 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [일원내시경교실 목요점심집담회 2016-2-4]
[일원내시경교실 목요점심집담회 2016-2-4]
![]() 1. 위암 life cycle
1. 위암 life cycle
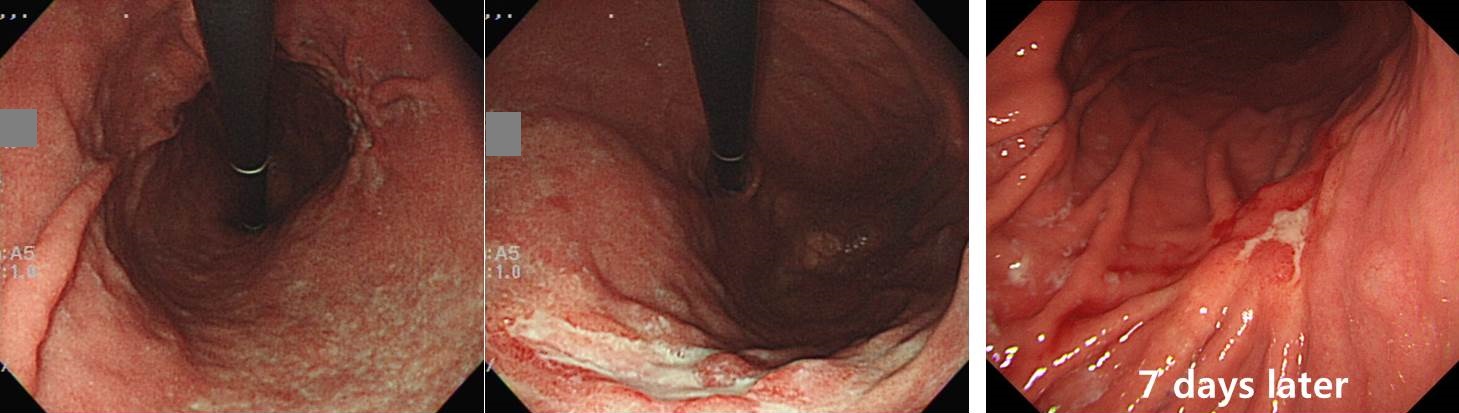
의뢰 전 내시경 검사와 의뢰 후 내시경 검사에서 모양이 사뭇 다른 경우가 있습니다. 이유는 대강 3가지 입니다. (1) 위암 진단 후부터 약을 복용하는 사람이 많습니다. (2) 조직검사 후 모양이 변형될 수 있습니다. (3) 위암은 life cycle이 있습니다.
Stomach, total gastrectomy:
Advanced gastric carcinoma
1. Location : middle third, Center at mid body and posterior wall
2. Gross type : Borrmann type 3
3. Histologic type : tubular adenocarcinoma, poorly differentiated
4. Histologic type by Lauren : diffuse
5. Size : 3.8x2.4 cm
6. Depth of invasion : invades serosa (pT4a)
7. Resection margin: free from carcinoma, safety margin: proximal 4 cm, distal 11.8 cm
8. Lymph node metastasis : no metastasis in 78 regional lymph nodes (pN0)
9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : present
12. Peritoneal cytology : negative
13. AJCC stage by 7th edition: pT4a N0
![]() 2. Mucinous adenocarcinoma
2. Mucinous adenocarcinoma

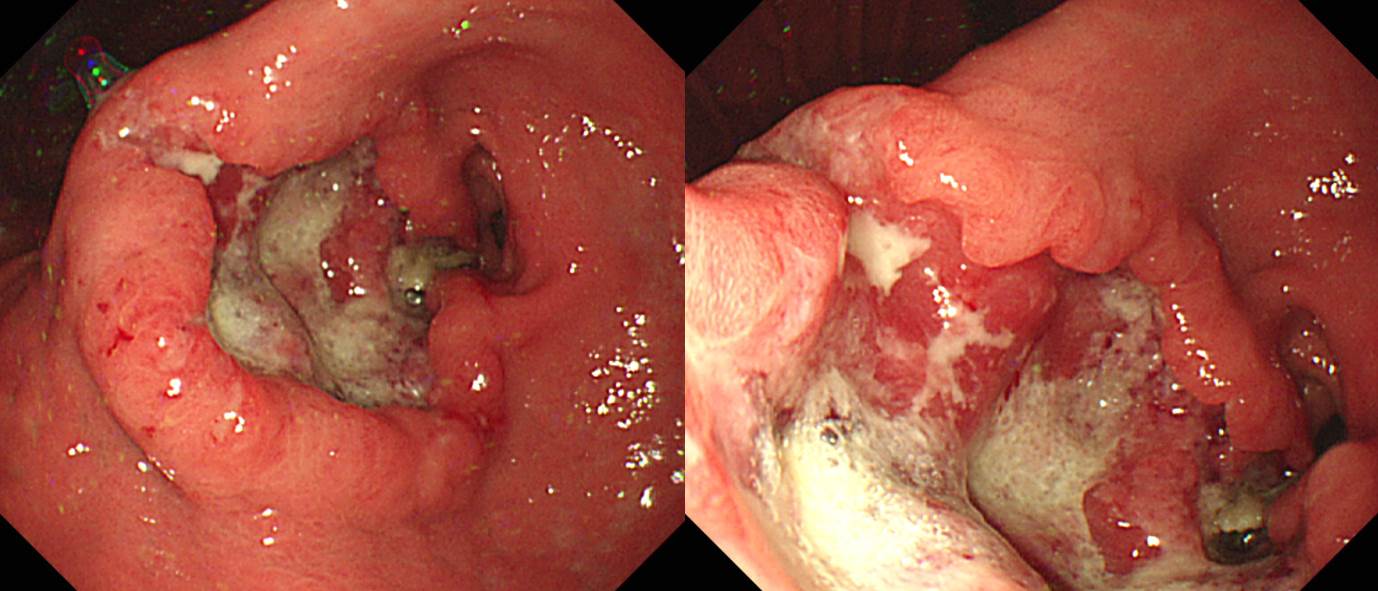
보만 2형일까요 혹은 보만 1형일까요? 고민되는 증례입니다. 보통 2형으로 부르는 것 같습니다.
Stomach, radical subtotal gastrectomy:
Advanced gastric carcinoma
1. Location : lower third, Center at lower body and anterior wall
2. Gross type : Borrmann type 2
3. Histologic type : mucinous adenocarcinoma (mucin production: 60%) with signet ring cell feature
4. Histologic type by Lauren : diffuse
5. Size : 4x4 cm
6. Depth of invasion : penetrates subserosal connective tissue (pT3)
7. Resection margin: free from carcinoma, safety margin: proximal 3.5 cm, distal 3.5 cm
8. Lymph node metastasis : no metastasis in 39 regional lymph nodes (pN0)
9. Lymphatic invasion : present
