EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Familial adenomatous polyposis (FAP) 가족성 선종성 용종증] - 終
[Familial adenomatous polyposis (FAP) 가족성 선종성 용종증] - 終


PDF 14M
2026-7-5. PDF (20 페이지 요약)
1. Introductory case - 위내시경 소견으로 FAP를 의심하였던 환자
3. Genetics
5. Ampullary adenoma 유두부 선종
6. Overview of the upper GI tract lesions 상부위장관 질환
7. Non-ampullary duodenal adenoma 비유두부 십이지장 선종
8. Fundic gland polyposis 위저선 용종증
9. Gastric adenoma 위선종
10. Gastric cancer 위암
11. Extracolonic manifestations and related conditions - 갑상선암 때문에 FAP를 발견 (cribriform-morular variant)
12. Screening policy
14. FAP 환자가 total colectomy를 거부한다면?
15. FAQ
16. References
![]() 1. Introductory case
1. Introductory case
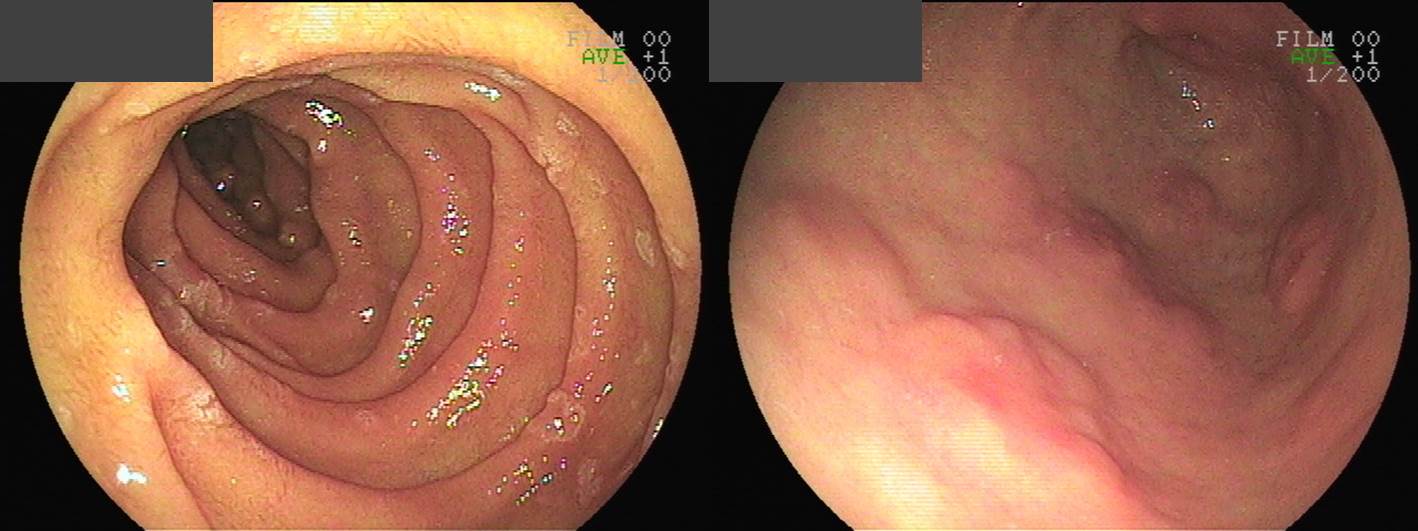
40대 후반 남성입니다. 우연히 시행한 상부내시경에서 다발성 위 선종과 십이지장 선종이 발견되어 의뢰되었습니다.
FAP 가능성 고려하여 대장내시경을 시행하였습니다. 위 선종과 십이지장 선종은 내시경치료를 하였습니다.
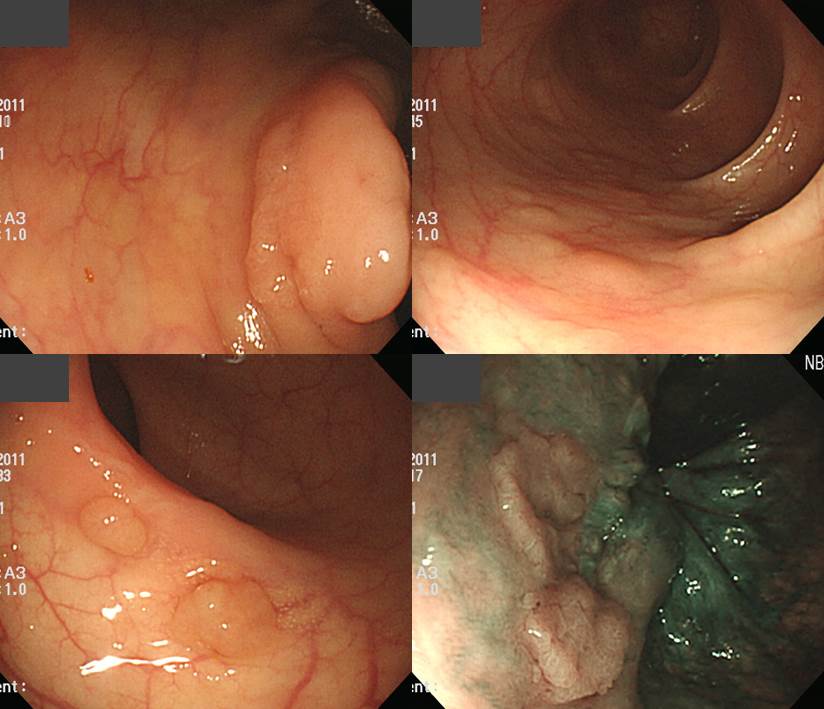
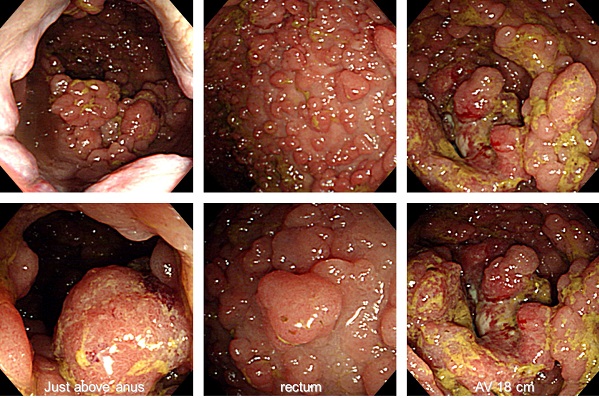
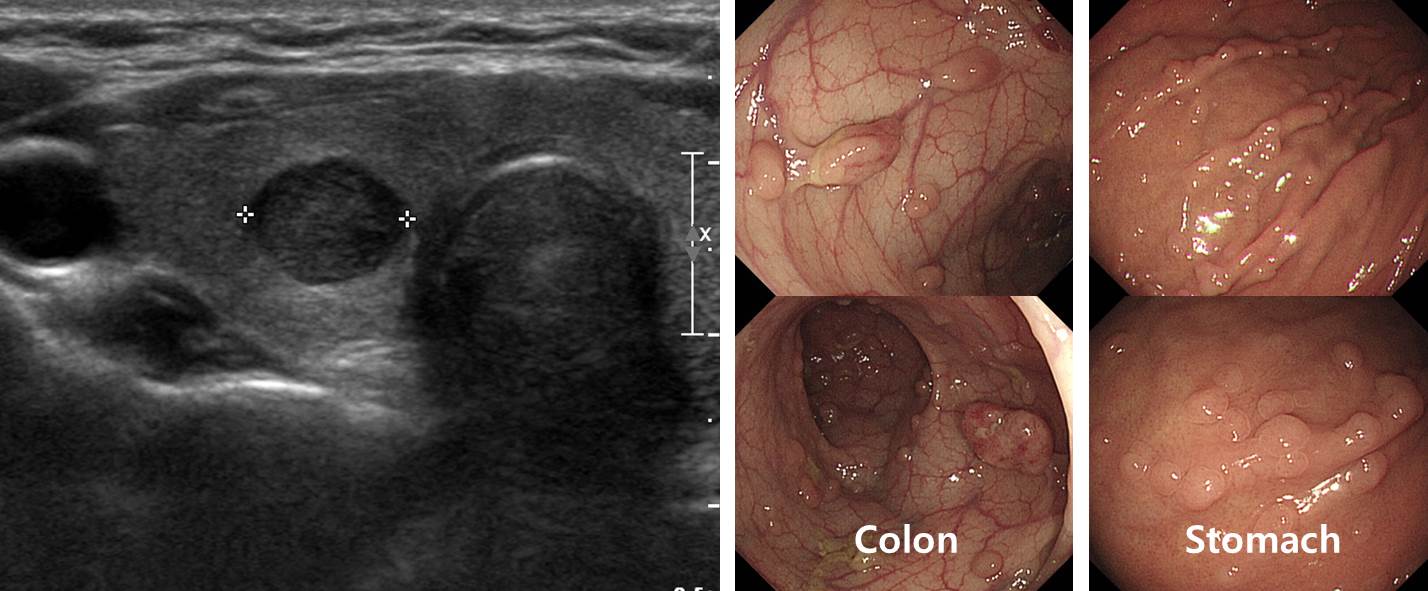
- 소견: Cecum과 IC valve에 수개의 용종이 있었음. 상행결장부터 하행결장까지는 비교적 정상 점막 의 소견을 보임. AV 20cm부터 투명한 병변이 수십개 관찰되었으며(NBI에서는 도드라져 보임 ), AV 10cm이하로는 수십개의 용종이 관찰되었음.
- 내시경 진단: r/o attenuated FAP
- 참고: AV 20cm 위쪽으로는 눈에 보이는 용종은 모두 제거 하였습니다. AV 20cm 이하부위는 병변의 갯수가 너무 많아 제거가 불가능 하였습니다. Anus 직상방의 LST는 항문의 정맥총과 너무 가까이 있어, 조직검사 확인 후 치료여부를 결정하면 되겠습니다.
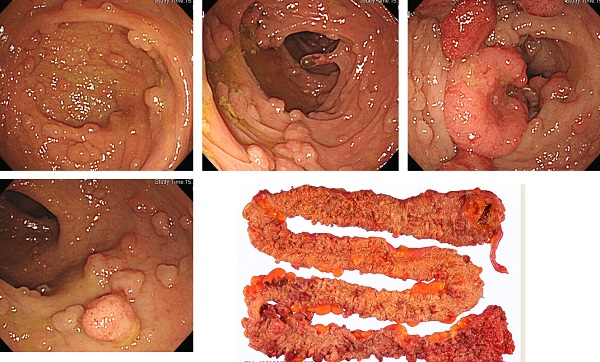
FAP 가능성 고려하여 유전자 검사를 시행하여 germline mutation이 발견되었습니다. 복강경 대장절제술을 시행하였습니다.

- Tubular adenomas, multiple (about 200)
- Traditional serrated adenoma and tubular adenoma in vermiform appendix
- Consistent with familial adenomatous polyposis, probably attenuated form
가족들 유전자 검사를 시행하여 아드님에서도 동일 germline mutation이 발견되어 수술을 권했습니다.
