙЬЗгАд КЛ КЮКаРК ОЦЗЁПЭ ААНРДЯДй.
1 cm ЙЬИИРЧ ЙйЗПНФЕЕ РЧНЩКЮРЇДТ ЙйЗПНФЕЕЗЮ СјДмЧЯСі ОЪЕЕЗЯ БЧЧЯАэ РжНРДЯДй. СЖСїАЫЛчЕЕ ЧЯСі ИЛЖѓАэ ЧеДЯДй (should not be performed).
Recommendation 2 . Endoscopic biopsy should not be performed in the presence of a normal Z line or a Z line with < 1 cm of variability (strong recommendation, low level of evidence).
BE has been traditionally defined as the presence of at least 1 cm of metaplastic columnar epithelium that replaces the stratifi ed squamous epithelium normally lining the distal esophagus. The reason why such segments < 1 cm have been classifi ed as "specialized IM of the esophagogastric junction" (SIM-EGJ) and not BE is because of high interobserver variability as well as the low risk for EAC. Patients with SIM-EGJ have not demonstrated an increase in the development of dysplasia or EAC in large cohort studies aft er long-term follow-up, in contrast with patients with segments of IM >1 cm.
ЙйЗПНФЕЕЖѓЕЕ dysplasiaАЁ ОјРИИщ ГЛНУАцРЛ ГЪЙЋ РкСж ЧЯСіДТ ОЪЕЕЗЯ БЧЧЯАэ РжНРДЯДй.
Acknowledging recent data on the low risk of malignant progression in patients with nondysplastic BE, endoscopic surveillance intervals are attenuated in this population; patients with nondysplastic BE should undergo endoscopic surveillance no more frequently than every 3-5 years.
Neither routine use of biomarker panels nor advanced endoscopic imaging techniques (beyond high-definition endoscopy) is recommended at this time. Endoscopic ablative therapy is recommended for patients with BE and high-grade dysplasia, as well as T1a esophageal adenocarcinoma. Based on recent level 1 evidence, endoscopic ablative therapy is also recommended for patients with BE and low-grade dysplasia, although endoscopic surveillance continues to be an acceptable alternative. Given the relatively common recurrence of BE after ablation, we suggest postablation endoscopic surveillance intervals.
ChomopreventionРИЗЮ PPI ЛчПыРЛ БЧЧЯАэ РжНРДЯДй.
Recommendation 26 . Patients with BE should receive once-daily PPI therapy. Routine use of twice-daily dosing is not recommended, unless necessitated because of poor control of refl ux symptoms or esophagitis (strong recommendation, moderate level of evidence).
PPI therapy is common in patients with BE, in part because of the high proportion of those patients who also have symptomatic GERD. In these cases, the use of PPIs is substantiated by the need for symptom control, making consideration of chemoprevention secondary. However, even in patients without refl ux symptoms, in whom BE is incidentally found during evaluation of other symptoms and/or signs, the use of PPIs deserves consideration. Several cohort studies now suggest that subjects with BE maintained on PPI therapy have a decreased risk of progression to neoplastic BE compared with those with either no acid suppressive therapy or those maintained on H2RA therapy. In addition, the risk profi le of these medications is favorable in most patients, and the cost of this class of drugs has diminished substantially in recent years because of the availability of generic forms of the medications.
These factors, combined with the theoretical consideration that the same infl ammation that may be in part be responsible for pathogenesis of BE may also promote progression of BE, make the use of PPIs in this patient population appear justifi ed, even in those without GERD symptoms. Given the low probability of a randomized study of PPI use in BE, decisions regarding this intervention will likely rely on these retrospective data and expert opinion.
![]() Clinical impact of second-look endoscopy after ESD (Jee SR. EJGH 2016)
Clinical impact of second-look endoscopy after ESD (Jee SR. EJGH 2016)
КЮЛъДыПЭ АэНХДыАЁ ЧљЗТЧЯПЉ ESD ШФ second-look endoscopyРЧ РЧЙЬИІ КаМЎЧЯПДНРДЯДй. РќУМРћРИЗЮ negative studyРдДЯДй. Ся routineЧЯАд second-look endoscopyИІ Чв ЧЪПфАЁ ОјДйДТ АЭРдДЯДй. ПРШїЗС second-look endoscopyИІ ЙоРК ШЏРкПЁМ УтЧїЗќРЬ ГєОвНРДЯДй. РњРкЕщРК second-look endoscopy РкУМАЁ УтЧїРЛ РЯРИХГ РЇЧшРЬ РжДйДТ СЁРЛ СіРћЧЯПДНРДЯДй.
