EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [IDEN 2017]
[IDEN 2017]
Day 1 | Day 2 | Day 3 | 이준행 강의
일시: 2017년 6월 2일 - 4일
장소: 그랜드힐튼 호텔
내시경학회가 열리는 같은 날 같은 장소에서 식품의약품안전평가원 등에서 '규제과학'에 대한 심포지엄을 열고 있었습니다. 제목이 '4차 산업혁명과 헬스케어 규제과학 심포지엄'이었는데요... 저는 규제보다는 자율로 가는 것이 4차 산업혁명의 핵심이라고 생각하고 있었는데 정부에서 일하는 분들은 저와 정반대로 생각하는 모양입니다. 그런데...... 규제도 과학인가요?

2017년 6월 3일 IDEN 올림푸스 부스에서 대장내시경 모델을 발견했습니다.
![]() 1. Young endoscopist forum (6월 2일 금요일 오전)
1. Young endoscopist forum (6월 2일 금요일 오전)
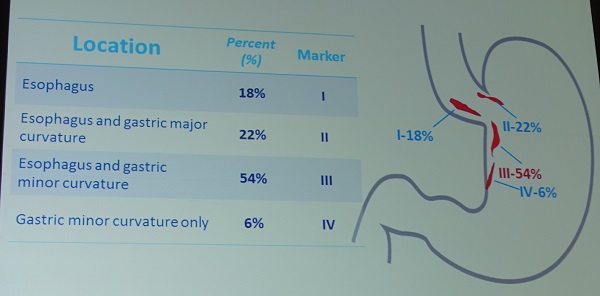
[몽고 Ariunzul Dashdondog] Mallory Weiss tear에 대한 발표가 있었습니다. Tear의 위치에 대한 분석이 흥미로웠습니다.
* 참고: EndoTODAY Mallory-Weiss tear
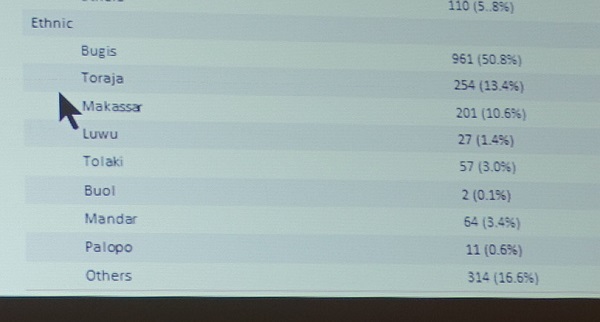
인도네시아 South Sulawesi 지역 Makasaar 市 Hasanuddin 대학의 Rini Bachtiar 선생이 대장내시경에 대하여 발표하였는데, demographics table의 ethnics라는 부분이 흥미로웠습니다. 어느 부족에 속하는지 기록을 남기는 모양입니다.
베트남의 Pham Chau는 상품화된 endoloop가 아닌 self-made endoloop를 사용하여 출혈없이 용종을 절제할 수 있었다고 발표하였습니다.
Trichobezoar에 대한 흥미로운 증례 포스터가 있었습니다.
![]() 2. International school for career university (6월 2일 오전)
2. International school for career university (6월 2일 오전)
1) Successful life as therapeutic endoscopist (Seiichiro Abe, National Cancer Center, Tokyo, Japan. seabe@ncc.go.jp)
일본 의사답게 자신의 나이가 40이고 1976년생이라고 말하면서 강의를 시작했습니다. 두 가지 hurdle을 언급했습니다. (1) advanced therapeutic endoscopy (2) submission and presentation in English.
자신의 첫 ESD (위체부 소만의 경계가 불분명한 큰 IIa lesion이었음) 사진을 보여주었는데 3 pm에 시술을 시작하여 다음 날 2 am에 시술이 끝났습니다.
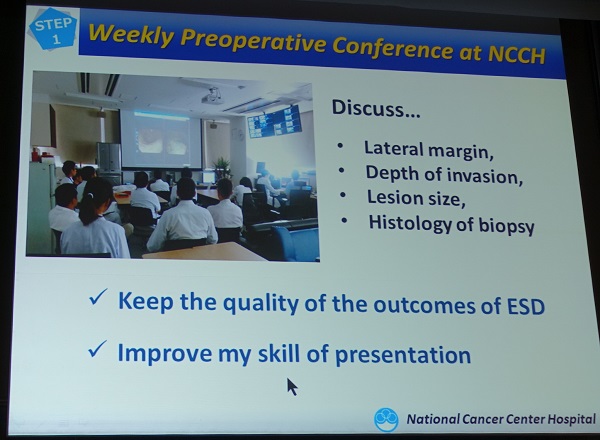
Weekly preoperative conference at NCCH 슬라이드가 가장 부러운 부분이었습니다. 매주 금요일에 surgeon과 함께 다음 주 시술할 ESD 환자를 리뷰하는데, 외국인도 많이 참여하기 때문에 - 매년 100명 정도의 외국인 내시경 의사가 방문 - 영어로 진행된다고 합니다. 사실 2004년 제가 NCCH를 방문했을 때에도 같은 방식이었는데 아직까지 계속되고 있는 모양입니다.
2) How to accelerate your manuscript publications (함기백)
어항 속의 작은 붕어(koi)가 강에서는 큰 물고기로 자라는 것처럼 의사도 큰 물에서 활동해야 한다는 comment로 강의를 시작하셨습니다.
Clinical Endoscopy를 소개해 주셨는데 현재 impact factor는 1.063입니다. 74% 정도는 한국 논문 기타는 해외 논문입니다.
3) Avoiding instant rejection (Hilary Hamilton-Gibbs. Managing editor of Endoscopy)
You never get a second chance to make a first impression.
i) Is my title optimal?
ii) What about my cover letter?
iii) Is my abstact optimal?
iv) Is my manuscipt well formatted?
![]() 3. International hands-on course (EUS, ESD, IEE), sponsored by Olympus-AP (6월 2일 금요일 오후)
3. International hands-on course (EUS, ESD, IEE), sponsored by Olympus-AP (6월 2일 금요일 오후)
1) ESD (Tutor: Seichiro Abe, 정대영, 최기도, 정현수)
준비에 고생이 많으셨던 김상균 교수님과 함께.



2) EUS
3) EIS - magnifying endoscopy with NBI, EMRC and clip, EMRP and clip
![]() 4. Live demonstration (6월 3일 토요일 오전)
4. Live demonstration (6월 3일 토요일 오전)
1) EGC (고려대 안안병원) - 간경변 환자의 전정부 전벽의 IIa+IIc lesion이었습니다. 290 내시경을 이용하여 NBI를 켠 상태에서 Near Focus로 병소를 관찰한 후 marking 부터 시술을 시작했습니다.
이용찬: Hyaluronic acid를 사용할 때 smoke가 더 많이 발생하는 것 같습니다. Transparent hood를 사용하면 traction ESD를 할 필요가 없습니다.
Fujishiro: Margin은 differentiated histology에는 3 mm, undifferentiated histology에서는 5 mm 이상 margin을 확보해야 합니다. Marking 전에 NBI magnification을 이용하여 상세히 관찰해야 합니다. 일본에서는 ESD에 대한 전체 가격이 정해져 있으므로 여러 knife를 사용할 수 있지만, 병원에서는 비용 정책을 고려해야 합니다. 일본에서는 대부분 marking보다 2-3mm 바깥으로 incision을 하는 경우가 많습니다. 병소가 어려운 위치에 있는 경우는 360도 circumferental cutting 보다 일부를 남기는 방식이 좋습니다. 절제 병소가 totally isolation 되는 것보다 일부 당겨지는 부분이 남는 것이 시술이 쉽기 때문입니다.

Lau: 홍콩에서의 가격 정책은 일본과 비슷합니다. 일본에서는 dental floss를 많이 사용합니다.
남: 현재 보험 급여 문제로 hyaluronic acid를 사용할 수 없고 하나의 knife만 써야 합니다.
2) POEM in a patient with esophageal diverticulum (시술자: Philip Chiu, Hong Kong University)