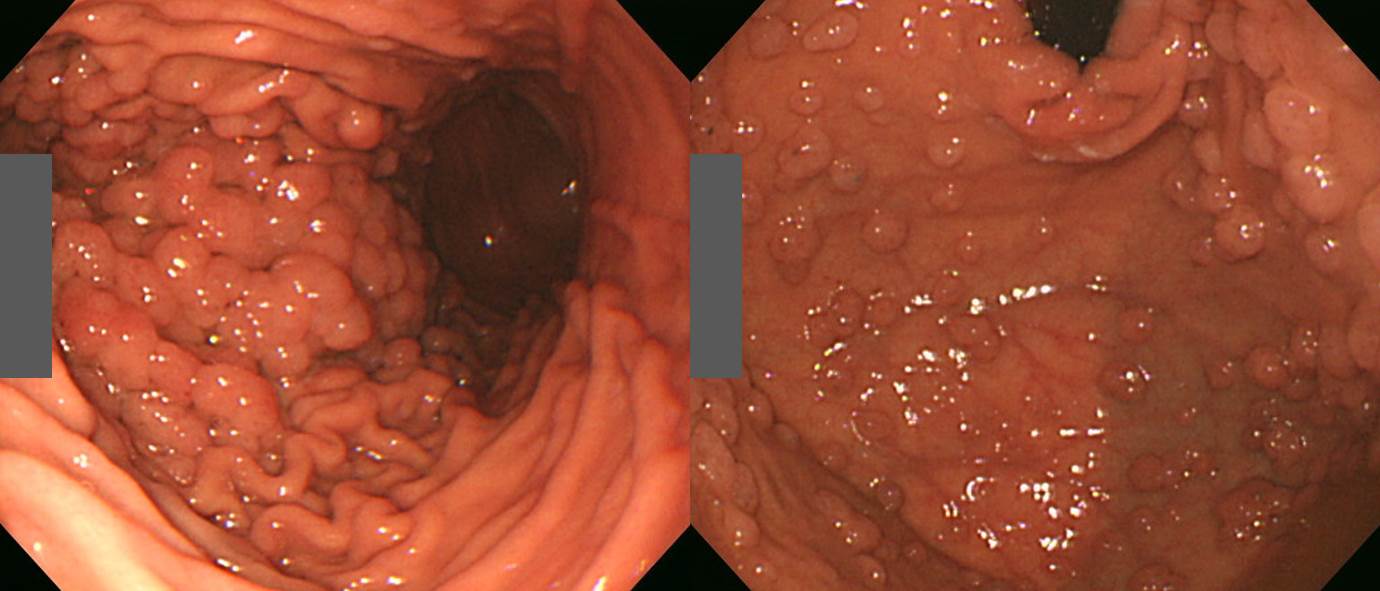
또 다른 환자의 대장내시경과 수술 소견입니다. 용종이 되지 않은 점막에서도 선종성 변화가 있음을 알 수 있습니다.
![]() 2. 가족성 선종성 용종증 (familial adenomatous polyposis, FAP)이란?
2. 가족성 선종성 용종증 (familial adenomatous polyposis, FAP)이란?
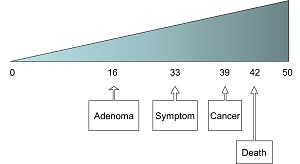
FAP는 전체 대장암의 1% 미만을 차지하고 있으나 유전적 특성이 잘 알려진 매우 중요한 질환입니다. FAP 환자는 대부분 오랜 기간 무증상으로 지내는데, 용종이 많아지고 커지면서 변비, 설사, 복통, 체중감소, 빈혈, 출혈 등이 나타날 수 있습니다. 다발성 용종이 나타난 환자에서 대부분 10-20년 이내에 암이 발생되므로 암을 동반하지 않은 다발성 용종 단계에서 조기에 발견하여 대장 전절제술로 치료하는 것이 최선입니다.
FAP with rectosigmoid cancer
FAP with sigmoid cancer
최근 우리나라에서 과거에 비하여 FAP 환자들이 자주 발견되고 있습니다. 이 환자들에 대한 적극적인 치료로 생존율도 크게 향상되었습니다. 그러나 아직 일반인구보다 기대여명이 낮은 상태인데 이러한 이유 중 하나는 대장 전절제술 후 상부위장관 암 발생률이 높기 때문입니다. FAP 환자의 90%이상에서 상부위장관 선종이 발생하며 상당수가 암으로 진행하는 것 같습니다. FAP 환자에서 대장암 다음으로 흔한 암종이 유두암(ampullary cancer)을 포함한 십이지장암입니다. 서구에서 대장 전절제술을 받은 FAP 환자의 10-15%는 유두암이나 십이지장암으로 사망합니다. 우리나라는 위암의 호발지역으로 FAP 환자에서 위선종이나 위암이 종종 발견되고 있다.
여자 52세 (2023)
위 환자의 위내시경 소견 (2023)
Familial adenomatous polyposis (FAP) syndrome is a complex entity, which includes FAP, attenuated FAP, and MUTYH-associated polyposis. (GIE 2020)
The MUTYH gene is a DNA base excision repair gene that repairs DNA injury from oxidative stress. MAP, first described in 2002, is an autosomal recessive condition associated with an increased risk of CRC development. MUTYH-associated polyposis is an autosomal recessive polyposis syndrome caused by biallelic pathogenic germline variants in the MUTYH gene. MUTYH is a base excision repair gene whose protein repairs oxidative damage to the DNA. Oxidation of guanine leads to the formation of 8-oxo-6, 7, 8-dihydroxy-2 deoxyguanosine. Failure of base excision repair results in mispairing of this nucleotide with adenine and resultant somatic CG?AT transversions in multiple genes, including the APC and KRAS genes. The target genes that are mutated as a consequence of oxidative damage strongly influence the polyposis phenotype. The two most common MUTYH gene pathogenic variants in Western Europeans and North Americans are Y179C and G396D. However, pathogenic variants at different loci have been reported in other populations. Patients with MUTYH-associated polyposis may be homozygous or compound heterozygous for these or other pathogenic variants in the MUTYH gene.
Biallelic MUTYH pathogenic mutations lead to the development of multiple colorectal adenomas, usually <100 in a patient’s lifetime. The colonic polyposis phenotype is similar to AFAP with possible rectal sparing and a right-sided colon predominance. A higher prevalence of serrated adenomas has also been observed in patients with MAP.
Ggenetic testing for mutations in MUTYH should be considered in those with (1) 20 or more colorectal adenomas over multiple colonoscopies, (2) a known family history of MAP, (3) 10 or more adenomas found on a single colonoscopy, or (4) criteria for serrated polyposis syndrome with at least some adenomas noted on examination.
FAP는 유전성 질환입니다. 대장에서는 melanosis와 sessile polyp 들이 있고, 위에서는 단 몇개의 polyp들이 있었던 환자인데 FAP의 가족력을 고려하면 FAP임을 짐작할 수 있어야 합니다.
35세 남성
![]() 3. Genetics of FAP
3. Genetics of FAP
1) Germline mutations of the APC gene on chr 5q21
2) APC gene : tumor suppressor or “gatekeeping” gene
3) 15 exons, 2843 amino acid, 309K daltons
4) Important in cell adhesion, signal transduction, and transcriptional activation
5) Downstream targets : Beta-catenin and c-myc
6) More than 300 different mutations
7) Most are insertions, deletions, and nonsense mutations that lead to frame shifts or premature stop codons, resulting in truncation of the APC gene product
8) The most common mutation is a deletion of AAAAG in codon 1309
APC 유전자의 구조
APC 유전자의 기능
APC 유전자의 구조
Genotype-phenotype correlation
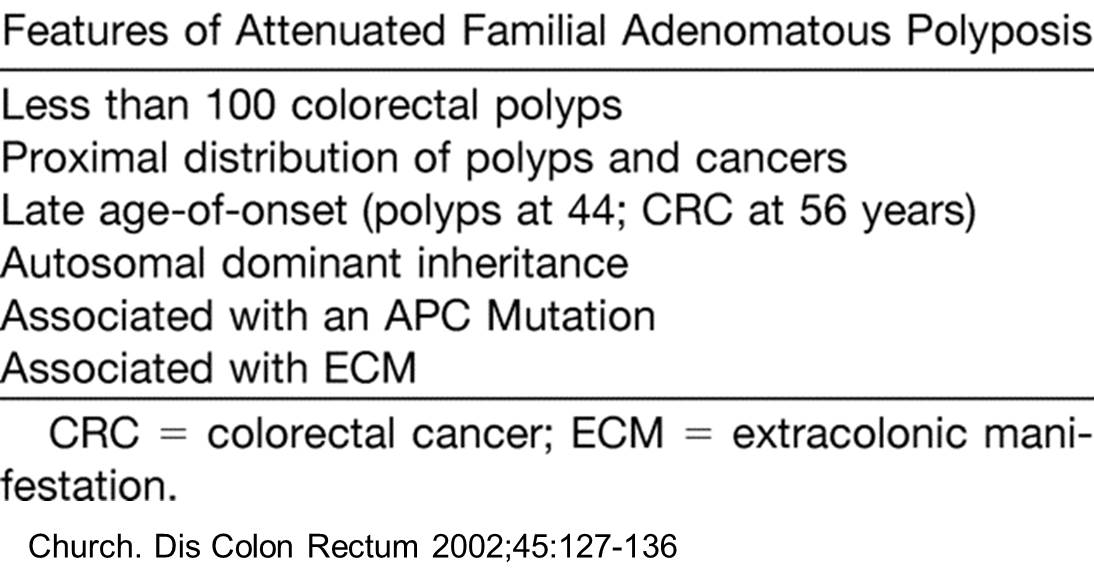
![]() 4. Attenuated FAP
4. Attenuated FAP
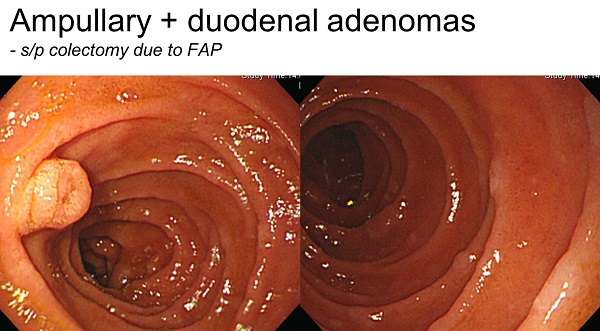
![]() 5. 유두부 선종. Ampullary adenoma
5. 유두부 선종. Ampullary adenoma
유두선종은 FAP 환자에서 종종 발생하며 암으로의 발생위험을 가지고 있으며, FAP 환자의 주요 사망 원인입니다. 일반인구에 비하여 유두암 발생률이 200~300배 높습니다. 일생 동안 암발생위험이 5~12%이므로, 일단 발견되면 내시경 유두절제술을 시행합니다.
![]() 6. Upper GI tract lesions. 상부위장관 질환
6. Upper GI tract lesions. 상부위장관 질환
2011년 서울대병원에서 148명의 FAP 환자의 위내시경에서 위선종이 14.2%, 십이지장 선종이 15.5%라고 발표한 바 있습니다. (Gut Liver 2011). 2019년 내시경학회에서 아산병원과 이대병원 팀이 아래와 같은 훌륭한 초록을 발표하였습니다. 진료에 크게 도움될 것 같습니다. 치료하지 않고 경과관찰하는 위선종과 십이지장 선종이 아주 많다는 것을 알 수 있습니다.
Upper gastrointestinal neoplasm in Familial Adenomatous Polyposis: a single-center, retrospective study
Introduction: Although the upper gastrointestinal (GI) neoplasms are not rare in patients with familial adenomatous polyposis (FAP), only few studies have focused on the upper GI lesions, especially in Asians. Therefore, we tried to investigate the frequency and clinical outcomes of upper GI tumor in FAP patients. Patients and Methods: Among the patients who were diagnosed as FAP between December 2005 and December 2017, those who underwent esophagoagastroduodenoscopy (EGD) were eligible. The clinical features and treatment outcomes of upper GI neoplasms were retrospectively investigated and analyzed. Results: Among a total of 230 patients with FAP, 218 patients underwent EGD and the upper GI neoplasms were detected in 168 (77.1%) patients as follows: fundic gland polyp in 132 patients (78.6%), gastric adenoma in 37 (22.0%), gastric cancer in 8 (4.8%), and duodenal adenoma in 134 (79.8%). The patients with gastric cancer performed endoscopic submucosal dissection (ESD) in 62.5% and gastrectomy in 37.5%. In 1 patients, EGC was recurred 71 months after ESD and received additional ESD. Gastric adenoma was treated by ESD in 32.4%, endoscopic mucosal resection (EMR) in 13.5%, argon plasma coagulation (APC) in 8.1%, band ligation in 2.7%, and no treatment in 43.2%. In duodenal adenoma, EMR was done in 32.1%, APC in 17.9%, polypectomy in 0.7%, band ligation in 0.7%, and no treatment in 48.5%. There were no patients who underwent surgery for gastric adenoma and duodenal adenoma. Conclusion: On the basis of these results, endoscopic surveillance in FAP patients is important for the early detection of neoplasm and avoiding invasive surgery.