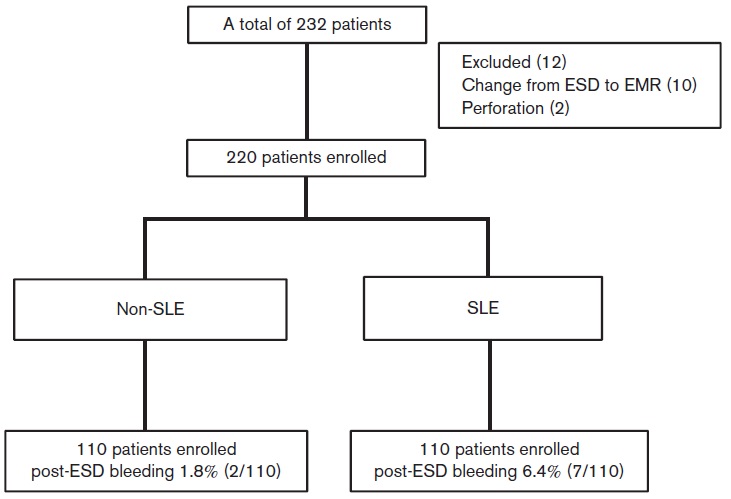
РќРћРИЗЮ ЕПРЧЧеДЯДй. ВР ЧЪПфЧЯСі ОЪРК АЫЛчДТ КЮРлПы, ЧеКДСѕИИ РЯРИХГ ЛгРдДЯДй.
![]() ЛѓКЮРЇРхАќ ГЛНУАц НУМњРЧ БЙАЁАЃ ТїРЬ (Uedo N. Digest Endosc 2016 - Epub)
ЛѓКЮРЇРхАќ ГЛНУАц НУМњРЧ БЙАЁАЃ ТїРЬ (Uedo N. Digest Endosc 2016 - Epub)
РЯКЛАњ РЯКЛРЬ ОЦДб ДйИЅ ГЊЖѓ(ХИРЬПЯ, ХИРЬ, ИЛЗЙРЬСіОЦ, ЧбБЙ, СпБЙ, РЬХЛИЎОЦ, ЙЬБЙ, ШЃСж Ею)РЧ ПЉЗЏ МБЛ§ДдЕщРЧ ГЛНУАц styleПЁ ДыЧб survey АсАњАЁ ЙпЧЅЕЧОњНРДЯДй. ЧбБЙПЁМДТ РњИІ ЦїЧдЧЯПЉ 5КаРЬ МГЙЎПЁ ТќПЉЧЯПДНРДЯДй.
International groupРЧ ДыЧЅМКРЬ ЖГОюСіДТ РкЗсРЬСіИИ РЯКЛРЧ ГЛНУАц ЧіШВРЛ ЛьЦьКМ Мі РжДТ ССРК БтШИЖѓАэ Л§АЂЕЫДЯДй. SurveyРЮ АќАшЗЮ ЧіНЧАњДТ ОрАЃ ДйИІ Мі РжДйДТ СЁРЛ АЈОШЧи СжММПф.
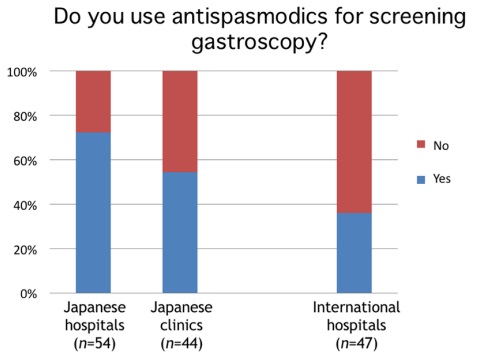 РЯКЛРЬГЊ БтХИ ГЊЖѓ И№ЕЮПЁМ antispasmodicsИІ ЛчПыЧЯСі ОЪДТ АцПьАЁ ИЙОвНРДЯДй. РњДТ ЦЏКАЧб БнБтСѕРЬ ОјРИИщ АХРЧ ЧзЛѓ ЛчПыЧпДТЕЅПф... АэЙЮЧи КМ РЬНДРдДЯДй. AntispasmodicsИІ ЛЉАэ АЫЛчЧиЕЕ АсАњПЁ ТїРЬАЁ ОјДйИщ ОіУЛ ЦэЧиСњ АЭ ААНРДЯДй.