전신마취하에 positive pressure ventilation을 한 상태에서 CO2, TT knife, Spray coagulation를 이용하였습니다.
2016년 윤영훈 교수님 발표자료 중
G-POEM이 gastric paresis에서 사용될 수 있지만 아직 홍콩에서의 경험은 부족하다고 합니다.
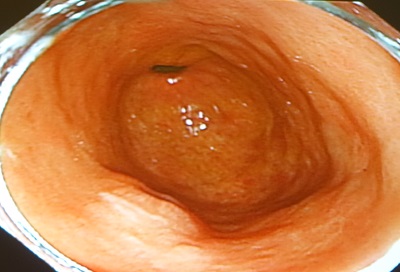
3) Colon ESD (시술자: 서울아산병원 변정식)
아산병원 변정식 교수님께서 distal sigmoid colon에 위치한 nodular mixed type LST를 standard Dual knife를 이용하여 멋지게 시술하셨습니다. 차분하게 시술하는 모습이 인상적이었고 너무 멋졌습니다. 변정식 교수님은 역시 대단한 분입니다. BEST of the BEST라고 생각합니다.
Pocket creation method (PCM)에 대한 논의가 있었습니다. 특히 병소가 큰 경우에 PCM가 유용하다고 합니다.
Matsuzaki I. Gastrointest Endosc 2017
Submucosal dissection이 80% 이상 진행된 상태에서 중력에 의하여 병소의 뒤쪽이 잘 보이지 않았는데 변정식 교수님의 환자의 자세를 90도 변경하여 flip이 중력에 의하여 떠오르도록 하였습니다.
Fujishiro: Cicumferential cutting 후 S-O clip 등을 적용하면 시간이 절약됩니다. 그러나 변교수님의 시술의 경우는 traction method를 적용하지 않아도 좋을 것 같습니다.
일본에서는 최근 bipolar ESD knife가 개발되어 적용되고 있다고 합니다 (B-knife, 동경암센터 사이토 선생님). 지금까지의 모든 ESD knife (IT-2 knife, Dual knife, Hook knife)는 monopolar current를 사용하기 때문에 전류가 위장관 벽을 통과하므로 deep injury가 가능합니다. Bipolar current를 사용하면 전류가 local curcuit를 돌기 때문에 deep injury가 발생하지 않는 장점이 있습니다. Abe 선생님은 위에서는 크게 도움되지 않는 것 같지만 대장에서는 적용할 수 있을 것 같다는 의견을 주었습니다.
![]() 5. Unanswered issues in gastric ESD (6월 4일 토요일 오전)
5. Unanswered issues in gastric ESD (6월 4일 토요일 오전)
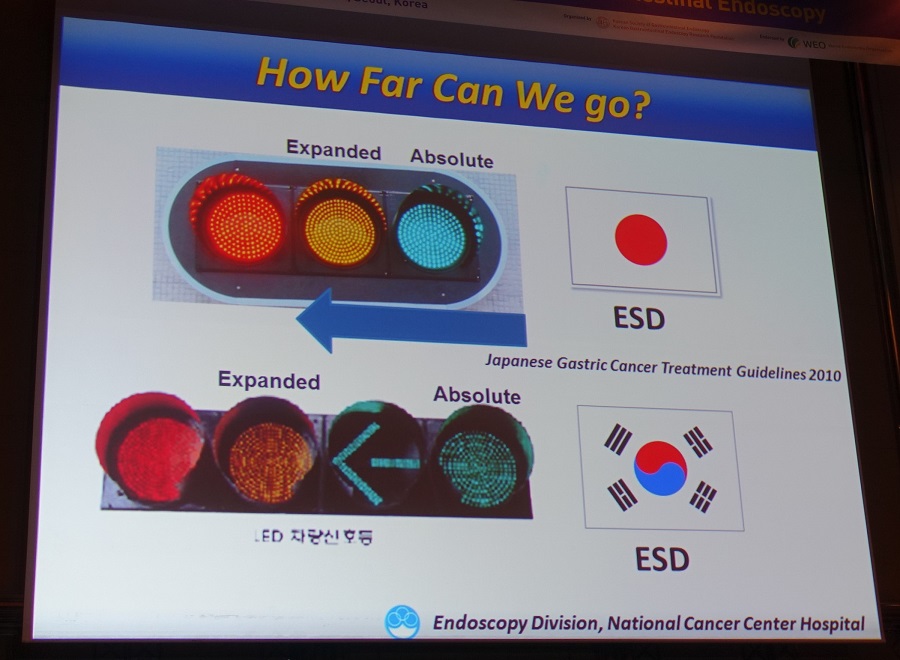
1. Endoscopic management of signet ring cell carcinoma - How far can we go? Seiichiro Abe (National Cancer Center Hospital, Tokyo)
이준행 혼잣말: 이처럼 내시경 소견과 병리 소견을 상세히 분석하는 것이 일본 내시경계의 힘이라고 생각합니다. 다른 어느 나라에서도 이와 같이 할 수 없습니다. 물론 우리나라에서도 못하고 있습니다. 質보다는 量을 추구하는 문화에서는 영원히 불가능한 일입니다.
Tumor size underestimation에 대하여 상세히 설명하셨습니다. Undifferentiated type EGC에서는 NBI magnification를 사용하여도 demarcation line을 정확히 측정할 수 없습니다. "Biopsies taken outside the lesion are essential." 4 quadrant negative biopsy가 꼭 필요하다고 합니다.
일본 의사들에 비하여 한국 의사들이 undifferentiated type으로 적응증을 확장하는데 걱정이 많은 것 같습니다.
지금까지 ESD indication의 적용은 retrospective data에 근거한 것입니다. 일본에서는 최근 두 개의 prospective study를 통하여 근거 확보를 위하여 노력하고 있다고 합니다.
- JCOG1009/1010: Phase II trial of ESD for expanded indication of undifferentiated-type EGC
- J-WEB/EGC: Large prospective cohort (about 10,000 pts) using web registry system
[이준행 혼잣말] Surgical database를 이용한 분석에서도 한일간의 결과가 다르게 나오고 있습니다. 같은 기준 (expanded indication for undifferentiated type EGC)을 적용할 때 일본 surgical data에서는 림프절 전이가 거의 없는 것으로 나오지만 우리나라 surgical data에서는 0.5-2% 정도의 림프절 전이가 있는 것으로 발표되고 있습니다. 예를 들면, 2011년 서울아산병원의 연구(Chung JW. JGH 2011)에 따르면 저자들이 Criteria III로 명명한 'undifferentiated less than 20 mm without ulceration'에서는 통계적으로 유의한 수준의 림프절 전이 위험이 있는 것으로 분석된 바 있습니다 (1.15%, 3/261, 95% CI, 0-2.44%). 저는 병리의사의 눈이 다르기 때문으로 생각합니다. 우리는 우리 데이타에 근거하여 치료하는 것이 맞습니다. 우리의 ESD specimen은 우리의 병리의사가 판독하기 때문입니다. Abe 선생님의 강의를 들었지만, 우리나라에서는 당분간 ESD indication 확장은 조심스럽게 접근해야 한다는 생각이 달라지지 않았습니다. 저는 1 cm 이하의 flat, pale, signet ring cell carcinoma 정도에 대해서는 ESD를 고려할 수 있지만, 이보다 확장하는 것은 시기상조라고 생각하고 있습니다.
* 참고: EndoTODAY Undifferentiated-type 조기위암의 림프절 전이 위험
2. Long-term outcome after curative and non-curative endoscopic resection of early gastric cancer. (연세대학교 박준철)


박준철 교수님의 close follow up이 중요하다고 강조하셨는데, Inoue 좌장께서는 그 방법에 대하여 몇 가지 comment를 하셨습니다. 역시 일본인답게 EUS를 강조하시더군요.
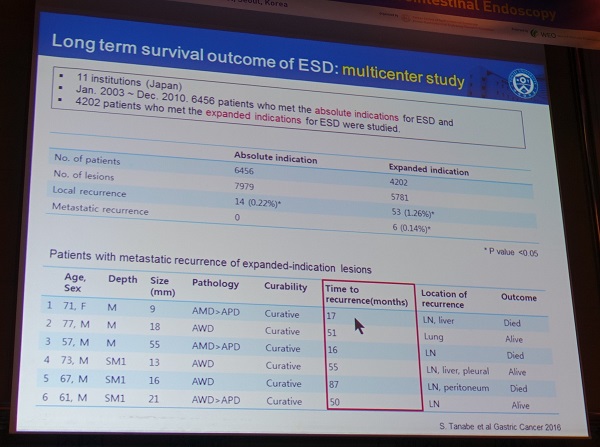
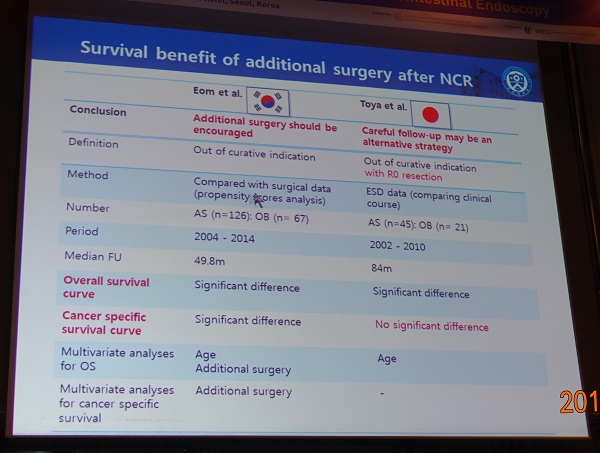
3. Management after non-curative resection based on prognostic model. (Nariya Uedo, Osaka International Cancer Center)
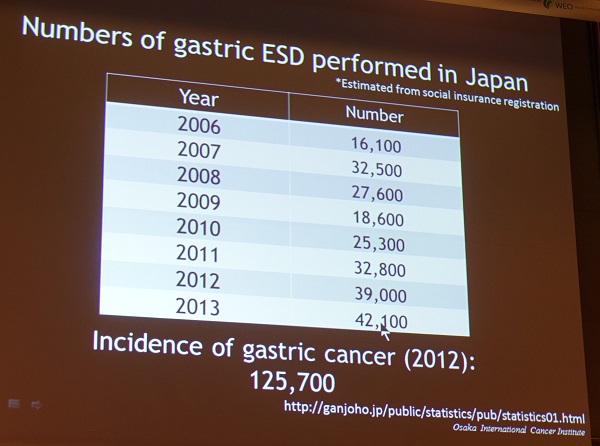

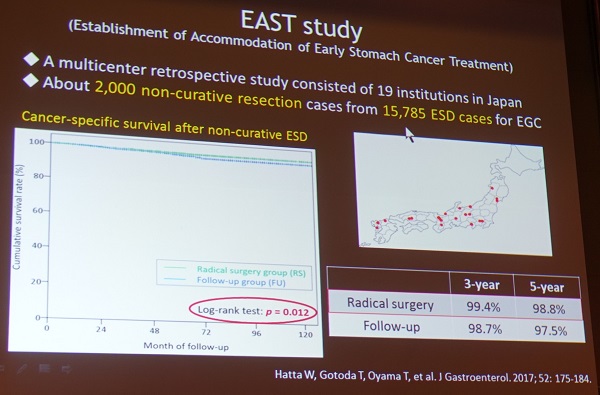
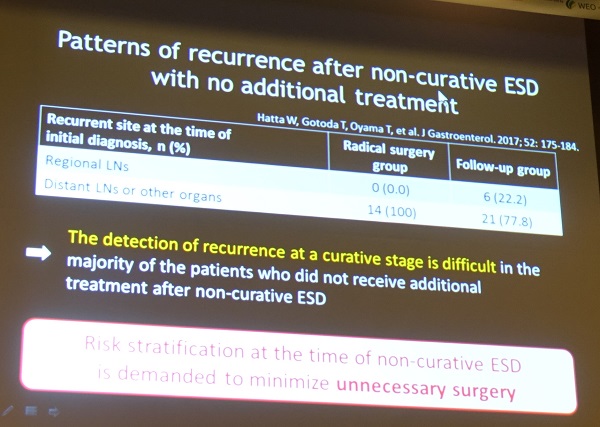
Detection of recurrence at a curative stage is difficult.
Hatta. Am J Gastroenterol 2017
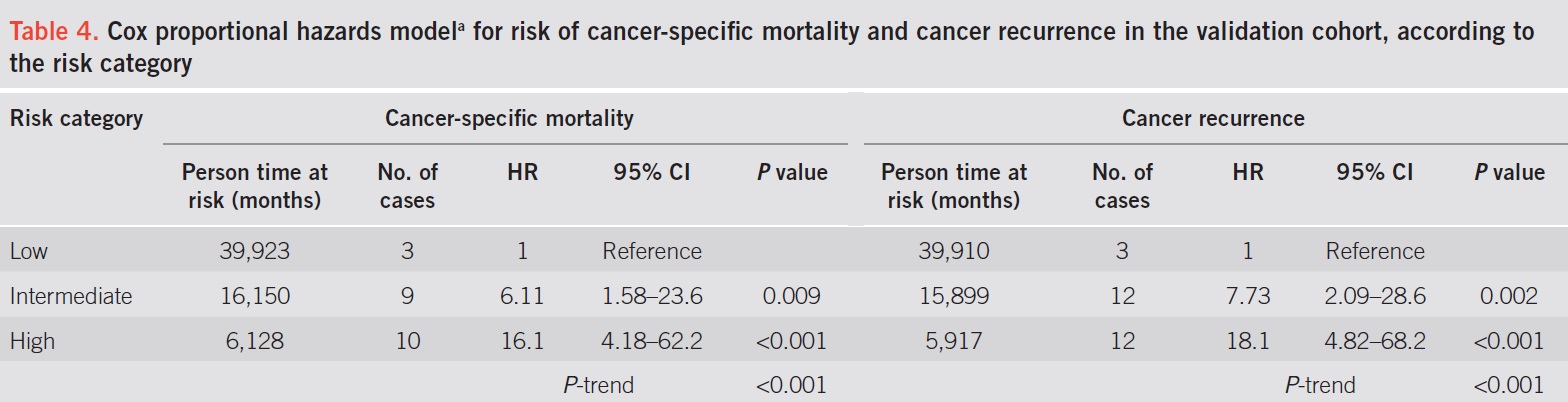
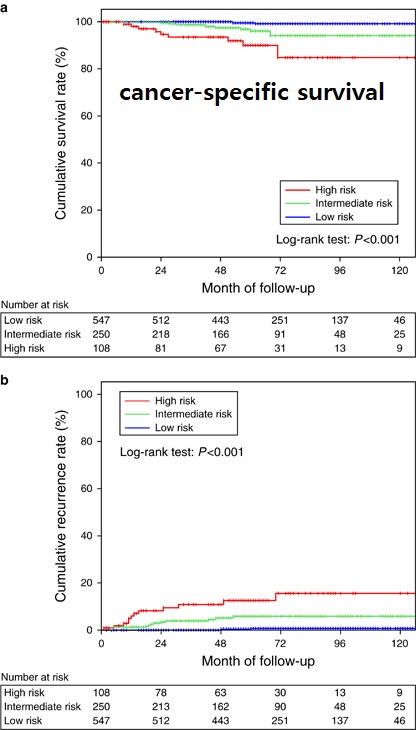

