EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [십이지장 암. Duodenal cancer] - 終
[십이지장 암. Duodenal cancer] - 終
1. 소장암 개요
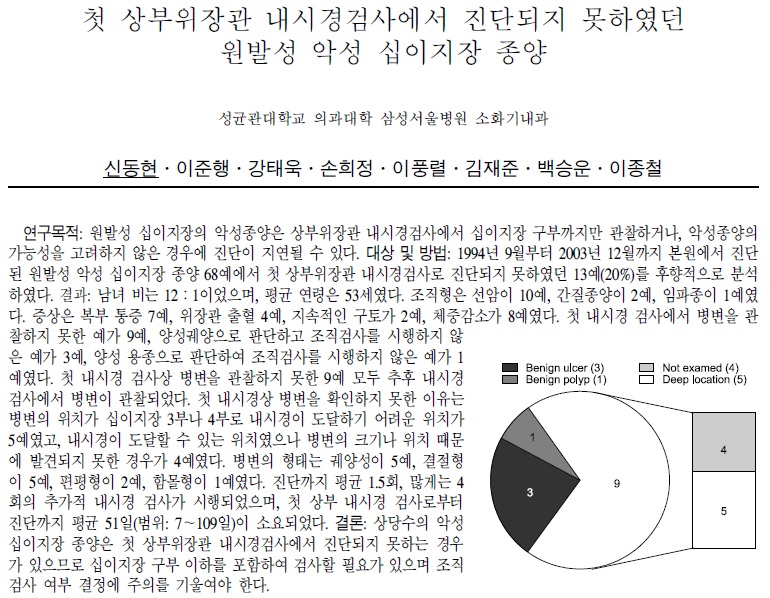
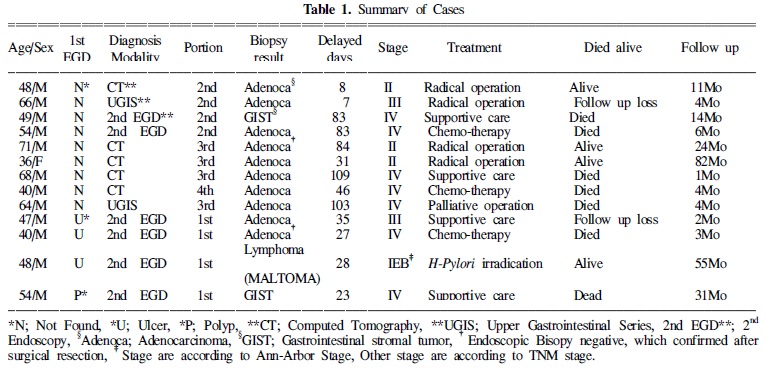
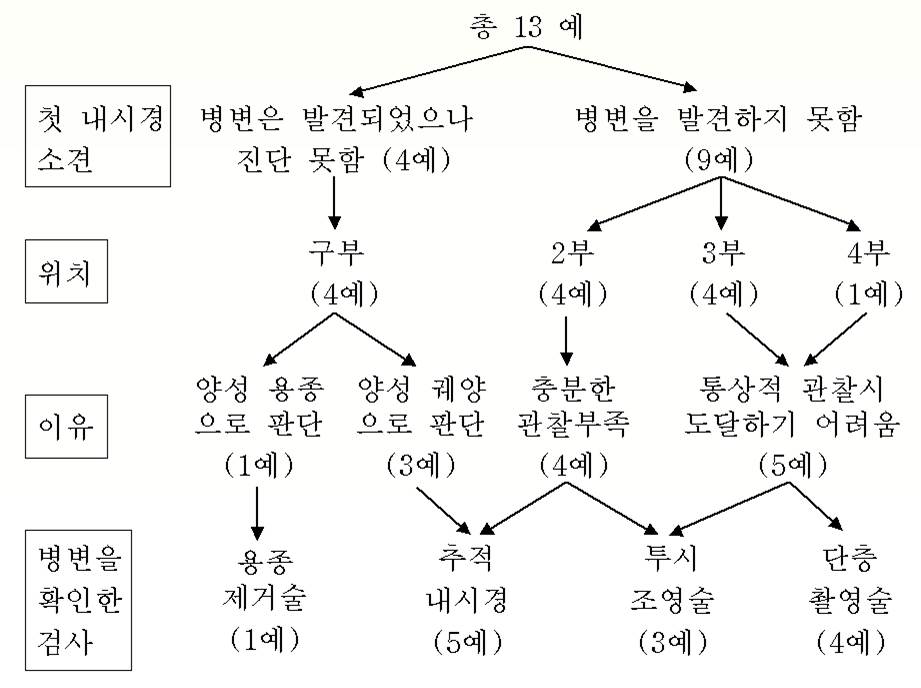
2. 첫 상부위장관 내시경 검사에서 진단되지 못한 원발성 악성 십이지장 종양
3. 상부위장관 내시경으로 도달할 수 있는 부위의 십이지장암
4. 상부위장관 내시경으로 도달할 수 없는 부위의 십이지장암
5. FAQs
6. References
![]() 1. 소장암 개요
1. 소장암 개요
