EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Ectopic pancreas. 이소성췌장] - 終
[Ectopic pancreas. 이소성췌장] - 終
1. Introduction
2. Endoscopic findings - 위체하부 소만 SMT 양상의 ectopic pancreas
3. Ectopic pancreas of the cardia
4. Endoscopic treatment of ectopic pancrea
5. Small bowel ectopic pancreas 소장 이소성 췌장
6. Role of MRI in the evaluation of ectopic pancrea MRI의 역할
7. FAQ
8. References
![]() 1. Introduction
1. Introduction
1) Location of heterotopic pancreas
- According to the analysis of 431 published cases
- 30.5% in the duodenum, 26.5% in the stomach, 16.5% in the jejunum, 5.8% in the ileum, 5.3% in the Meckel's diverticulum.
- 95% of heterotopic pancreatic lesions found in the stomach
- located in the pylorus or in the antrum GC within 5 to 6 cm from the pylorus
esophagus, cystic duplicates of ileum, mesentery, omentum, colon, gall bladder, cystic duct and choledochus, spleen, liver, lymph nodes, urinary bladder, lungs and Fallopian tubes.
2) Predominantly intramural masses
- 75% are submucosa, and the other are intramuscular or subserosal.
3) The macroscopic appearance of heterotopic pancreas is a benign-appearing firm submucosal mass on a broad basis, sharply circumscribed from the surrounding tissue. The distinguishing feature of heterotopic pancreas is the central umbilication representing probably a rudimentary excretory duct (present in less than 50 % of cases).
4) The size of heterotopic pancreas may vary from microscopic to few centimetres.
5) 위의 ectopic pancreas는 위내시경 조직검사로 확인되는 경우도 있고 확인되지 않는 경우도 있습니다.
6) Acini는 없고 duct만 있는 경우는 adenomyoma라고 불리기도 합니다.
Distal antrum의 mass로 내원하셨습니다. Submucosal tumor 양상이고 중앙이 다소 함몰되어 있었습니다. 조직검사를 하였고 ectopic pancreas로 확인되었습니다.
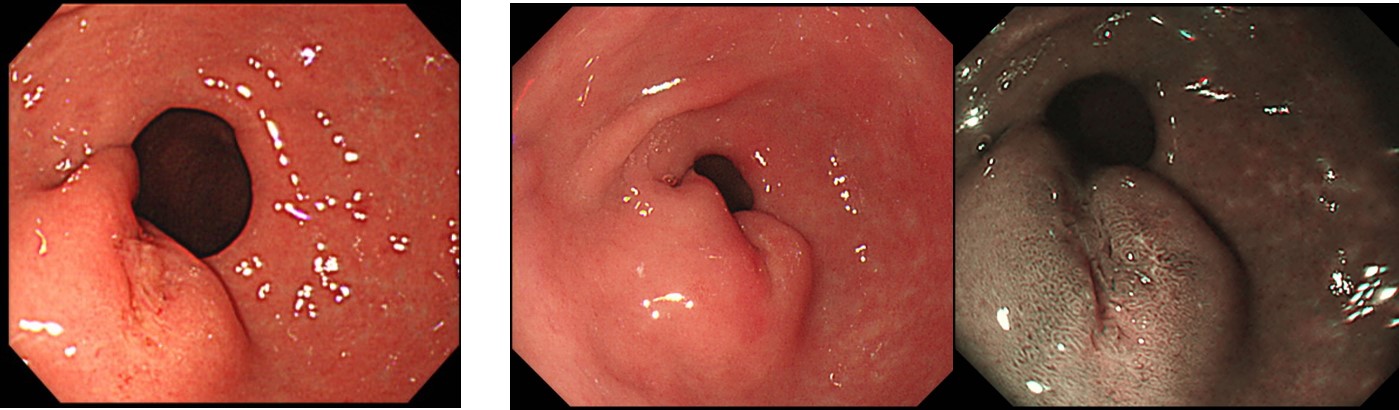
왼쪽 조각에는 점막하층에, 우측 조각에는 점막층에 pancreas 조직이 보입니다.
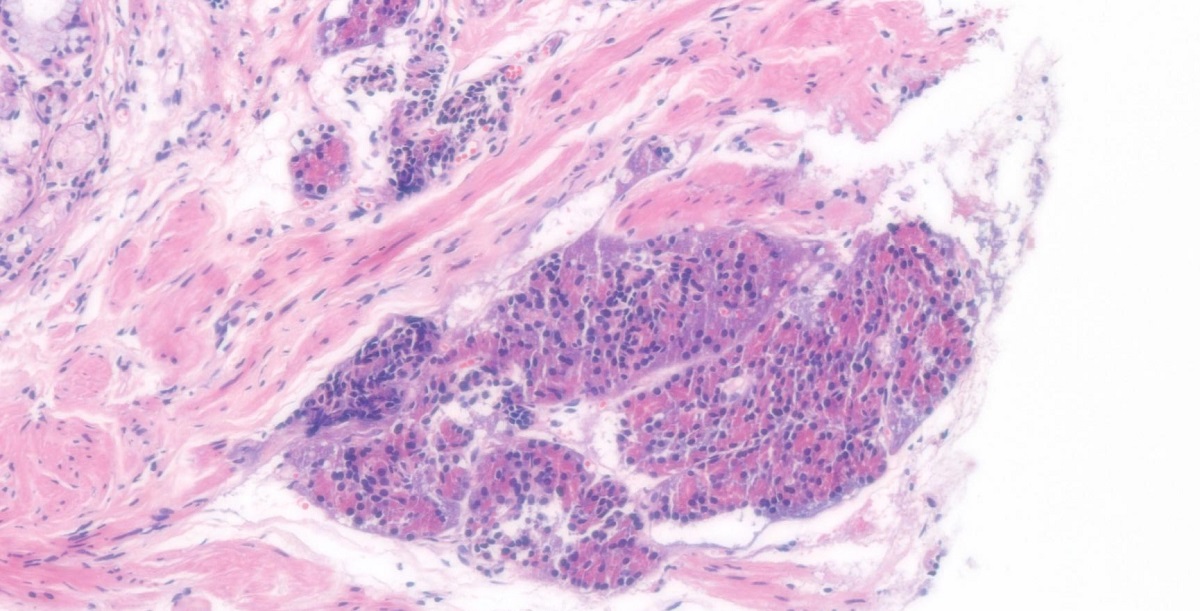
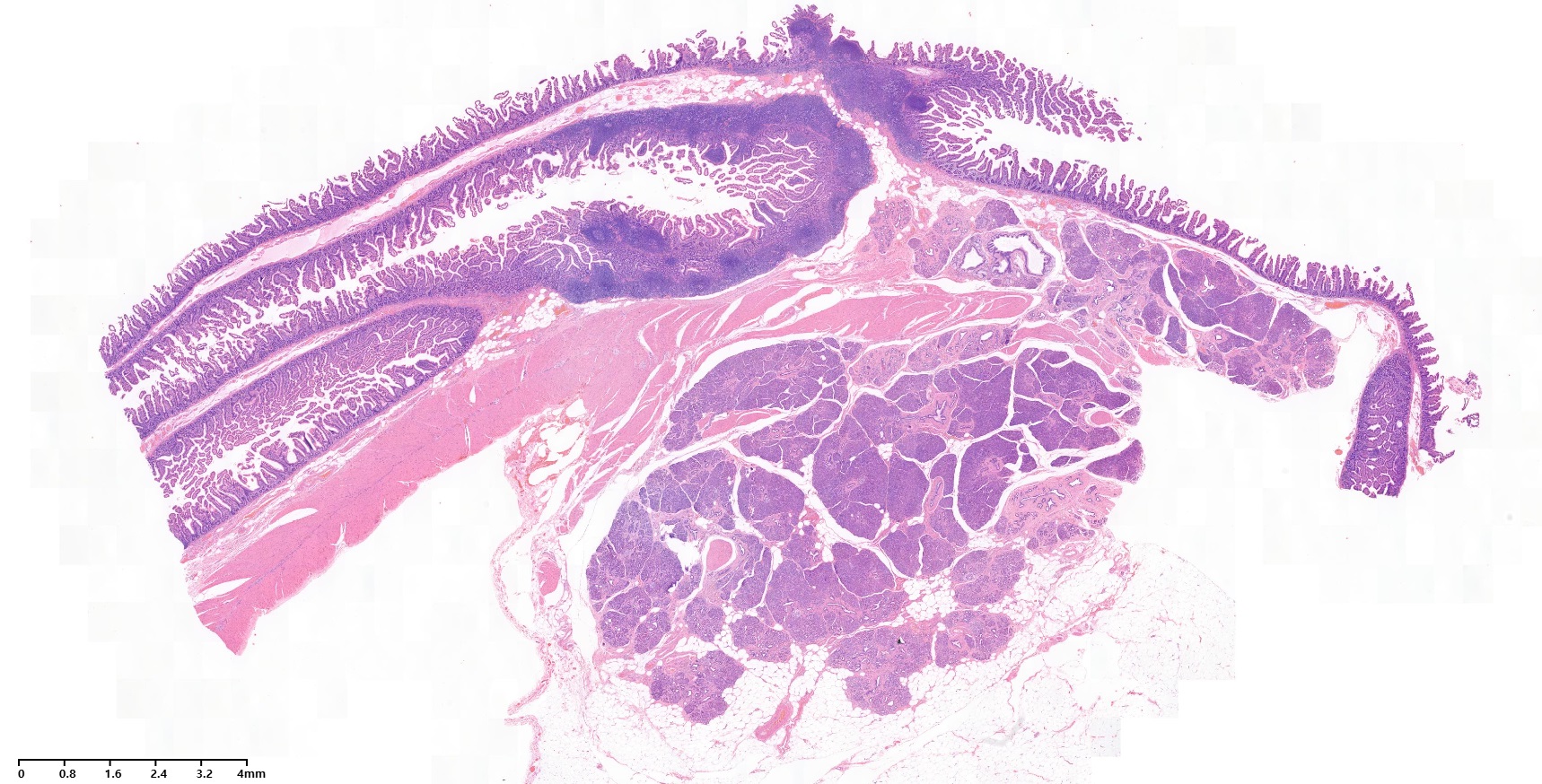
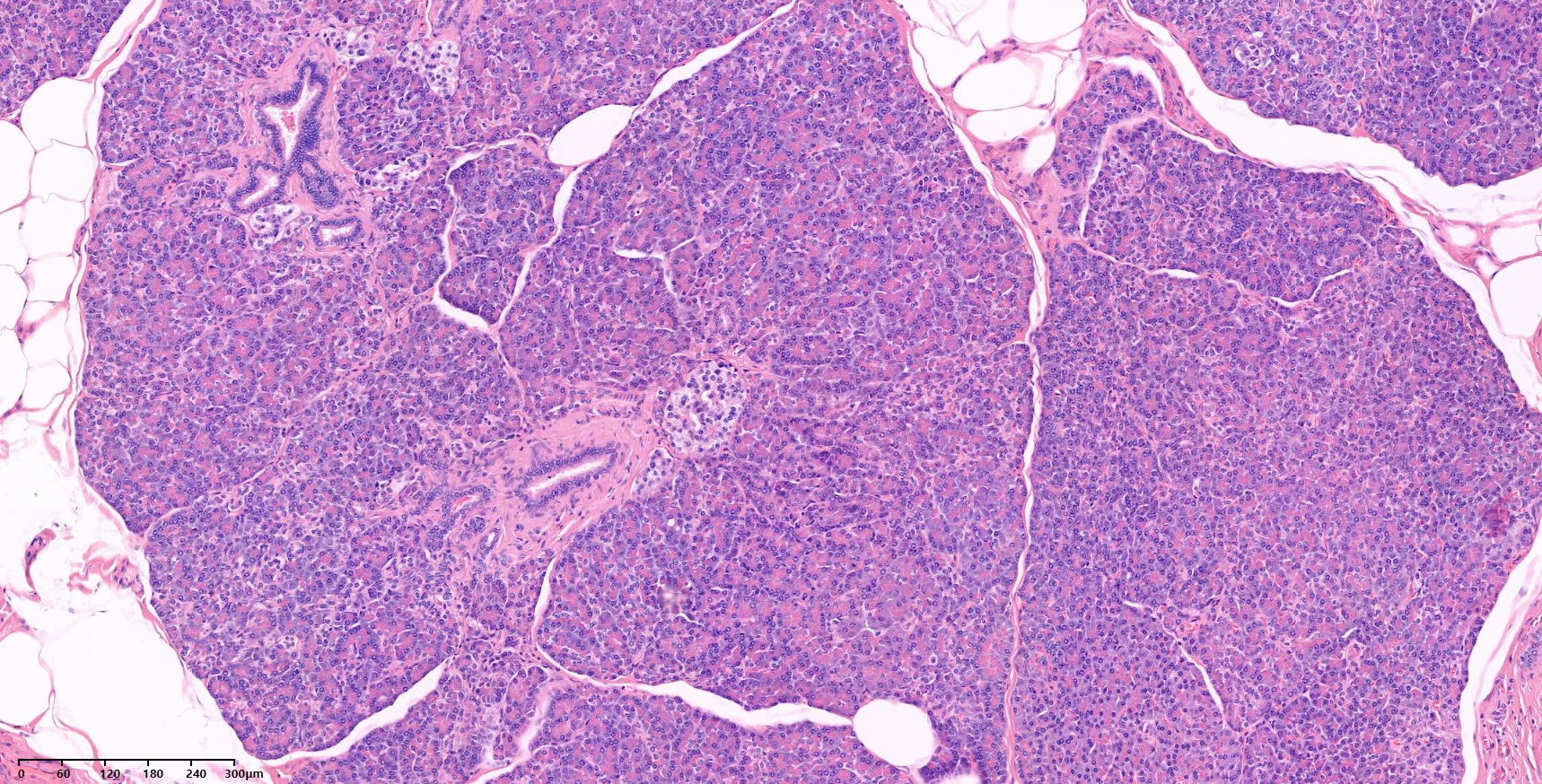
위체하부 후벽의 점막하종양으로 wedge resection을 하여 ectopic pancreas로 확인하였습니다.
Deep submucosal layer와 근육층 사이에 pancreas 조직이 보입니다.