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. AJCC stage by 7th edition: T3 N0
![]() 3. Poorly differentiated neuroendocrine carcinoma
3. Poorly differentiated neuroendocrine carcinoma
수술 전 조직검사로 정확히 진단하기 어려운 종류입니다.
Stomach, subtotal gastrectomy:
Poorly-differentiated neuroendocrine carcinoma (G3)
1. Name of Procedure: Organ resection
2. Site of Tumor: Stomach (Antrum)
3. Diagnosis: Neuroendocrine carcinoma (G3)
4. WHO classification(2010): Poorly differentiated neuroendocrine carcinoma, large cell type
5. Multiplicity: Single
6. Size: 6x6 cm
7. Extent: Serosa
8. Grading: Mitotic Count(/10HPF): >20 (about 60/10 HPF)
9. Immunohistochemical Stains:
1) Synaptophysin : Positive
2) Chromogranin A: Negative
3) OPTIONAL : CD56 (+)
10. Lymphovascular invasion: present
11. Perineural invasion: present
12. Lymph node metastasis: [Number of positive nodes/Total number of nodes(7/32)
13. Resection Margins: Negative,Safety margin : proximal 3.5 cm, distal 3 cm
14. Other Pathologic Components: Presence of tumor necrosis (60 %)
![]() 4. Signet ring cell carcinoma of the rectum
4. Signet ring cell carcinoma of the rectum

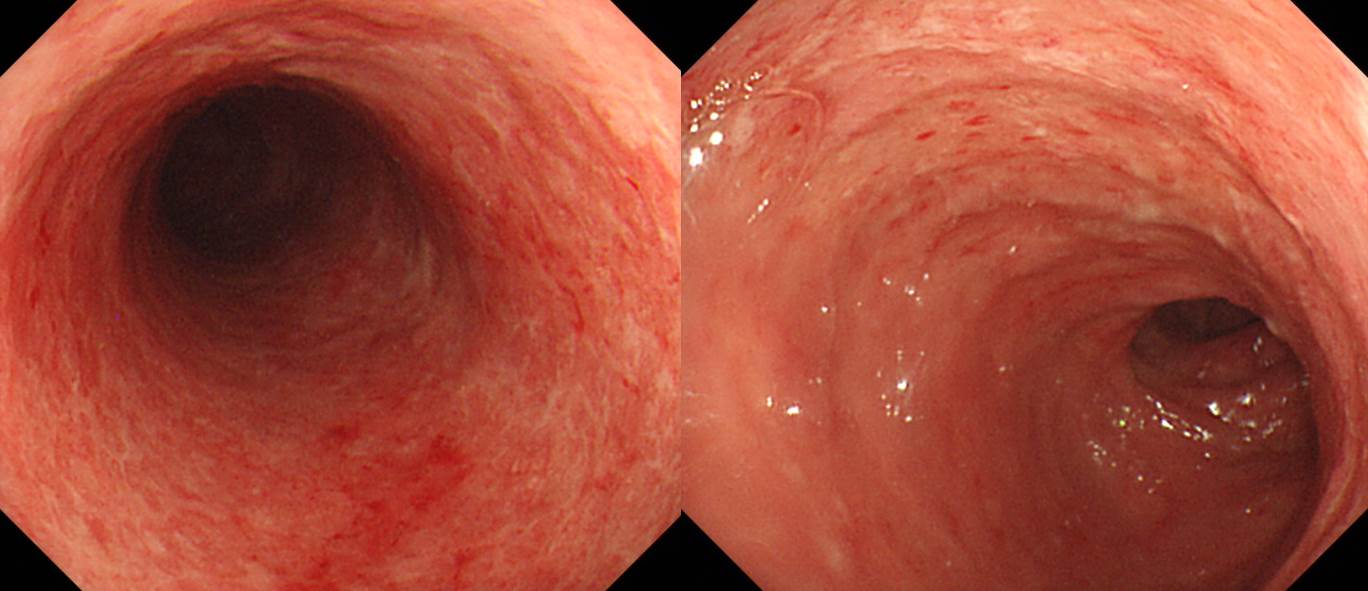
잔변감을 주소로 대장내시경을 한 환자입니다. 대장내시경에서 soft, nodular, submucosal lesion들이 upper rectum에서 발견되어 submucosal tumor나 infiltrative disease를 감별하였는데 조직검사에서 signet ring cell carcinoma with lymphatic spaces, either primary or metastatic의 결과였습니다. Staging work up에서 LN, soft tissue, bone metastasis가 있어 FolFIRI 복합항암치료 시작하였습니다.
![]() 5. Eosinophilic colitis
5. Eosinophilic colitis
CBC에서 WBC 18,660 (eosinophil 44.4%), 직장과 대장 조직검사에서 focal colitis with eosinophilic infiltration으로 나와 eosinophilic colitis로 진단하였습니다.