결론 slide가 아주 마음에 들었습니다. 데이타에 근거하고 환자의 상태와 철학에 따라 최종 방침을 결정해야 할 것 같습니다.
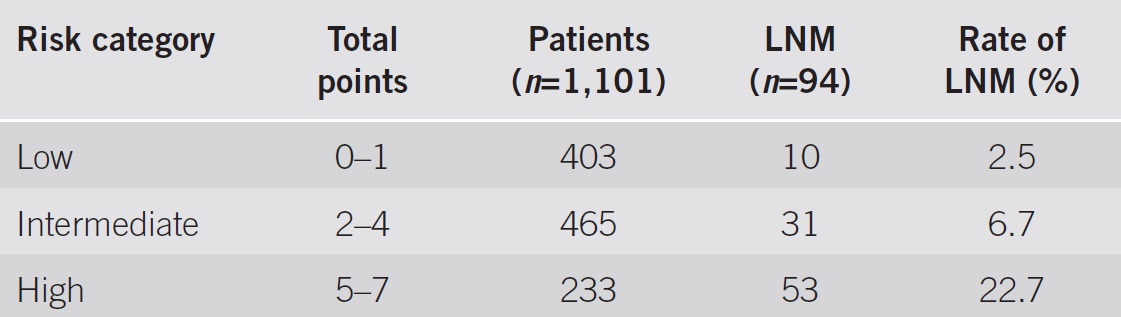
[이준행 질문] In the prognostic model, the score for lymphatic invasion is 3, so it is very important. However, evaluation of lymphatic invasion is difficult and depends on the operator and staining method. Would you tell me the role of immunohistochemical staining for the evaluation of lymphatic invasion?
[Uedo 선생님 답변] eCura prognostic model은 retrospective data이므로 immunohistochemical staining을 하였던 환자도 있고 그렇지 않은 환자도 있습니다. Osaka cancer cancer에서는 submucosal invasion이 있었던 환자에 대해서는 immunochemical staining을 하고 있습니다.
![]() 6. Endoscopic diagnosis of various gastric lesions (6월 3일 토요일 오후)
6. Endoscopic diagnosis of various gastric lesions (6월 3일 토요일 오후)
1. Endoscopic diagnosis of chronic gastritis based on Kyoto system. (Tetsuya Ueo, Oita Red Cross Hospital, Japan)
Red streak는 Hp 음성에서 보이는 소견인 반면, spotty redness는 Hp 양성에서 보이는 소견입니다.

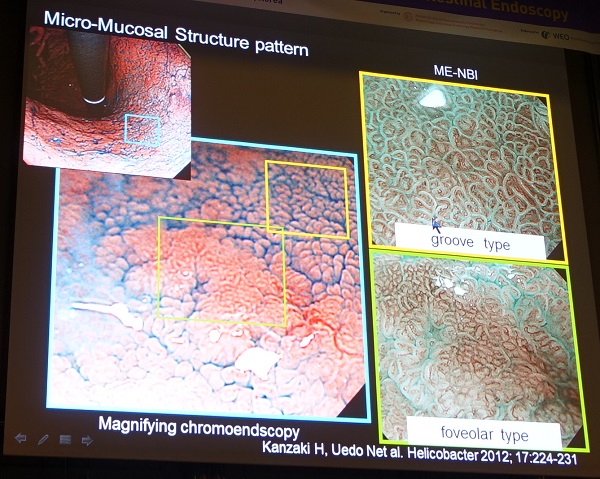

Sticky mucous는 조직학적으로 purulent exudate임 Hp 양성에서 보이는 소견입니다.
위축성위염 환자의 Hp 제균치료 후 mottled patchy erythema가 발견됩니다.
[이준행 질문] Kyoto classification is good, but I think it takes long time to evaluate the whole gastric mucosa by Kyoto system. Would you please tell me your routine upper endoscopic examination? How long does it take?
[Ueo 선생님 답변] In my routine practice, upper endoscopy takes about 5-6 minutes including WLE and NBI.
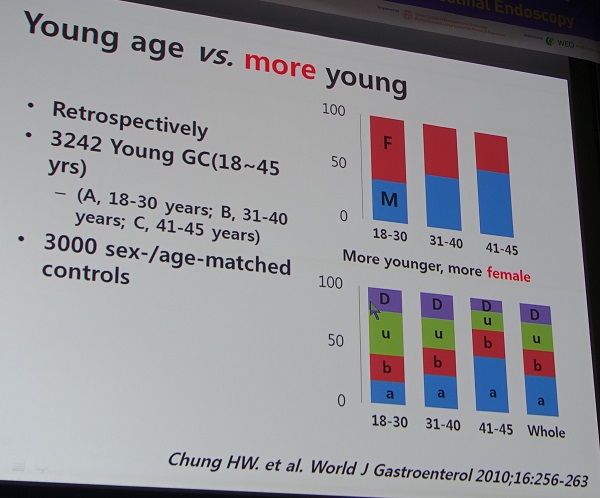
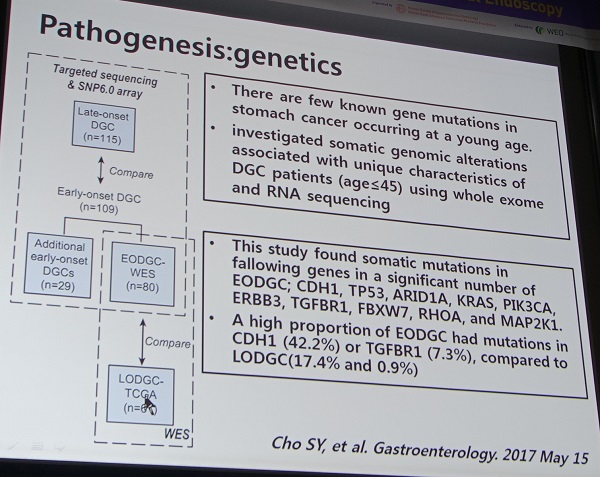
2. Gastric cancers in younger population. (연세대 이상길)
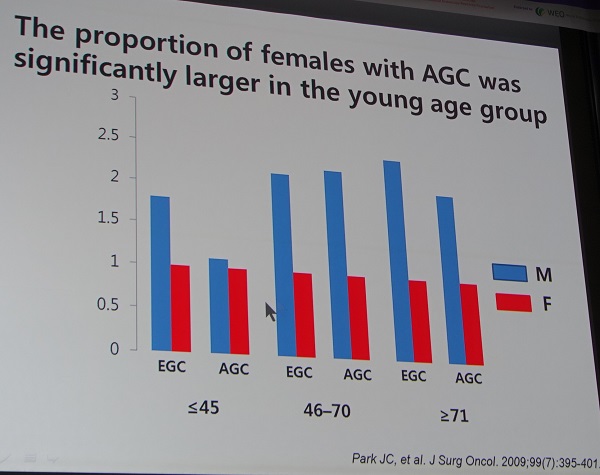


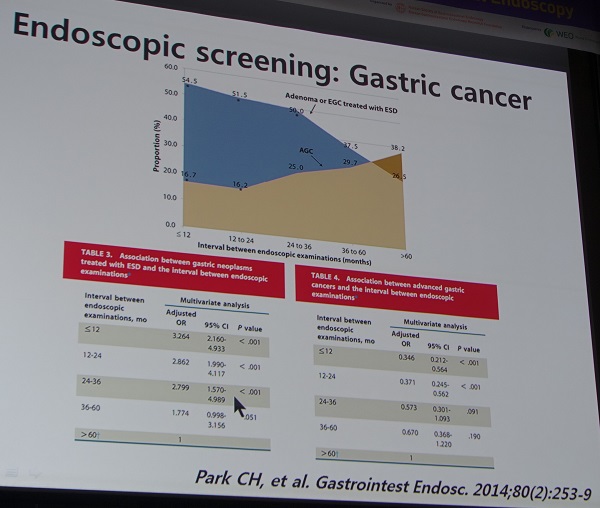
[Uedo 선생님 comment] 저희 기관에서 젊은 위암 환자는 거의 항상 Helicobacter 양성입니다. 따라서 몇몇 지역에서는 학생 시절에 urine 검사를 통하여 헬리코박터 감염자를 찾아서 제균치료를 하고 있습니다.
[이준행 혼잣말] 헬리코박터는 젊은 사람과 좀 더 나이가 있는 사람에서 위암 발생기전이 다른 것 같습니다. 젊은 사람에서는 undifferentiated type cancer를 만드는 경우가 많고 그보다 나이가 많은 경우는 differerentiated type cancer를 만드는 경우가 더 많습니다.
* 참고: EndoTODAY 젊은 환자의 위암
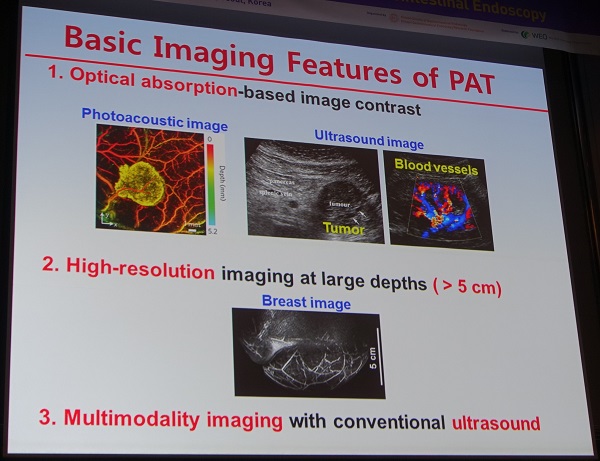
3. Photoacoustic endoscopy for gastric neoplastic lesions. (고려대 최혁순)
4. Magnifying endoscopy and other new technologies for gastric neoplastic lesions. (조주영)
![]() 7. Approach to subepithelial tumor of the upper gastrointestinal tract (6월 3일 토요일 오후)
7. Approach to subepithelial tumor of the upper gastrointestinal tract (6월 3일 토요일 오후)
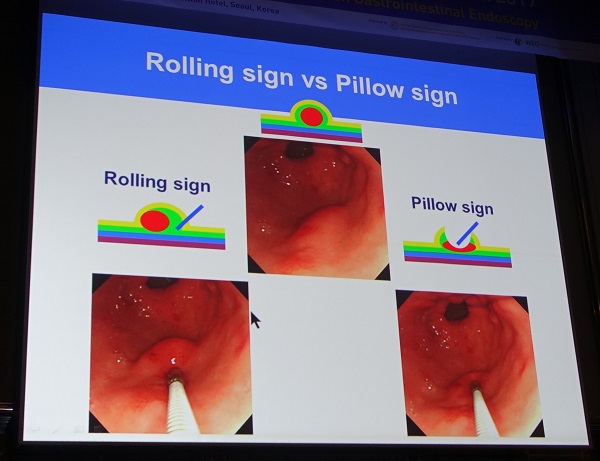
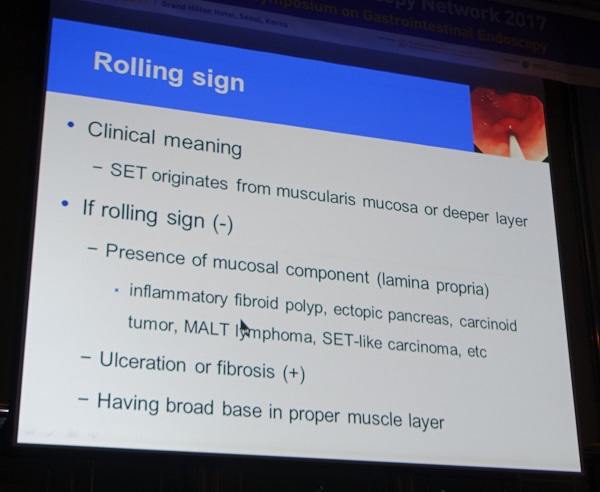
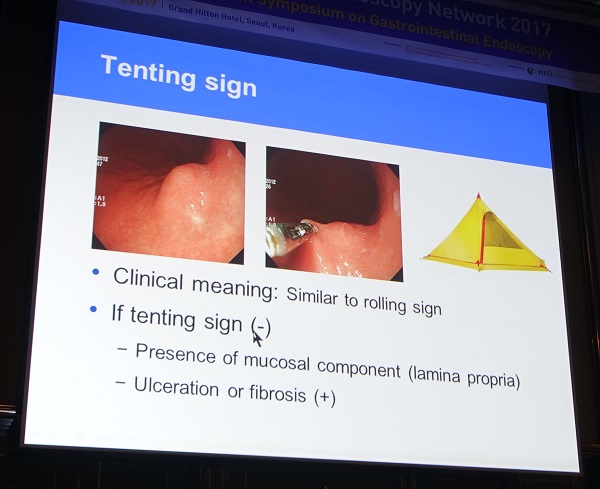
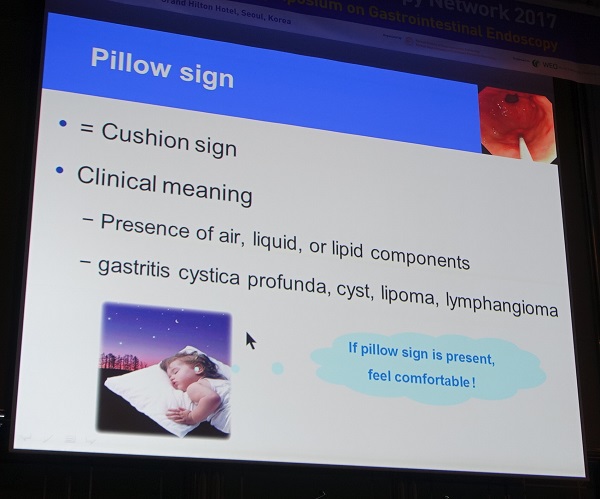
1. Diagnostic approach based on the systematic endoscopic findings. (부산대학교 김광하)
식도
위
십이지장