РЯКЛРЬГЊ БтХИ ГЊЖѓ И№ЕЮПЁМ antispasmodicsИІ ЛчПыЧЯСі ОЪДТ АцПьАЁ ИЙОвНРДЯДй. РњДТ ЦЏКАЧб БнБтСѕРЬ ОјРИИщ АХРЧ ЧзЛѓ ЛчПыЧпДТЕЅПф... АэЙЮЧи КМ РЬНДРдДЯДй. AntispasmodicsИІ ЛЉАэ АЫЛчЧиЕЕ АсАњПЁ ТїРЬАЁ ОјДйИщ ОіУЛ ЦэЧиСњ АЭ ААНРДЯДй.
 РЯКЛПЁМДТ mucolytics/deforming agentsИІ АХРЧ ЧзЛѓ ЛчПыЧЯДТБКПф.
РЯКЛПЁМДТ mucolytics/deforming agentsИІ АХРЧ ЧзЛѓ ЛчПыЧЯДТБКПф.
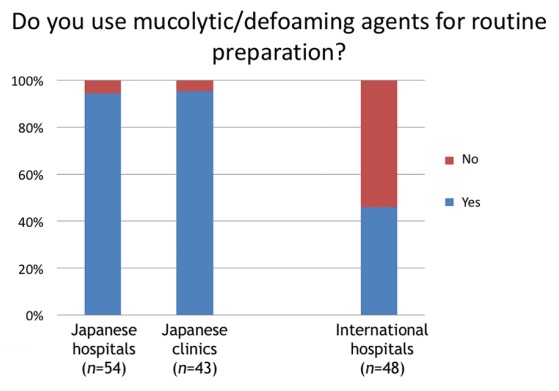
 РЯКЛРЧ clinicПЁМДТ transnasal endoscopyИІ ЛѓДчШї ИЙРЬ РЬПыЧЯАэ РжБКПф. ПьИЎГЊЖѓПЁМДТ ИХПь ЕхЙААд РЬПыЕЫДЯДйИИ...
РЯКЛРЧ clinicПЁМДТ transnasal endoscopyИІ ЛѓДчШї ИЙРЬ РЬПыЧЯАэ РжБКПф. ПьИЎГЊЖѓПЁМДТ ИХПь ЕхЙААд РЬПыЕЫДЯДйИИ...
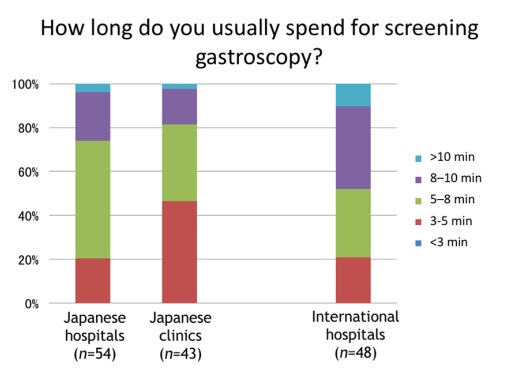 ЛѓКЮРЇРхАќ ГЛНУАцРЧ АЫЛч НУАЃРК ПЊНУ 5Ка РќШФАЁ АЁРх ИЙРК АЭ ААНРДЯДй. 3КаРК КаИэШї КЮСЗЧб НУАЃРдДЯДй.
ЛѓКЮРЇРхАќ ГЛНУАцРЧ АЫЛч НУАЃРК ПЊНУ 5Ка РќШФАЁ АЁРх ИЙРК АЭ ААНРДЯДй. 3КаРК КаИэШї КЮСЗЧб НУАЃРдДЯДй.
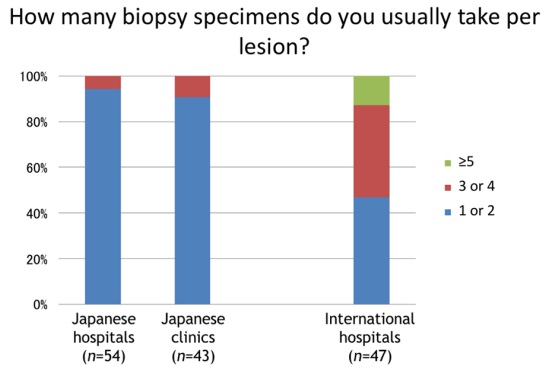 РЯКЛЛчЖїЕщРК КДМв Дч СЖСїАЫЛч МіАЁ ИХПь РћНРДЯДй. ЧбАГ ШЄРК ЕЮАГ СЄЕЕ target biopsy ЧЯДТ АЭРЬ РЯКЛ НКХИРЯРдДЯДй.