소장(small bowel)은 약 5-6 미터로 소화관 전체 길이의 75%이고, 흡수면적의 90% 이상을 차지합니다. 소장 종양은 모든 소화관 종양의 1-5%를 차지하며 발생률은 10만명당 1예 이하입니다.
소장의 종양이 적은 이유는 명확하지 않은데 어떤 책에서 옮기면 아래와 같습니다.
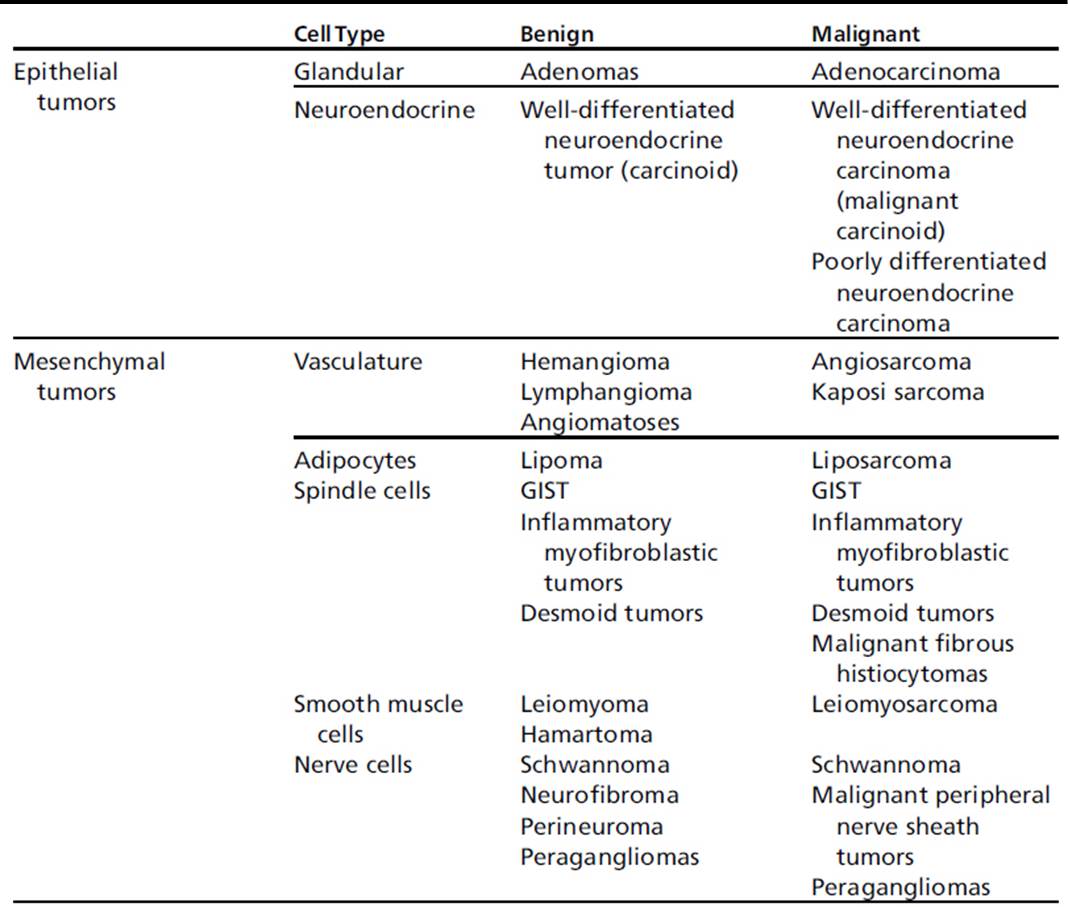
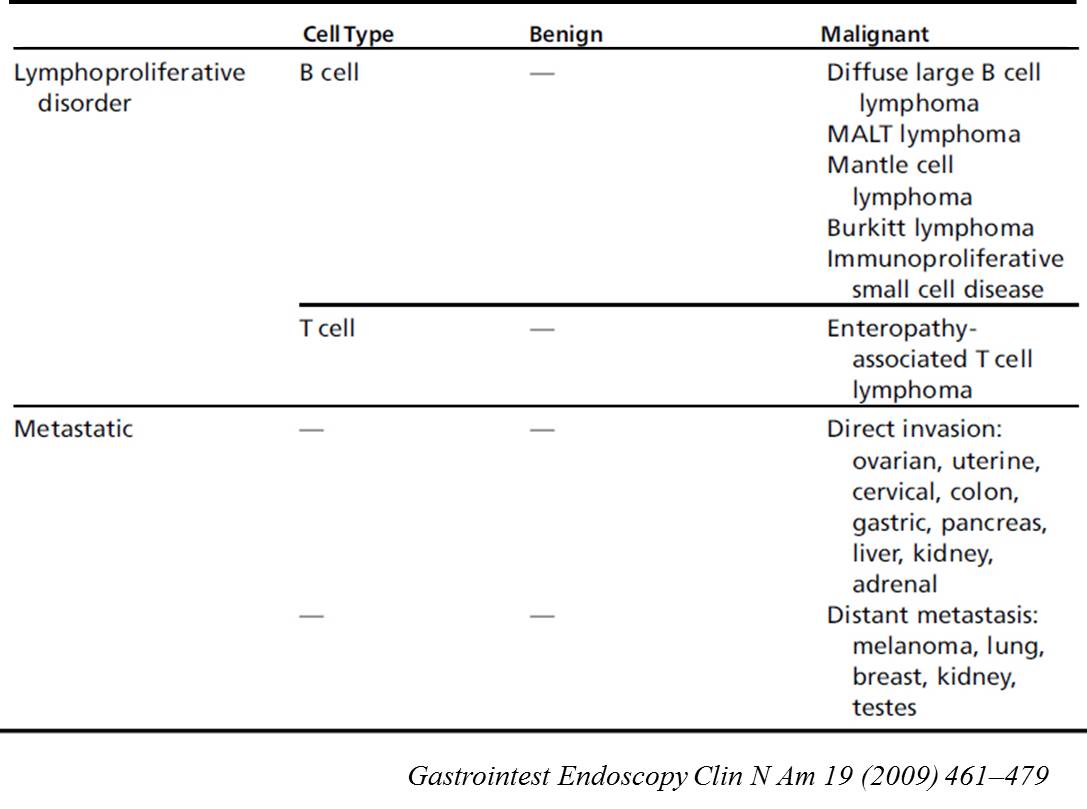
소장 종양의 분류
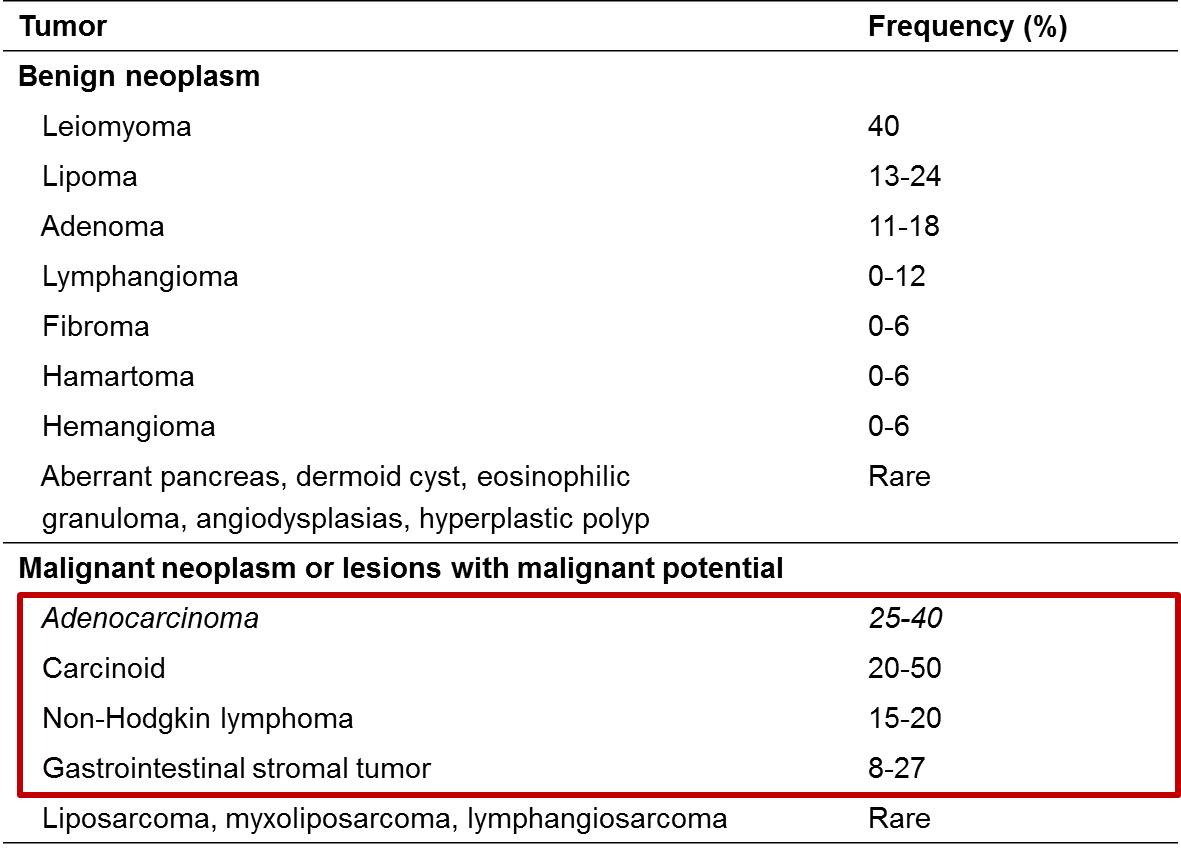
소장 종양의 상대적 빈도
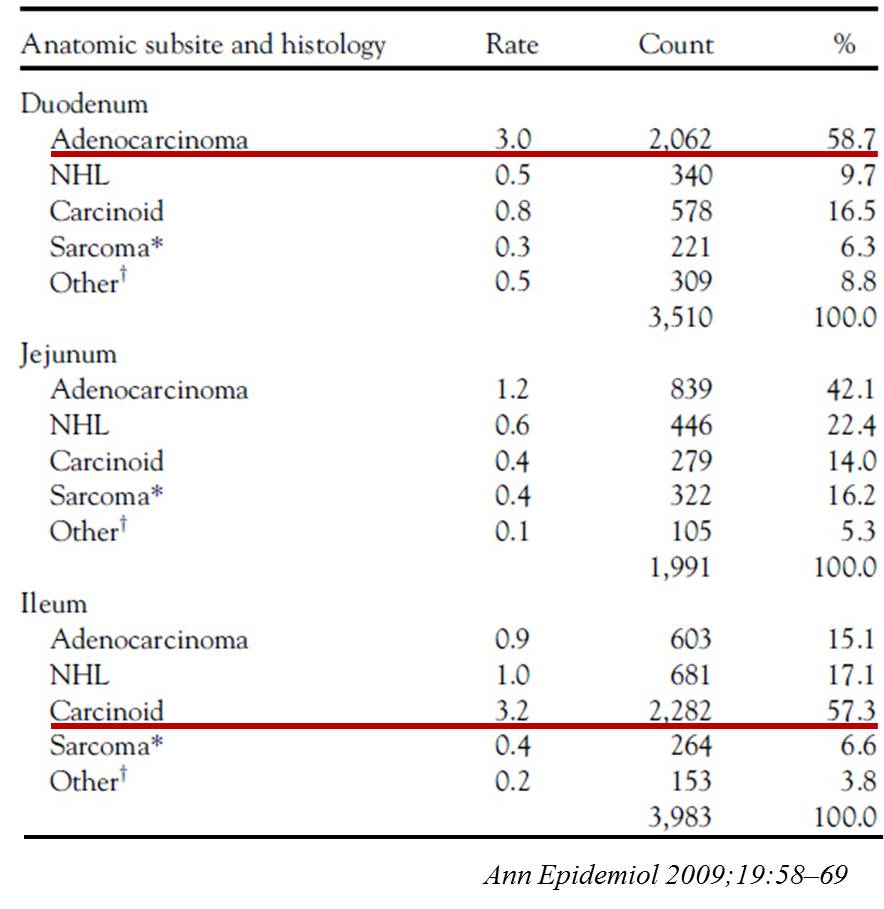
위치별 소장 종양의 상대적 빈도. 십이지장에는 adenocarcinoma가 많고, 회장에는 carcinoid가 많습니다. Lymphoma는 고루 분포합니다.
