EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [논문 읽기 2016년 3월]
[논문 읽기 2016년 3월]
![]() REGATTA trial - 일본과 한국의 외과 선생님들의 공동연구인 REGATTA trial 결과가 발표되었습니다 (Fujitani K. Lancet Oncology 2016). 양국 위암관련 내외과의사들의 첫 공동연구입니다. 훌륭한 성과 축하합니다.
REGATTA trial - 일본과 한국의 외과 선생님들의 공동연구인 REGATTA trial 결과가 발표되었습니다 (Fujitani K. Lancet Oncology 2016). 양국 위암관련 내외과의사들의 첫 공동연구입니다. 훌륭한 성과 축하합니다.
단일 전이가 있는 환자가 대상이었습니다. "We did an open-label, randomised, phase 3 trial at 44 centres or hospitals in Japan, South Korea, and Singapore. Patients aged 20-75 years with advanced gastric cancer with a single non-curable factor confined to either the liver (H1), peritoneum (P1), or para-aortic lymph nodes (16a1/b2) were randomly assigned (1:1) in each country to chemotherapy alone or gastrectomy followed by chemotherapy."
등록된 환자는 175명이었으나 참여 기관이 44곳이나 되었던 연구입니다. 한 기관에서 4명만 등록되었으니 상당한 우여곡절이 있었을 것 같습니다. 게다가 23명 (13.1%)은 항암치료도 받지 못하였읍니다. 여하튼 결과는 명확했습니다. "Median overall survival was 16·6 months (95% CI 13·7-19·8) for patients assigned to chemotherapy alone and 14·3 months (11·8-16·3) for those assigned to gastrectomy plus chemotherapy (hazard ratio 1·09, 95% CI 0·78-1·52; one-sided p=0·70)."
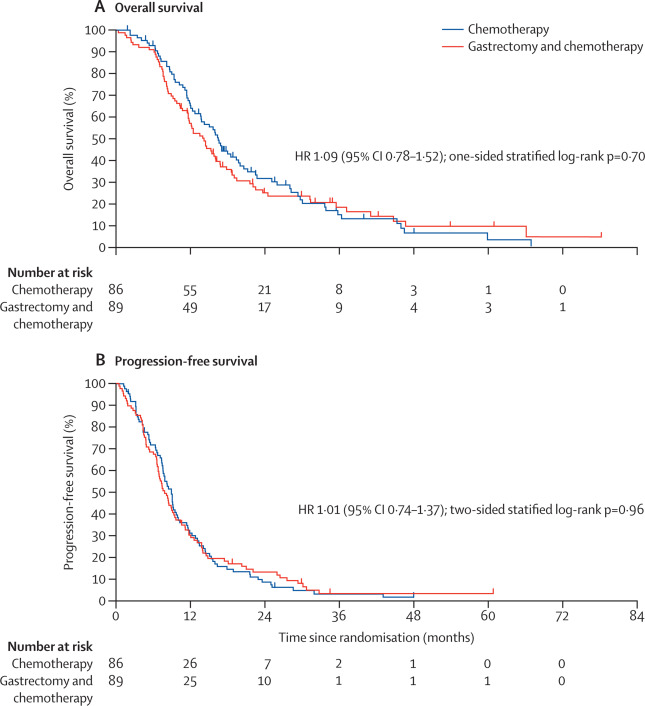
결론은 다음과 같았습니다. "Since gastrectomy followed by chemotherapy did not show any survival benefit compared with chemotherapy alone in advanced gastric cancer with a single non-curable factor, gastrectomy cannot be justified for treatment of patients with these tumours." 쓸모없는 수술은 하지 말자는 것 같습니다.
국내 언론에 관련 기사가 실렸습니다. [2016-2-26. 경향신문] 말기 위암의 위절제술 생존율 높이기 어려워
![]() Cancer screening in LT patients
Cancer screening in LT patients
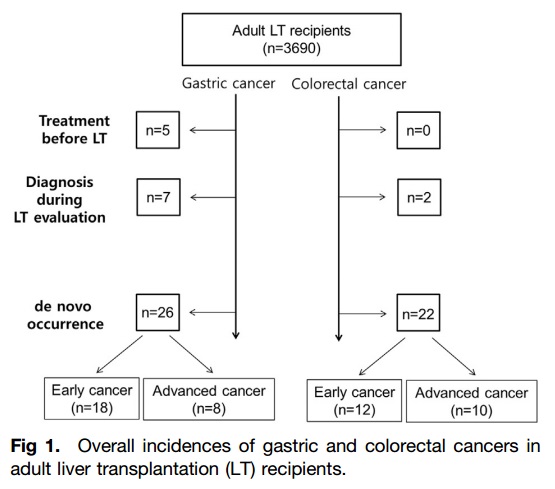
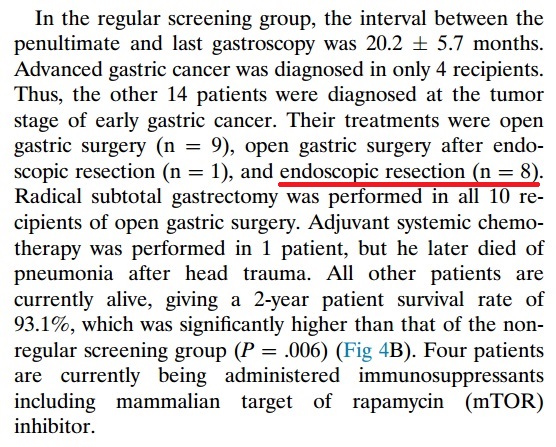
간이식 환자에서 암검진의 효과에 대한 아산병원 자료가 발표되었습니다 (Jung DH. Transplant Proc 2016 ). 정기적인 검진을 받으면 조기진단이 가능하고 생존율이 향상된다고 합니다. 논문에는 아산병원의 간이식 환자의 암검진 프로토콜이 소개되어 있었습니다.