[경과관찰 중인 증례]
대장수술 후 위고도선종으로 EMR을 받으신 분인데 추적검사에서 다발성 flat adenoma가 위와 십이지장에서 발견되었음. 환자와 상의하였고 1년 후 추적내시경 예약함 (2018. 남62세)
[American Society for Gastrointestinal Endoscopy guideline on the role of endoscopy in familial adenomatous polyposis syndromes (GIE 2020)]
Recommendations (stomach). The optimal strategies for surveillance and endoscopic management of patients with FAP (including AFAP and MAP) are unknown, with various recommendations issued by polyposis registries around the world. During screening and surveillance endoscopy, we recommend careful evaluation of polyps including FGPs with random biopsy sampling and complete resection of polyps >1 cm for the evaluation of indolent dysplasia and malignant transformation, particularly in the setting of diffuse gastric polyposis and large gastric mounds. All antral polyps should be endoscopically removed, given the high probability of adenoma. Surgery should be reserved for patients with FGP and adenomas harboring advanced histologic features who fail endoscopic management.
이준행 註 (2020-5-9): 위내시경을 자주 시행하는 우리나라에서는 ASGE guideline 2020에서 언급한 바와 같이 random biopsy를 시행하거나 1cm 이상의 fundic gland polyp을 모두 제거하는 것은 불필요할 것 같습니다. Antral polyp도 선종일 수 있어서 모두 제거하라는 것도 비현실적입니다. 잘 관찰하여 의심되는 것만 검사하고 확인된 것만 제거하는 것도 벅찬 일일 것입니다.
![]() 7. 비유두부 십이지장 선종. Non-ampullary duodenal adenoma
7. 비유두부 십이지장 선종. Non-ampullary duodenal adenoma
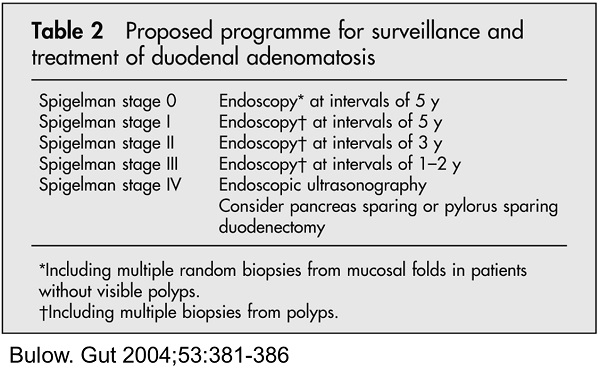
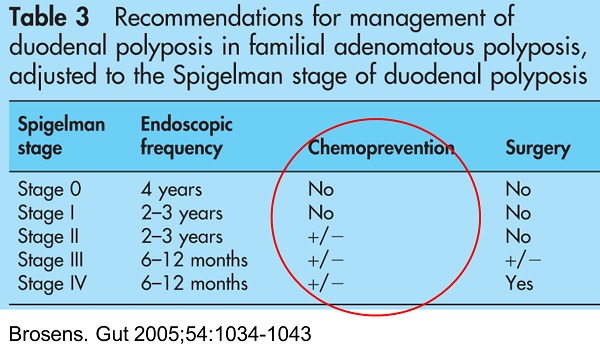
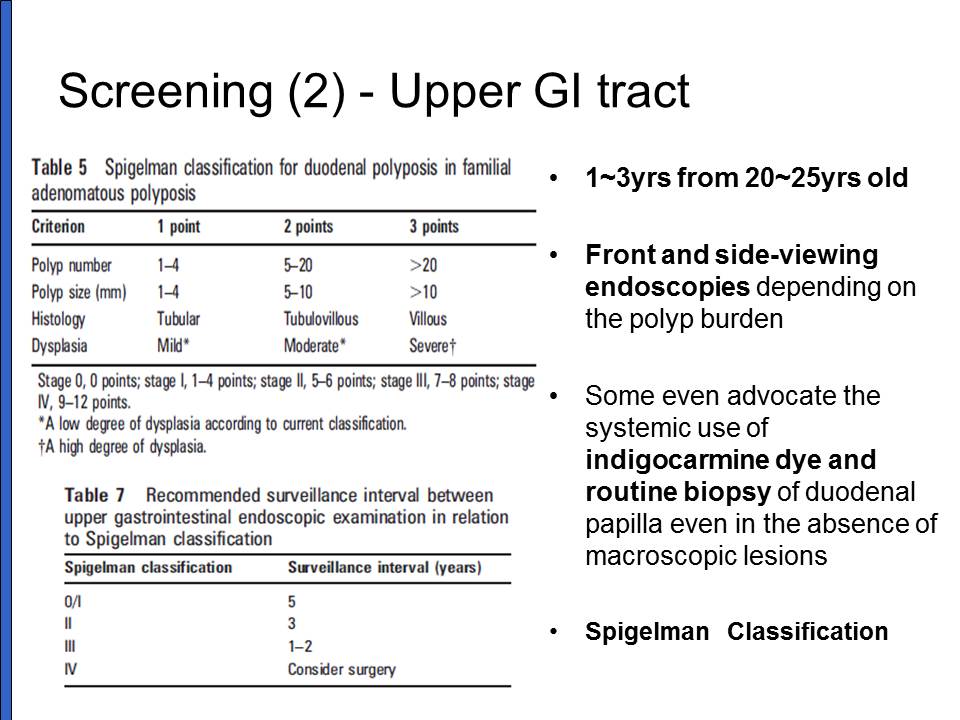
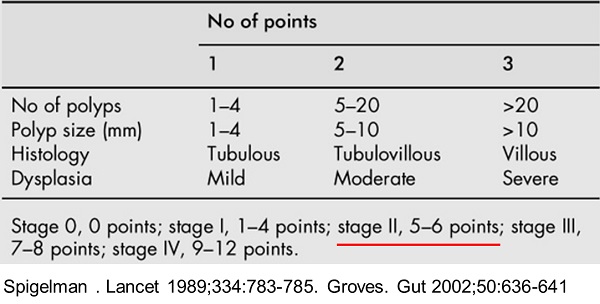
십이지장 선종은 FAP 환자의 대부분에서 발견되고 일생 동안 거의 100%에서 발생합니다. 십이지장 2부나 3부에 많습니다. 십이지장 선종은 수, 크기, 조직학적 분류, 그리고 이형성 정도 등 4가지 지표로 계산하는 Spigelman 병기로 분류합니다.
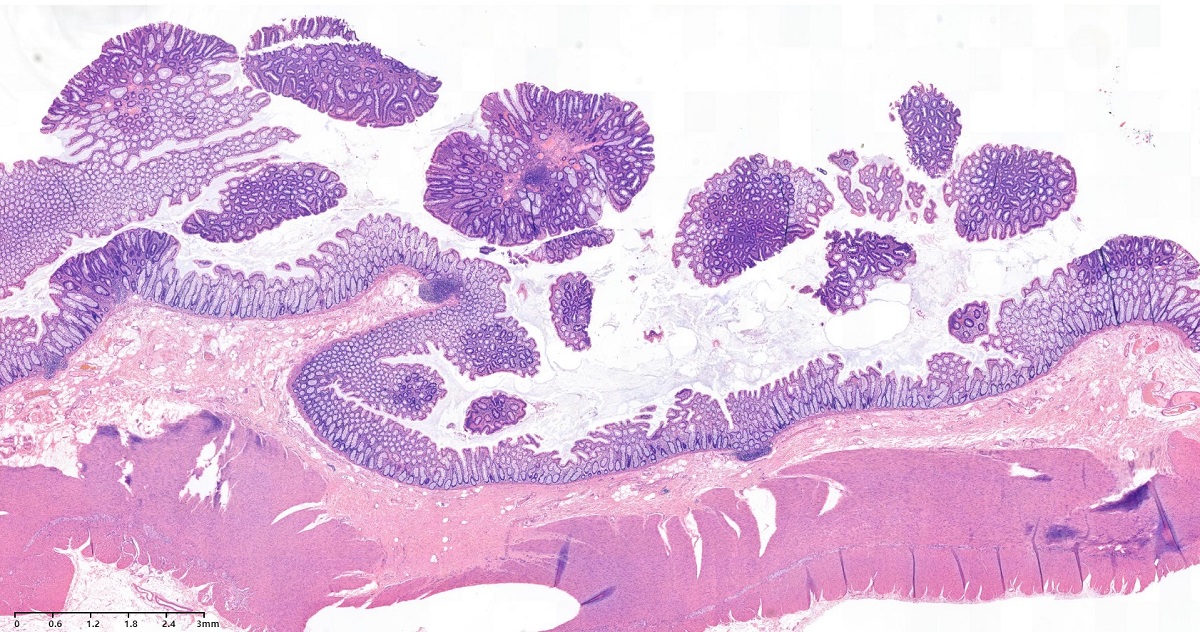
FAP 환자의 십이지장 선종 조직 소견. 십이지장 브루너샘 상방에 선종이 보인다.
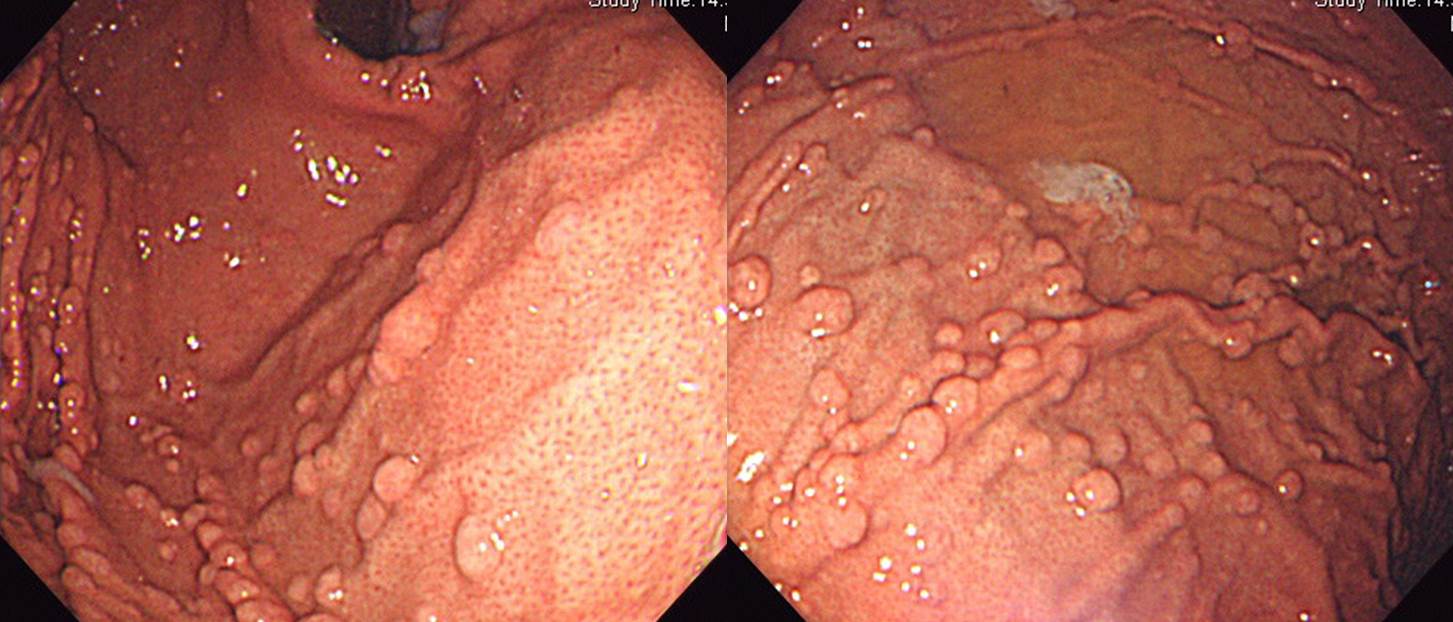
Duodenal adenomas in FAP
Duodenal adenomas in FAP
십이지장의 이러한 미세한 변화들에 대해서는 어떻게 할 것인가 고민입니다. 이 모든 것들을 선종으로 count 하면 Spigelman 병기가 높아지기 마련이니까요.