РЯКЛЛчЖїЕщРК КДМв Дч СЖСїАЫЛч МіАЁ ИХПь РћНРДЯДй. ЧбАГ ШЄРК ЕЮАГ СЄЕЕ target biopsy ЧЯДТ АЭРЬ РЯКЛ НКХИРЯРдДЯДй.
![]() РЇОЯ ПЕПЊПЁМ АЁРх ПЕЧтЗТРЬ ГєРК ГэЙЎ 100АГ (Powell AG. Int J Surg 2016)
РЇОЯ ПЕПЊПЁМ АЁРх ПЕЧтЗТРЬ ГєРК ГэЙЎ 100АГ (Powell AG. Int J Surg 2016)
РЇОЯ ПЕПЊПЁМ АЁРх ПЕЧтЗТРЬ ГєРК ГэЙЎ 100АГАЁ ЙпЧЅЕЧОњНРДЯДй. 1ЕюРК ParsonnetРЧ 1991Гт NEJM ГэЙЎ Helicobacter pylori infection and the risk of gastric carcinoma РЬОњНРДЯДй. 100РЇ ГЛПЁ ПьИЎГЊЖѓ ГэЙЎРЬ 3АГ РжОњНРДЯДй
7РЇ. МПяДы ГЛАњ ЙцПЕСж БГМіДдРЧ 2010Гт Lancet ГэЙЎ Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial
50РЇ. ЧбИВДыПЁ АшМЬАэ NCI ПЌМі Сп ЙкБйФЅ БГМіДдРЬ РлМКЧб 1994Гт Proc Natl Acad Sci U S A ГэЙЎ Genetic changes in the transforming growth factor beta (TGF-beta) type II receptor gene in human gastric cancer cells: correlation with sensitivity to growth inhibition by TGF-beta
61РЇ. ПЌММДы ПмАњ 2000Гт Br J Surg ГэЙЎ Recurrence following curative resection for gastric carcinoma
![]() ХЉЗаКД ШЏРкРЧ РЇГЛНУАц МвАп
ХЉЗаКД ШЏРкРЧ РЇГЛНУАц МвАп
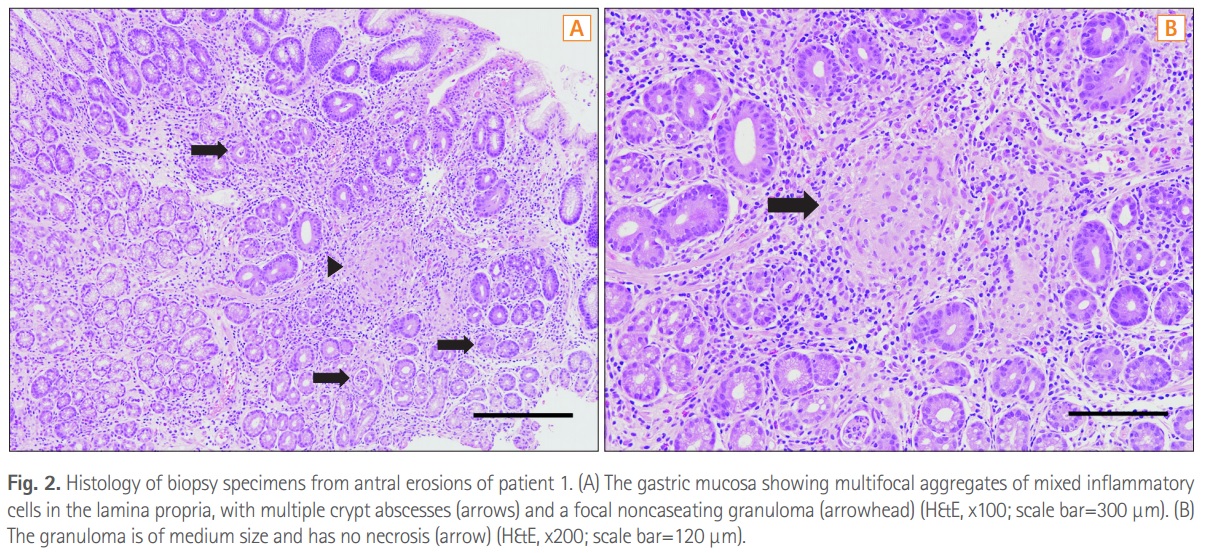
Intestinal Research 2016Гт УЙШЃПЁ НЧИА Gastric lesions in patients with CrohnЁЏs disease in Korea: a multicenter studyИІ МвАГЧеДЯДй. ХЉЗа ШЏРкПЁМ gastric noncaseating granulomaАЁ prognostic valueИІ АЁСњ Мі РжДйДТ АсЗаРЬ НХМБЧпНРДЯДй.