제가 흥미롭게 본 것은 LT 전후 위암의 발견과 임상 경과였습니다. LT 후 검진을 통해 발견된 위암의 절반 정도를 내시경으로 치료했다는 점이 중요할 것 같습니다.
저도 간이식 후 위암환자를 몇 분 치료한 경험이 있습니다. 일전에 EndoTODAY에서 소개한 바 있는데 아래에 옮깁니다 (EndoTODAY 20130807).
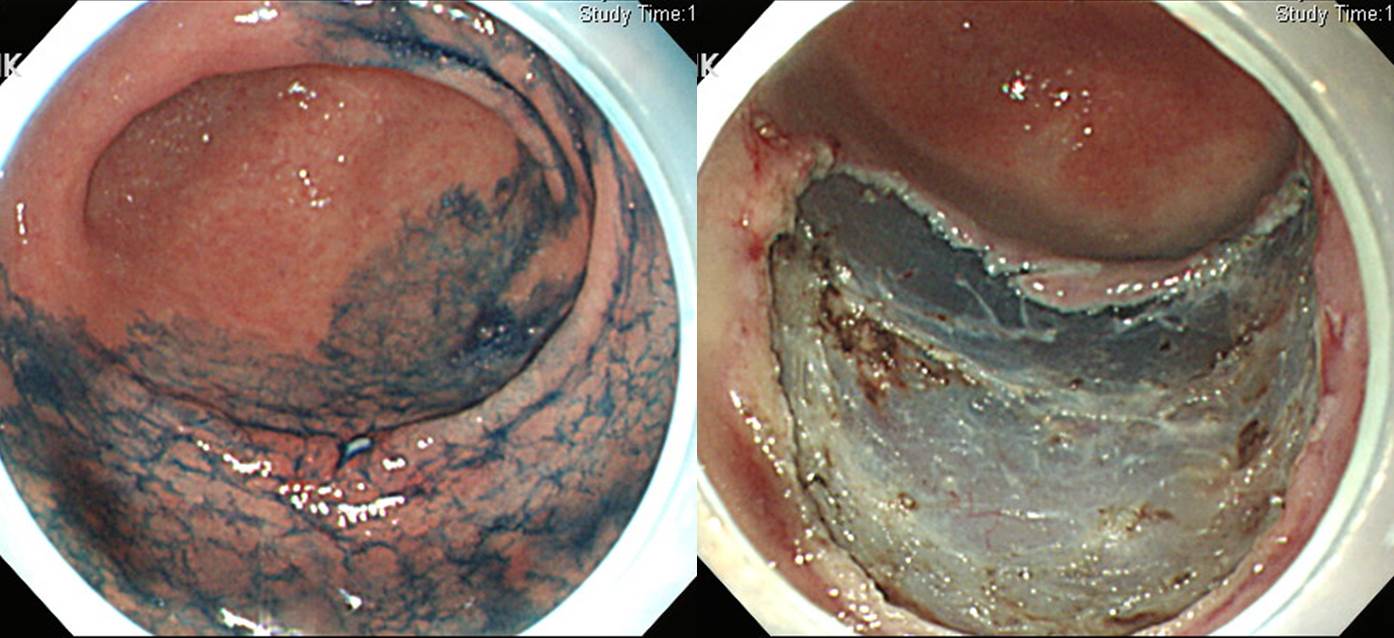
간경변으로 3년 5개월 전 간이식 수술을 받은 환자로 최근 위에서 high grade dysplasia가 발견되어 의뢰되었습니다. 내시경 사진을 검토한 후 위암일 가능성이 50% 정도는 된다고 평가를 하였으며 내시경절제술을 추천하였습니다. ESD를 시행하였고 아래와 같은 병리결과를 얻어 complete resection으로 판정하였습니다.
병리결과: Tubular adenocarcinoma, well differentiated, 2.4x0.9cm, Depth of invasion : invades mucosa (muscularis mucosa), Resection margin: free from carcinoma
간이식을 받은 환자였으므로 시술 전 면역억제제를 어떻게 조절할 것인가로 고민을 하였습니다 (tacrolimus와 mycophenolate를 사용하고 있었음). 외과 담당 선생님과 상의하여 "간이식 받은 지 오래 되었고, 현재 간기능 정상이므로 면역억제제를 1~2일 중단하는 것은 크게 무리가 없겠다"는 답변을 받고 2일간 투약을 중지하였습니다. 이 환자의 경우는 문제없이 퇴원을 하셨습니다만, 간 이식을 받은 지 얼마되지 않은 환자가 오신다면 어떻게 할지 고민이 됩니다. Individualize 할 수 밖에 없는 문제라고 생각합니다.