Primary eosinophilic gastrointestinal disorders (EGIDs) represent a spectrum of inflammatory gastrointestinal disorders in which eosinophils infiltrate the gut in the absence of known causes for such tissue eosinophilia.
EGIDs can be subgrouped as eosinophilic esophagitis (EE), eosinophilic gastroenteritis (EG), and eosinophilic colitis (EC). The least frequent manifestation of EGIDs is EC. EC is a heterogeneous entity with a bimodal age distribution, presenting with either an acute self-limited bloody diarrhea in otherwise healthy infants or as a more chronic relapsing colitis in young adults.
The pathophysiology of primary EC appears related to altered hypersensitivity, principally as a food allergy in infants and T lymphocyte-mediated (i.e. non-IgE associated) in young adults. In adults, symptoms include diarrhea, abdominal pain, and weight loss. Endoscopic changes are generally modest, featuring edema and patchy granularity. Although standardized criteria are not yet established, the diagnosis of EC depends on histopathology that identifies an excess of eosinophils. Therapeutic approaches are based on case reports and small case series, as prospective randomized controlled trials are lacking. Eosinophilic colitis in infants is a rather benign, frequently food-related entity and dietary elimination of the aggressor often resolves the disorder within days. Adolescent or older patients require more aggressive medical management including: glucocorticoids, anti-histamines, leukotriene receptors antagonists as well as novel approaches employing biologics that target interleukin-5 (IL-5) and IgE.
참고문헌: Eosinophilic colitis: epidemiology, clinical features, and current management. Therap Adv Gastroenterol. 2011 Sep;4(5):301-9
© 일원내시경교실 바른내시경연구소 이준행