일부 superficial submucosal layer나 deep mucosal layer에 췌장 조직이 보이기는 하지만 (검은 화살표) 내시경 조직검사에서 이 부위를 targeting 할 수는 없습니다. 아주 어쩌다 우연히 나오는 경우가 있을 뿐입니다.
Singapore Med J 2014의 설명을 옮깁니다.
Ectopic or heterotopic pancreas is a relatively rare finding, with a reported incidence of 0.55% - 13.70% at autopsy. The stomach, duodenum and the proximal jejunum are the most common sites. Other less commonly reported sites in the gastrointestinal tract are the ileum, Meckel’s diverticulum, oesophagus, colon, mesentery and omentum. Ectopic pancreatic tissue has also been reported in the liver, gallbladder, spleen, common bile duct, retroperitoneum, umbilicus, lymph nodes, and in extra-abdominal locations such as the lungs and mediastinum.
By four to five weeks of gestation, the pancreas is formed by the ventral and dorsal buds of the endodermal lining of the duodenum. The dorsal bud grows more rapidly than the ventral bud. The dorsal bud forms the upper part of the head, body and tail of the pancreas, while the ventral bud forms the lower part of the head and uncinate process. The ventral bud rotates toward the dorsal bud and finally fuses with the dorsal bud. During the process of rotation, the ventral and dorsal buds of the pancreas are in close proximity to the stomach and duodenum. This may result in the incorporation of pancreatic primordial germ cells into the bowel loops, which may potentially develop into pancreatic tissue later on. Rarely, one of the buds may get detached and carried along the long axis of the bowel, thus explaining the site of ectopic pancreas remote from the normal anatomical location. Another theory of the origin of ectopic pancreas is the differentiation of totipotent endodermal cells into pancreatic tissue in the intestinal tract, as well as in extra-abdominal locations. This may explain the presence of pancreatic tissue in the lungs, mediastinum and retroperitoneum.