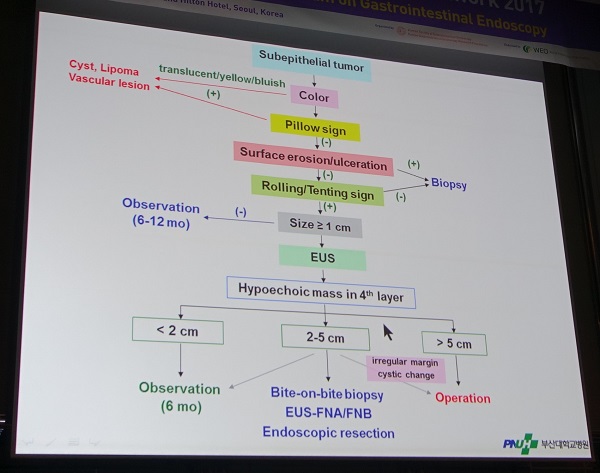
[이준행 질문] 선생님의 algorithm에서 1cm가 EUS의 기준이지만, EUS로 측정한 크기가 2cm 이하면 observation을 권하셨습니다. 그렇다면 EUS 기준이 2cm이면 적당할 것 같습니다. 1-2cm에서 EUS를 권하는 이유는 무엇입니까?
[김광하 교수님 답변] Layer와 정확한 크기를 측정하기 위함입니다.
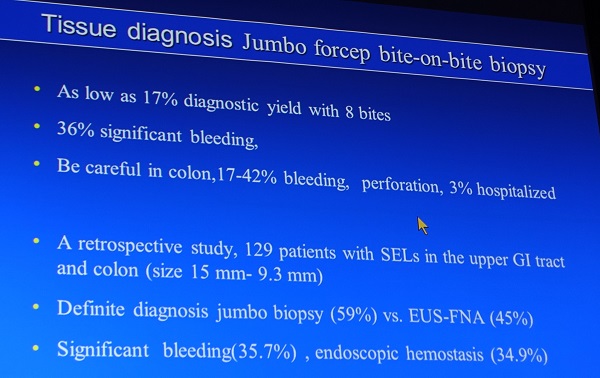
2. EUS-guided diagnosis including tissue confirmation. (가톨릭대학교 조유경)
최근 유럽 가이드라인에서는 3rd layer SMT는 가능하면 조직을 얻도록 권하고 있습니다.
이 슬라이드를 보면서 며칠 전 EndoTODAY 위암 484를 통하여 소개한 증례가 떠올랐습니다. Cardia의 보만 4형 진행성 위암이었는데, 위암 진단 1년 전 cardia에 SMT가 있었습니다.
조유경 교수님께서 보여주신 증례와 비슷하지 않나요? 증거는 없으나 이때의 작은 SMT도 암이지 않았나 생각하고 있습니다.
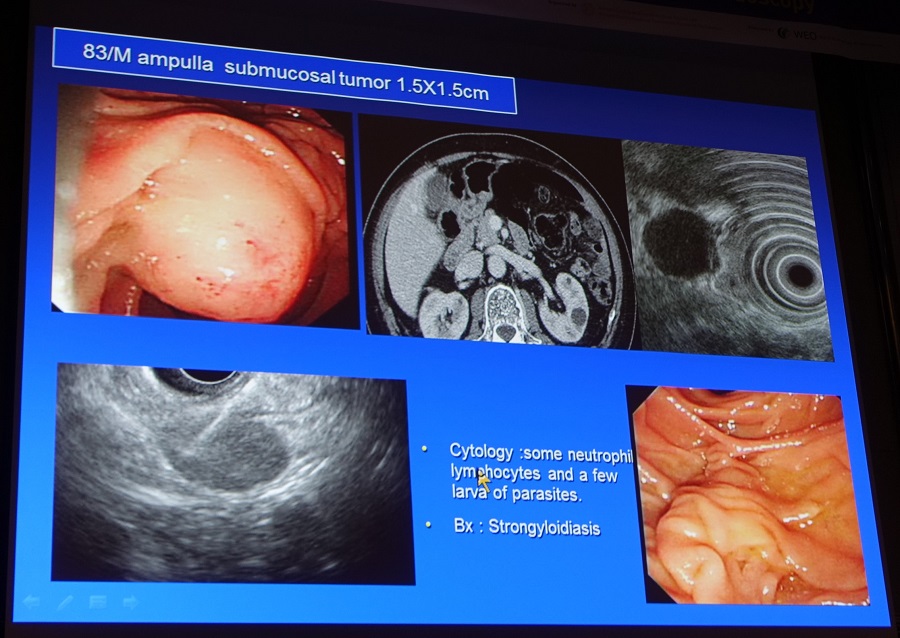
십이지장 점막하종양 양상으로 발견된 분선충증. 이번 심포지엄에서 가장 흥미로웠던 증례였습니다. 저는 기생충학 박사이니까요.^^ (참고: EndoTODAY 분선충)
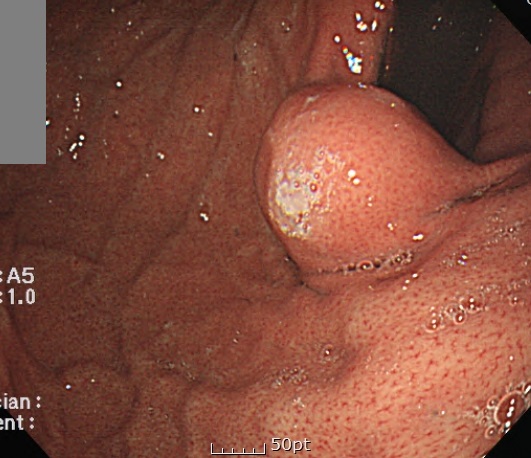
이 부위의 ectopic pancreas는 종종 있는 모양입니다만 조직학적으로 증명된 경우는 매우 드문 일입니다. 2015년 한 애독자의 편지에서 비슷한 경우가 있었습니다. 30대 남자 외국인 노동자였고 귀국 전 건강검진을 하다가 cardia SMT가 발견되어 의뢰되었던 경우였습니다. 외국으로 나갈 예정이었고 본인이 적극적으로 진단하기를 원하고 GIST가능성이 있다면 수술까지 받고 싶다고 하였기 때문에 EUS-FNA를 시행하였던 사연이 있었습니다. 아래 사진입니다.

