 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [StomachTODAY 026. Open question]
[StomachTODAY 026. Open question]
EndoTODAY 애독자 한 분께서 질문을 주셨는데 제가 답변할 수 없었습니다. 여러 선생님들께 여쭙고자 하오니 부디 의견을 부탁드립니다.
[2018-2-14. 애독자 질문]
얼마 전 내원한 환자의 위내시경 소견으로 문의드립니다. 주변 분들과 펠로우시절 교수님께 문의드렸는데 모두들 처음보는 소견이라고 합니다.
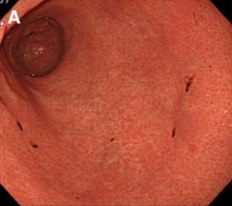
환자는 54세 남자고 폐결핵, 대상포진 과거력이 있습니다. 복통은 없으나 배가 부글거리는 증상이 기분 나쁘게 지속된다고 하여 내원하였습니다. 위,대장내시경, 복부CT 검사를하였는데 대장내시경이나 복부 CT에는 특이소견이 없었습니다. 위내시경에서 전정부는 정상이었고, 체부, 분문부, 저부에 미만성으로 5mm 이하 크기의 중심 헤마틴을 보이는 얕은 미란이 넓게 분포했습니다. 미란의 모양과 크기는 다양했고 점막부종도 동반되어 있었습니다. 사진을 첨부합니다. 교수님의 고견을 부탁드립니다.
참고가 되실지 모르겠는데요. 환자는 의료급여자로 약간 위생상태가 안 좋아보이지만 심한 편은 아니었습니다.


Peripheral blood eosinophil : 13.8%
RPR Ab : 음성
위내시경 조직검사:
H. pylori : (-)
Neutrophils : (++)
Monocytes : (++)
Atrophy : (-)
Intestinal metaplasia : (-)
Diagnosis: Chronic active gastritis, moderate with erosion and prominent eosinophilic infiltrate.
[2018-2-19. 애독자 1 답변]
Eosinophilic gastritis 로 진단해도 되지 않을까요? 조직검사에서 HPF당 eosinophil count를 해보면 진단이 될 것 같습니다.
[2018-2-19. 애독자 2 답변]
내시경 소견이 쉽지는 않지만 결국 내시경소견은 raised erosive gastritis라고 진단할 수 있지 않을까 생각합니다. Peripheral eosinophilia와 Bx에서 prominent eosinophilic infiltrate가 있었던 것을 고려하고, 위장 외에 십이지장, 식도에 특이소견이 없다면 (내시경 사진이 없어서 알 수 없습니다만…) 내시경 + 병리소견을 종합한 진단은 Eosinophilic gastritis라고 할 수 있을 것 같습니다. 아마도 약물에 의한 반응으로 생각되며 eosinophilia가 있었던 것도 약물에 의한 systemic reaction을 시사하는 소견이라고 생각합니다.
[2018-2-20. 애독자 3 답변]
제가 본 소견으로는 이 사진들은 헤마틴 침착이 아니라 "봉소염성 위염(phlegnomous gastritis)" 양상으로 발현된 "호산구성 위염(eosinophlic gastritis)"입니다.
참고로 헤마틴 침착은 아래 그림과 같이 보입니다. 위내 pH가 지나치게 낮을 때 발생하는 벽내출혈반이라서 부종이 없고, 위 사진보다 훨씬 더 적은 수의 발적들이 납작하고 단정하게 보입니다.
문의하신 사진은 "pus, mucosal edema, cell infiltration이 심한 suppurative reaction"으로, phlegnomous gastritis 소견으로 보입니다. 다만, "세균 감염으로 인한 호중구 증가"가 아닌 "기생충 감염이나 약물 등으로 인한 호산구 증가"를 보이는 호산구성 위염일 것 같습니다.
[2018-2-22. 애독자 4 답변]
1. VDRL 검사를 한번더 해보시는것이.
2. Serun IgE level check 해 보심이..
3. 기생충 검사도..
4. 증상이 심하지 않을땐 경과관찰 1달 후 내시경 검사후 변화하는 양상을 확인 해 보는것도 좋을 듯 합니다.
[2018-2-21. 이준행 답변]
환자를 직접 보는 의사가 결정할 수 밖에 없다고 생각됩니다. 내시경 소견을 "pus, mucosal edema, cell infiltration이 심한 suppurative reaction"으로 보신 선생님 의견에 동의할 수 있는 상황이고, 조직검사에서 eosinophilic infiltration이 많고 CBC에서 호산구 증가를 보인 점을 고려하여 eosinophilic gastritis, r/o drug-induced 혹은 r/o parasite-related 등을 의심해보면 좋겠습니다. 증상이 경미하거나 저절로 좋아지면 경과관찰 정도면 좋겠지만 증상이 심하거나 악화되면 재검이 필요해 보입니다.
위 기생충은 드문데 수년 전 저희는 strongyloidiasis를 경험한 바 있습니다. 저희 증례와 문헌의 유사 증례를 소개합니다. 보통 감염되더라도 증상이 없는 경우가 많습니다. 드물게 위장관 궤양을 일으킬 수 있습니다.