Ectopic pancreas can be classified according to the Heinrich classification. Type I ectopic pancreas contains all the elements of normal pancreatic tissue such as acini, ducts and islet cells. Type II contains pancreatic acini and ducts without islet cells, while only pancreatic ducts are seen in Type III.
Most cases of ectopic pancreas are incidentally diagnosed during gastroduodenoscopy, EUS or CT performed for other reasons, as in our case. However, patients with ectopic pancreas may be affected by the inflammatory or neoplastic process, similar to a normal pancreas. Patients with ectopic pancreas may present with complications such as bleeding, stricture, ulceration, pancreatitis, pseudocyst and malignant transformation. Most ectopic pancreas measure less than 2 cm in size, but can also be as large as 5 cm. Ectopic pancreas occurring in the gastrointestinal tract is usually seen in the submucosal layer, making it difficult to differentiate from gastrointestinal stromal tumour (GIST).
![]() 2. Endoscopic findings. 내시경 소견
2. Endoscopic findings. 내시경 소견
한 애독자가 보내주신 사진
내시경 조직검사로 확인된 ectopic pancreas
내시경 조직검사로 확인된 ectopic pancreas
7년간 경과관찰 중 변화가 없었음. Ectopic pancreas로 추정
Stomach, subtotal gastrectomy: early gastric carcinoma
1. Location : lower third, center at antrum and lesser curvature
2. Gross type : EGC type IIa+IIc
3. Histologic type : tubular adenocarcinoma, poorly differentiated
4. Histologic type by Lauren : intestinal
5. Size : 0.9x0.8x0.3 cm
6. Depth of invasion : extension to submucosa (sm3) (pT1b)
7. Resection margin: free from carcinoma, safety margin: proximal, 4.6 cm; distal, 3.5 cm
8. Lymph node metastasis : no metastasis
9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : not identified
Heterotopic pancreas in the prepyloric antrum of anterior wall
![]() [위체하부 소만 SMT 양상의 ectopic pancreas]
[위체하부 소만 SMT 양상의 ectopic pancreas]
위체하부 소만, 특히 약간 후벽쪽은 췌장과 매우 가깝습니다. 그래서인지 이 부위에 SMT 양상의 ectopic pancreas를 종종 만납니다. 전정부 대만 ectopic pancreas와 달리 umbilicated된 소견은 거의 없습니다. 종종 bridging fold를 동반합니다. Stomach MRI를 찍으면 췌장과 signal이 유사하므로 감별진단에 크게 도움된다고 하지만 비보험이라 검사가 쉽지 않습니다. 수술하는 예가 많습니다만, 감별진단이 잘 되면 수술하지 않고 지낼 수 있으니 얼마나 좋은 일입니까?