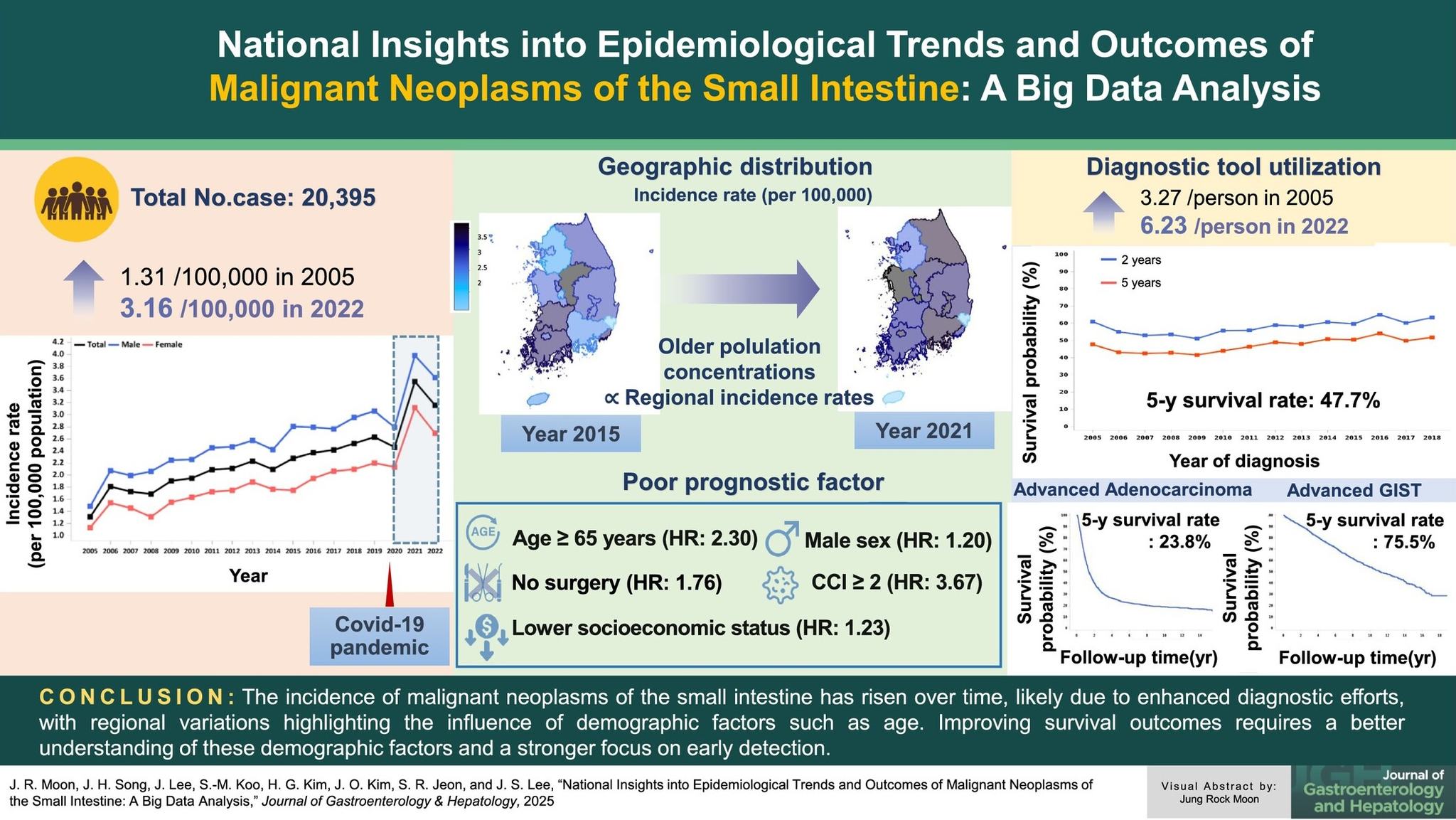
2025년 우리나라 big data 연구가 발표되었습니다.
![]() 2. 첫 상부위장관 내시경 검사에서 진단되지 못한 원발성 악성 십이지장 종양
2. 첫 상부위장관 내시경 검사에서 진단되지 못한 원발성 악성 십이지장 종양
상부위장관 내시경 검사자는 늘 위암을 걱정합니다. 십이지장의 관찰은 상대적으로 소홀한 경우가 있습니다. 2005년 대한소화기내시경학회에서 '첫 상부위장관 내시경 검사에서 진단되지 못한 원발성 악성 십이지장 종양'을 발표하면서 이 문제를 다룬 바 있습니다. 사실 소홀했다기보다는 내시경으로 도달하기 어려운 부위의 병소가 많았다고 하는 편이 옳을 수 있습니다만...
![]() 3. 상부위장관 내시경으로 도달할 수 있는 부위의 십이지장암
3. 상부위장관 내시경으로 도달할 수 있는 부위의 십이지장암
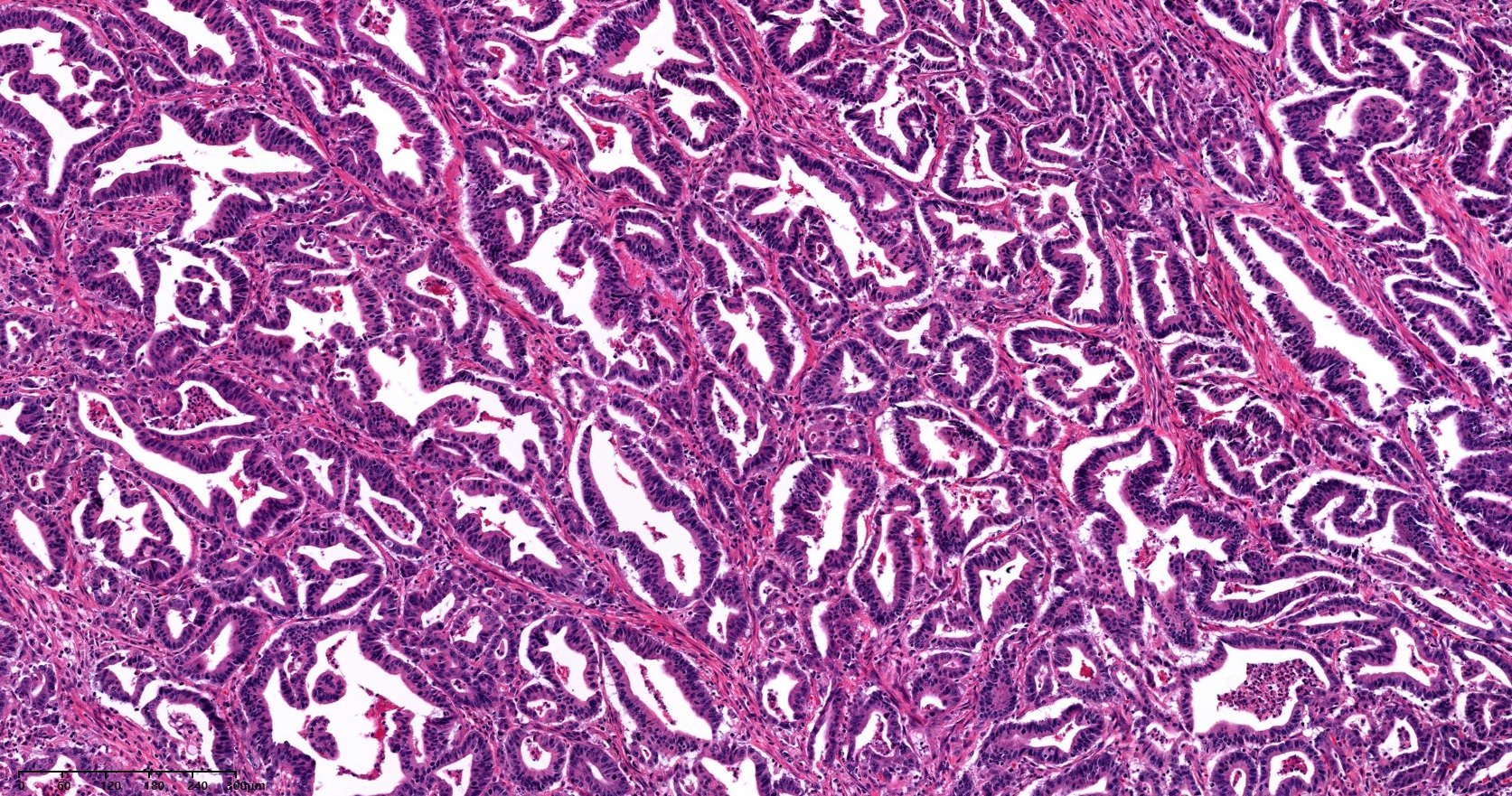
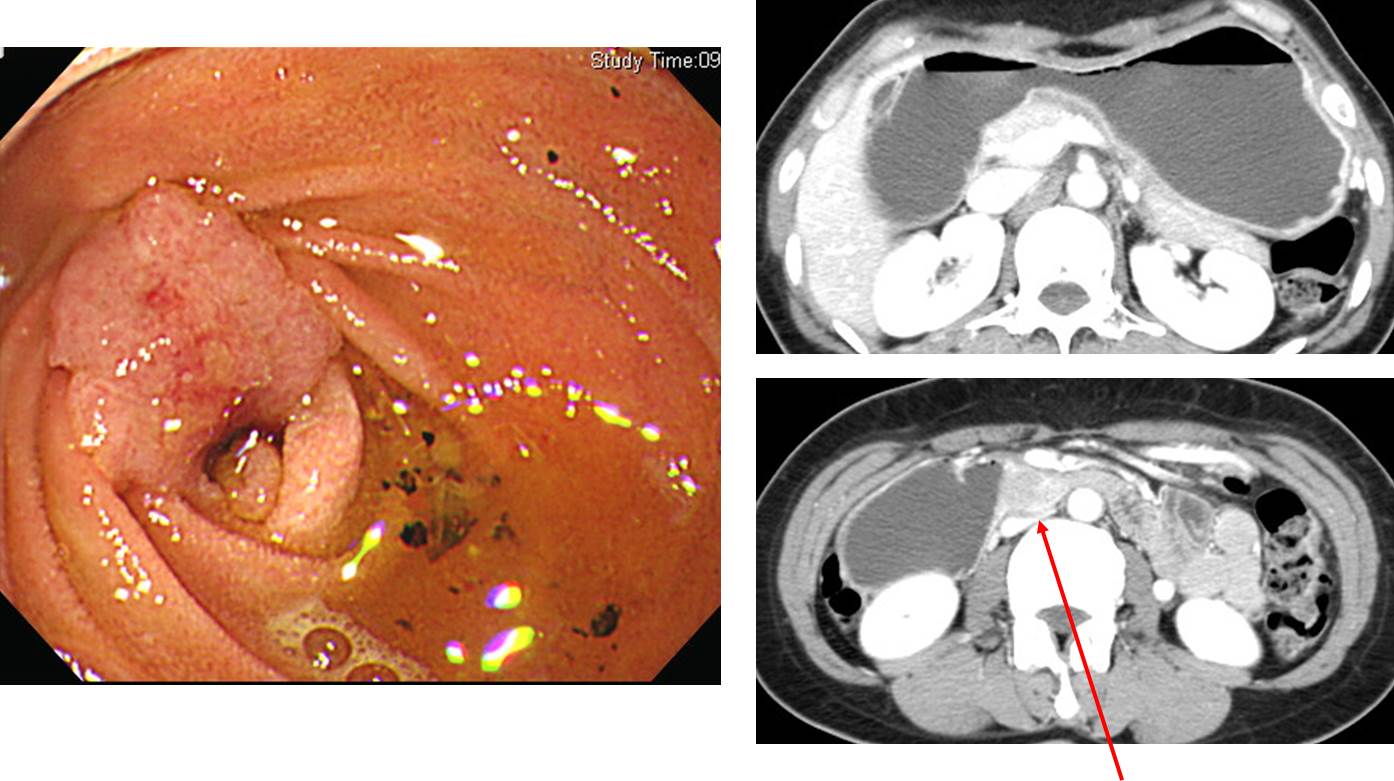
검진내시경에서 우연히 발견된 십이지장 병소입니다. 진단이 무엇이겠습니까?
조직검사는 moderately differentiated adenocarcinoma로 나왔습니다. PPPD 수술을 하였습니다.
PERIAMPULLARY DUODENAL CANCER
1. Type of specimen : PPPD
2. Histopathologic Diagnosis : Adenocarcinoma, moderately differentiated
(1) Tumor site : periampullary
(2) Tumor size : 1.2x1.1 cm
(3) T1a : Tumor invades lamina propria
(4) Involvement of pancreas and duodenal muscle layer : absent
(5) N0 : No regional lymph node metastasis (0/20: "LN6", 0/1; "LN8", 0/1; "LN7,9", 0/3; "LN12", 0/8; periduodenal, 0/7)
(6) M0 : No distant metastasis
(7) Negative (pancreas, common bile duct, retropancreatic) resection margins
(8) Autolysis, gallbladder
(9) Focal pancreatitis (frozen-1), not neuroendocrine tumor
R0 : complete resection with grossly and microscopically negative resection margins추적내시경 검사에서 재발 소견이 없었습니다.
PPPD나 Whipple 수술 후 내시경에서 anatomy를 잘 알기 어려운 경우가 많은데 이 환자에서는 duodenal bulb의 일부가 명확히 잘 관찰되었습니다.
[2023-5-30 EndoTODAY Quiz]
M/58 (2022)