![]() Mixed histology in ESD candidates
Mixed histology in ESD candidates
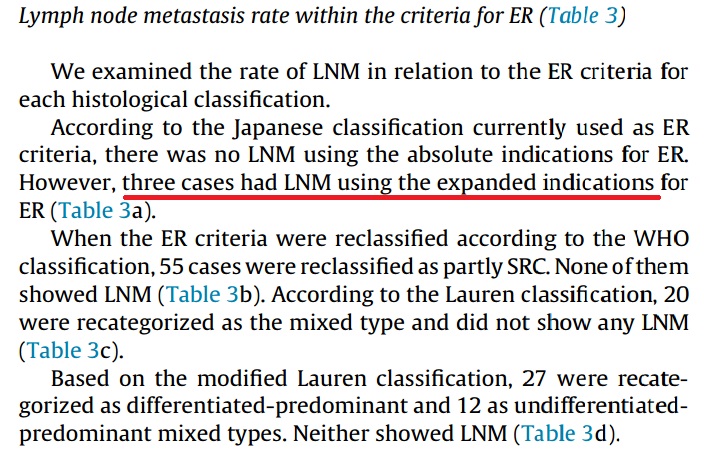
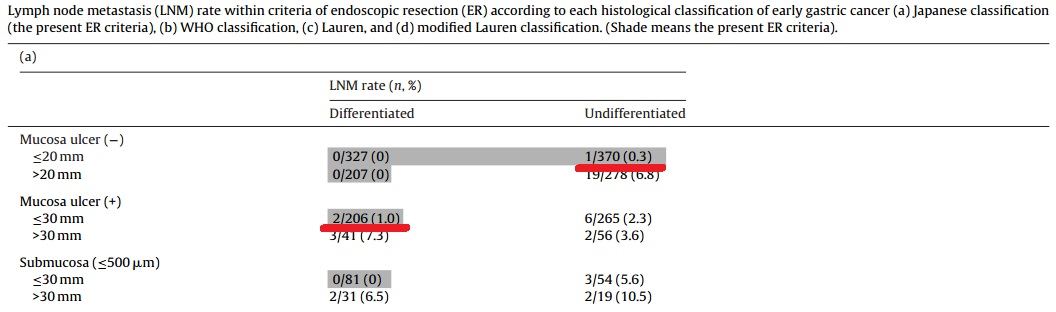
연세대학교 강남세브란스병원 김지현 교수님팀에서 수술 환자의 병리결과를 새로운 각도로 분석한 논문이 발표되었습니다 (Yoon HJ. Pathol Res Pract 2016).
제가 흥미롭게 본 것은 ESD 적응증에 해당하는 환자의 림프절 전이 양상입니다. 자료가 축적될수록 '일부 expanded indication에서 림프절 전이가 분명히 존재한다'는 것이 명백해지고 있습니다. 3 cm 이하의 분화형 점막암에서도 궤양이 있는 경우에는 림프절 전이를 반드시 고려해야 할 것 같습니다. 점막하암은 말할 나위도 없습니다.
이 연구의 내용을 처음 본 것은 2014년 KINGCA였습니다 (링크). 당시 제가 comment 하였던 내용을 아래에 옮깁니다.
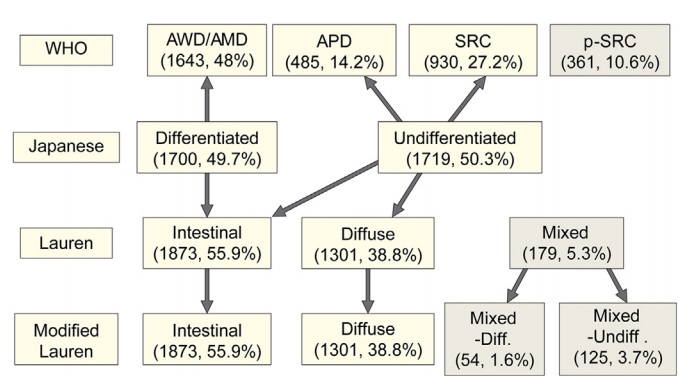
연세대학교에서 'Is new criteria for mixed histology is necessary for endoscopic resection in EGC?'라는 제목의 발표를 하였습니다. 제가 흥미롭게 본 것은 Japanese classification입니다. 우리는 흔히 일본에서 말하는 differentiated cancer는 WHO 분류로 well-differentiated와 moderately-differentiated adenocarcinoma를 합한 것과 비슷하다고 생각합니다. 그런데 이번 발표를 보니 일본 분류에서 differentiated가 49.7%인 반면 well-differentiated와 moderately-differentiated adenocarcinoma의 합은 48%였습니다. 즉 2% 차이가 있습니다. 이 환자들은 어떤 조직학적 특징인 있는지 궁금할 뿐입니다. 일본 분류를 WHO 분류와 mapping하는 일은 무척 어려운 일입니다. 2 프로 부족합니다.

좋은 논문 축합니다.
![]() Non-Helicobacter bacteria in the stomach
Non-Helicobacter bacteria in the stomach
서울대 김나영 교수님께서 위점막에서 헬리코박터 이외의 nitrosating or nitrate-reducing bacteria의 존재를 pyrosequencing으로 찾아본 결과를 발표하셨습니다 (Jo HJ. Helicobacter 2016 - Epub).
RESULTS: The number of NB other than HP (non-HP-NB) was two times higher in the cancer groups than in the control groups, but it did not reach statistical significance. The number of non-HP-NB tends to increase over time, but this phenomenon was prevented by HP eradication in the HP-positive control group, but not in the HP-positive cancer group.
CONCLUSION: We could not find the significant role of bacteria other than HP in the gastric carcinogenesis.
이 그림의 의미는 무엇일까?
![]() Role of second look endoscopy after gastric ESD
Role of second look endoscopy after gastric ESD
ESD 후 이차 내시경 (second look endoscopy, SLE)의 유용성에 대한 새로운 분석입니다 (Kim SJ. World J Gastrointest Endoc 2016 - Epub). 문헌에서 제시된 표와 같이 ESD 후 이차 내시경의 유용성을 검증한 모든 논문은 negative date였습니다.