수술(wedge resection)로 확인된 ectopic pancreas
수술(wedge resection)로 확인된 ectopic pancreas
수술(wedge resection)로 확인된 ectopic pancreas
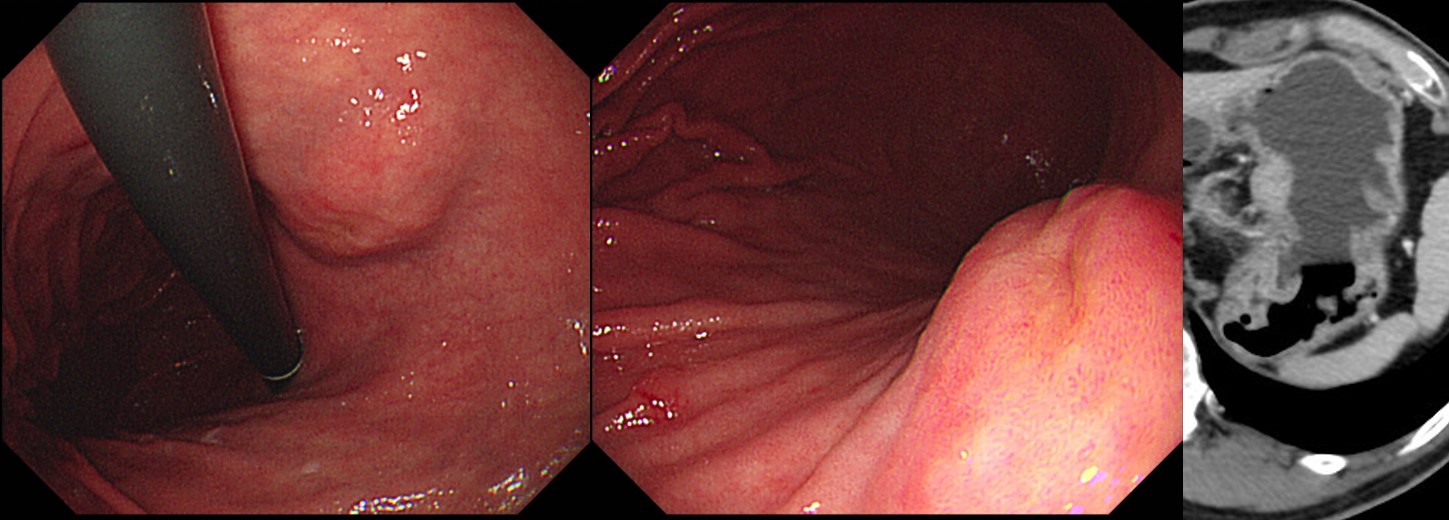
수술(wedge resection)로 확인된 ectopic pancreas. 병소가 작아서 수술하지 말고 경과관찰 할 것을 권했으나 환자가 수술을 원하심. 타 의료기관에서 병소가 커졌다고 들은 상황에서는 경과관찰을 권하더라도 결국 수술을 선택하는 환자가 많음.
수술(wedge resection)로 확인된 ectopic pancreas. 전 의료기관에서 수술을 권유받고 오신 분입니다. 내시경과 CT 소견 등 고려하여 경과관찰을 권하였으나 환자는 수술받기를 원하셨습니다. 예상하였던 ectopic pancreas가 나왔습니다. 한번 수술 이야기를 들으면 경과관찰을 추천해도 여간해서는 수술을 잊지 못하는 것이 환자들 마음 같습니다. 최종 치료방침 결정 전 좀 더 고민하는 태도가 필요합니다.
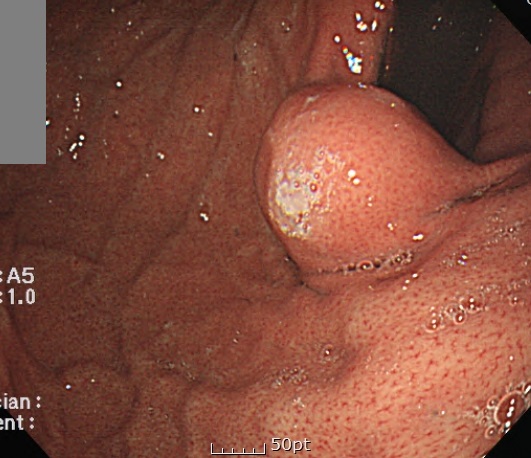
위각 직상방 SMT인데 duct opening 같은 구조가 보이며 조직검사에서 ectopic pancreas로 확인되었습니다.
![]() 3. Cardia의 이소성 췌장
3. Cardia의 이소성 췌장
[2015-11-11. 애독자 증례 편지 11]
30대 남자 외국인 노동자이고 귀국 전 건강검진을 하다가 cardia SMT가 발견되어 의뢰되셨습니다.
보통 이 정도는 F/U을 하면서 크기 변화를 보는데 자기 나라로 가면 F/U이 안 된답니다. 저는 pancreatobiliary EUS영역이 아닌 gastric SMT는 EUS-FNA를 자주 하지는 않고 있습니다. FNAB에서 GIST가 나왔는데 작다고 수술을 하지 않고 지켜보는 건 좀 이상해서 입니다. 아예 뭔지 모르고 추정하는 게 좋지, 조직학적으로 확진되면 작더라도 해결을 해야 된다는 것이 제 생각입니다. 그래서 2cm 이하면 그냥 F/U을 하고, 2cm 이상 3cm이하면 나이가 젊으면 수술적 치료를 고려하고 나이가 많을 경우 3cm까지는 지켜봅니다. 젊은 사람에서 수술을 적극적으로 고려하는 이유는 SMT수술은 wedge resection으로 충분하고 위험성이 그렇게 높지 않기 때문입니다. 하지만 cardia SMT는 좀 예외라서 EUS-FNA을 가끔 하기도 합니다. 이 환자의 경우 외국으로 나갈 예정이고 본인이 적극적으로 진단하기를 원하고 GIST가능성이 있다면 수술까지 받고 싶다고 하였습니다. EUS-FNA를 시행하였습니다.