3. Case-based discussion - A case of gastric subepitheial tumor (제주대학교 나수영)
원인 미상의 SMT에 대한 workup 후 ESD로 제거하였고 최종 결과 Anisakis에 의한 submucosal eosinophilic abscess로 추정되었던 환자입니다.
이 사진에 대하여 김광하 선생님은 GIST의 모양이라기보다는 inflammation일 가능성이 높으므로 EUS를 하되 지금 하지 않고 4주 후에 시행하는 것이 좋겠다는 의견을 주셨습니다.
이 사진에 대하여 조유경 선생님은 3rd layer 병소이고 4th layer 침윤은 없으므로 내시경 절제술을 할 수 있을 것이라고 Complete resection이 되지 않고 partial resection이 되더라도 조직학적 진단에는 문제가 없다고 comment 하셨습니다. 김광하 교수님께서는 GIST나 다른 SMT의 전형모양은 아니므로 bite on bite technique으로 조직을 얻어보겠다는 의견을 주셨습니다.
조직검사 결과에 대하여 김광하 교수님께서는 이 정도 소견에서는 parasite infection의 가능성이 있으므로 추적관찰을 할 수 있다고 답하면서, 아니사키아시스는 급성 복통을 일으키는 경우가 보통이지만 acute 증상이 없는 경우도 있다고 덧붙이셨습니다.
Submucosal fibrosis가 있어서 시술이 쉽지 않았지만 완벽한 절제는 가능하였습니다.
Heavy infiltration of eosinophils in submucosa, with abscess formation, suspicious of sequelae of parasitic infestation.
아니사키스증이 가장 많은 곳이 제주입니다. 과거에 비해서는 많이 줄었다고 합니다.
* 참고: EndoTODAY 아니사키스
![]() 8. Diagnosis of EGC and its precursors: endoscopy and beyond (6월 4일 월요일 breakfast session) - Nariya Uedo (Osaka International Cancer Center)
8. Diagnosis of EGC and its precursors: endoscopy and beyond (6월 4일 월요일 breakfast session) - Nariya Uedo (Osaka International Cancer Center)
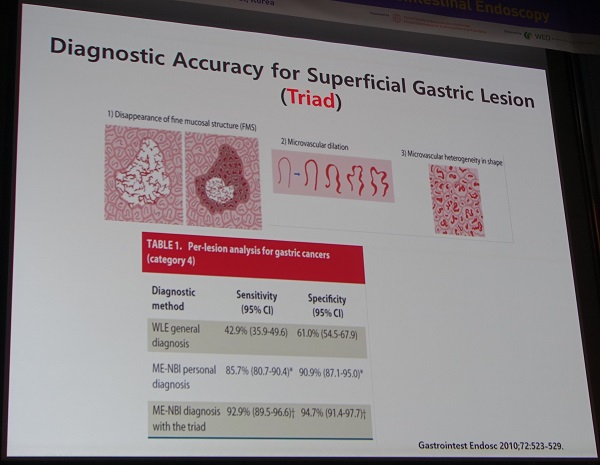
백색광 내시경에 비하여 NBI-M (NBI를 켜고 확대내시경으로 관찰하는 것)은 sensitivity는 비슷하지만 specificity는 상당히 좋습니다. 즉 별 것 아닌 것 같은 것들을 잘 가려낸다는 뜻이고, 이는 임상적으로 불필요한 조직검사를 현저히 줄일 수 있을 것 같다는 이야기였습니다.
다소 이해하기 어려운 슬라이드였는데요... 암진단에 있어서 demarcation line은 sensitivity가 높은 반면 specificity는 낮고, irregular macrovascular pattern이나 irregular microsurface pattern는 specificity가 높다는 이야기였습니다. 이를 잘 활용하면 진단적 가치를 높일 수 있습니다.
병소 옆에 white globe appearance가 보이면 암일 가능성이 높습니다.
Takashi Kanesaka. Endosc Int Open 2015
Takashi Kanesaka. Endosc Int Open 2015
각 소견의 진단 정확도 (Takashi Kanesaka. Endosc Int Open 2015)
Representative cases for each endoscopic microvascular finding. Target lesions indicated with white arrows. a Case 1: dilation and tortuosity were present, but difference in caliber and variation in shape were absent. This lesion was histologically diagnosed as noncancerous. b Case 2: tortuosity was present but dilation, difference in caliber, and variation in shape were absent. This lesion was histologically diagnosed as noncancerous. c Case 3: dilation, difference in caliber and variation in shape were present, but tortuosity was absent. This lesion was histologically diagnosed as cancerous. d Case 4: tortuosity and variation in shape were present but dilation and difference in caliber were absent. This lesion was histologically diagnosed as cancerous. (Takashi Kanesaka. Endosc Int Open 2015)
전향적 임상연구에서는 큰 차이를 보여주지 못했습니다.
좌장 table에서 찍은 마지막 결론 슬라이드입니다. 멋진 강의였습니다. Uedo 선생님. 감사합니다.
Uedo 선생님의 강의와 10분 정도의 토론 이후에도 많은 개별적인 질문이 있었습니다. 아무래도 우리나라에서는 아직 위암 확대내시경 부분에 대한 경험이 적기 때문인 것 같았습니다. 그래서 위암의 확대내시경 관찰법(3단계 접근법)을 짧게 소개합니다.
1 단계 (정상 소견 익히기) - 위암 내시경 진단을 위해서는 fundic mucosa와 pyloric mucosa의 정상 NBI 확대내시경 소견을 잘 알아야 합니다. Microvascular structure와 microsurface structure가 위치에 따라 다르기 때문입니다.
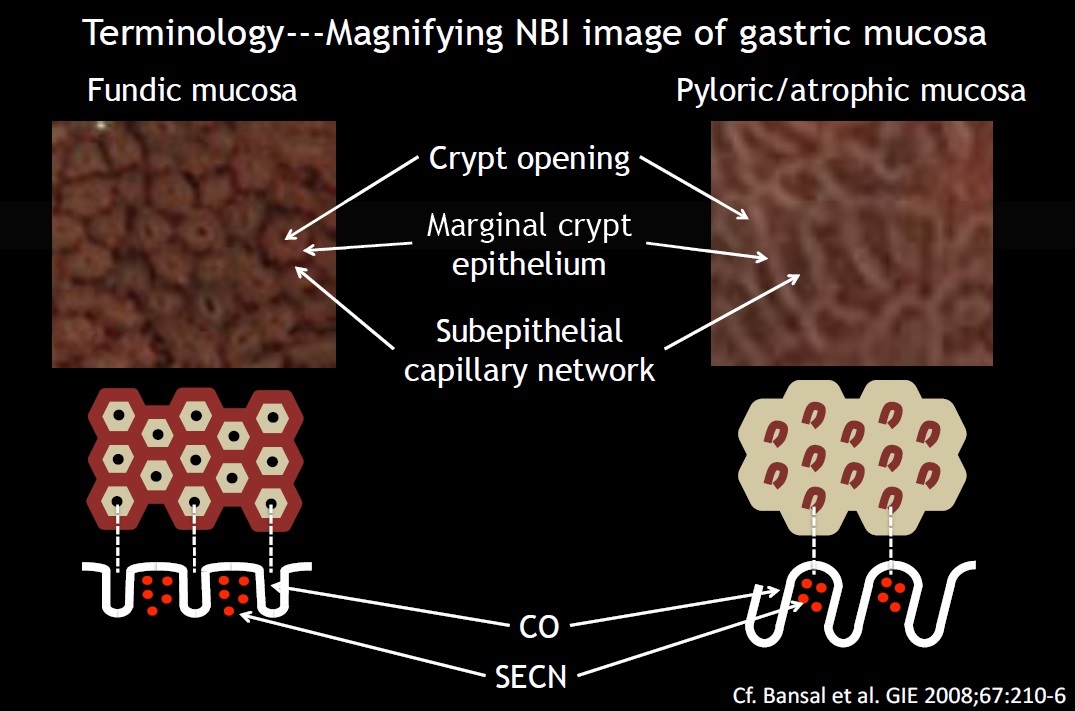
- Microvascular architecture (V) : subepitherial capillary network (SECN), CV (collecting venule)
- Microsurface structure (S): marginal crypt epithelium (MCE), crypt opening (CO)
2 단계 (demarcation line 찾기) - 백색광 내시경으로 관찰하다가 의심스러운 함몰부위가 있으면 NBI 확대내시경을 적용합니다. 정상과 비정상의 경계가 보이면 이를 demarcation line이라고 부릅니다. 한 임상연구에 의하면 검진 환자의 20% 정도에서 suspicious lesion이 보여 NBI 확대내시경을 했다고 합니다.
Digest Endosc 2015년 7월호. WEO Upper GI Cancer Committe
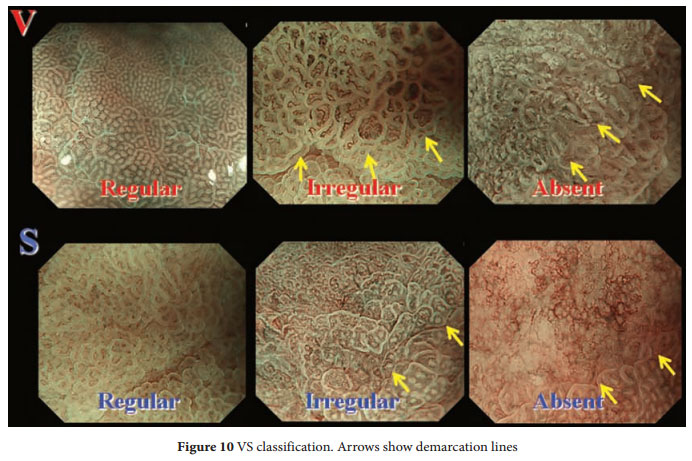
3 단계 (IMVP와 IMSP 확인) - 일단 demarcation line이 있으면 microvascular pattern과 microsurface pattern을 관찰합니다 (VS classification). Irregular microvascular pattern (IMVP)이나 irregular microsurface pattern (IMSP)이 있으면 위암으로 진단할 수 있습니다.