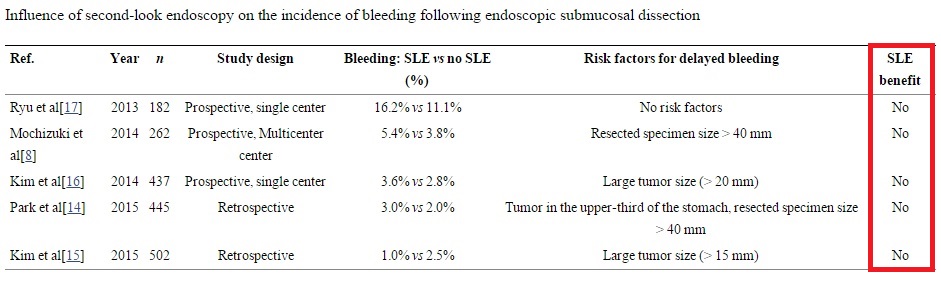
이번 문헌에는 고위험 환자에서 선택적인 이차 내시경은 도움될지 모른다는 언급이 있습니다 ("SLE might be an important tool for the prevention of the delayed bleeding in selected high-risk patients"). 그러나 저는 이와 같은 언급을 신뢰하지 않습니다. 기존 연구에서 이차 내시경의 효과가 예외없이 부정되었고, 출혈 자체의 빈도가 낮고, 입원 환자의 출혈은 잘 관리될 수 있기 때문입니다.
저의 결론은 이렇습니다. "ESD 후 second look endoscopy의 역할은 입증된 바 없습니다. 지금까지 모든 연구는 negative 결론입니다."
* 참고: EndoTODAY ESD 후 이차 내시경
![]() Colonoscopy surveillance after colorectal cancer resection
Colonoscopy surveillance after colorectal cancer resection
대장암 수술 후 대장내시경에 대한 US multi-society task force 가이드라인이 나왔습니다 (Kahi CJ. GIE 2016). 대장암 수술 1년 후 대장내시경을 하고, 문제가 없으면 3년 후(=수술 4년 후), 또 문제가 없으면 5년 후(=수술 9년 후)에 검사하도록 권하고 있습니다. 우리나라에서는 조금 더 자주 할 수 있겠지만, 그렇다고 너무 자주 하는 것은 좋지 않다고 생각합니다. 예를 들어 매년 검사하는 것은 분명 over입니다.
Recommendation: We recommend that patients who have undergone curative resection of either colon or rectal cancer receive their first surveillance colonoscopy 1 year after surgery (or 1 year after the clearing perioperative colonoscopy).
Recommendation: We recommend that, after the 1-year colonoscopy, the interval to the next colonoscopy should be 3 years (ie, 4 years after surgery or perioperative colonoscopy) and then 5 years (ie, 9 years after surgery or perioperative colonoscopy). Subsequent colonoscopies should occur at 5-year intervals until the benefit of continued surveillance is outweighed by diminishing life expectancy. If neoplastic polyps are detected, the intervals between colonoscopies should be in accordance with published guidelines for polyp surveillance intervals. These intervals do not apply to patients with Lynch syndrome.
![]() Clip artifact
Clip artifact
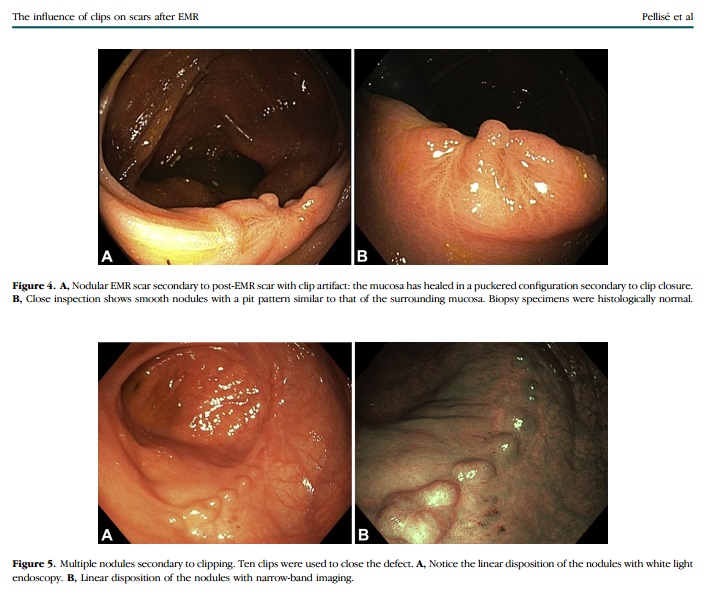
대장 ESD 후 clip에 의한 artifact를 보여주는 흥미로운 논문이 있었습니다 (Pellise M. GIE 2016). 특징은 "nodular elevation of the mucosa with a normal pit pattern"라고 합니다.