Methods: Among 492 patients with CD receiving upper gastrointestinal (GI) endoscopic evaluation in 19 Korean hospitals, we evaluated the endoscopic findings and gastric histopathologic features of 47 patients for our study. Histopathologic classification was performed using gastric biopsy tissues, and H. pylori infection was determined using the rapid urease test and histology. Results: There were 36 men (76.6%), and the median age of patients at the time of upper GI endoscopy was 23.8 years (range, 14.2-60.5). For CD phenotype, ileocolonic disease was observed in 38 patients (80.9%), and non-stricturing, nonpenetrating disease in 31 patients (66.0%). Twenty-eight patients (59.6%) complained of upper GI symptoms. Erosive gastritis was the most common gross gastric feature (66.0%). Histopathologically, H. pylori-negative chronic active gastritis (38.3%) was the most frequent finding. H. pylori testing was positive in 11 patients (23.4%), and gastric noncaseating granulomata were detected in 4 patients (8.5%). Gastric noncaseating granuloma showed a statistically significant association with perianal abscess/fistula (P=0.0496).

![]() РЮЕЕПЁМ ИИМК МвРх МГЛчРЧ ПјРЮ
РЮЕЕПЁМ ИИМК МвРх МГЛчРЧ ПјРЮ
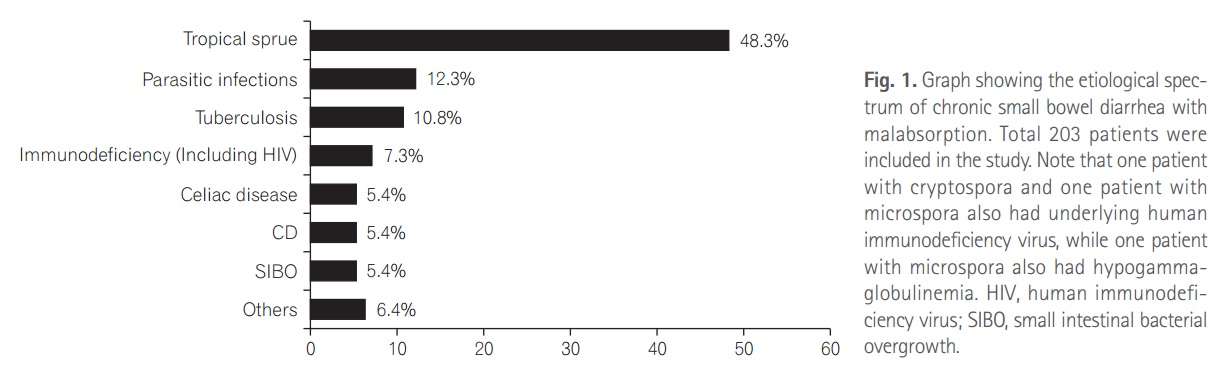
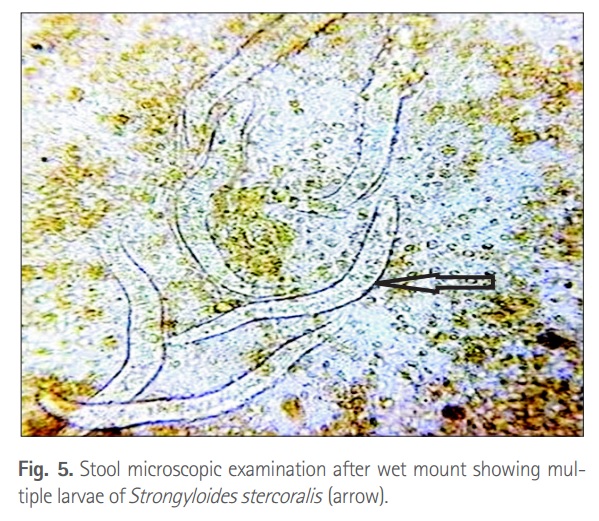
Intestinal Research 2016Гт УЙШЃПЁ НЧИА Spectrum of chronic small bowel diarrhea with malabsorption in Indian subcontinent: is the trend really changing?РЛ МвАГЧеДЯДй. РЮЕЕПЁМДТ Л§АЂКИДй БтЛ§УцСѕРЬ ОЦСїЕЕ СпПфЧб КЮКаРЛ ТїСіЧЯАэ РжОњНРДЯДй. КаМБУц (Strongyloides stercoralis)ЕЕ ШяЙЬЗгБКПф.
© РЯПјГЛНУАцБГНЧ ЙйИЅГЛНУАцПЌБИМв РЬСиЧр