Pentax 사의 신형 내시경 Imagina를 이용하여 관찰한 FAP 환자의 십이지장 선종들입니다. 많은 선종들이 한 화면에 들어옵니다. 이 모든 것을 치료(소작술)할 필요가 있는지 불명확합니다. 아직까지 표준적인 치료는 경과관찰입니다. Sulindac 등의 효과는 입증되어 있지 않고 부작용 우려가 큽니다. 이래 저래 고민하지 않을 수 없습니다.
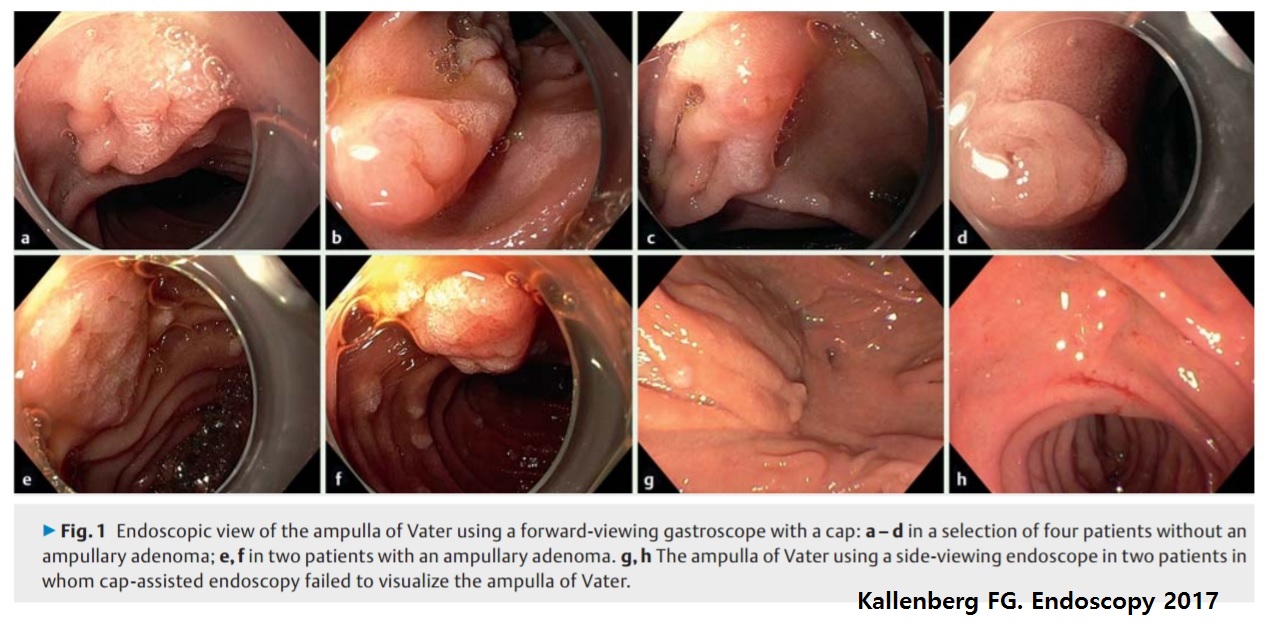
십이지장 유두부 선종은 직시경보다 측시경으로 잘 관찰할 수 있습니다. Cap을 장착한 직시경으로 관찰하면 측시경과 거의 비슷한 관찰을 할 수 있다는 연구도 있습니다 (Kallenberg FG. Endoscopy 2017). 그러나 모든 환자에서 Cap-직시경이나 측시경을 사용해야 할지는 미지수입니다. 저는 그냥 보통 직시경으로 관찰하고 있습니다.
십이지장 선종은 내시경에서의 처음의 Spigelman 병기에 따라 암 발생위험이 높아지는데, IV기 십이지장 선종 환자에서 암 발생 비율은 7%에서부터 36%입니다. FAP 환자 114명을 추적관찰한 연구에서 유두암 3명, 십이지장암 3명이 발생하였습니다. 십이지장 선종은 대부분 다발성이므로 한 두 개의 선종을 치료한다고 해결되는 것이 아닙니다. 재발할 가능성이 현실적으로 100% 입니다.
십이지장 선종의 치료원칙은 경과관찰을 하다가 Spigelman IV가 되면 수술(Whipple 혹은 PPPD)하는 것입니다. 그러나 암발생 위험이 높은 환자에서 경과관찰만 권하는 것은 쉽지 않습니다. 임상의들의 고민이 클 수 밖에 없습니다.
Sulindac이나 celecoxib를 쓰면 병소의 크기나 범위가 약간 줄어들지만 선종은 없어지지 않습니다. 장기간 약제 사용에 따른 부작용도 적지 않기 때문에 임상에서는 잘 처방되지 않습니다.
광역동치료가 시도된 바 있으나 이 또한 사용빈도는 낮습니다. 최근에는 간단하고 안전한 APC가 많이 사용되고 있습니다. APC의 효과에 대한 장기추적 성적은 아직 없습니다.
APC ablation을 이용한 십이지장 선종의 치료
또 다른 고민은 Spigelman 병기가 1-2인 환자에서 발견되는 십이지장암이 절반 정도 되는 것입니다. 참 어려운 이슈입니다.
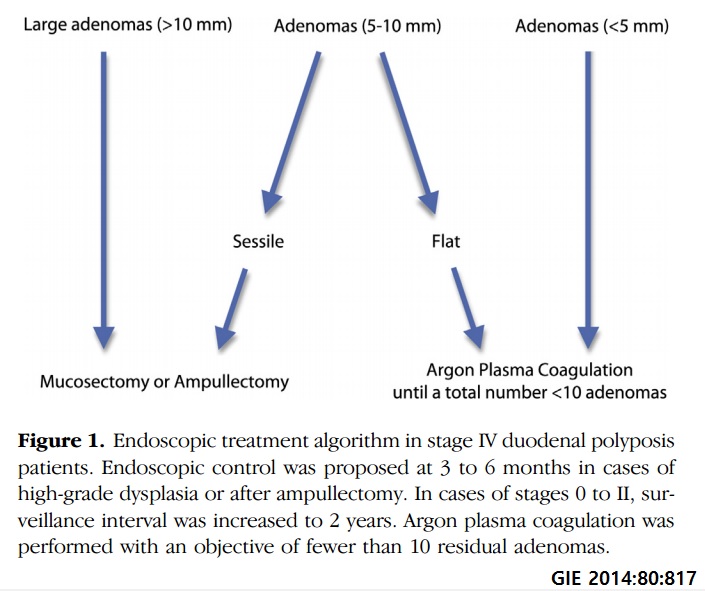
[2014-12-24 추가] Gastrointestinal Endoscopy 2014년 11월호에 Endoscopic treatment of severe duodenal polyposis... 논문이 실렸습니다. FAP 환자에서 십이지장 선종증이 심하면 수술을 하는 것이 원칙입니다만 늘 합병증이 걱정입니다. 2012년에는 postoperative morbidity rate가 42%라는 프랑스의 보고도 있었습니다. 이번 논문은 내시경으로 해도 대강은 된다는 것입니다. 장기 성적이 없으므로 좀 더 지켜봐야 하겠지만... 이번에 소개된 algorithm입니다.
[2019-4-25] FAP 환자의 duodenal adnoma에 대한 최근 문헌을 함께 공부하였습니다. 십이지장암을 예측하는데 Spigelman stage가 그다지 정확하지 않다는 내용이었습니다.
[American Society for Gastrointestinal Endoscopy guideline on the role of endoscopy in familial adenomatous polyposis syndromes (GIE 2020)]
Recommendations (duodenum). In summary, duodenal polyposis occurs in almost all FAP patients, with most having earlystage disease. Progression to stage IV disease occurs in about 15 to 20 years with a median age at diagnosis of duodenal cancer in the fifth decade. Important aspects of management are to identify and closely follow patients with risk factors for developing malignancy, such as those with Spigelman stages III and IV at baseline EGD, as well as individual polyp characteristics of HGD, polyp size >1 cm, and flat, carpeted growth that may be difficult to completely resect. Particular attention to the periampullary area, where 50% of the cancers occurs, is recommended. Endoscopic treatment is used to downstage disease with the goal to delay the development of stage IV disease. Advanced duodenal disease should be followed more closely and treated more aggressively. Once Spigelman stage IV is present, multidisciplinary discussion is recommended to assess the appropriate time for surgical resection. Although endoscopic resection of duodenal and ampullary lesions is recommended, it is unknown if this truly changes the natural history of cancer risk based on the original Spigelman stage because there is an underlying field defect in the duodenum. Further long-term prospective studies are needed to evaluate this important question.
이준행 註 (2020-5-9): 위에서는 매우 aggressive한 방법이 제시된 반면 십이지장에서는 내시경 치료의 효과를 자신하지 못하는 분위기군요. Ampullary area는 암발생이 많고 치료가 확실하게 될 수 있으므로 ampullectomy를 적극적으로 시행하는 것은 좋을 것 같습니다. Non-ampullary area에서는 무리하지 않는 것이 나을 것입니다. 저는 가끔 ablation을 하기도 하지만 그냥 경과관찰 하는 환자도 많습니다.
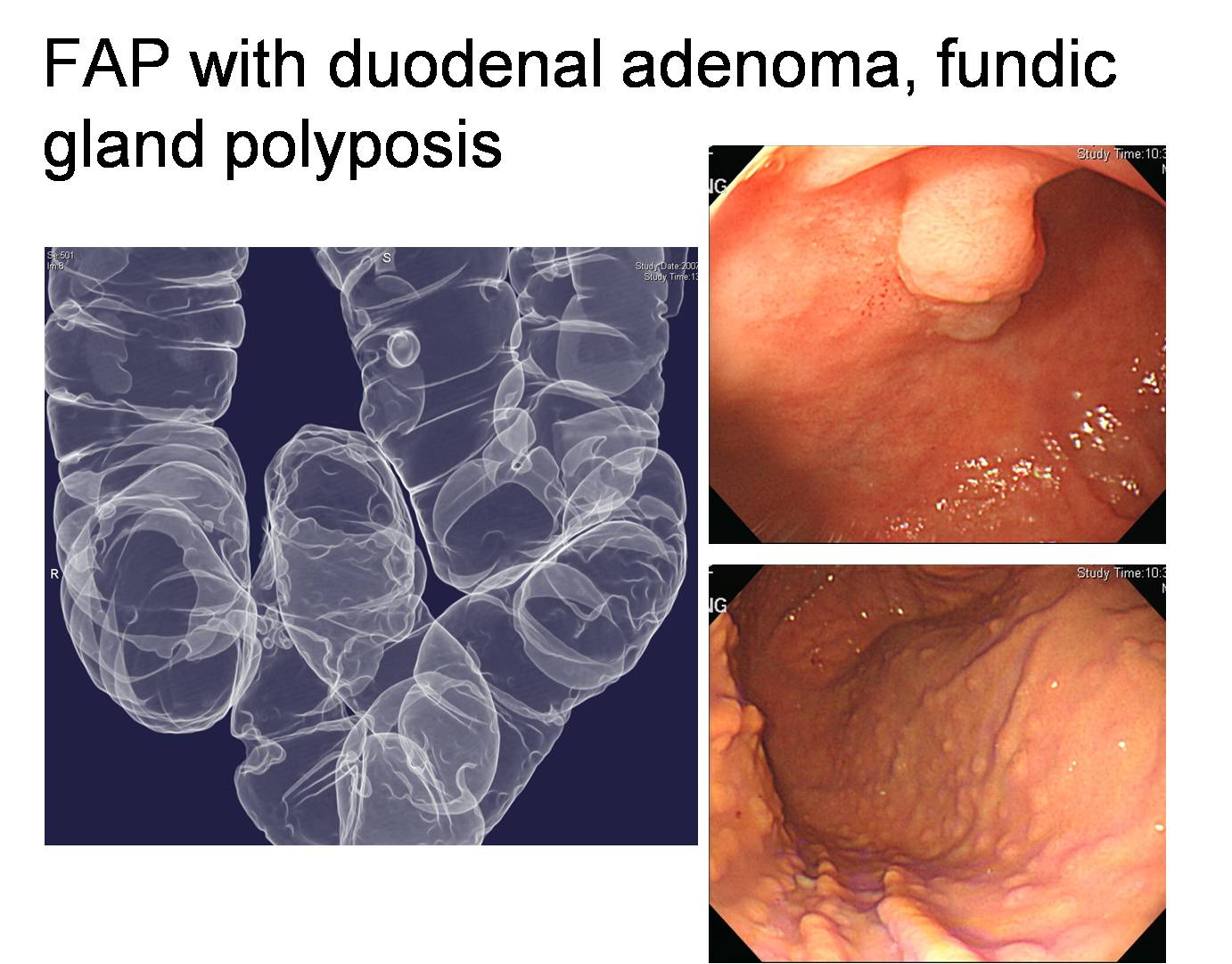
20년 전 대장암 수술하신 FAP 환자의 multiple duodenal adenomas와 fundic gland polyposis. 수 년 간 관찰 중이지만 큰 변화가 없었음.