![]() 간질 (Biliary fascioliasis diagnosed by EUS)
간질 (Biliary fascioliasis diagnosed by EUS)
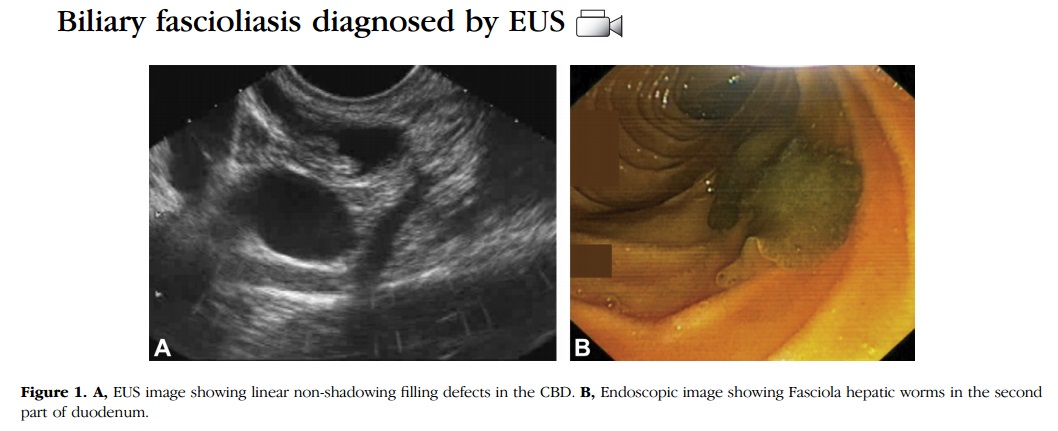
우상복부 통증으로 내원한 46세 여성에서 EUS로 진단하고 ERCP로 제거한 간질 증례가 보고되었습니다 (Mohamadnejad M. GIE 2016). 이란 증례였습니다. EUS에서 "mobile, free-floating cylindrical, nonshadowing filling defects"로 보였다고 합니다.
* 참고: EndoTODAY 간질 (Fasciola hepatica)
![]() 대장 ESD 천공
대장 ESD 천공
홍성노 교수님께서 내시경학회 ESD 연구회 registry data를 이용하여 대장 ESD 천공 예측 모델을 개발하였습니다(Hong SN. GIE 2016 - Epub). 아래 4개 인자가 중요하다고 합니다.
The risk score points attributed to each risk factor were weighted according to respective adjusted ORs in multivariate logistic regression of the derivation set. Respective adjusted ORs were rounded to the nearest whole number to keep the score simple. Points were assigned to each predictor for ESD-induced perforation as follows: tumor located in the colon (+2 points), tumor size at 1-cm increments (+1 point with 1-cm increments), endoscopist experience of greater than or equal to 50 ESDs (-1 point), and submucosal fibrosis (+2 points).
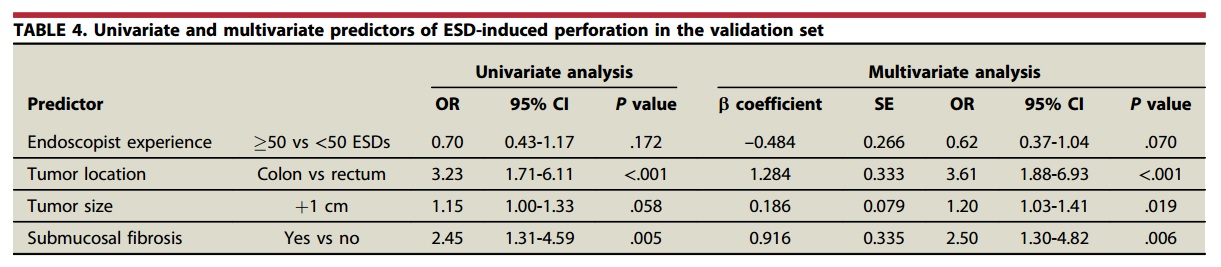
제가 더 흥미롭게 본 것은 천공의 빈도와 형태였습니다. 천공의 빈도가 6.6%(135/2,046)로 제 짐작보다 다소 높았습니다. Microperforation이 frank perforation보다 3배 가량 흔했다는 점도 조금 의외였습니다. 위 ESD와 대장 ESD는 사뭇 다른 모양입니다.
사실 저는 대장 ESD에 대하여 뭐라 말할 입장이 아닙니다. 경험이 없기 때문이지요. 저의 처음이자 마지막 대장 ESD입니다. Dual knife나 Flex knife가 없었기에 뾰족한 needle knife로 circumferential cutting을 하던 중 frank perforation이 발생하여 clipping하였습니다. 처절한 실패였습니다. 이 환자 이후로는 상부 ESD만 하고 있습니다.^^

좋은 연구 축하합니다.
![]() 수입에 따라 위암 치료가 달라진다?
수입에 따라 위암 치료가 달라진다?
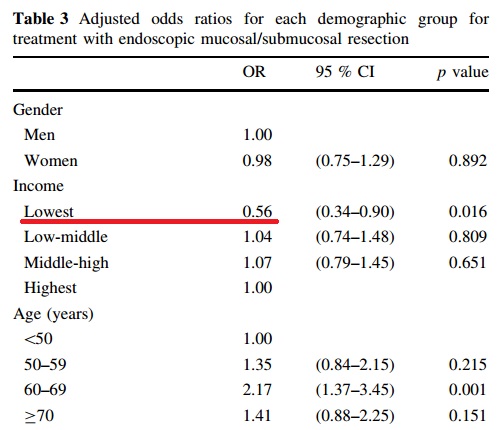
'Relationship between socioeconomic status and accessibility for endoscopic resection among gastric cancer patients'라는 흥미로운 논문을 소개합니다 (Kim NY. Gastric Cancer 2016). 위암 환자 중 소득이 낮은 20% 환자들은 다른 소득군에 비하여 내시경치료를 받을 확률이 낮다고 합니다. 가장 소득이 높은 20%에 비하여 odds ratio가 0.56이였습니다. 기전은 명확하지 않습니다. 저자들은 아마도 가난한 사람들이 검진을 덜 받기 때문일 것으로 추론하고 있습니다. 관련 데이타는 제시하지 못했지만...