T3N0M0 (T3: tumor invaded through muscularis propria into subserosa, or extends into mesentery or retroperitoneum without serosal penetration)
2.4x1.5cm. adenocarcinoma, well differentiated arising from adenoma, high grade. Confined to the mucosa
초고령으로 수술을 못하시고 1년 조금 넘어 obstruction 증상 발생
Partial resection으로 치료하였고 점막에 국한된 0.6cm 암이었습니다. 최근 같아서는 내시경 절제술로 치료할 수 있다고 생각됩니다.
M/D adenocarcinoma, 3.5 x 3 cm, extension to subserosa, metastasis to 3 out of 10 regional lymph nodes
Duodenal cancer (M/D adenocarcinoma, 4 x 2 cm, extension to periduodenal soft tissue and pancreas, LN 1/34) + stomach cancer
Poorly differentiated adenocarcinoma, proper muscle invasion (F/62, 2019)
Obstruction (+), hepatic metastasis (+)
Poorly differentiated carcinoma
Mucinous adenocarcinoma, 5 x 5 x 3 cm, directly invades other organs (pancreas), involvement of vessel (SMA and SMV: op. record without histologic evaluation), regional lymph node metastasis (13/16)
O & C due to SMA, pancrease, stomach metastasis
Bowel habit change로 대장내시경에서 우측 대장암이 발견되었고 우연히 시행한 위내시경에서 duodenal adenocarcinoma도 함께 진단되었음. Whipple 수술과 right hemicolectomy를 동시에 시행하였음.
Duodenal papillary adenocarcinoma
Duodenal signet ring cell carcinoma
Depressed type FAP-associated early duodenal carcinoma
F65 (2015). 첫 조직검사에서 암으로 나오지 않았던 증례
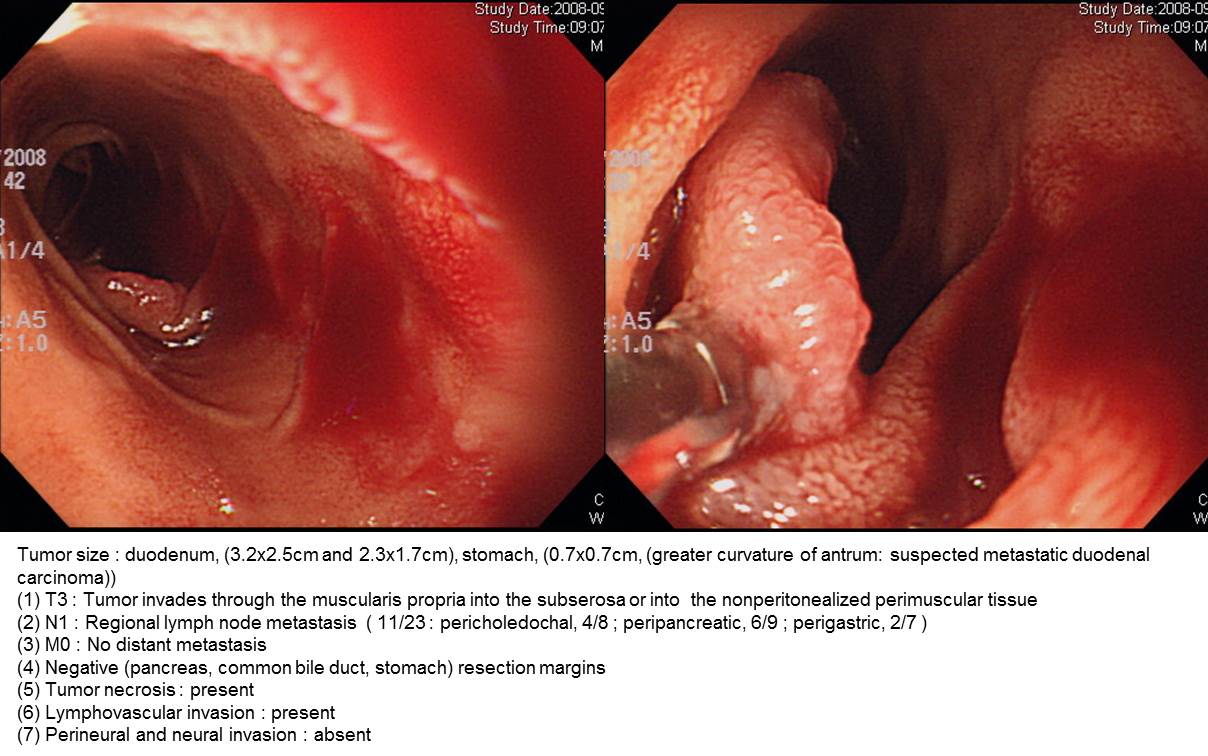
외부 내시경에서 "duodenal 3rd part ulcer and stricture (biopsy: atypical glands)" 소견으로 의뢰된 분으로 내시경 재검에서 M/D adenocarcinoma로 수술한 증례입니다. 내시경 소견과 수술 병리를 소개합니다.