조직검사상 ectopic pancreas가 나와 환자는 happy하게 자기 나라로 갔습니다. Hollow를 전공하시는 고수 선생님들은 굳이 EUS-FNA를 시행하지도 않고 ectopic pancreas를 맞추실 수 있지 않았을까 생각도 듭니다. 전 자신이 없어어 EUS-FNA를 시행하였습니다.
[2015-11-11. 이준행 답장]
매우 적절한 판단이었다고 생각합니다. 제가 'hollow를 전공하는 고수'에 낄 수 있는지 생각해 봅니다. 사실 cardia의 ectopic pancreas는 처음 보았거든요. 전정부의 전형적 병소를 제외하고는 복잡한 검사 없이 ectopic pancreas를 쉽게 진단하기는 쉽지 않습니다. 최근 삼성서울병원 민병훈 교수 주도로 gastric SET에 대한 EUS-FNA 한 결과가 논문으로 나와 소개합니다 (Lee M. Medicine (Baltimore) 2015).
[2017-6-3. 이준행 추가]
2017년 6월 3일 IDEN에서 성모병원 조유경 교수님께서 비슷한 증례를 보여주셨습니다.

![]() 4. Endoscopic treatments. 내시경 치료
4. Endoscopic treatments. 내시경 치료
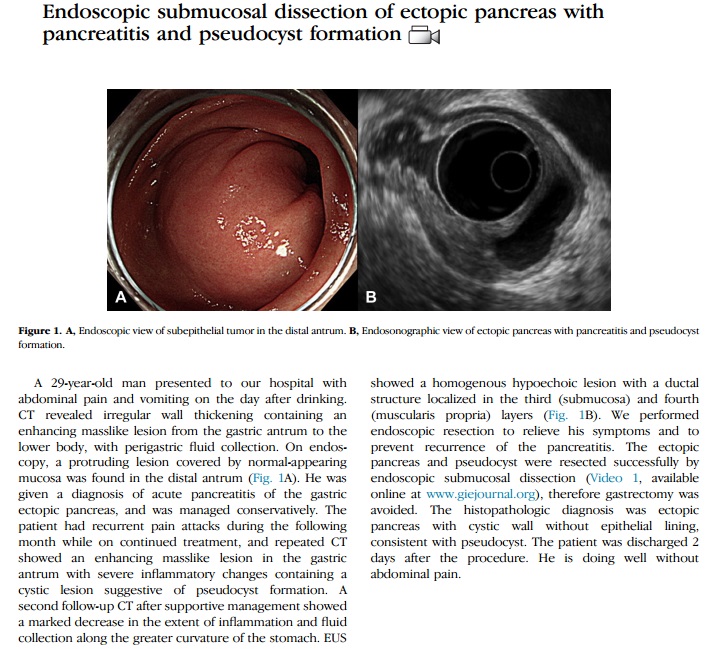
2015년 12월 Gastrointestinal Endoscopy 지에 아산병원 내과 공은정 선생님께서 ESD로 치료한 complicated ectopic pancreas 증례를 발표하였습니다 (Gong EJ. GIE 2015). 위 전정부의 ectopic pancreas 였는데, pancreatitis와 cyst formation이 병발하였다고 합니다. 학회지에 접속하면 멋진 동영상을 볼 수 있습니다. 멋진 증례보고 축하합니다.