![]() 9. Management of upper GI bleeding - an issue of Asian endoscopiy societies. (6월 4일 일요일 오전)
9. Management of upper GI bleeding - an issue of Asian endoscopiy societies. (6월 4일 일요일 오전)
1. Prevention of NSAIDs- or aspirin-related peptic ulcers (James Lau, Chinese University of Hong Kong)
PPI는 small bowel bleeding을 증가시킬 수 있습니다.
[이준행 comment] "PPI는 small bowel bleeding을 증가시킬 수 있다." 부분에 대해서는 2017년 5월 8일 월요집담회 (이혁 교수님 특강)에서 상세히 논의한 바 있습니다. 당시 자료를 아래에 옮깁니다.
PPI를 사용하면 오히려 small bowel injury가 많을 수 있다는 최근 연구입니다. 예를 들어 반복적인 small bowel bleeding으로 입원하신 환자가 그때마다 위내시경에서는 큰 이상이 없었다면, 이 환자는 PPI를 피하고 mucoprotective agent를 쓰는 것이 더 좋을 수 있겠습니다.
우측 box에 해당하는 환자들에서 small bowel injury가 발생하면 그로 인한 손해가 막심할 수 있습니다. 이런 환자들에서 PPI는 좀 더 조심스럽게 선택되어야 할 것 같습니다.
소장 쪽에는 PPI가 아예 빠졌음에 주목합시다.
[이준행 보충 설명] NSAID 사용자가 소장 출혈로 내원하면 퇴원시 습관적으로 PPI를 처방하는 관례가 있었습니다. "소장 출혈은 막을 수 없더라도 적어도 위십이지장 출혈 예방에는 도움이 되겠지..."라는 순진하고 막연한 생각 때문이었습니다. 그러나 이제는 소장 출혈 환자에서 PPI를 쓰지 말아야 할 것 같습니다. 적어도 반복 소장 출혈 환자에서는.
2. Predictors of outcome in patients with bleeding peptic ulcer - which one is better? (가톨릭대 김병욱)
Forrest classification. Lancet 1974;2:394
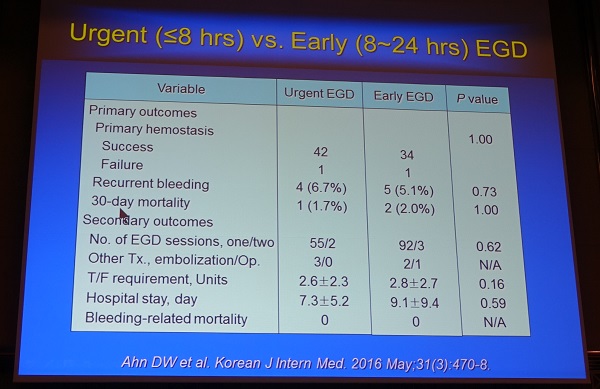
[이준행 comment] 안전하게 적당히 빨리 하면 충분하지 아주 빨리 내시경할 필요는 없습니다. 서두르다가 일을 그르치는 경우가 더 많을 것 같습니다.
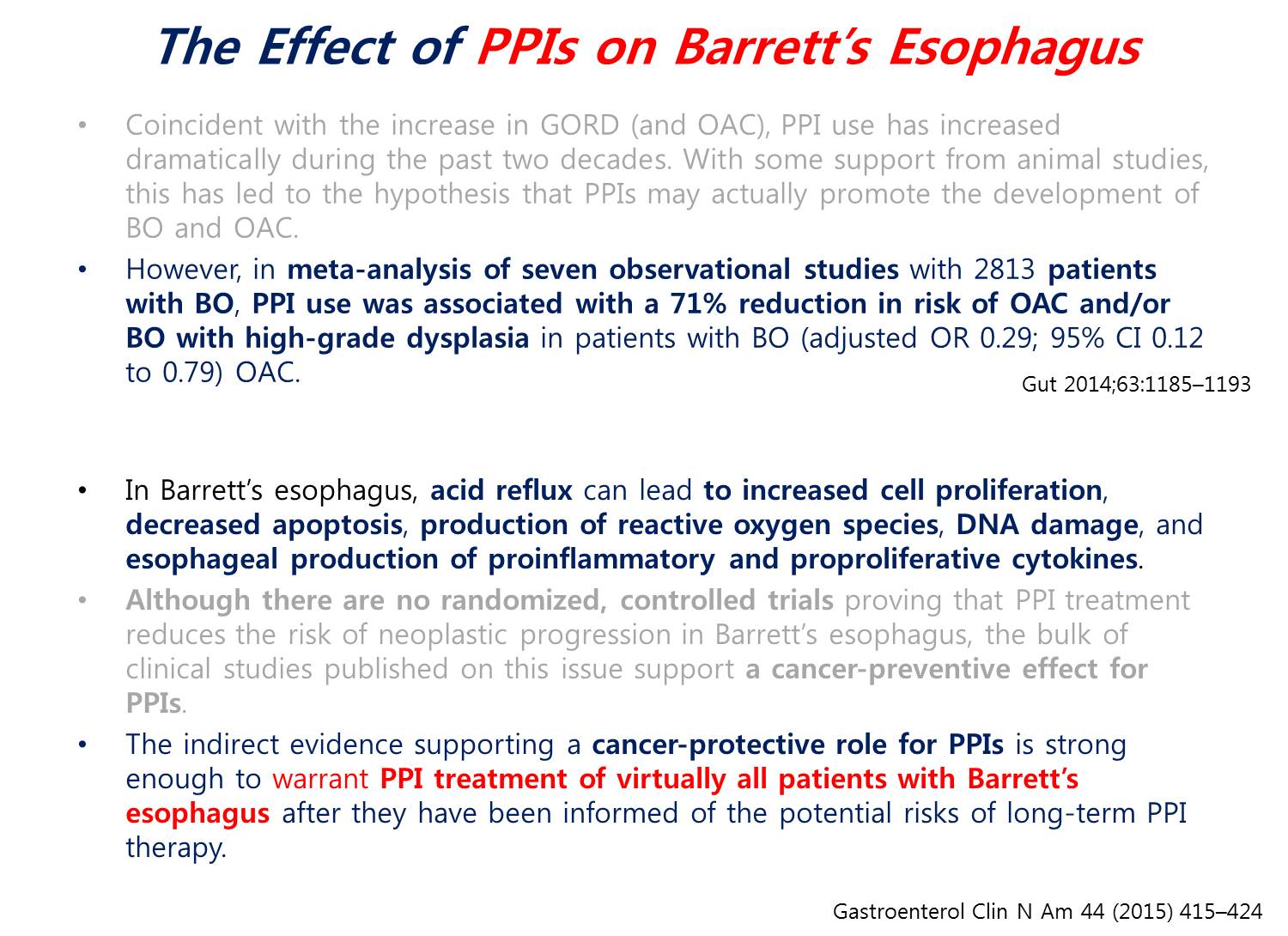
![]() 10. Update on the diagnosis and treament of Barrett’s esophagus. (6월 4일 일요일 오후)
10. Update on the diagnosis and treament of Barrett’s esophagus. (6월 4일 일요일 오후)
1. Endoscopy of the lower esophagus for the detection of Barrett's esophagus and related neoplastic conditions. Lars Aabakken (Deptment of Medicine, Rikshospitalet University Hospital, Norway. lars.aabakken@medisin.uio.no)
WATS3D - 회전하는 brush를 이용하여 많은 sample을 얻은 후 3D scan을 하여 입체적으로 분석하는 새로운 방법입니다.
특별한 brush를 이용하여 조직을 얻은 후 computer를 이용하여 3-D로 조직학적 관찰을 할 수 있다는 것입니다.
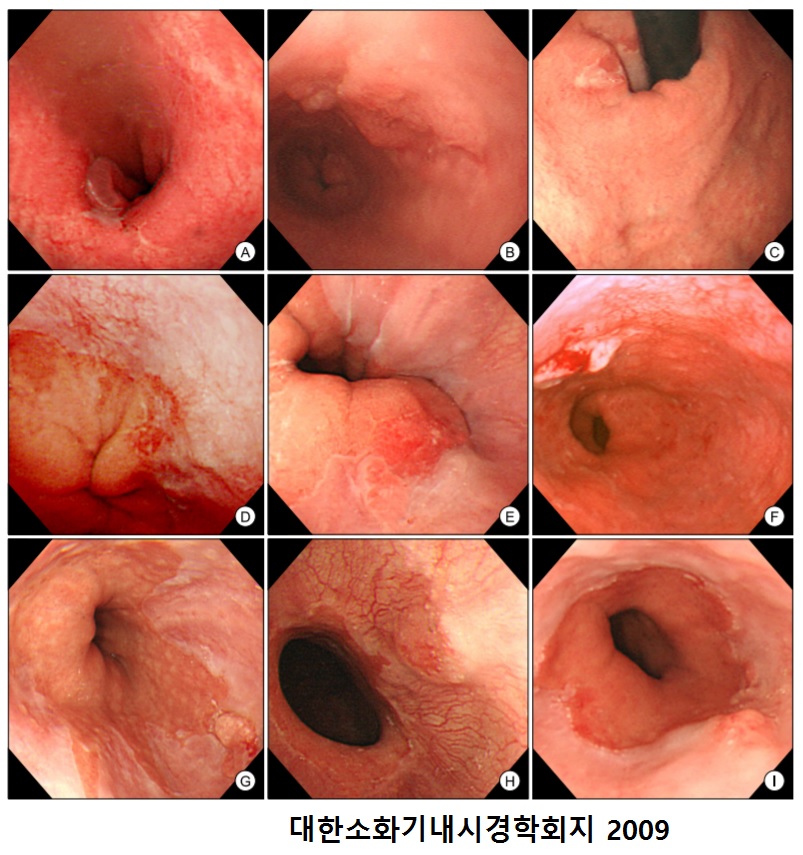
최근 발간된 유럽 바렛 가이드라인을 소개하셨는데 저는 두 가지가 중요한다고 생각했습니다. (1) 1 cm 미만은 무시하라는 것("a minimum length of 1 cm")과 (2) 조직검사로 specialized intestinal metaplasia가 필요하다는 점입니다. 반가운 마음에 다음과 같이 질문하였습니다. "Overdiagnosis can be a big problem, so I strongly agree with your first statement that the minimum length of columnar metaplasia is 1 cm for the diagnosis of Barrett's esophagus. In Korea, early stage Barrett-associated adenocarcinomas are usually realated with short segment Barrett esophagus, and some of them is very short, less than 1 cm. Do you often see Barrett-associated adenocarcinoma in a very short Barrett esophagus?" 2009년 삼성서울병원에서 경험하였던 Barrett's adenocaricnoma에 대한 짧은 보고를 낸 적이 있습니다 (김상중. 대한소화기내시경학회지 2009).
정대영 교수님께서 "Seattle protocol을 따르는 의사가 얼마나 되는가?" 질문을 하셨습니다. 연자는 "very few"라고 답하였습니다. 가이드라인에서는 2cm마다 4 quadrant biopsy를 하는 Seattle protocol이 언급되는데, 너무 번거롭기 때문에 임상에서 이를 따르는 사람이 very few 한 것 같습니다. 다음 연자인 Ponchon은 42%라고 자랑스럽게 답했습니다.
2. Risk evaluation and treatment for Barrett's esophagus and related neoplasia in the Western countries. Thierry Ponchon
1) Photodynamic therapy는 부작용이 너무 많습니다. esophageal stenosisrk 36%.
2) Radiofrequency ablation: 최근 메타분석에서 intestinal metaplasia (= 바렛) 재발 9.5% Dysplasia 발생 2.0%, carcinoma 1.2%
3) Cryotherapy는 대강 radiofrequency와 비슷합니다.
4) EMR - Piecemal EMR is not abandoned.

5) ESD - 연자는 "If there is any mucosal abnormality, ESD for me."라고 말했습니다.
Floor에서 non-dysplasitc Barrett에서 PPI의 역할에 대한 질문이 있었는데, 연자는 "증상이 없으면 PPI를 쓰지 않는다"고 답했습니다. 이 부분에 대한 전문가들의 의견은 아직 하나로 모이지 못하고 있지만, 최근에는 증상이 없더라도 PPI를 투여하는 쪽으로 데이타가 모이고 있습니다. 2016년 5월 9일 월요점심집담회에서 이풍렬 교수님께서 보여주셨던 슬라이드를 소개합니다. 저의 경험에 의하면 long segment Barrett esophagus 환자는 대부분 증상이 있었던 것 같습니다. 증상이 있는 경우에는 당연히 PPI를 처방하였지만, 혹시 증상이 없는 long segment Barrett esophagus 환자가 오더라도 PPI를 처방할 생각을 갖고 있습니다 (심평원 기준은 아니지만...)
3. Risk evaluation and treatment for Barrett's esophagua and related neoplasia in the Eastern countries. (아산병원 김도훈)
日本은 확실히 특이합니다. Palisading vessel을 기준으로 삼는 곳은 일본밖에 없네요...
日本은 확실히 특이합니다. Barrett esophagus가 현저히 증가하는 곳은 일본밖에 없네요...
Seattle protocol을 따라 조직검사를 하는 의사의 비율을 조사한 결과입니다. [이준행 comment] 제가 보기에는... 현실은 이보다 훨씬 훨씬 적을 것 같습니다. 아직까지 한 명도 만난 적이 없습니다. 일전에 한 모임에서 이와 비슷한 질문을 한 적이 있는데, 'Seattle protocol에 따라 엄청나게 많은 조직검사를 하겠다'고 답한 선생님께 문의하였습니다. "정말 그렇게 많이 하십니까?" "아니요, 아직까지 한번도 그렇게 해 본 적이 없습니다. 앞으로 그런 환자를 만나면 그렇게 해 볼 생각이라는 것일 뿐입니다." 그렇습니다. Seattle protocol은 현실적이지 않고, 필요하지도 않다고 생각합니다. 설문조사는 현실을 정확히 반영하고 있는 것은 아닙니다. 그냥 꿈일뿐...