Intensive downstaging polypectomy (IDP) for multiple duodenal adenomas, 즉 매우 많은 polypectomy를 해서 duodenal adenomas를 관리하는 방법이 소개되었습니다 (Endoscopy 2023). 오직 일본에서만 할 수 있는 일이라고 생각합니다. 우리나라 현실에서는 불가능.
[2025-2-7] 금요내시경세미나 후 comment
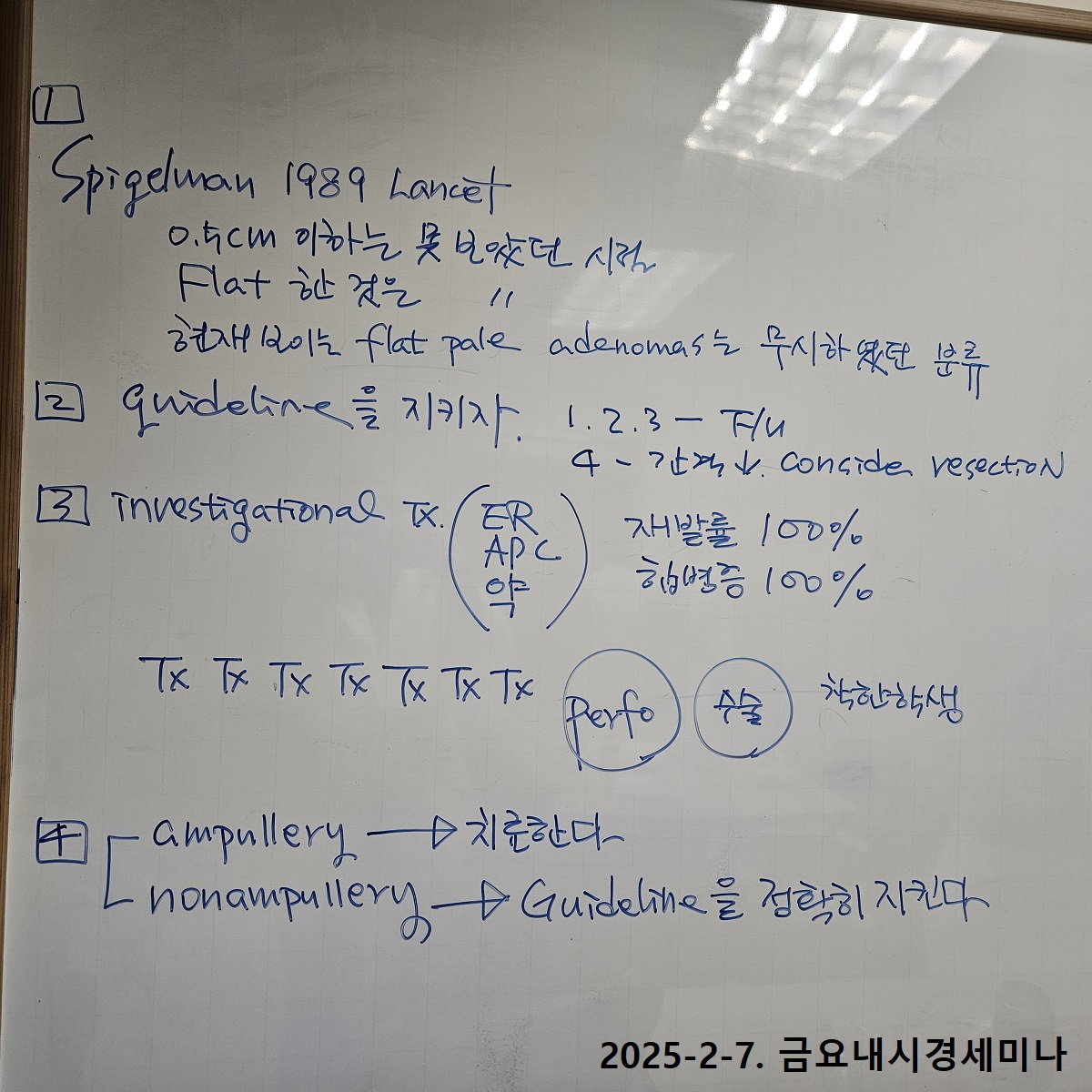
금요내시경세미나에서 FAP 환자의 duodenal adenoma에 대한 토론이 있었습니다. FAP 환자의 생존율이 높아지면서 십이지장 병소를 자주 만나게 됩니다. Ampullary와 non-ampullary를 나누는 것이 우선입니다. Ampullary adenoma는 대부분 절제술을 하면 되는데 non-ampullary adenoma는 힘조절이 중요합니다. 세상사 모두 그렇지만 적절한 치료가 중요한 치료입니다. 저는 가이드라인을 따를 것을 권합니다. 가이드라인은 Spigelman stage 3까지는 치료 없이 경과관찰을 하는 것입니다. 물론 investigational 치료도 고려할 수 있지만 합병증 발생률이 너무 높아서 걱정입니다.
![]() 8. 위저선용종증. Fundic gland polyposis
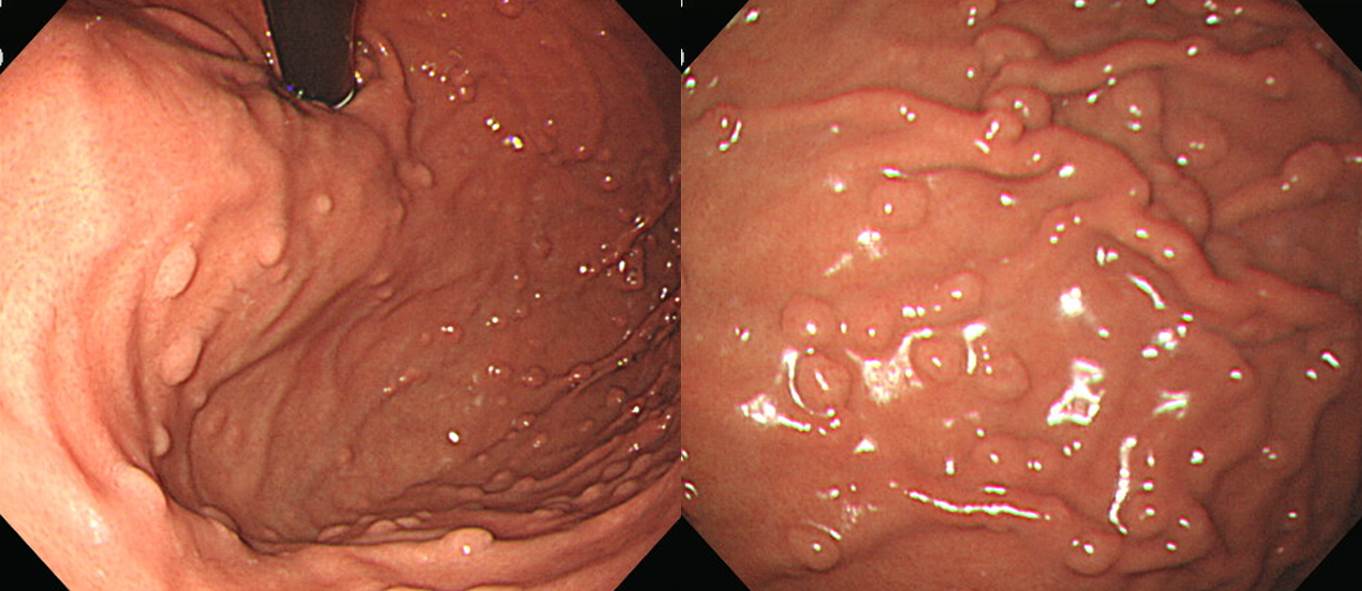
8. 위저선용종증. Fundic gland polyposis


위저선 용종은 FAP 환자의 90%에서 발견됩니다. FAP 환자가 아닌 일반인에서 우연히 발견되는 소수의 산발적 위저선 용종은 전암성 병소가 아니므로 아무런 치료도 필요하지 않습니다. 그에 반하여 FAP 환자의 위저선 용종은 40% 정도에서 이형성을 보입니다. 즉 FAP 환자의 위저선 용종은 병리학적인 관점에서 산발적인 위저선 용종과 차이가 있습니다. FAP 환자에서 위저선 용종의 이형성이 선행된 상태에서 이차적으로 APC 변이가 발생시에는 매우 드물지만 전암성 병소가 될 가능성도 가지고 있습니다. 그러나 그 빈도는 매우 낮기 때문에 FAP에서 발견되는 위저선 용종에 대해서는 특별한 치료를 하지 않고 경과관찰만 권하고 있습니다.
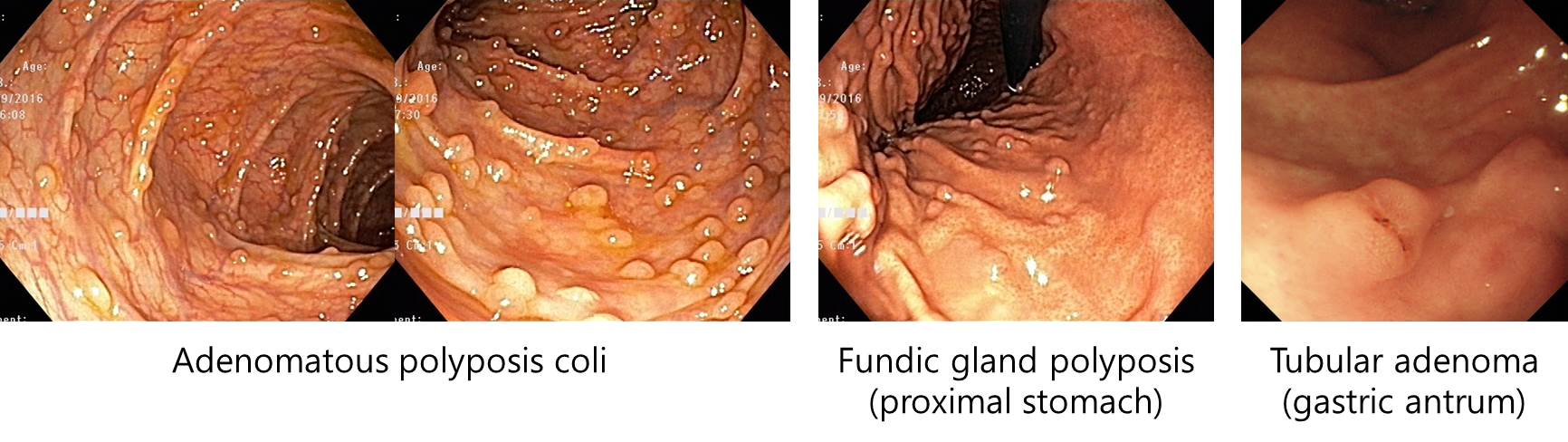
(2017, F/25) 대장 선종이 attenuated FAP 정도 혹은 그보다 약간 많은 정도이지 대장 전체가 adenomatous polyp들로 깔린 경우는 아닙니다. 그러나 위에 뚜렷한 fundic gland polyposis가 있는 것으로 유추하건데 FAP가 틀림없습니다.