내시경 소견: Duodenal 2nd to 3rd portion부위에 lumen을 encircling하는 mass 관찰되었으며 소아용 대장 내시경을 이용하여 진입 시도하였으나 mass의 위치가 angulation 직후이고 lumen이 좁아져있어 scope이 통과되지 못했습니다. 위내시경으로 바꾸어 try했으나 최대한 삽입해도 mass의 입구까지 밖에 도달하지 못하여, 다시 소아용 대장내시경에 cap을 장착후 try했으나 역시 진입불가능하여 최대한 forcep을 밀어넣어 조직검사를 시행했습니다.
DUODENAL CANCER
1. Type of specimen : PPPD
2. Histopathologic Diagnosis : Adenocarcinoma, moderately differentiated
(1) Tumor site : duodenal
(2) Tumor size : 4.5x4 cm
(3) T3 : Tumor invades through the muscularis propria into the subserosa
(4) Involvement of pancreas: absent
(5) N1 : Regional lymph node metastasis (2/16: "peri-SMA tissue" for frozen section-1, 0/1; "LN8,12", 0/6; "periCBD&peripancreatic LN", 1/3; periduodenal, 1/2; peripancreatic, 0/4)
(6) M0 : No distant metastasis
(7) Negative (pancreas, common bile duct, retropancreatic) resection margins
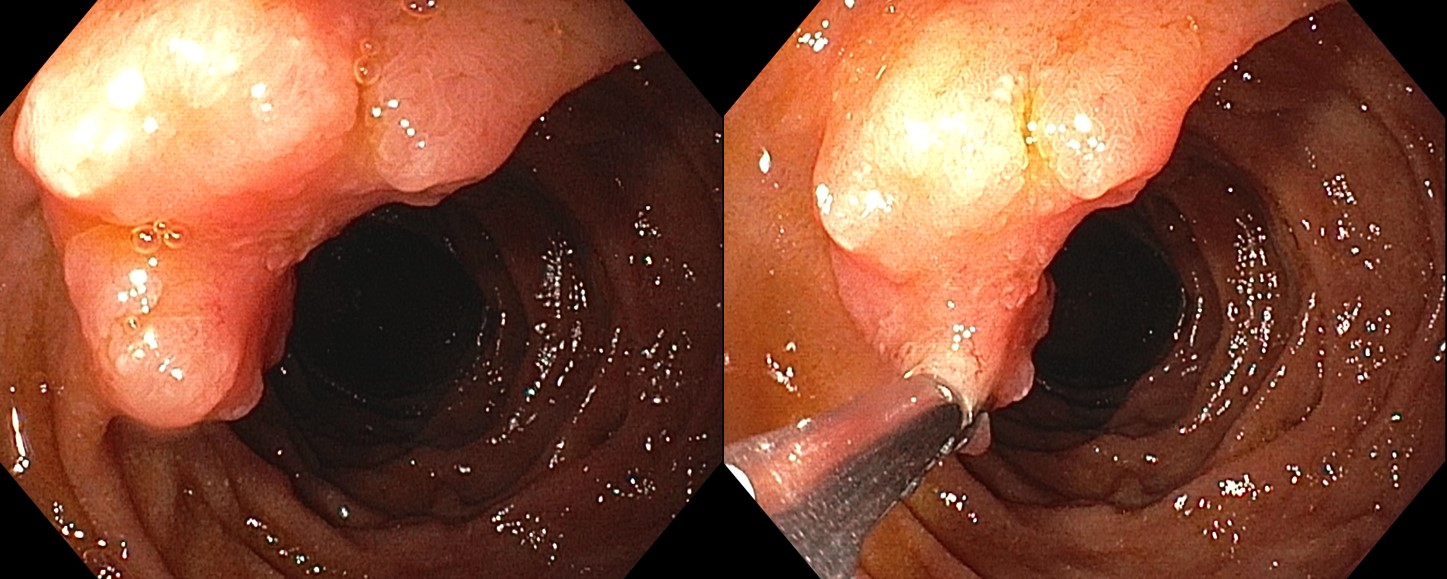
조직검사에서 십이지장 선종으로 의뢰되었습니다. EMR을 하였는데 의외로 암이 나왔다고 합니다. 암은 1 mm도 안 되고 대부분 선종이라고 하니 다행입니다.
EMR for duodenal adenoma was done.
Duodenum, endoscopic submucosal dissection:
Adenocarcinoma, well differentiated (focal: < 10 %) arising from mainly adenoma (90 %)
1. Location : duodenum second portion
2. Size of carcinoma : < 1 mm
3. Size of adenoma : (1) longest diameter, 7 mm (2) vertical diameter, 4 mm
4. Depth of invasion : invades mucosa (lamina propria) (pT1a)
5. Resection margin : free from carcinoma(N)
6. Lymphatic invasion : not identified(N)
7. Venous invasion : not identified(N)
PERIAMPULLARY DUODENAL CANCER