[2013-7-7. 애독자(H대 교수)의 증례]
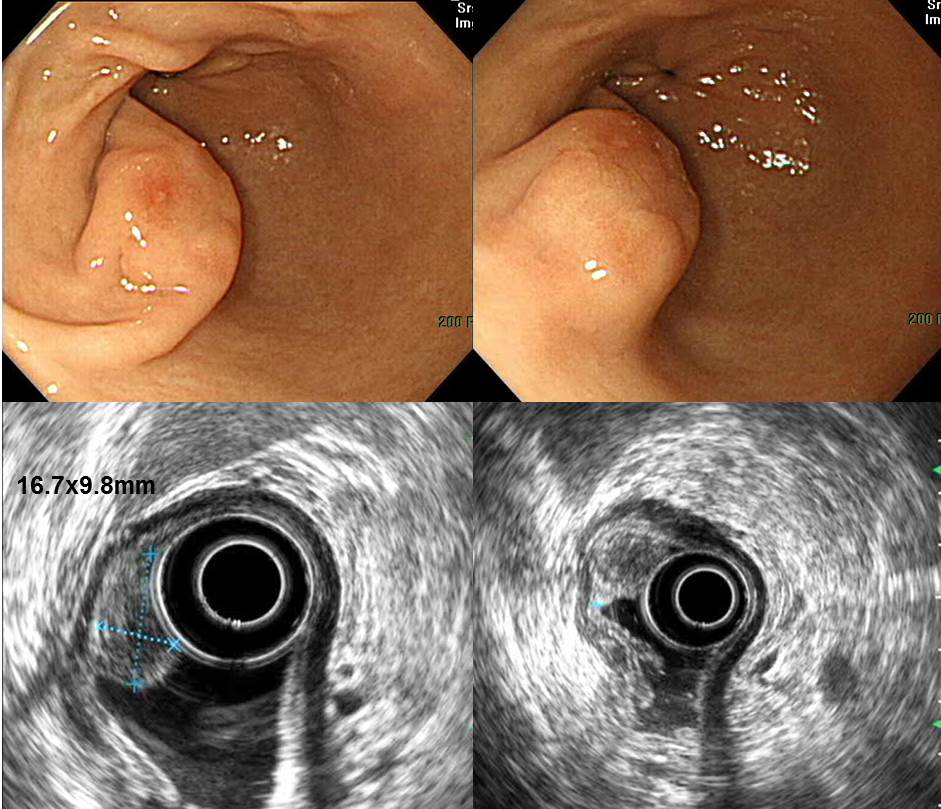
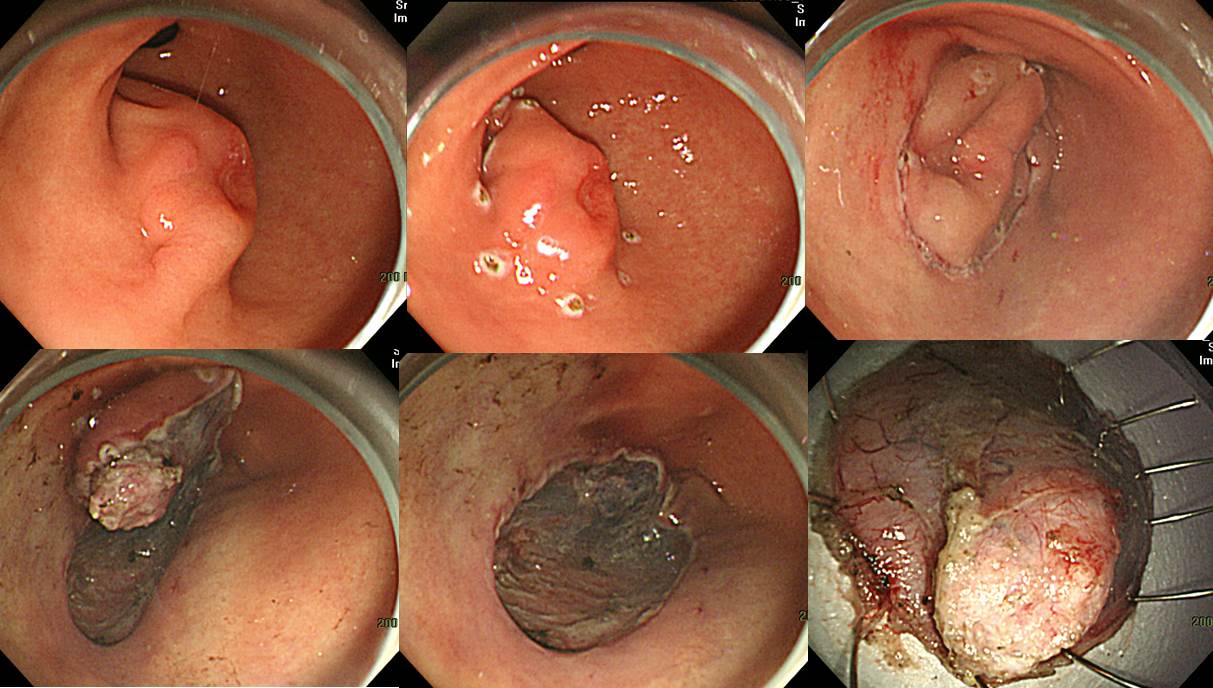
최근 SMT로 추적관찰(3rd layer에 heterogenous hypoechoic lesion에 기인하는 mass였음)하는 중, 6개월 후 내시경 검사에서 SMT 중심부에 궤양이 발생하여 malignant GIST를 배제하기 위해 ESD를 시행하였고 ectopic pancreas로 진단된 증례가 있어 메일을 드립니다.
첫 work dup
추적관찰 중 궤양이 발생하여 ESD 시행
[2013-7-9. 이준행 의견]
좋은 증례 감사합니다. Ectopic pancrea ESD는 주변 조직과 adhesion이 심해 시술이 어려운 것으로 소문이 자자한데, 본 증례에서는 깔끔하게 잘 된 것 같습니다. 수고 많으셨습니다. 좋은 증례 공유해 주셔서 감사합니다.
![]() 5. Small bowel ectopic pancreas. 소장 이소성 췌장
5. Small bowel ectopic pancreas. 소장 이소성 췌장
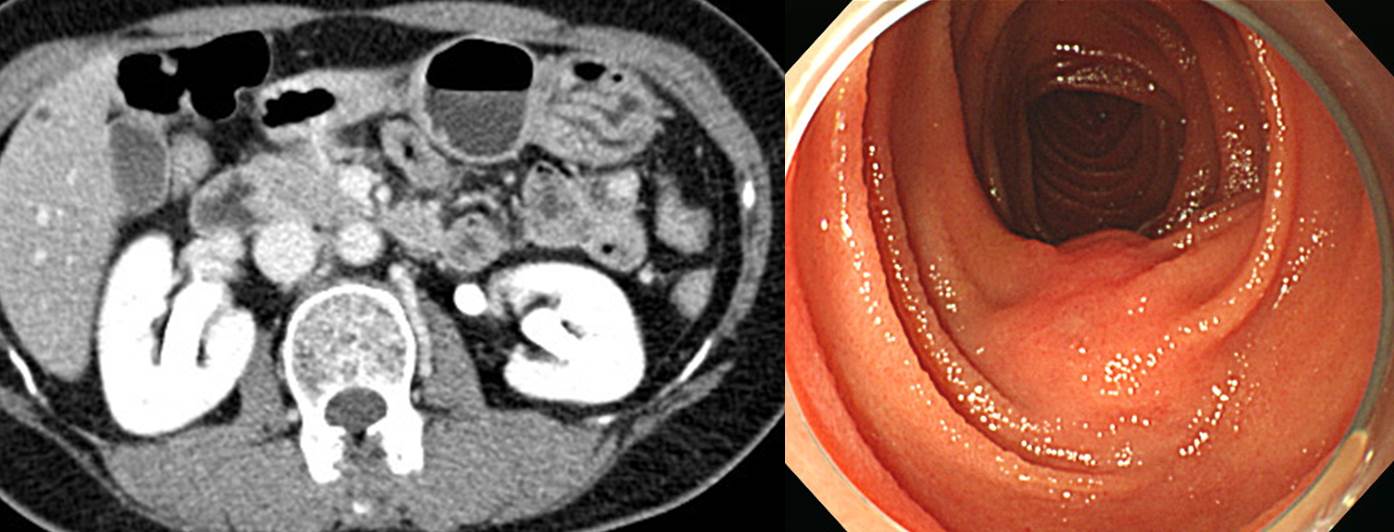
건진내시경에서 발견된 십이지장 병소입니다. 조직검사에서 pancreatic tissue가 관찰되었습니다.