FAP로 total colectomy를 받으신 분의 위내시경에서 위저부와 위체부에 다발성 용종이 발견되었습니다. 전형적인 fundic gland polyposis입니다. 조직검사에서 fundic gland polyp으로 판독되는 것이 당연하겠지만 간혹 hyperplastic polyp으로 판독되기도 합니다. 병리판독 결과와 무관하게 이런 경우는 fundic gland polyposis가 옳습니다.
FAP 환자에서 몇 개 정도의 fundic gland polyps 만 있는 경우도 가능합니다.
FAP 환자에서 fundic gland polyposis는 대부분 매우 많거나 없거나 둘 중 하나입니다. 몇 개만 있는 경우는 흔하지 않은 것 같습니다. 이 환자는 fundic gland polyp의 수도 작고 높이도 낮아서 언끗 보면 fundic gland polyposis가 없다고 오인하기 쉬운 경우입니다.
FAP 환자이신데 gastric fundic gland polyposis가 없었던 경우
Colon, total colectomy : Numerous tubular adenomas with low grade dysplasia (more than 2000) ;
1) size: up to 0.4x0.3 cm
2) resection margin: free from adenoma
![]() 9. 위선종. Gastric adenoma
9. 위선종. Gastric adenoma
FAP 환자의 위선종에 대한 자료는 거의 없습니다. FAP에서 위선종의 발생률이 낮고 그 동안 관심이 없었기 때문에 자료가 부족하여 자연경과도 알기 어렵습니다. 위암과 위선종이 많은 우리나라에서 FAP 환자의 위선종이 더욱 많이 발견되는 것 같습니다. 그러나 FAP 환자의 위선종이 FAP와 관련된 것인지는 알기 어렵습니다다. 2011년 국내 문헌에 의하면 상부위장관 내시경을 시행한 FAP 148명에서 위선종이 14.2%, 위암이 2.7%였습니다 (Park. Gut Liver 2011;5:46-51).
현실적으로 선종이 소수면 내시경절제술을, 다수면 소작술을 시행할 수 밖에 없습니다. 그런데 해도 해도 또 생깁니다. 할만큼 했는데 또 생기면 지쳐서 그만 둘 수 밖에 없기도 합니다. 암이 되는 그날까지 그냥 두는 수 밖에 없을 수도 있습니다.
FAP 환자에서 발견된 위선종
FAP 환자에서 발견된 다발성 위선종에 대한 내시경 절제술

Gastric adenomas in FAP
Gastric adenomas and duodenal adenoma in FAP
Gastric adenoma in FAP
![]() 10. 위암. Gastric cancer
10. 위암. Gastric cancer
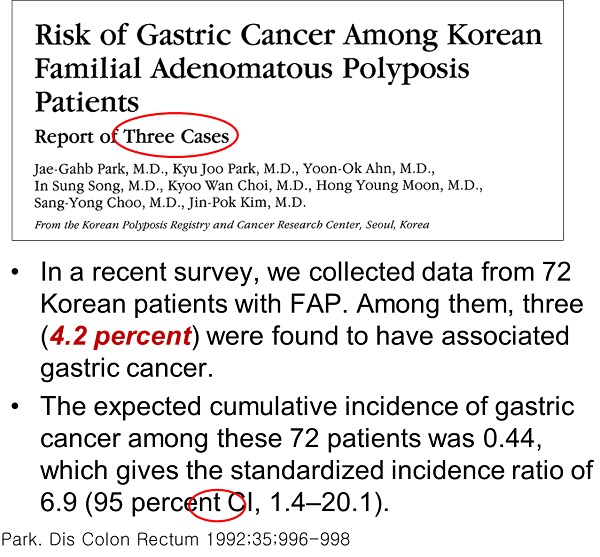
FAP 환자에서는 일반인에 비하여 (1) 발생률이 약 3배 높고, (2) 발생연령이 낮고, (3) 다발성이고, (4) 위 하부에 발생합니다. 한국과 일본에서 FAP 환자의 위암 발생률이 높은 경향입니다. FAP 환자에서 발생한 위암이 FAP와 직접 관련된 것인지 알기는 어렵습니다.
위암에 대하여 가장 보편적인 수술은 subtotal gastrectomy with Billroth II anstomosis입니다. FAP 환자에서 이 수술을 시행하면 한가지 문제가 생깁니다. 십이지장에 대한 surveillance를 할 수 없다는 점입니다. FAP 환자의 대장 수술 후 가장 흔한 사망원인이 십이지장이므로 surveillance는 필수적인데 이게 불가능해지면 큰 문제가 아닐 수 없습니다. 가능하면 B-I anastomosis를 하도록 추천하고 있습니다.
![]() 11. Extracolonic manifestations and related conditions
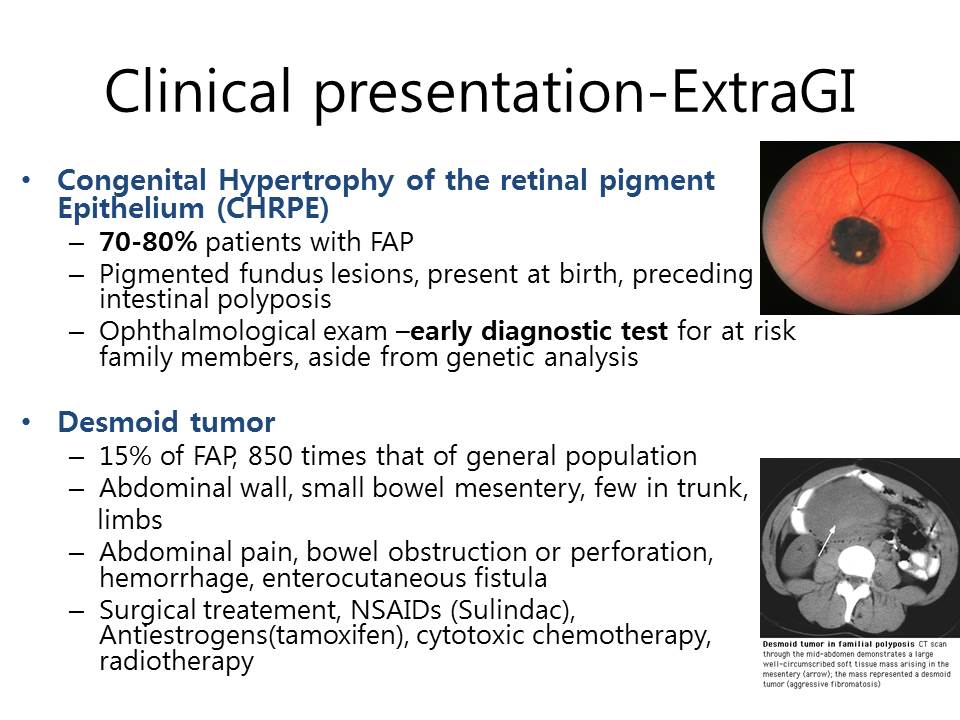
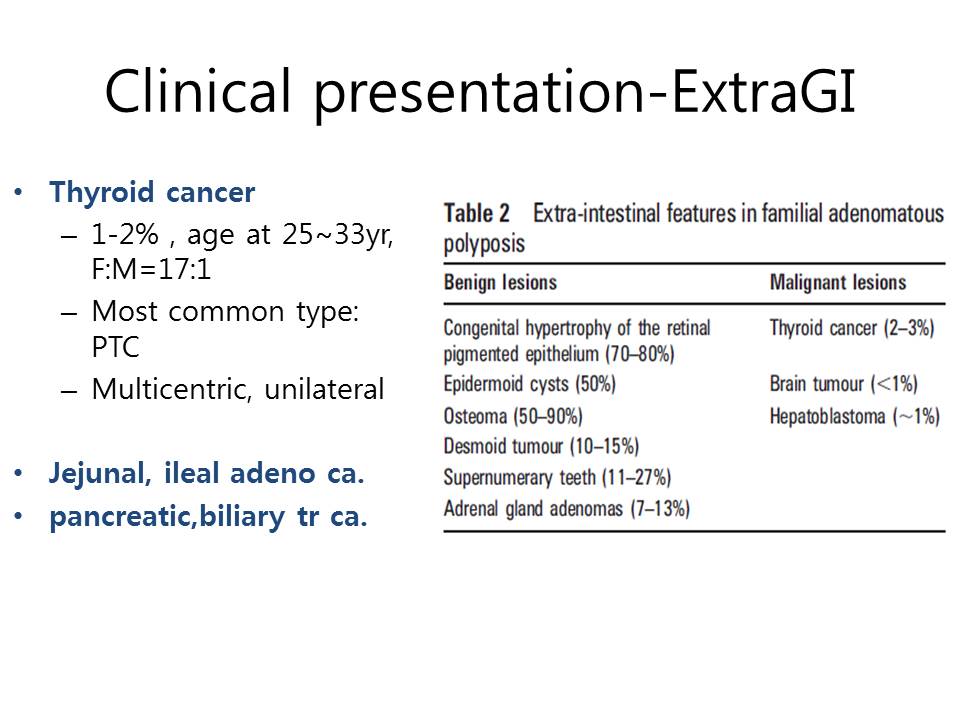
11. Extracolonic manifestations and related conditions
갑상선암으로 수술 후 대장 검사를 통하여 FAP로 확진된 환자입니다. 병리 결과는 아래와 같습니다.
Thyroid gland, lymph node, total thyroidectomy with central(anterior compartment) neck dissection: Papillary carcinomas (x3):
1) Subtype: Cribriform-morular variant
2) Tumor location: Both lobes
3) Tumor size: 0.8x0.8x0.8cm (lower pole, right), 0.3x0.3x0.2cm (mid pole, left), 1.5x1.2x1.1cm (lower pole, left) (참고: cribriform-morular 갑상선암 중 FAP와 연관된 경우는 다발성이 많음)
4) Lymph vessel invasion: Absent
5) Blood vessel invasion: Absent
6) Extrathyroid extension: Present (minimal)
7) Surgical margins: Negative
8) Tumor multicentricity: Present
9) Lymph nodes ; No regional lymph node metastasis (0/2: "right central LN", 0/1; "left central LN", 0/1)
10) Other pathology: None
11) Parathyroid glands: No
12) pT1b N0
β-catenin: Positive in tumor cells
p27: Positive (1+, 5%)
Cyclin D1: Positive (2+, 25%)
Note: This tumor is associated with germline mutations in APC gene (e.q, familial adenomatous polyposis) although rarely associated with somatic mutations. Clinical work up is recommended.
Cribriform morular type thyroid cancer 병리 자료 (다른 환자). Cribiriform한 모습이 잘 보임.
Pathology outlines
그 많은 갑상선암 환자 중 왜 이 환자만 FAP 검사를 했을까요? 갑상선암의 병리학적 특성 때문이었습니다. FAP와 동반되는 경우가 많은 histological subtype이었기 때문에 병리과에서 FAP 가능성을 언급하였고, 내과에서 이를 확인하였습니다.