1. Type of specimen : Whipple resection
2. Histopathologic Diagnosis : Mucinous adenocarcinoma (mucin production: 60%)
(1) Tumor site : duodenal
(2) Tumor size : 2x1 cm
(3) T2 : Tumor invades duodenal wall (muscularis propria)
(4) Involvement of pancreas : absent
(5) N1 : Regional lymph node metastasis (1/19 : "L/N", 0/13; LYMPH NODE, 1/6)
(6) M0 : No distant metastasis
(7) Negative (pancreas, common bile duct, retropancreatic) resection margins
DUODENAL CANCER
1. Type of specimen : Whipple resection
2. Histopathologic Diagnosis : Adenocarcinoma, moderately differentiated
(1) Tumor site : duodenum
(2) Tumor size : 2.5x2.3 cm
(3) T3 : Tumor invades through muscularis propria into subserosa
(4) N0 : No regional lymph node metastasis (0/49) : "LN 7,9", 0/6; "LN8", 0/13; "LN12", 0/12; "LN14", 0/2; "LN16", 0/7; peripancreatic, 0/9)
(5) M0 : No distant metastasis
(6) Negative intestinal, radial resection margins
(7) peritumoral inflammatory reaction: mild
R0 : complete resection with grossly and microscopically negative resection margins
AJCC Stage (8th Edition, 2018)
Stage IIA: T3 N0 M0
유방암 간전이와 거의 동시에 발견된 원발성 십이지장암 (증상: 토혈)
[십이지장 궤양으로 의뢰된 십이지장암] - 소장질환 029
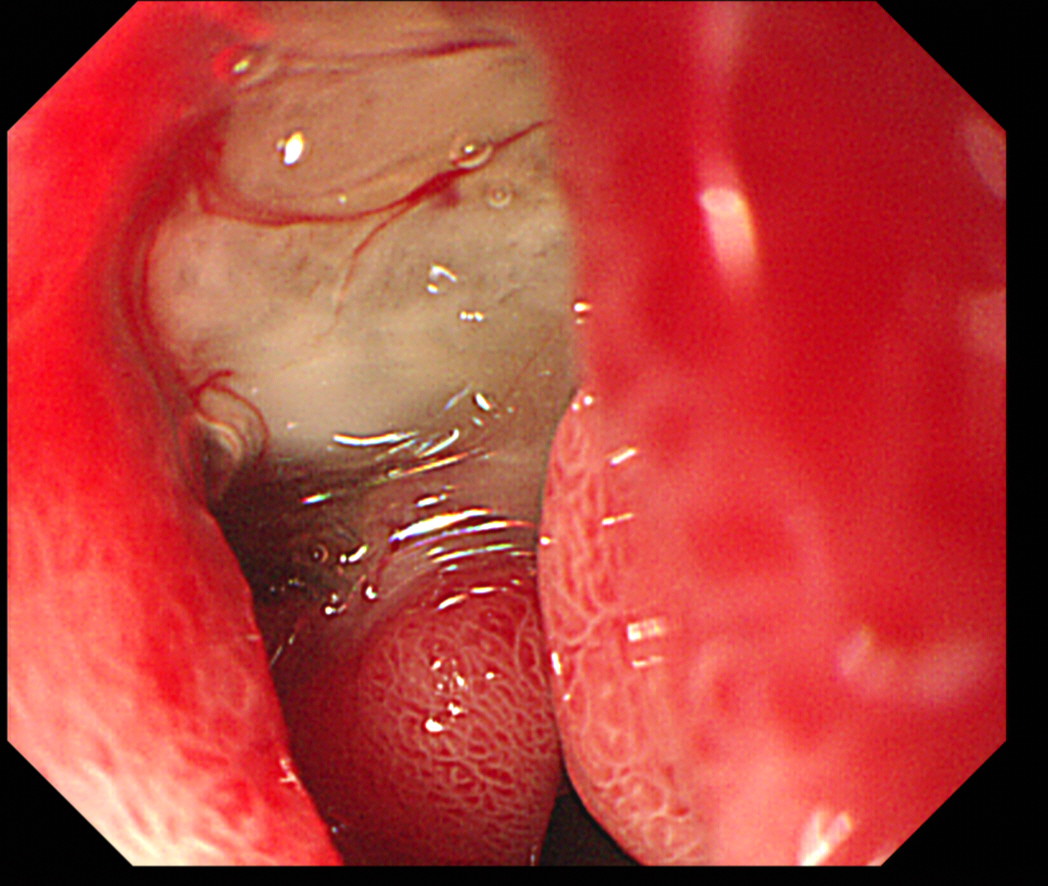
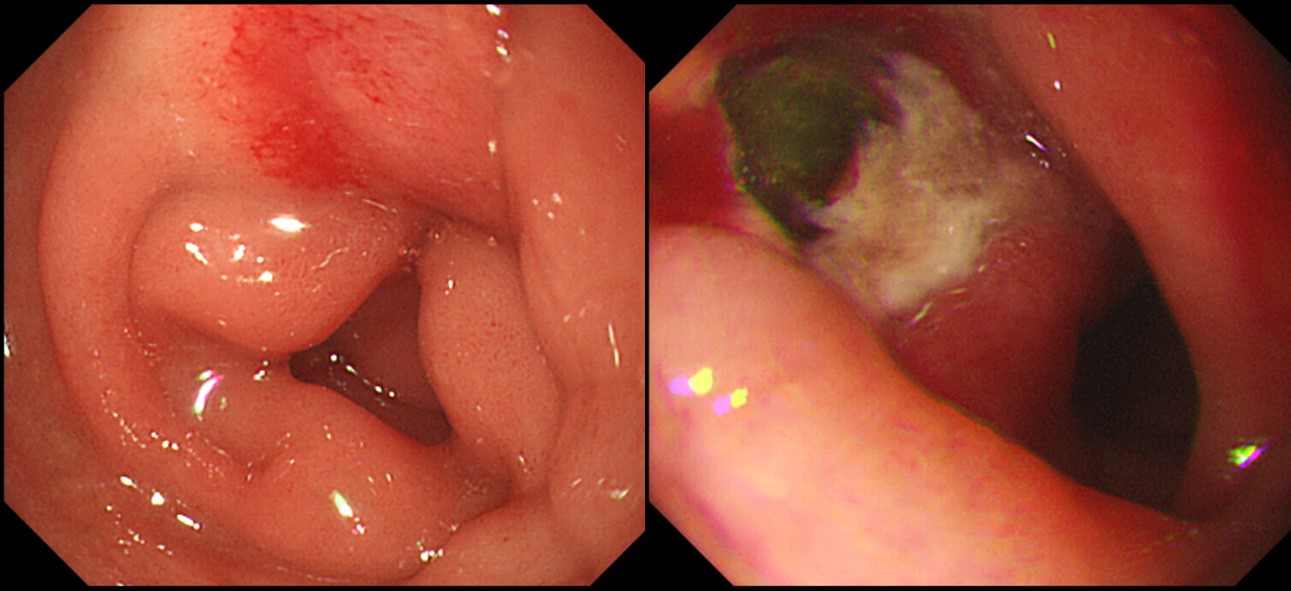
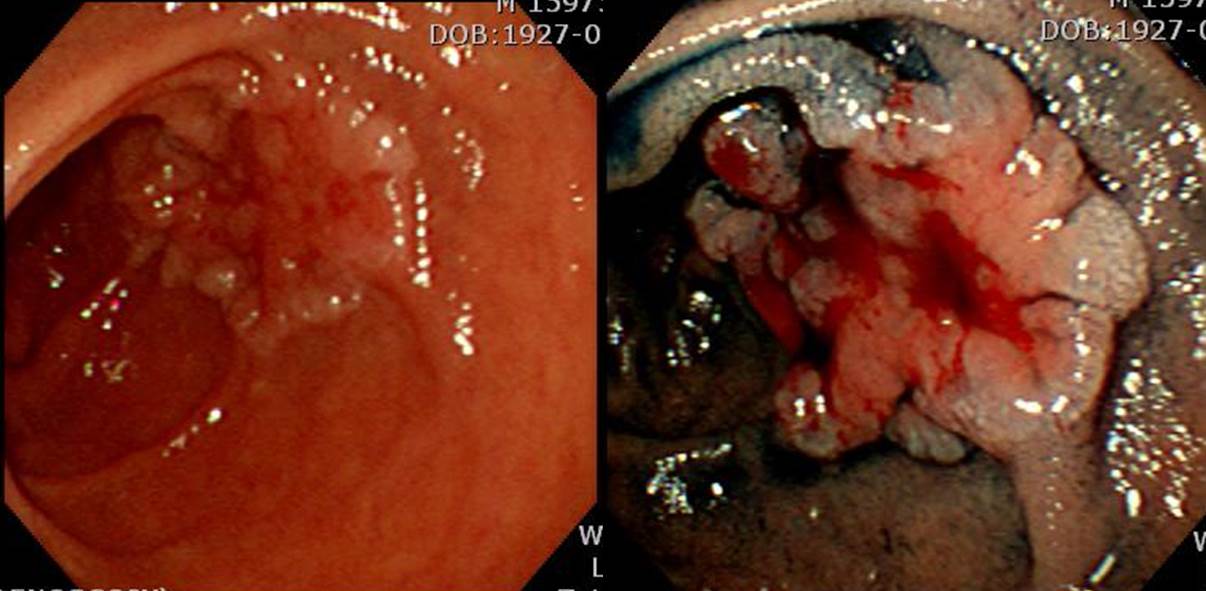
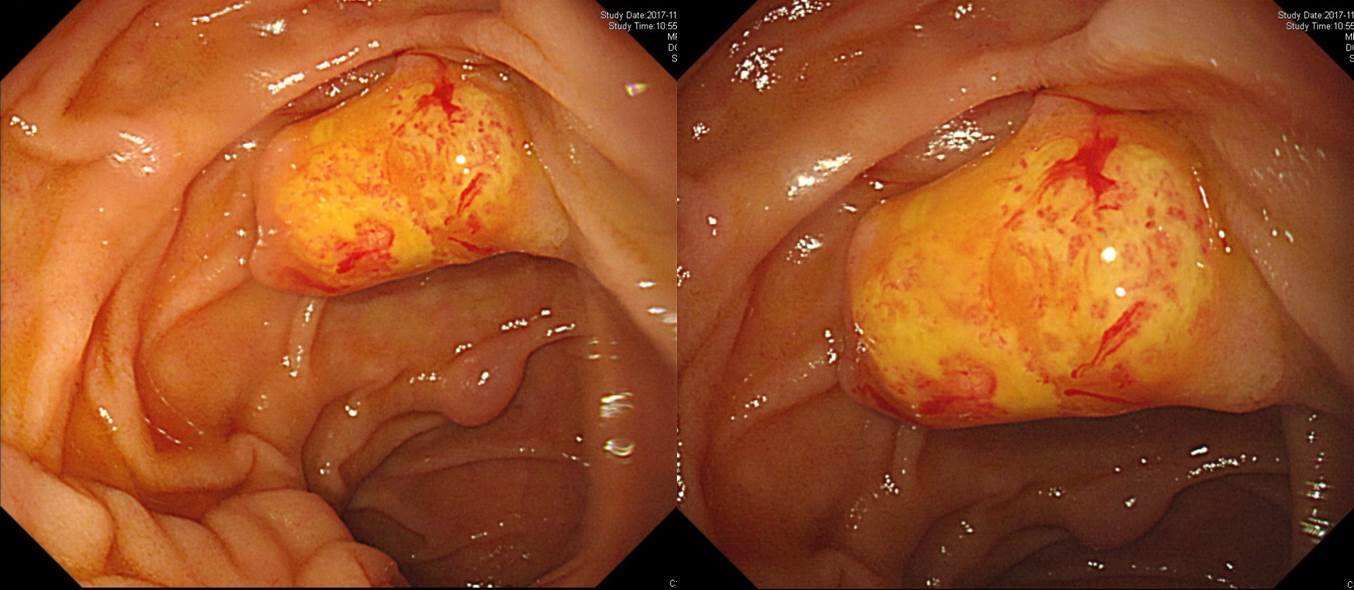
55 years old woman visited the health screening center due to abdominal pain for a few weeks. A duodenal lesion was found and referred. What is your impression?