우리나라처럼 의료비가 싼 나라에서도 소득에 따라 의료이용은 상당히 다릅니다. 싼 가격으로 모든 것을 통제하려는 정부의 시도는 실패할 수 밖에 없습니다. 저소득군의 건강수준을 높이기 위해서는 가격 할인 이외의 대책이 필요합니다. 공공의료를 확대해야 하는 것이지요.
![]() Gastric cancer screening in USA
Gastric cancer screening in USA
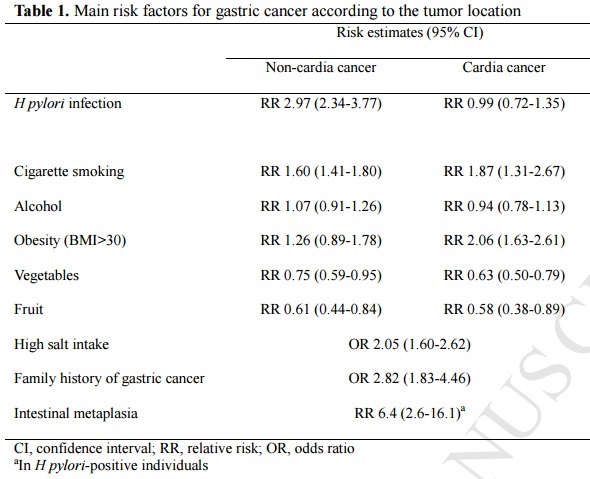
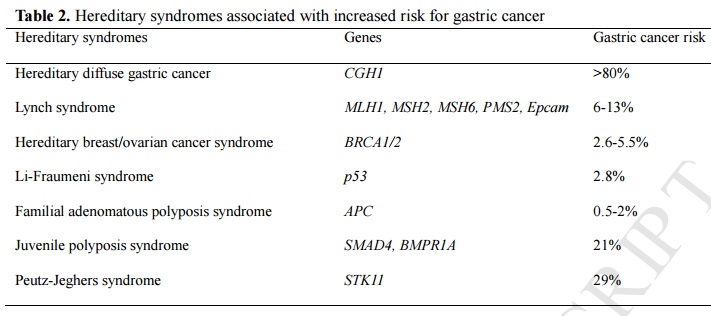
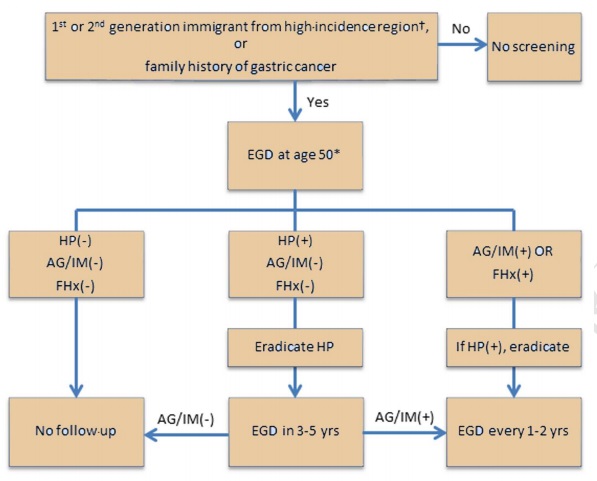
부산대학교 김광하 교수님께서 미국 연수 중에 GIE에 투고한 종설이 나왔습니다 (Kim GH. GIE 2016 - Epub). 제목은 "Screening and Surveillance for Gastric Cancer in the United States: Is it needed?" 위암이 많은 나라에서 온 이민자나 위암 가족력이 있는 사람에서는 검진이 필요하다고 주장하셨습니다.
![]() 잔위암에 대한 최근 종설 (Ohira. WJG 2016)
잔위암에 대한 최근 종설 (Ohira. WJG 2016)
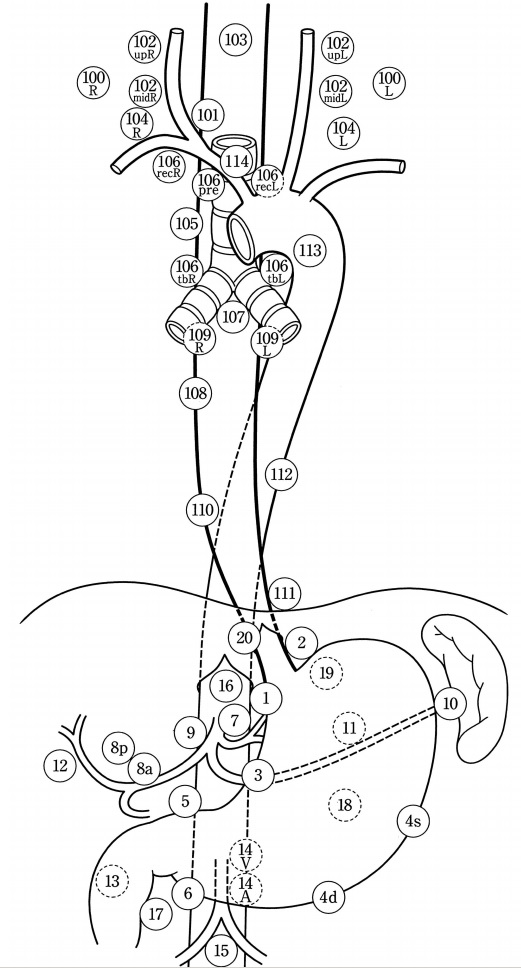
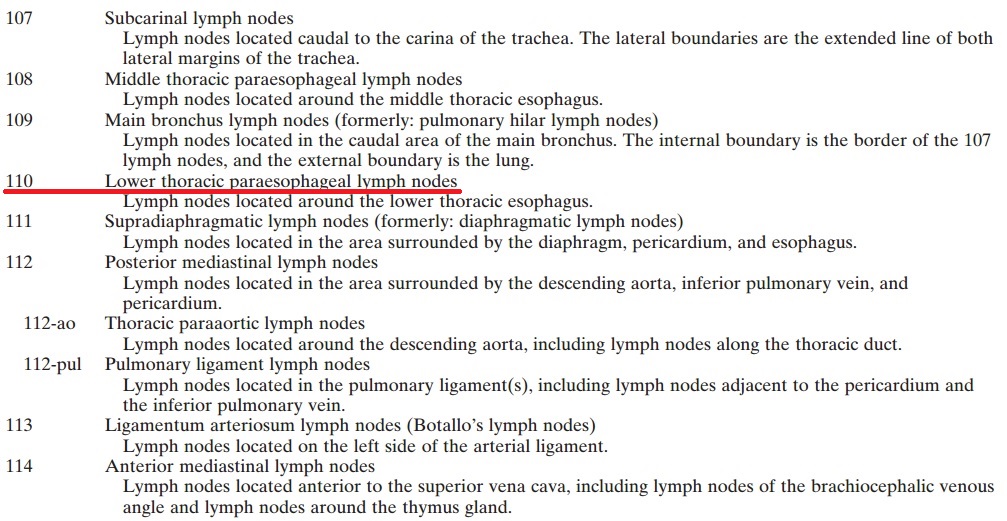
원위 위절제술 후 lymphatic drainage 양상에 변화가 일어납니다. 아마도 수술 과정에서 정상적인 lymphatics가 절제되기 때문일 것입니다. 그 결과 잔위암과 원발성 근위부 위암(primary proximal gastric cancer)의 림프절 전이에 약간의 차이가 발견됩니다. 잔위암에서는 splenic artery (11번), splenic hilum (10번), lower mediastinum (110, 111번), jejunal mesentery의 림프절 침윤이 흔합니다.
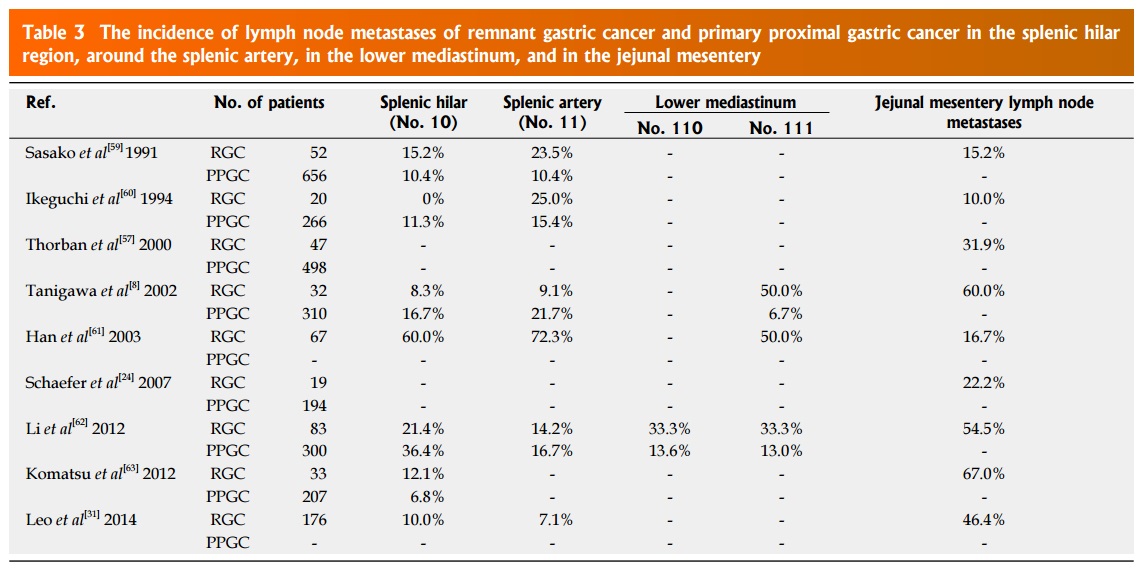
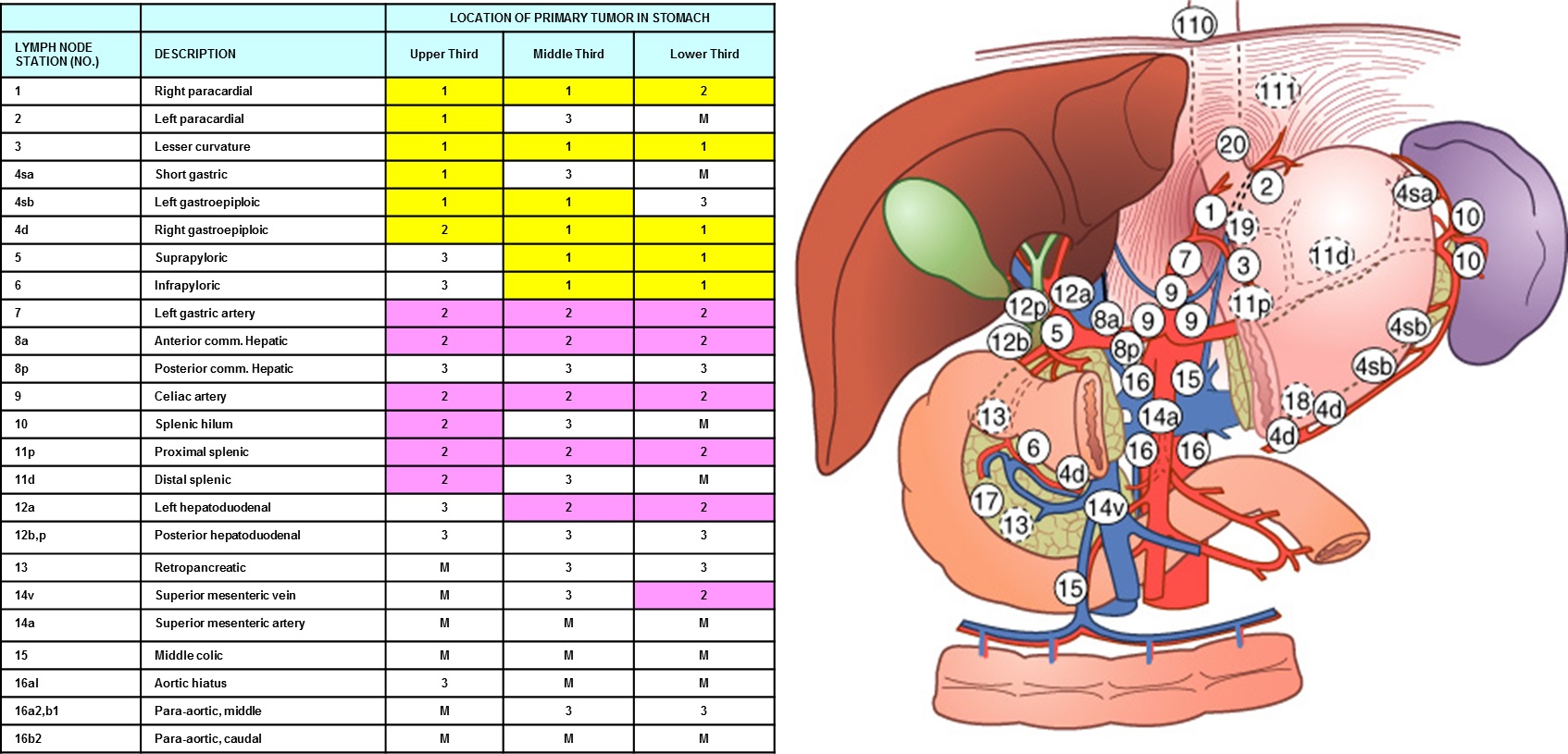
It has been reported that RGC has unique patterns of lymph node metastasis compared with PPGC. In PPGC, the main lymphatic flow drains to the lymph nodes along the celiac artery through the lymph nodes at the lesser curvature, the left