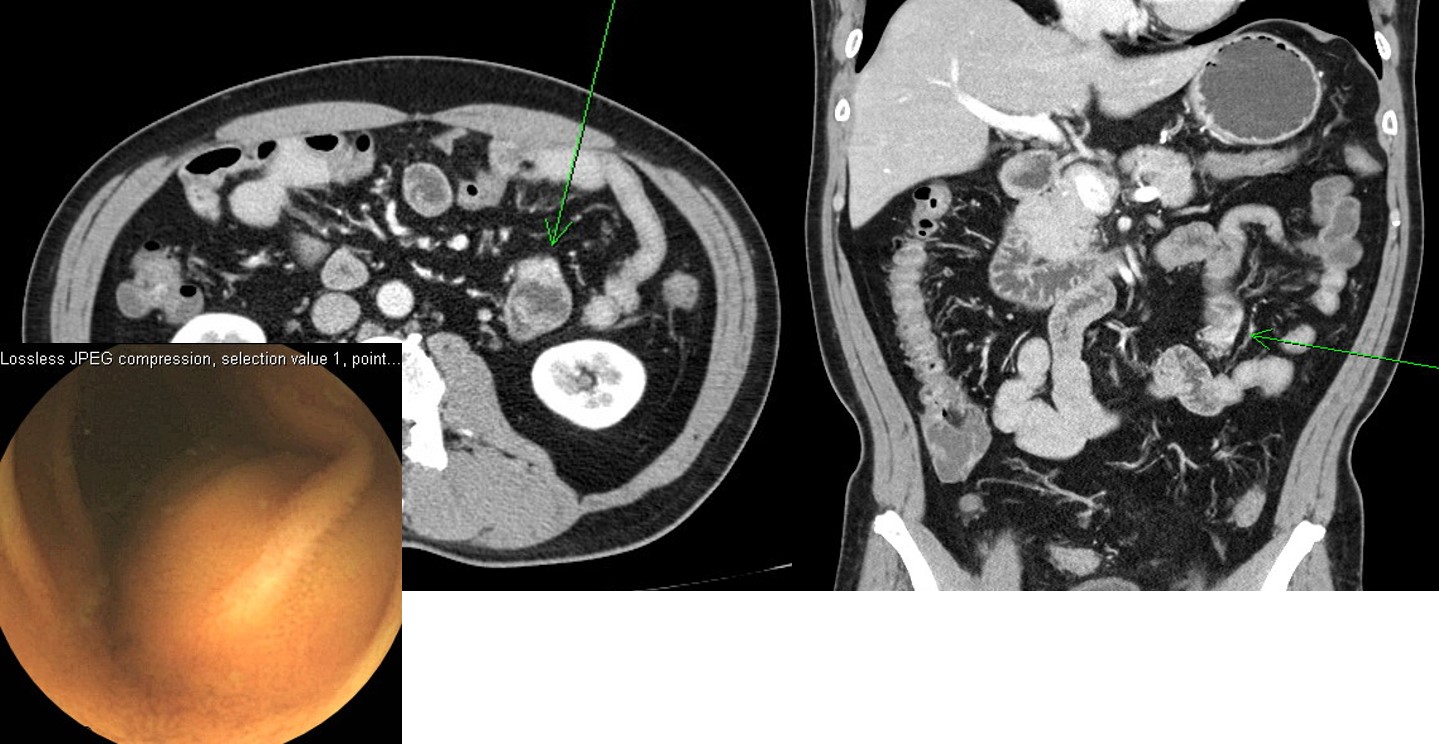
위 질환으로 시행한 CT에서 우연히 발견된 소장 병소입니다. 위 수술을 하면서 소장도 resection을 하였습니다. Ectopic pancreas였습니다.
우연히 발견된 소장 종양이었습니다. CT 판독은 "proximal jejunum에 delayed phase에서 잘 관찰되는 nodule이 있는데 subepithelial tumor의 가능성이 있음. Pancreas와는 dynamic enhancement pattern이 달라 GIST 또는 NET 등의 tumorous condition으로 판단함."이었고 소장내시경 조직검사는 "focal glandulomuscular proliferation"였습니다
최종 결론은 소장의 ectopic pancreas였습니다.
![]() 6. Role of MRI in the evaluation of ectopic pancreas. MRI의 역할
6. Role of MRI in the evaluation of ectopic pancreas. MRI의 역할
위의 ectopic pancreas는 MRI로 평가할 수 있습니다 (보험 규정이 문제입니다. 과거에는 인정비급여였는데 2020년에는 1회에 한해 진단 목적 MRI가 보험이 된다는 소문은 있으나 공문을 받은 것이 없어서 매우 애매합니다). 내시경 소견이 ectopic pancreas에 합당한 환자에서 pancreas MRI를 찍어보면 sequence에서 위점막하종양과 pancreas의 signal intensity가 같으면 거의 확실하게 ectopic pancreas임을 추정할 수 있습니다.
여자 42세 (2018)
CT: Gastric prepyloric antrum GC side에 약 2.7 cm의 outer wall based lesion이 의심됨. 인접한 duodenal bulb로의 extension도 있음. 위치 및 모양을 고려하였을 때 GIST보다는 ectopic pancreas의 가능성이 더 고려되고 이러한 경우 pancreas MRI를 시행하면 pancreas와 signal intensity를 비교하여 GIST와 ectopic pancreas 간의 감별이 가능함.
MRI: Stomach CT에서 지적한 prepyloric antrum에 2.7 cm 크기의 길쭉한 모습의 submucosal tumor로 보이는 병변은 크기에서 변화가 없는 모습임. 조영증강 양상이나 signal intensity가 pancreas와 같아 지난 CT에서 언급한 바와 같은 ectopic pancreas의 가능성이 가장 크겠음.
![]() [FAQ]
[FAQ]
[2014-9-13. 애독자 질문]
안녕하십니까? EndoTODAY를 사랑하는 독자입니다. 저는 췌담도를 전공하고 있습니다. 위 점막하종양은 볼록한 형태입니다. 그런데 이소성 췌장은 왜 umbilication이 있을까요? 찾아본 저널에는 아래와 같은 내용이 있었습니다. 물렁물렁한 lipoma도 빵빵한 찐빵 같은 모양인데 왜 ectopic pancreas는 umbilication이 있을까요?