*참고: Cribriform-morular variant of papillary thyroid carcinoma: a distinctive type of thyroid cancer (2017)
"The aim of this systematic review is to study the features of cribriform-morular variant of papillary thyroid carcinoma (CMV-PTC) by analysing the 129 documented cases in the English literature. The disease occurred almost exclusively in women. The median age of presentation for CMV-PTC was 24 years. Slightly over half of the patients with CMV-PTC had familial adenomatous polyposis (FAP). CMV-PTC presented before the colonic manifestations in approximately half of the patients with FAP. Patients with FAP often have multifocal tumours in the thyroid. Microscopic examination of CMV-PTC revealed predominately cribriform and morular pattern of cancer cells with characteristic nuclear features of papillary thyroid carcinoma. Psammoma body is rare. On immunohistochemical studies, β-catenin is diffusely positive in CMV-PTC. The morular cells in CMV-PTC are strongly positive for CD10, bcl-2 and E-cadherin. Pre-operative diagnosis of CMV-PTC by fine-needle aspiration biopsy could be aided by cribriform architecture, epithelial morules and β-catenin immunostaining. Mutations of APC gene are found in the patients with CMV-PTC associated with FAP. In addition, mutations in CTNNB1, RET/PTC rearrangement and PI3K3CA mutations have been reported. BRAF mutation is negative in all CMV-PTC tested. Compared to conventional papillary thyroid carcinoma, CMV-PTC had a lower frequency of lymph node metastases at presentation (12%) and distant metastases (3%) as well as lower recurrence rates (8.5%) and patients' mortality rates (2%). To conclude, patients with CMV-PTC have distinctive clinical, pathological and molecular profiles when compared to conventional papillary thyroid carcinoma."
2026년 2월 은퇴이신 정재훈 교수님의 '최신 임상갑상선학 2'에서 옮깁니다. 특이한 점은 이 책이 비매품이라는 것입니다. 발간사에는 2024년 봄 제작된 '최신 임상갑상선학'도 100여부만 제작하여 제자들과 일부 지인들에게만 배포하였다는 내용이 있습니다. 미배품이기 때문인지 영한 혼용으로 씌여 있어 편하게 읽힙니다. 제가 좋아하는 style입니다.
"2022년 WHO 분류에 의하면 cribriform-morular 갑상선암은 더 이상 갑상선 유두암의 variant가 아니다... 삼성서울병원에서 15예의 cribriform-morular 갑상선암을 분석한 결과 평균 연령은 26세, 평균 종양 크기는 1.0cm였다... 2예를 제외하고 모든 예에서 초음파는 양성종양을 시사하는 소견이었다. 세포검사에서 9예는 classic PTC로, 1예는 여포종양으로, 그리고 5예에서만 cribriform-morular 갑상선암으로 진단하였다... APC 유전자의 somatic mutation이나 beta-catenin 유전자 변이(CTNNB1)도 APC 유전자의 germ-line mutation과 마찬가지로 cribriform-morular 갑상선암을 유발할 수 있다."
![]() 12. Screening policy
12. Screening policy
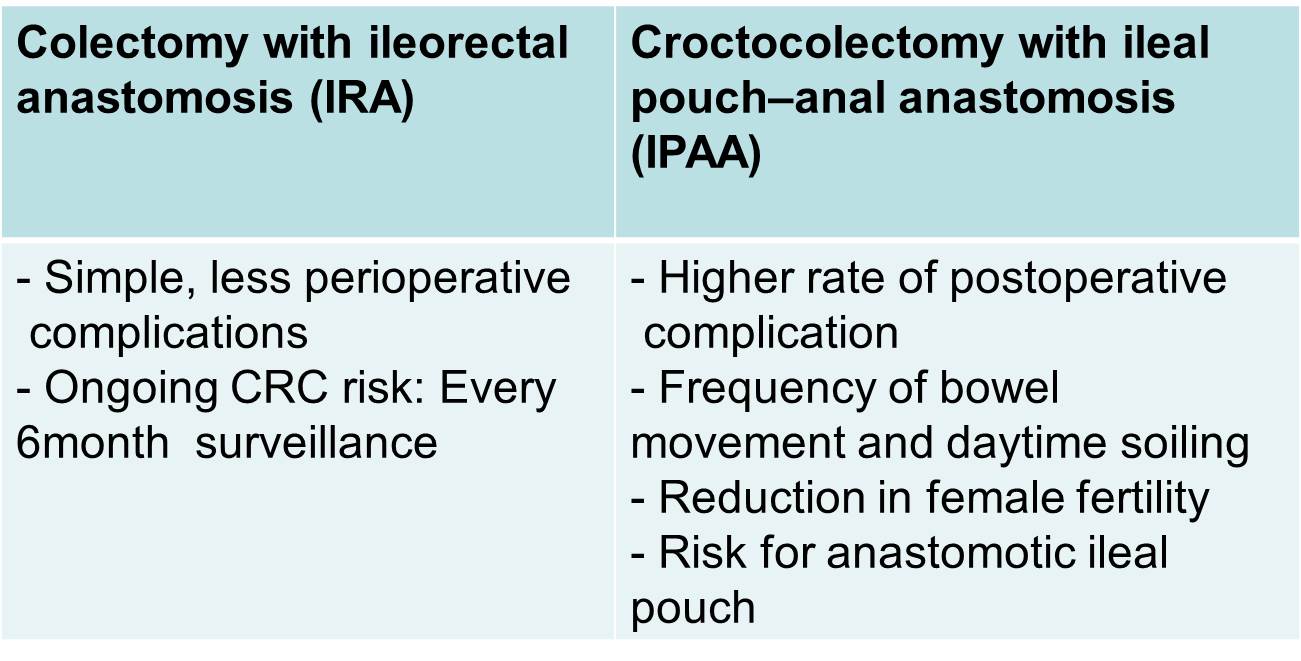
![]() 13. Treatment
13. Treatment
Familial adenomatous polyposis: long-term outcomes of pouch surveillance and risk of neoplasia. Endoscopy 2023
The long-term outcomes for pouch surveillance in familial adenomatous polyposis are unknown. This retrospective cohort study examined risk factors for adenomas or advanced lesions following pouch surgery and included a group with over 10 years of surveillance. Pouch adenoma progression was slow and most advanced lesions occurred after 10 years. High grade dysplasia and cancer were rare. Patients engaging early in a surveillance program may be able to have a personalized surveillance strategy based on their pouch phenotype.
![]() 14. FAP 환자가 total colectomy를 거부한다면?
14. FAP 환자가 total colectomy를 거부한다면?
2016년 1월호 Endoscopy지에 일본 연구자들이 total colectomy를 거부한 환자의 내시경 치료에 대한 놀라운 논문을 발표했습니다 (Ishikawa H. Endoscopy 2016). 세 센터의 환자를 모은 후향적 연구였는데 inclusion criteria는 다음과 같았습니다.
Included patients were adults with FAP who had > 100 colorectal adenomas and/or a germline mutation in the APC gene, detected primarily by the Protein Truncation Test, and who strongly refused to undergo colectomy and were managed instead by endoscopic polyp clearance. The following patients were excluded: 1) patients with CRC, 2) those with large adenomas not amenable to endoscopic removal, 3) those with dense polyposis, or 4) patients who refused further endoscopic removal.
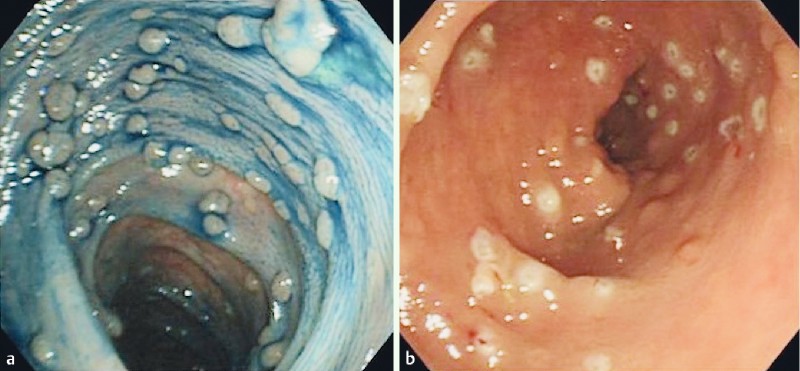
Figure 1. Endoscopic images. a Before polypectomy. b After polypectomy.
평균 29세에 찾아온 환자 95명을 5.1년 경과관찰하면서 환자 당 8회의 대장내시경을 통하여 55,701개의 용종을 제거하였습니다. 환자 당 475개의 용종(내시경 검사 당 73개)을 제거한 셈입니다. 1,000개 이상의 용종을 제거한 환자도 16명이나 되었습니다. 이 많은 용종을 제거했는데 출혈이나 천공은 하나도 없었다고 합니다. 더욱 놀랍습니다.
Results: Of the 95 eligible patients, five (5.3 %) were excluded. The remaining 90 patients (median age at first visit 29 years [range 16-68 years]; 46 males) were followed for a median of 5.1 years (interquartile range [IQR] 3.3-7.3 years). During this period, a total of 55,701 polyps were resected without adverse events such as bleeding or perforation. The median numbers of endoscopic treatment sessions and polyps removed per patient were 8 (IQR 6-11) and 475 (IQR 211-945), respectively. Five patients had noninvasive carcinoma (Category 4.2 according to the revised Vienna classification), detected within 10 months from the start of the follow-up period. All of these patients were treated endoscopically, without signs of recurrence during a median follow-up of 4.3 years (IQR 2.0-7.1 years). No invasive colorectal cancer was recorded during the study period. Two patients (2.2%) underwent colectomy because the polyposis phenotype had changed to dense polyposis.
Conclusion: Endoscopic management of FAP is feasible and safe in the medium term.
물론 용종이 너무 많았던 FAP 환자의 경우("dense polyposis")는 처음부터 제외되었습니다. 아무리 그렇더라도 한 환자당 거의 500개의 용종을 제거한다는 것은 저로서는 도저히 상상할 수 없는 일입니다. 저자들은 "medium term"에서는 별 문제가 없는 것 같다고 하였지만 long term 결과를 꼭 살펴봐야 할 연구라고 생각됩니다.
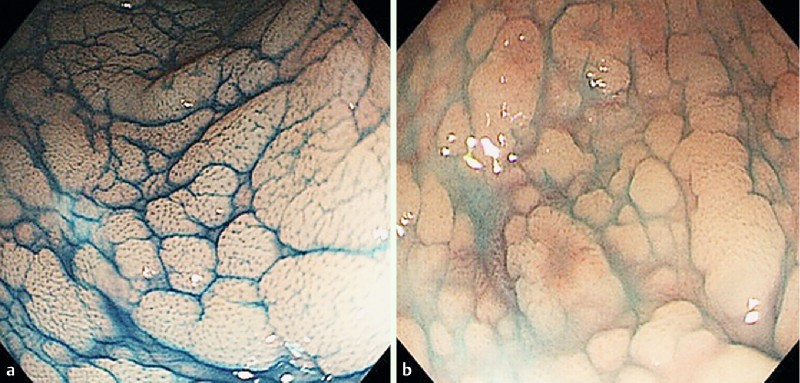
Figure 3. Endoscopic appearance of dense polyposis. a With indigo carmine dye application. b Without indigo carmine dye application. The entire surface of the mucosa is covered with innumerable flat adenomas.
이번 일본 연구 다음에 Spain의 연구가 실렸습니다 (Valentin F. Endoscopy 2016). 일부 FAP가 포함되었는지는 모르겠으나 10-100개 정도의 대장 용종이 있었던 265명에 대한 후향적 연구였는데 제법 많은 사람들이 암이 되거나 수술을 받았습니다.
Patients underwent a median of 5 colonoscopies, and 17 patients (6.4 %) were diagnosed with CRC. A total of 32 patients (12.1 %) underwent surgery, including 15 (5.7 %) for prophylaxis without a diagnosis of CRC.