Long-segment Barrett esophagus와 연관된 adenocarcinoma를 멋지게 ESD로 치료한 증례를 보여주셨습니다. 노란색으로 표시한 부분을 제외한 거의 330도 정도 ESD였습니다. [이준행 comment] 저는 아직까지 비슷한 증례를 한 명도 경험한 적이 없습니다. 모두 short 또는 ultrashort segment Barrett esophagus와 관련된 바렛식도암이었습니다. 그래서 질문을 했는데요, 김도훈 선생님도 "long-segment Barrett esophagus와 연관된 adenocarcinoma를 ESD로 치료한 경험은 딱 1예였다"고 답하셨습니다. 그렇습니다. 매우 드문 일입니다. 김도훈 선생님의 멋진 치료 축하합니다. 대단한 실력입니다.^^
* 참고 1) EndoTODAY 바렛식도 - 종설 (2009)
* 참고 2) EndoTODAY 바렛식도선암 - 강의록 (2015)
* 참고 3) FAQ on Barrett's esophagus
![]() 11. Endoscopy education systems and new concepts in GI endoscopy
11. Endoscopy education systems and new concepts in GI endoscopy
1. Third space endoscopy for submucosal tumor - from POEM to POET. Haruhiro Inoue (Showa U, Tokyo, Korea)
2008년 9월 8일부터 2016년 3월 21일까지 시행한 POEM 1408예에 대한 분석 결과를 보여주셨습니다.
Diffuse esophageal spasm 증례는 LES myotomy를 하지 않고 esophageal body만 길게 myotomy를 해 주고 있습니다.
Gastric POEM (G-POEM)는 very simple procedure입니다. Entry site와 myotomy site가 매우 가깝기 때문입니다 (이 이유를 물어보았는데.... myotomy의 길이가 2cm로 짧기 때문에 submucosal tunnel이 짧아도 되고 시술이 어렵지 않다고 합니다). Duodenal muscle은 매우 thin하여 십이지장 근육은 myotomy를 하지 않습니다.
POET (peroral endoscopic tumor resection) - endoscopic submucosal tumorectomy를 POEM 비슷하게 시술하는 것입니다.
Full layer resection in the esophagus (ectopic pancreas가 repeated mediastinitis를 일으켰던 경우)라는 놀랍고 무서운 시술을 소개하셨습니다.
Preservation of the mucosa intact is the most important.
Hook knife를 사용한 증례가 있어서 질문을 했는데요... 보통은 triangle knife를 사용하지만 매우 까다로운 경우, fine한 시술을 해야하는 경우에는 hook knife를 사용하기도 한다고 합니다.
[이준행 comment] IDEN 2017 Inoue 선생님 강의를 들으면서 더없이 부러웠습니다. 2008년 9월 8일 오후 세계 최초 POEM 시술 장면을 동영상으로 보여주셨습니다. 현재 technique과 거의 동일한 방식이었습니다. 게다가 세계 최초 POEM 시술 환자를 2017년 5월 다시 만나 함께 찍은 사진을 자랑스럽게 소개하셨습니다. 그러니까 첫 시술 8년 후 다시 그 환자를 만나 뿌듯해하셨던 장면입니다. 잘 먹지 못하던 환자가 POEM 시술 후 20kg나 늘었다고 좋아했다는 것입니다. 얼마나 부럽습니까. 정말 대단하다고 생각합니다.
세계 최초 POEM 시술 장면
세계 최초 POEM 시술 환자의 시술 전 후 증상 변화와 Eckerdt score
세계 최초 POEM 환자의 시술 8년 후 모습
2. Endoscopy education through on-line community e-mail. (성균관대 이준행)
PPT PDF 3.2M
Thank you very much for your kind introduction.Today, I’d like to split my discussion into three parts. First part will be brief thinking on education. Second part will be a short introduction to the basic endoscopy training course at my institution. Finally, I will show you my personal experience on how to keep CEE, continuous endoscopy education, through sending daily e-mail endoscopy education material. The name of the program is EndoTODAY.
This is a famous painting by 김홍도, one of the greatest artists in Chonsun dynasty. It shows what is required for a good learning environment, such as small group, experienced teacher, nice textbook, repetitive education, positive and negative feedback. In addition, not only simple knowledge but also philosophy should be important part of the curriculum. This kind of ideal teaching and learning condition is very difficult to find in the recent busy endoscopy rooms.
A few years ago, I attended an education workshop on problem-based learning, PBL, in the University of Hawaii.
This is the summary of their ideas on teaching and learning. In order to be successful in the clinical teaching, we need to know our learners, their goal and expectations, their past experiences, and their knowledge and gaps. Teaching tools are another important aspect. They should be time-efficient, and contribute for the distribution of the learning experience. In addition, we can extend our teaching and learning beyond actual contact time.
This is a picture in a recent endoscopy box simulator training at my institution. Yes. It is a very close contact. But it’s not sufficient. There are so many students, residents, fellows, but the number of teaching staffs is limited. And they are already busy doing patients care and research.
When I was a young resident learning endoscopy, the first thing I learned were basic endoscopy techniques. How to insert the endoscope through the throat, how to examine the whole stomach without blind area, how to take biopsies, how to make an endoscopy report, etc. At that time, I didn’t have enough knowledge about basic endoscopic findings of chronic gastritis, peptic ulcers, EGCs, AGCs, reflux esophagitis, hiatal hernia, and so on. Now I want to say “I am sorry.” to the patients during my early endoscopy experience. Everything changed or should be changed. We need to start teaching and learning basic endoscopic knowledge before starting technical education.
Left side is traditional classic endoscopy learning method. After short period of observation, you can or you should insert the endoscopy. Be brave. That’s it. Nothing more. Just a lot of experiences. Right-hand side is our recent approach. Basic lectures…
This is the overview of the 3 month basic endoscopy training course at my institution. It includes on-line lecture, off-line staff lecture, book reading, journal club, description training, conferences, hands-on programs and finally EndoTODAY.
Most basic self-learning materials are on-line YouTUBE lectures by me and other professors.
Of course, there are some basic off-line staff lectures. We also consider book-reading with coaching very important.
Weekly description exercise is a good way of learning how to approach clinically important diseases. Professors give detailed personal feedback, which is a great workload for us, but very important part of our training.
Box simulator training is a very popular to our young doctors. They enjoy a lot learning basic endoscopy skills.
We have Monday GI conference,
And Thursday endoscopy conference with lunch boxes. Nice lunch boxes are very import, because
If you feed them, they will come. If you don’t feed them, they will not come.
Occasionally, we have night-time learning sessions called one point lesson. You can see some of the important lectures on YouTube.
Most of the education materials in our conferences are saved in endotoday.com. It is kind of an on-line archives.
Using all the education tools and conferences, we think that balance between push and pull is well established in basic endoscopy training. The problem is the later part. In my opinion, after the initial endoscopy training, we rely too much on PULL for CEE (Continuous Endoscopy Education). If they come, they will be updated. If they don’t come, nobody knows. We need to keep them updated.
Finally, I will show you my personal experience on how to keep CEE, continuous endoscopy education, through sending daily e-mail endoscopy education material. The name of the program is EndoTODAY.
I started running a personal homepage 18 years ago.
After the fellowship training, I got a teaching position at Samsung Medical Center. There were a lot of questions from the fellows and residents. I started sending the intranet mail with the answers to all the young doctors in my department.
More and more doctors, mostly from other hospitals, asked me to send the daily endoscopy education material to them.
The number of daily EndoTODAY recipients are rapidly increased. Now more than 2,000 people receive my e-mail everyday.
I try to keep the program interactive. I got a lot of questions and comments.
I did a survey how EndoTODAY is used in the real clinical setting. Most people read the EndoTODAY materials in the morning. They read more than half of the materials, and it took less than 5 minutes.
At that time, my conclusion was that we successfully established a daily E-mail learning program using an Intranet. EndoTODAY is a new and useful method for teaching and learning interesting cases during busy working hours.
Sometimes, I got thank you letters from my on-line students.
This is another thank you letter. A case of intestinal parasite, D. latum.
As I mentioned before, balance between push and pull is important. Even after initial endoscopy training, we can keep CEE (Continuous Endoscopy Education) by push daily endoscopy education material using e-mail (EndoTODAY).
Ladies and gentleman, I’d like to conclude my talk by saying that daily interactive e-mail learning program, EndoTODAY, is a new education platform which is time-efficient, contributes for the distribution of the learning experience, and extend teaching and learning beyond actual contact time.
Thank you very much for your attention.
* Advanced endoscopy technique에 대한 video clip을 올려주면 좋겠다는 의견이 있었습니다. 현재 준비 중이고 조만간 initial product를 볼 수 있을 것이라고 답변하였습니다. 애독자 여러분. 조금만 기다려 주십시요.
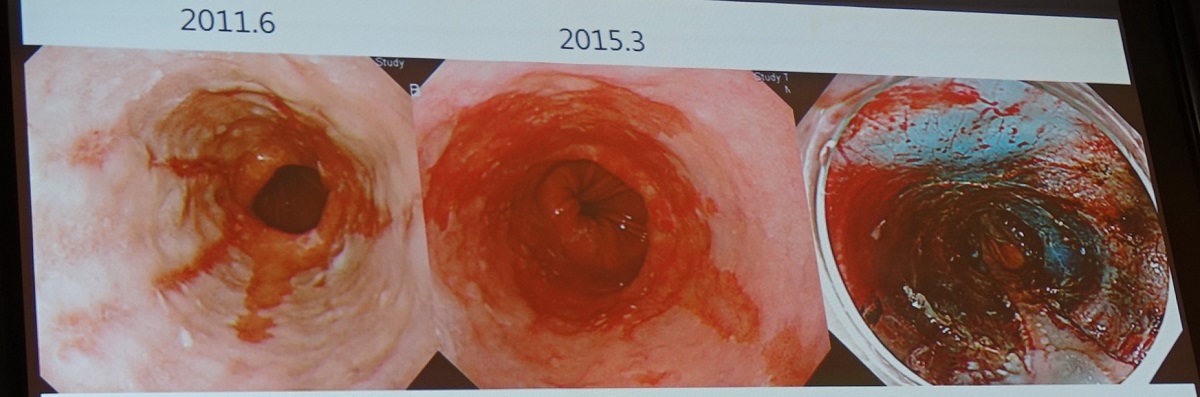
3. Progress in the understanding about the pathogenesis of gastroduodenal ulcers. (차병원 함기백)
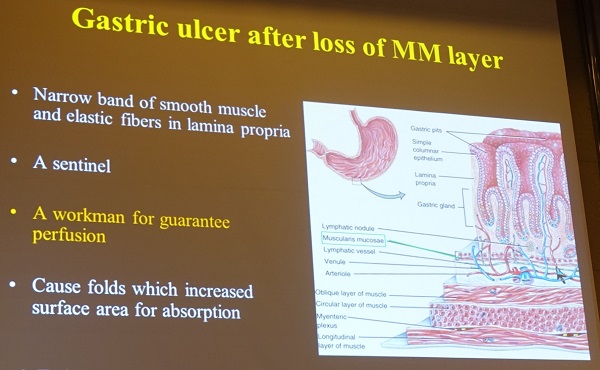
함교수님은 muscularis mucosa의 중요성을 강조하셨습니다. Muscularis mucosa가 무너지면 blood supply가 감소되고 ischemia에 의하여 궤양이 발생합니다.
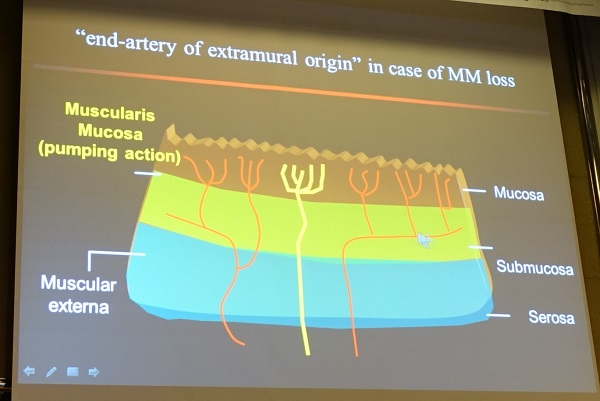
소만에서 궤양이 많은 이유는 "end-artery of extramural origin"입니다. 따라서 소화성 궤양은 perfusion defect 질환이라고 할 수 있습니다.
다음 책을 바탕으로 좀 더 자세히 소개합니다. The Stomach Physiology, Pathophysiology and Treatment, Domschke, W., Konturek, S.J. (Eds.) (Google books)
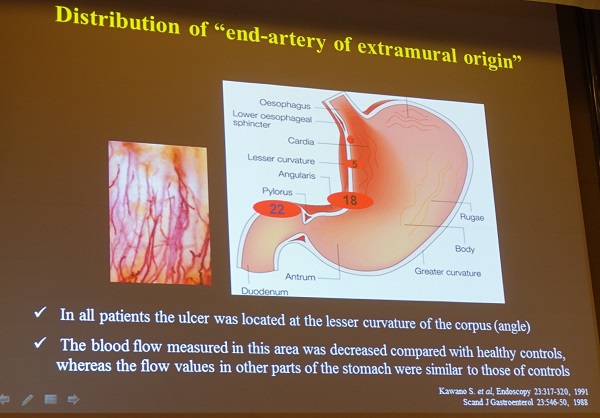
궤양이 흔한 곳에 end-artery of extramural origin도 흔합니다.
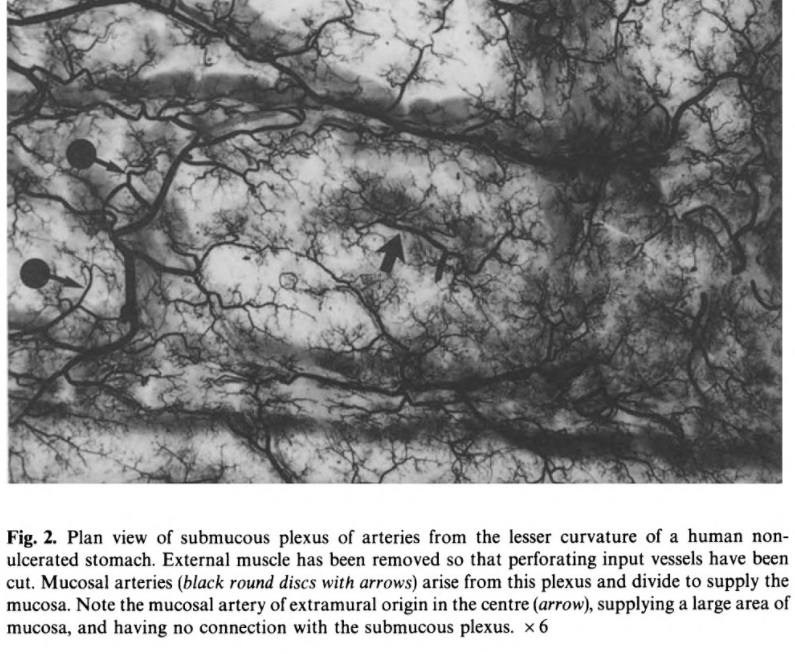