The macroscopic appearance of heterotopic pancreas is a benign-appearing firm submucosal mass on a broad basis, sharply circumscribed from the surrounding tissue. The distinguishing feature of heterotopic pancreas is the central umbilication representing probably a rudimentary excretory duct (present in less than 50 % of cases).
[2014-9-14. 이준행 답변]
좋은 질문인데 저는 답을 모르겠습니다. 일부 ectopic pancreas는 외분비 기능이 있어 duct opening이 위치한 가운데 부위가 움푹 꺼진 것 아닐까 추정할 뿐입니다. 그런데 항상 umbilication이 있는 것도 아닙니다. 내시경 치료 혹은 수술로 확인한 ectopic pancreas는 대부분 umbilication이 없었습니다 (Umbilication이 없기 때문에 감별진단을 위하여 내시경 치료 혹은 수술을 했다고 보는 것이 맞습니다).
이소성췌장(ectopic pancreas = heterotopic pancreas)은 드물지 않습니다. 다만 진단이 어려울 뿐입니다. EUS는 specificity가 만족스럽지 못합니다. EMR/ESD는 어렵고 출혈도 흔합니다 (사실 저는 한번도 경험이 없습니다). 최근에는 endoscopic tunnel resection으로 조직을 확인하기도 합니다 (2014년 IDEN에서 고려대 박종재 선생님께서 live demonstration을 하셨습니다). 현실적으로는 대부분 경과관찰을 하고, 영 찜찜하면 수술(wedge resection)을 보내고 있습니다.
결국 환자와 의사의 철학에 달려있습니다. 100%를 원하면 일이 어려워집니다. 암이 아니라는 것, malignant potential을 가진 GIST가 아니라는 것을 100% 보장해달라고 요구하면 의사의 선택권이 매우 제한됩니다. 어떻게든 잘라내는 수 밖에 없습니다. 물론 합병증 위험이 따릅니다. 비용도 문제고, 삶의 질도 문제입니다. 애써 치료한 후 불필요한 치료였다는 논란이 일 수도 있습니다. 결국 100% 확실하게 해 달라면 경과관찰을 못하고 절제술을 하는 수 밖에 없고 그에 따른 위험성은 환자 몫입니다. 그러니 어렵습니다. 철학적 문제입니다.
[2016-4-25. 애독자 질문]
교수님 ?안녕하십니까? 진정 내시경 검사할 때마다 엔도투데이 강의를 생각하면서 조심 조심하고 있습니다. 내시경을 안전하게 할 수 있게 해주셔서 감사합니다.
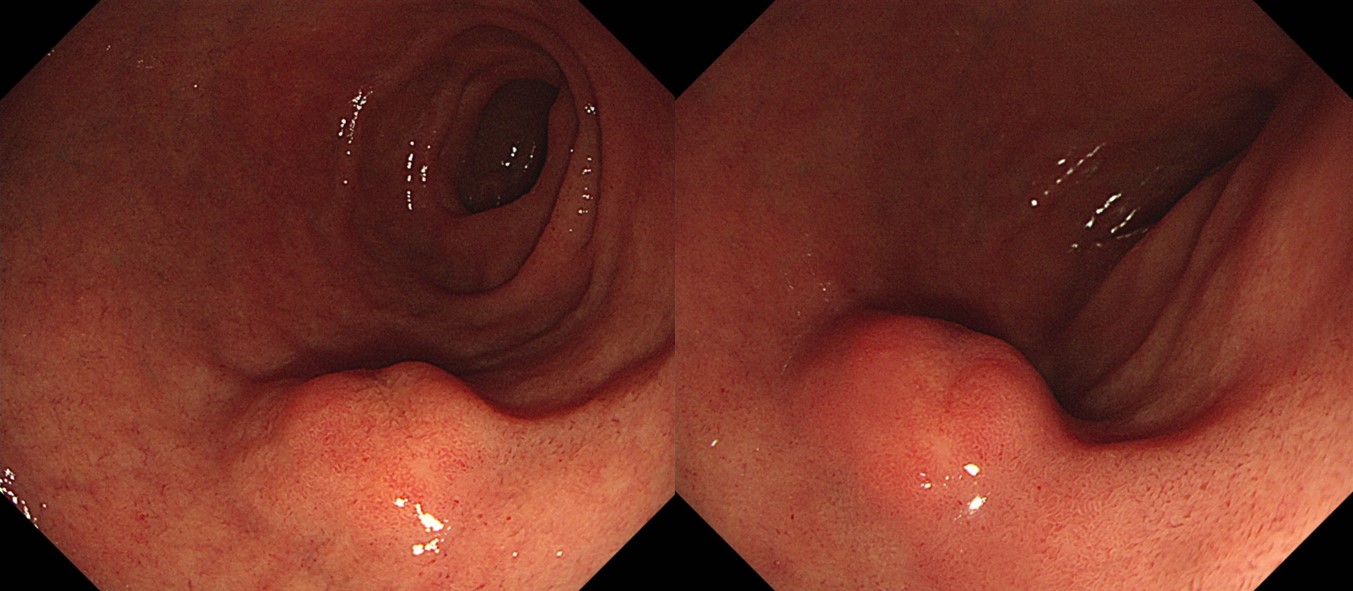
아래 사진들은 30대 초반 남자 검진 환자입니다. Congenital mucosal deformity 인지, ectopic pancreas 인지 문의드립니다. SMT 처럼 불룩 튀어나오지 않고 편평해도 ectopic pancreas로 볼 수 있는지요?
그리고, 환자가 이런 이소성췌장도 기능을 하는지 저에게 물어보았는데, 사실 저도 잘 모르는 문제였습니다. 이소성 췌장도 기능을 하는지요?
[2016-4-26. 이준행 답변]
예. 기능을 할 수 있습니다. 이소성 췌장도 가끔 췌장염을 일으키는 경우까지 있습니다. 아래 증례보고를 보시기 바랍니다 .
Pancreatitis of ectopic pancreatic tissue: a rare cause of gastric outlet obstruction
![]() [References]
[References]
1) Heterotopic pancreas at Pathology Outlines
2) Normal histology of pancreas
3) 미란성 위염 혹은 이소성 췌장? 만성위염 내시경진단 006
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.