일본 연구와 스페인 연구를 종합하여 미국의 Andrew Kaz (제가 2007년 미국 Seattle 연수 시절에 같은 실험실에서 함께 일했던 동료였습니다)가 editorial을 썼습니다. 비록 일본에서 좋은 결과를 보여주었지만 아직 수술을 하라는 가이드라인(AGC guideline 2015)을 바꿀 때는 아니다고 쓰고 있습니다.
While these studies do offer some reassurance about the feasibility of endoscopic management of patients with colon polyposis, the intensive procedural demands of the Japanese study, the relatively high cancer risk seen in the Spanish study, and the modest duration of follow-up should make us cautious about revising any current treatment guidelines. So what counsel should we provide to our patients with colon polyposis? First, based on our cumulative knowledge about colon polyposis syndromes, we should continue to stress that colectomy remains the treatment of choice for FAP or in any case of polyposis where endoscopic clearance of colon polyps is no longer achievable, as per current guidelines. Second, chemoprevention with nonsteroidal anti-inflammatory drugs such as aspirin, sulindac, or celecoxib has been shown to reduce the colorectal polyp burden in polyposis syndromes, although their effect on preventing cancer in these patients is less clear. Clinicians should emphasize that these medications are no substitute for colectomy, but they may make the strategy of colonoscopy and polypectomy more successful by reducing polyp size and/or number.?For those who decline colectomy or for whom colectomy is not yet indicated, it appears that carefully selected cases can be managed with polypectomy in the short term. We agree with Ishikawa et al. and others that high risk patients who defer colectomy should be managed by expert endoscopists with the capacity to offer chromoendoscopy, endoscopic mucosal resection, and other advanced resection techniques in a setting that allows for lengthy procedures . Although the optimal colonoscopy surveillance interval for patients with FAP and other polyposis syndromes who decline colectomy has yet to be determined, it is important for clinicians to educate this patient population about their cancer risk as precisely as possible and to ensure that they understand the limited evidence regarding long term outcomes of endoscopic treatment.
![]() [FAQ]
[FAQ]
[일자 미상. 애독자 질문]
FAP 및 hernia 로 수술 후 주기적으로 경과관찰 중인 분의 EGD를 시행하였습니다. Ampullary adenoma와 duodenal adenoma들을 발견하고 조직검사에서 모두 tubular adenoma로 확인되었습니다. 선종 개수를 명확히 셀 수는 없었지만 modified Spigelman's score 에 따르면 점수는 6-7점, stage II 이하가 아닐까 생각됩니다. 내시경 시행 당시 EGD로는 병변의 distal margin을 정확히 그리기 어려웠습니다. 이런 경우에 colonoscopy로라도 다시 재검사를 해서 십이지장을 모두 들여다 볼 필요성이 있는지, multiple duodenal adenomas는 내시경적으로 모두 절제하기 어려울 것으로 보이는데 ampullary adenoma는 내시경 절제를 해주는 것이 좋은지 여쭈고 싶습니다. 아니라면 6개월에 한번씩 내시경을 하다가 암 발생시 소장절제술을 해주는 것이 좋은 방법일까요.
[이준행 답변]
십이지장선종은 FAP 환자의 대부분에서 발생합니다. 십이지장 제 2부와 제 3부에서 많습니다. FAP 환자에서 십이지장선종은 수, 크기, histology (villous component 여부), dysplasia의 정도로 계산하는 Spigelman stage로 분류합니다. 십이지장 선종은 10% 정도 암발생 위험을 가진다고 보고 있습니다. 질병의 특성상 십이지장 선종은 다발성일 수 밖에 없으므로 선종 한 두 개를 치료한다고 해결되지 않습니다. 100% 재발한다고 보면 됩니다.
교과서나 논문에는 FAP 환자의 십이지장선종은 우선 경과관찰을 하다가 Spigelman stage IV가 되면 수술(이때 수술은 Whipple)을 하라고 되어 있습니다. 그러나 암발생 위험이 높은 환자에서 아무 치료도 하지 않기는 어렵기 때문에 고민일 수 밖에 없습니다. Sulindac이나 celecoxib를 쓰면 병소의 크기나 범위가 약간 줄어들지만 선종이 없어지는 것은 아닙니다. 부작용도 적지 않기 때문에 잘 처방되지 않고 있습니다. 최근에는 APC를 이용한 소작술이 유행입니다. 그러나 아직 이에 대한 좋은 임상연구는 없습니다. 유두선종은 내시경절제술을 해 주는 것이 보통입니다.
요컨데 유두선종 ampullectomy, 십이지장선종 APC 소작술을 권하겠습니다. 특별히 obstruction의 증세가 없으면 대장내시경으로 십이지장을 좀 더 깊숙히 볼 필요는 없다고 생각합니다.
[2014-4-10. 애독자 질문]
늘 귀한 자료 보내주셔서 아주 유익하게 도움 받고 있습니다. FAP 환자 증례를 잘 보았습니다. 제 환자 한 분이 FAP로 total colectomy를 했는데 위에서 반복적으로 선종이 발견되고 있습니다. 이 경우 선생님은 어떻게 하시는지요? 처음 발견된 것은 ESD를 했습니다만, 6개월 간격 추적검사에서 자꾸 선종이 발견되어 이제는 아예 APC로 소작술만 하고 있습니다. Total gastrectomy를 하기도 그렇구요... 그리고 선생님 증례처럼 duodenal adenomatosis가 있는 경우 참 난감할 것 같습니다.^^
[2014-4-11. 이준행 답변]
Germline mutation에 의한 병이므로 치료를 서두르기보다는 경과관찰을 잘 하다가 적절한 시점에 intervention을 하면 되겠습니다. 병변이 한두개면 절제술을 할 수 있고, 여러개면 소작술을 하거나 아니면 아예 지켜보는 것도 방법입니다. 치료없이 지켜보는 것이 마음에 걸리지만 현재 교과서적인 방법은 심해지기 전까지는 치료없이 지켜보는 것입니다. 지켜보는 것에 대하여 마음의 부담을 가질 필요는 없다고 생각합니다. 저는 "할 수 있으면 한다. 그러나 무리는 안 한다"라는 입장입니다. 아래 관련 자료를 참고하시기 바랍니다.
[2015-2-17. 애독자 질문]
매일같이 선생님의 일일공부를 받아보니, 늘 선생님과 얼굴을 마주하고 사는 기분입니다. 감사합니다. 구정 새해도 복 많이 받으십시오.
그리고 선생님께 한가지 여쭤볼 것이 있습니다. FAP으로 과거 total colectomy를 시행한 환자인데, angle에 ulcer가 있고 작은 nodular lesion이 angle을 중심으로 분포하고 있었습니다. 또한 duodenum도 몇개의 용종이 2nd portion에 있었습니다. 처음에는 angular lesion이 ulcer를 동반하고 있어 AGC로 생각하고 Bx하였고 nodule들도 Bx를 하였는데 cancer는 확인되지 않고 전부 tubular adenoma with low grade dysplasia만 나왔습니다. 위 병변에 대해서는 다시 EGD Bx를 할 생각인데, 문제는 십이지장 병변들도 모두 tubular adenoma with low grade dysplasia였습니다. papilla역시 neoplastic하였으나 pancreatitis 우려 때문에 Bx는 하지 않은 상태입니다. 위 병변에 대해서는 아마도 gastrectomy를 해야하지 않을까 생각도 되는데, 만일 위를 수술했다고 하더라도 small bowel에 있는 adenoma들이 또 걱정입니다. 지금은 2-3개 정도와 papillary lesion정도만 본 상태이지만 더 깊이 들어가면 더 많은 병변이 나올 수 있을 것 같아 고민입니다.
[2015-2-20. 이준행 답변]
고민되는 환자라는 점에 동의합니다. 정답이 없는 이유라고 생각됩니다만, 저의 생각은 과거에 말씀드린 바와 같습니다.
"Germline mutation에 의한 병이므로 치료를 서두르기보다는 경과관찰을 잘 하다가 적절한 시점에 intervention을 하면 되겠습니다. 병변이 한두개면 절제술을 할 수 있고, 여러개면 소작술을 하거나 아니면 아예 지켜보는 것도 방법입니다. 치료없이 지켜보는 것이 마음에 걸리지만 현재 교과서적인 방법은 심해지기 전까지는 치료없이 지켜보는 것입니다. 지켜보는 것에 대하여 마음의 부담을 가질 필요는 없다고 생각합니다. 저는 "할 수 있으면 한다. 그러나 무리는 안 한다"라는 입장입니다." (2014-4-11. 이준행)
Ampulla of vater의 선종은 papillectomy를 권합니다. 그러나 gastrectomy를 고려할 단계는 아닌 것 같습니다. 위와 십이지장의 다발선 선종은 내시경치료를 권합니다. Total gastrectomy와 Whipple 수술을 할 수도 있겠지만 암이 아닌 단계에서 그런 큰 치료가 필요한지도 의문이면서 삶의 질 저하의 문제도 고려해야 합니다. 절제술이나 소작술 등 적절한 내시경치료를 하면서 경과관찰을 하다가 선종이 너무 심해지거나 암이 된 경우에 수술을 고려해도 늦지 않을 것 같습니다.
[2020-5-27. 애독자 질문]
이준행 교수님께서 주신 내시경 quiz에 전형적인 FAP 환자가 있었습니다 (http://endotoday.com/endotoday/learning_05.html). 일단 adenomatous polyposis라는 진단명을 붙였는데요... "Familial"이라는 표현을 가계 history를 조사하지 않고 붙일 수 있는 지 궁금합니다.
[2020-5-27. 이준행 답변]
좋은 질문입니다. 내시경 소견 (대장 adenoma >= 100, 십이지장 flat adenoma, ampullary tumor, gastric fundic gland polyposis 등)이 있으면 진단은 거의 확실합니다. 원인은 APC 유전자의 germline mutation입니다. 80%는 가족력이 있고 20%는 없는 sporadic case입니다. 가족력이 없더라도 일단 환자가 되면 (= germline APC gene mutation이 생기면) 자식에게 autosomal dominant로 유전됩니다. 따라서 familial이라는 수식어를 붙이는데 하등에 어려움이 없습니다. Adenomatous polyposis라는 애매한 표현보다는 FAP라는 명료한 진단명을 쓰시기 바랍니다. 돌직구를 날리세요.
[2025-2-7] 금요내시경세미나 후 comment
금요내시경세미나에서 FAP 환자의 duodenal adenoma에 대한 토론이 있었습니다. FAP 환자의 생존율이 높아지면서 십이지장 병소를 자주 만나게 됩니다. Ampullary와 non-ampullary를 나누는 것이 우선입니다. Ampullary adenoma는 대부분 절제술을 하면 되는데 non-ampullary adenoma는 힘조절이 중요합니다. 세상사 모두 그렇지만 적절한 치료가 중요한 치료입니다. 저는 가이드라인을 따를 것을 권합니다. 가이드라인은 Spigelman stage 3까지는 치료 없이 경과관찰을 하는 것입니다. 물론 investigational 치료도 고려할 수 있지만 합병증 발생률이 너무 높아서 걱정입니다.
[2026-7-6] Facebook에서 이런 자료를 보았습니다.
![]() [References]
[References]
1) EndoTODAY familial adenomatous polyposis (FAP) 가족성선종성용종증
2) EndoTODAY 위 용종 Gastric polyp
3) EndoTODAY 위저선 용종과 위저선 용종증 Fundic gland polyp and fundic gland polyposis
4) [종설] Upper gastrointestinal lesions in patients with FAP (최이령, 이준행)
5) 용종증 폴립증후군 polyposis syndrome - 내시경세미나 강의록. 임종필. PDF 0.7M
6) [EndoATLAS] 전형적인 single fundic gland polyp의 내시경 소견
7) [EndoATLAS] Duodenal adenomas and fundic gland polyposis in FAP
8) Prevalence and endoscopic treatment outcomes of upper GI neoplasms in FAP Surg Endosc. 2022
9) MUTYH 관련 폴립증 MUTYH associated polyposis (2023년 8월 내시경학회 교육자료)
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.