Immediately after referral, endoscopic examination was done.
The pathology was adenocarcinoma (M/D). However, there were multiple hepatic metastatis.
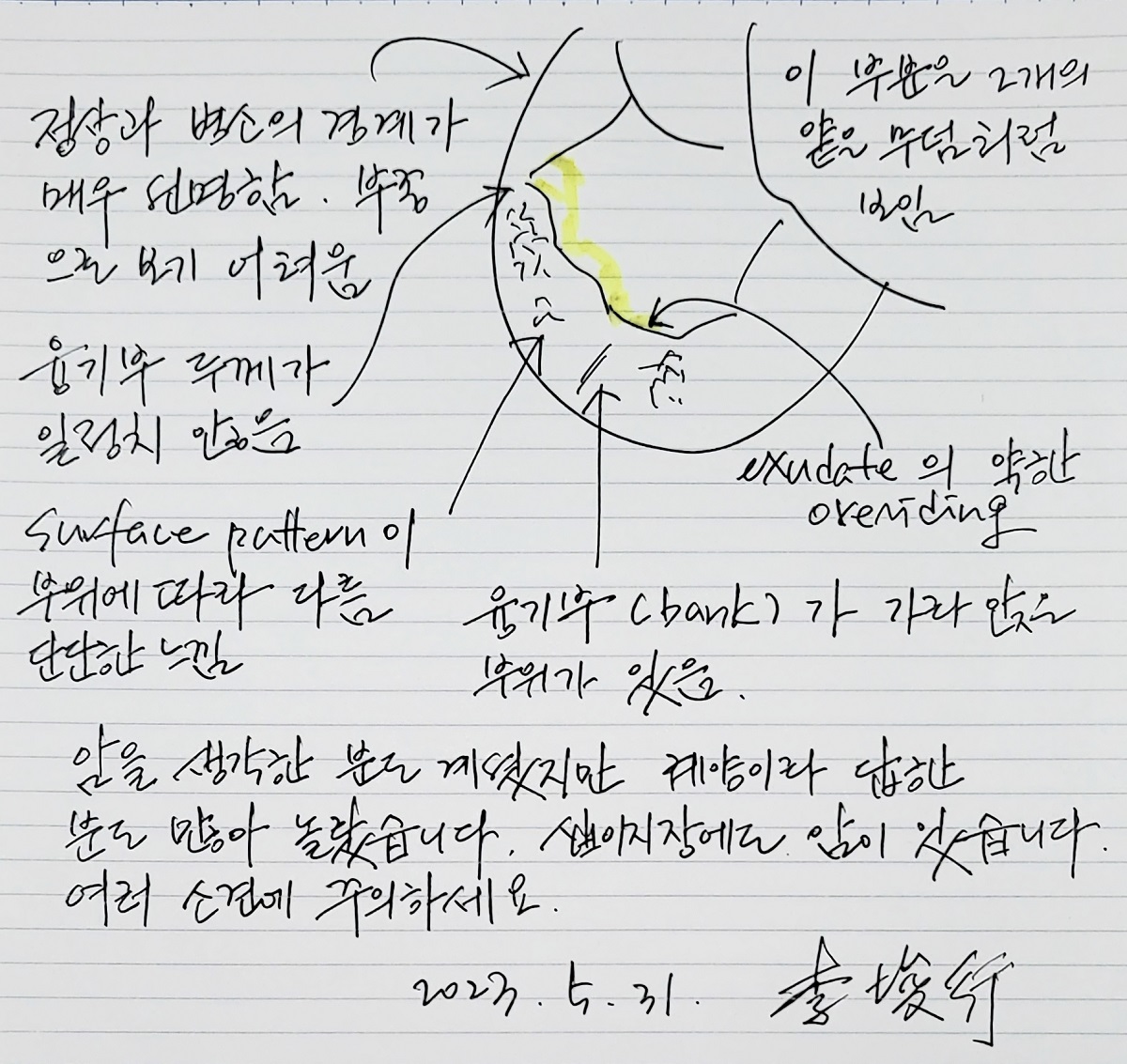
When I review the initial endoscopy and second endoscopic images, it looks like an acute benign duodenal ulcer with severe edematous change. Is there a clue suggessting cancer? It is very difficult. Compared the small ulcer crator, the mucosal edema is too severe. Benign ulcer symptoms usually disappear very quickly with medication. Considering the prominent edema and persistent symptom after medication may be important for the correct diagnosis. Biopsies are necessary for initial severe duodenal ulcer to rule out malignancy.
![]() 4. 상부위장관 내시경으로 도달할 수 없는 부위의 십이지장암
4. 상부위장관 내시경으로 도달할 수 없는 부위의 십이지장암
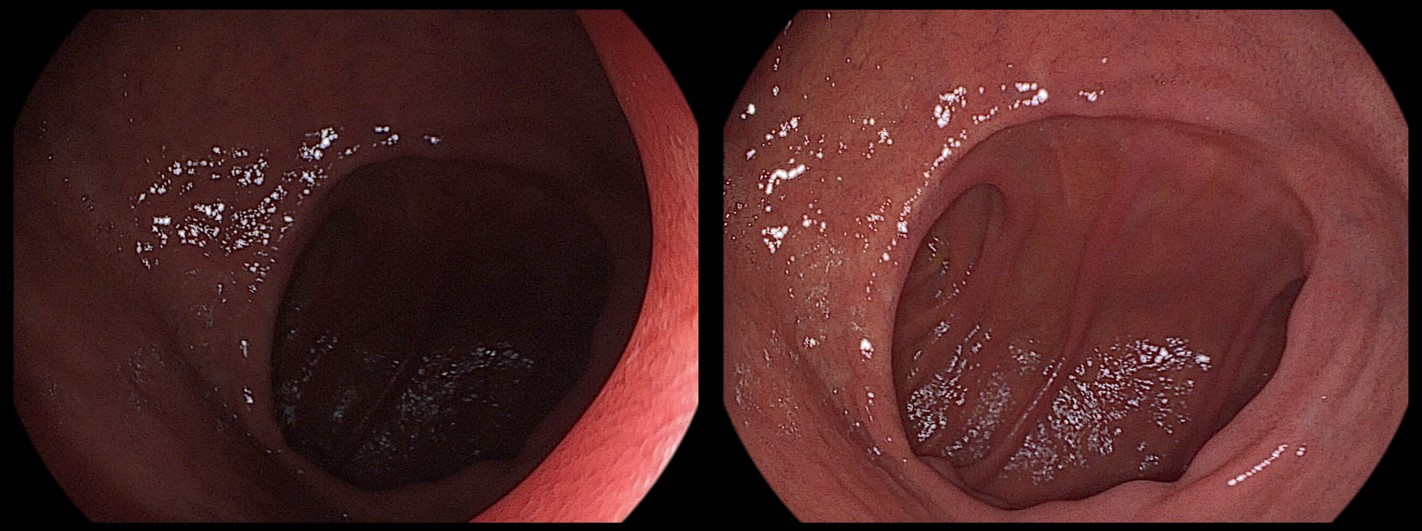
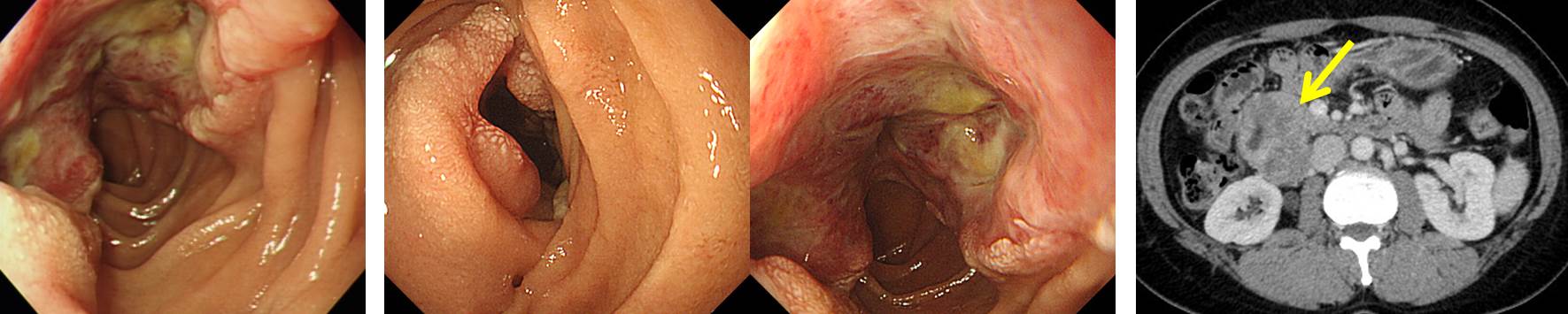
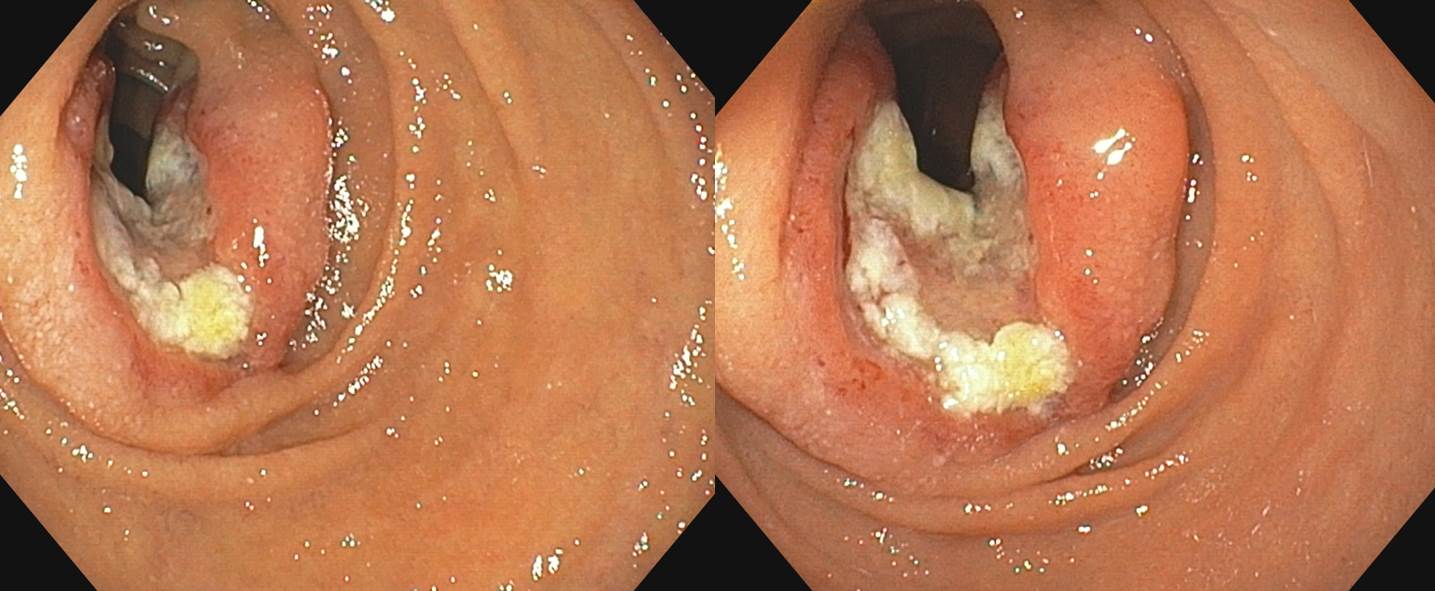
한달 전 시작된 복통, 구토 및 10 kg 정도의 체중감소로 상하부 내시경과 복부 CT 검사를 하였으나 원인이 명확하지 않아 의뢰된 환자입니다. CT를 검토하였고 left paraaortic area에 1 cm으로 커진 lymph node가 관찰되며 그 밖에도 여러 개의 작은 lymph node들이 left paraaortic area에서 관찰되고 있어 metastatic lymphadenopathy의 가능성을 배제하기 어렵다는 의견을 받았습니다. 이의 확인을 위하여 PET CT를 시행하였으며 "Left paraaortic area에 장경 4.2 cm인 hypermetabolic mass가 관찰되며 그 FDG 섭취가 증가(p-SUV = 13.3)됨. 양상으로 보아 malignancy의 소견으로 생각된다"는 판독을 받았습니다. PET CT에서 hypermetabolic mass의 내부에 air가 관찰되는 양상이어서 GI tract의 병소(즉 십이지장 제 3부, 4부 혹은 그 이하의 암)일 가능성을 생각하였습니다. EGD로는 들어갈 수 없는 부위였기 때문에 push enteroscopy 목적으로 colonoscope를 이용한 내시경을 시행하였습니다 (시행의: 임상강사 선생님). 