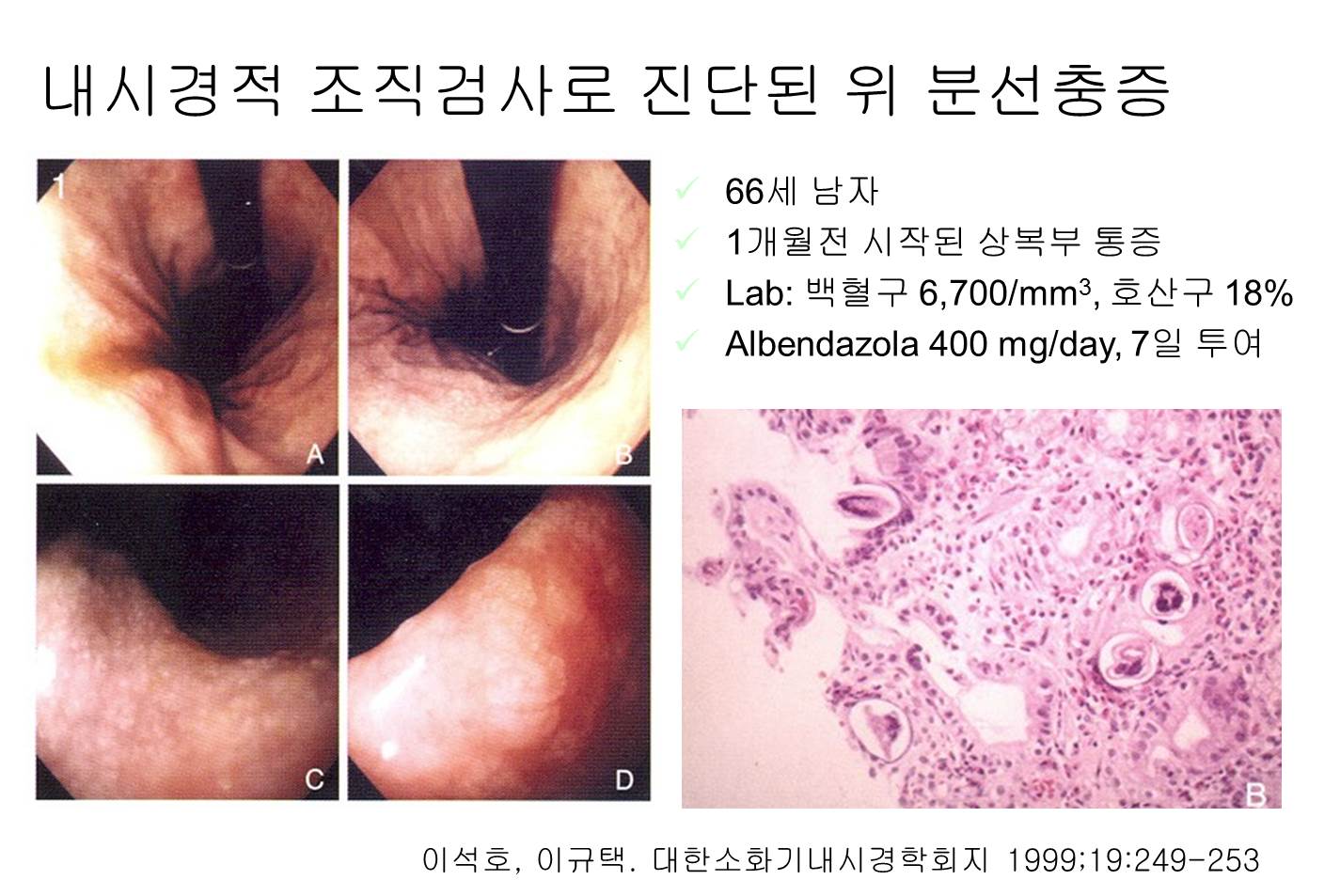
A 67-year-old man with a history of kidney transplantation for renal cell carcinoma presented for esophagogastroduodenoscopy for epigastric pain. The pain was described as a burning sensation, occurring four times a day. In a review of systems, the patient also endorsed intermittent nausea and vomiting, loss of appetite, and a five-pound weight loss over 3 weeks. Of note, he was on dual immunosuppressive therapy (mycophenolate and tacrolimus) as well as a recent prednisone taper due to suspicion of mild transplant rejection. Upper endoscopy showed antral nodules, erythema, and diffuse superficial erosions (a). The duodenal bulb also appeared diffusely erythematous with superficial erosions (b). Histologic examination was negative for Helicobacter pylori or cytomegalovirus but showed numerous larvae in the duodenal crypts and gastric pits consistent with strongyloidiasis (c). The patient was put on 12 mg of Ivermectin by mouth daily for two weeks. When he was seen by his primary-care physician one month after hospital discharge, the epigastric pain had resolved. Stool studies detected no remaining strongyloides. Given the resolution of his symptoms and negative stool studies, repeat endoscopy was not performed. (Am J Gastroenterol 2016)
![]() [References]
[References]
1) EndoTODAY 위염
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.