gastric artery, and the right side of the cardia. In RGC, it has been considered that the characteristics of lymph node metastases are different from PPGC because abnormal lymphatic formation is induced as a result of cutting off these lymphatic pathways at the initial surgery. Furthermore, Tokunaga et al mentioned that altered lymphatic drainage after DG may affect the long-term survival of RGC patients with advanced stage disease. Previous studies have investigated the incidence of lymph node metastasis focusing on around the splenic artery, in the splenic hilum, at the lower mediastinum, and in the jejunal mesentery. Some authors demonstrated a higher incidence of lymph node metastasis around the splenic artery, in the splenic hilum, and at the lower mediastinum in RGC; therefore, lymphadenectomy of these regions is recommended for curative surgery. In patients with previous B-II reconstruction, the rate of lymph node metastases in the jejunal mesentery has been reported to be 10.0%-67%. Thorban et al reported that RGC patients with lymph node metastases in the jejunal mesentery had a poor prognosis, with a median survival time (MST) of 13.2 mo. Similarly, Leo et al reported that RGC patients with lymph node metastases in the jejunal mesentery had worse outcomes than those with metastases in other lymph node stations. Therefore, jejunal mesentery lymph node dissection including the origins of each involved jejunal artery is recommended for RGC patients with previous B-II reconstruction. However, the details of the spread of lymph node metastases in RGC patients are still uncertain, because the number of patients examined in these studies was too small. (Ohira. WJG 2016)
미국와 일본의 흉부 림프절 명명법이 서로 다릅니다. 위 table에서 언급된 110, 111번은 일본식입니다. 미국 흉부외과쪽에서는 조금 다르게 부릅니다. 예를 들어 lower paratracheal nodes는 일본식으로는 110번, 미국식으로는 8L번입니다.
| 위치 | 서양식 | 일본식 |
| Lower paratracheal nodes | 8L | 110 |
| Diaphragmatic nodes | 15 | 111 |
| Paracardial nodes | 16 | 1 (右) 또는 2 (左) |
1) AJCC 7판에 따른 림프절 명명법
1L = left supraclavicular, 1R = right supraclavicular, 2L = left upper paratracheal, 2R = right upper paratracheal, 4L = left lower paratracheal, 4R = right lower paratracheal, 5 = aortopulmonary, 6 = anterior mediastinal, 7 = subcarinal, 8L = lower paraesophageal, 8M = middle paraesophageal, 9 = pulmonary ligament, 10L = left tracheobronchial, 10R = right tracheobronchial, 15 = diaphragmatic, 16 = paracardial, 17 = left gastric, 18 = common hepatic, 19 = splenic, 20 = celiac. The posterior mediastinal lymph node (3P) is not shown.
2) 일본 식도질환학회 림프절 명명법 (Esophagus 2004;1:61-88)
© 일원내시경교실 바른내시경연구소 이준행