십이지장 제 2부에서 lumen이 구부러져 제 3부로 진입하는 부위로부터 약 10 cm 하방에서 lumen을 좁히고 있는 blood oozing을 동반한 암이 발견되었습니다. 위치는 십이지장 제 4부로 판단되었고 조직검사에서는 adenocarcinoma가 나왔습니다. 수술을 권하였습니다. 오늘의 증례처럼 일반적인 상부위장관 내시경 검사 범위(식도부터 십이지장 제 2부)를 벗어나는 십이지장 제 3부나 제 4부의 암의 진단은 간단한 일이 아닙니다. High index of suspicion이 중요하다고 할 수 밖에 없습니다. 모두들 긴장합시다. [바른 내시경 이준행 @ endoedu.com; 2009. 7. 3.]
Adenocarcinoma (M/D), 9x9x4cm, L (+), LN (+) 6/9 Involvment pancreas, colon and mesentary
3달 전에 위내시경 받았던 증례
Peritoneal seeding, MUO (metastasis of unknown origin) workup으로 시행한 두번째 위내시경입니다 (첫 내시경은 의뢰 전 병원). 일반 위내시경에서 십이지장 제3부에 작은 mass가 의심되어 내시경 변경 후 cap을 장착하고 최대한 push하여 병변을 관찰하였다고 합니다. Fellow 황금빛 선생님. 참 잘하셨습니다. 칭찬하는 의미로 황선생님이 기술하신 내시경 결과지를 그대로 옮깁니다.
![]() [FAQs]
[FAQs]
[2024-5-2. 애독자 편지]
안녕하세요! 건양대병원 췌담도파트에서 일하고 있는 류기현이라고 합니다. 제가 요즘은 상부위장관내시경을 자주 하고 있지는 않지만 14년전 내시경을 한참 배우던 전임의 때 경험한 흥미로웠던 케이스 3개를 모아서 지난해 출판을 했습니다 (World J Clin Cases 2023).
내용을요약하면, "표준상부위장관내시경으로도 많은 퍼센트에서 근위 공장에 도달할 수 있다."입니다. 본 문헌에서는 내시경으로 근위공장의 GIST 를 확인하고 수술을 통해 위치를 증명한 3개의 케이스를 보고 했습니다.
실제 표준 상부위장관내시경을 십이지장유두부 이후부로 내시경을 더 밀어 넣고 대장내시경처럼 축유지/단축을 활용하면 공장에 도달하는 것을 자주 경험합니다. 이는 저처럼 투시장비가 있는 공간에서 시행을 하다보면 확인이 가능합니다. 소장내시경검사 시행 전 근위 공장내 종괴의 확인이나 조직검사에도 활용할 수 있지만 obscure GI bleeding 에 대한 2nd look endoscopy 시에도 많은 도움이 되리라 생각 됩니다.
[2024-5-2. 이준행 답변]
좋은 증례를 소개해 주셔서 감사합니다. 상부위장관내시경으로도 단축을 잘 하면 상당히 깊게, jejunum의 일부까지도 들어갈 수 있다는 것을 멋진 증례로 보여주셨습니다.
![]() [References]
[References]
1) SmallTODAY - 소장질환 증례토의
2) 십이지장 구부 위치표시
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.