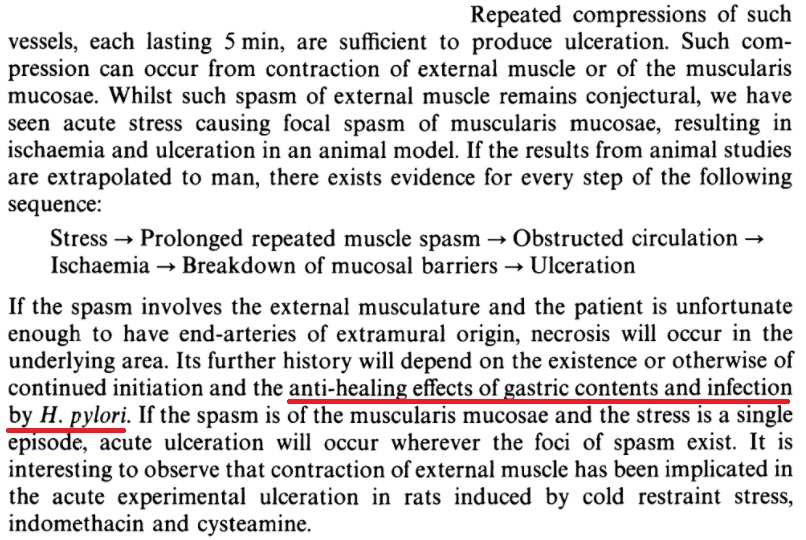
요컨데 근육 (proper muscle이나 muscularis mucosae) 수축으로 유도된 허혈로 궤양이 발생한다는 것인데, 특히 end-artery of extramural origin 부위 (위체부 소만)가 취약하고, 위산이 많거나 Helicobacter가 있으면 healing이 되지 않는다는 것입니다. End-artery of extramural origin이 없는 사람은 궤양이 잘 생기지 않습니다.
![]() 12. Selected posters
12. Selected posters
Autoimmune pancreatitis로 치료받은 병력이 있는 77세 남자가 hematochezia로 내원. CT에서 mesenteric root 주변의 soft tissue mass와 mesenteric lymphadenopathies가 발견되었고, serum IgG4가 정상 상한치의 2배인 266 mg/dL까지 상승되어 있었으며, 복강경으로 림프절 조직검사에서 "lymphoplasmocytic infiltration, moderate to severe fibrosis with many IgG4 positive plasma cells 소견이 나와 IgG4-relates sclerosing mesenteritis (SM)로 진단하고 steroid 사용으로 호전됨. SM was recently reported to be closely related to IgG4-realted disease, a systemic syndrome characterized by mass-like lesions in various organs infiltrated by IgG4-positive plasma cells and high serum IgG4 concentrations.
아산병원 포스터입니다. 대단한 서문입니다. "We developed computer-aided diagnostic system by using artificial intelligence and investigated its usefulness to predict histopathologic classification of colorectal tumors."
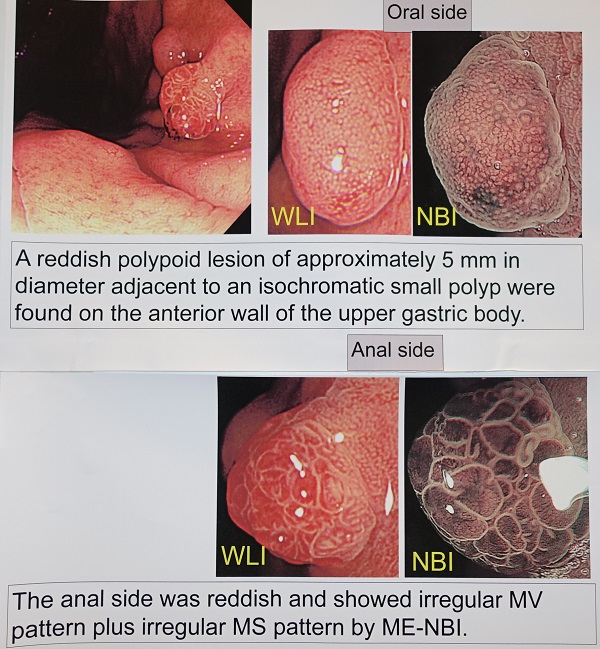
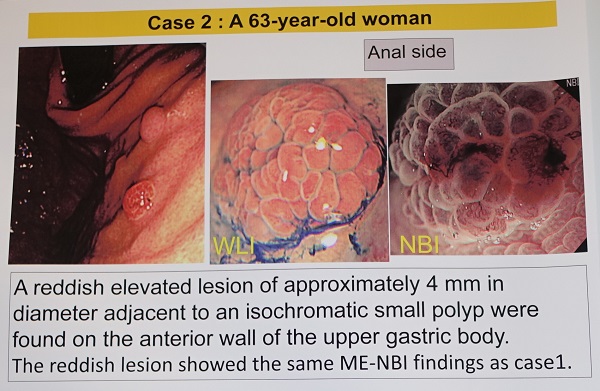
Osaka 암센터 포스터의 첫번째 증례입니다. Fundic gland polyp에서 암이 발생한 경우입니다. 두 용종이 보였고 anal side의 용종은 암이었다는 것입니다.
Osaka 암센터 포스터의 두번째 증례입니다. Fundic gland polyp의 유난히 붉은 부위는 암일 수 있어서 절제를 했는데, 결국 암으로 나왔다고 합니다. (Considering the diagnosis of case 1, we suspected that the reddish lesion was an adenocarcinoma occuring in a FGP and ESD was performed.)
Ductal adenocarcinoma from ectopic pancreas presenting as gastric subepithelial tumor (삼성창원병원)
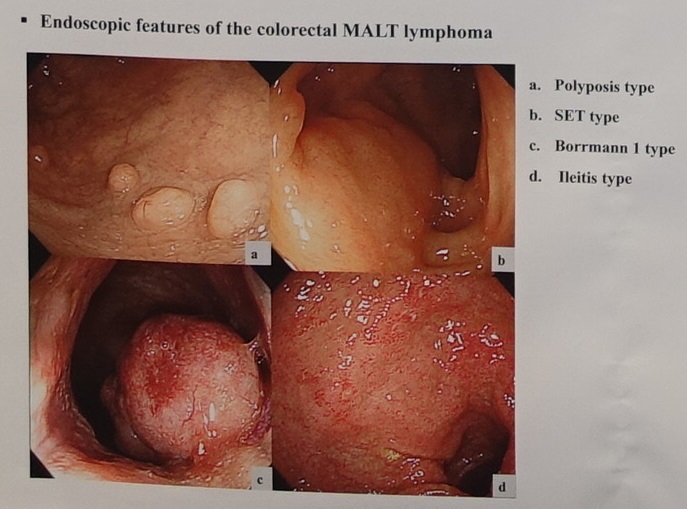
Colorectal MALToma (서울아산병원)
예수병원 포스터입니다. Oral steroid를 사용하여 협착을 막을 수 있었던 증례였습니다. "To prevent pyloric stricture, the patients were started on 20 mg per day of oral prednisolone from the next day after ESD, then were tapered step by step and discontinued at 8 weeks."
고려대학교에서 내시경 로봇을 만든 모양입니다.
![]() [References]
[References]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.