EndoTODAY ГЛНУАц БГНЧ
EndoTODAY ГЛНУАц БГНЧ
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [EsoTODAY 032 - GERD academy 1А]
[EsoTODAY 032 - GERD academy 1А]
2017Гт 10Пљ 22РЯ РжОњДј GERD academy 1АРЛ ОЦЗЁПЁ ПХБщДЯДй.
ДыЧбРЇОЯЧаШИПЁМ СжУжЧб GERD academyПЁ ДйГрПдНРДЯДй.
РњДТ "Important findings to be observed in endoscopic examination of GERD patients"ЖѓДТ СІИёРЧ АРЧИІ ЧпНРДЯДй. ГЛНУАц МвАп ЙшПьБтПЭ ГЛНУАц Л№РдЙ§ ЙшПьБтДТ ЧдВВ СјЧрЕЧОюОп ЧбДйДТ СЁРЛ АСЖЧЯПДНРДЯДй. ГЛНУАц Л№РдЙ§РЛ И№ИЃИщ ГЛНУАц МвАпРЛ СЄШЎШї РЬЧиЧв Мі ОјНРДЯДй. ЙнДыЗЮ ГЛНУАц МвАпРЛ АјКЮЧЯСі ОЪАэ ГЛНУАц Л№РдЙ§ИИ ЙшПьИщ ЕЙЦШРЬАЁ ЕЫДЯДй. РЬ ЕбРЧ БеЧќРЬ СпПфЧеДЯДй. ЛяМКМПяКДПјПЁМ МвШБтГЛАњ РЬПмРЧ ХИАњ МБЛ§Дд Йз ДйИЅ КДПј МБЛ§ДдЕщВВ СІАјЧЯАэ РжДТ ГЛНУАц ЙшПьБт--ГЛНУАц МвАп ЙшПьБтПЭ ГЛНУАц Л№РдЙ§ ЙшПьБтИІ ХыЧеЧб АГГфРдДЯДй-- ЧСЗЮБзЗЅРЛ МвАГЧЯПДНРДЯДй. СІАЁ СїСЂ hands-on trainingРЛ НУФбЕхИЎАэ РжНРДЯДй. АГКАРћРИЗЮ СјЗсРЧЗкМОХЭ(=SMC ЦФЦЎГЪСюМОХЭ)ПЁ ПЌЖєЧЯПЉ РЯСЄРЛ РтАХГЊ, 3-4Иэ ЦРРЛ ТЅМ РњПЁАд СїСЂ ПЌЖєРЛ СжМХЕЕ ССНРДЯДй. РЯПјГЛНУАцБГНЧРК КДПј РхКЎ, СјЗсАњ РхКЎРЬ ОјДТ ПИА ЙшПђХЭРдДЯДй.
PPT PDF 9.7M
GERD academy 2ЙјТА АСТДТ 2018Гт 2Пљ 24РЯ ПЙСЄРдДЯДй.
![]() 1. pH and impedance
1. pH and impedance
СжЗЮ МОчРЧ РдРхРЮЕЅПф, ГЛНУАцПЁМ АќТћЕЧДТ LA-A ШЄРК LA-BДТ СЄЛѓРЮПЁМЕЕ КИРЯ Мі РжРИЙЧЗЮ GERD СјДм БйАХЗЮ КЮСЗЧв Мі РжДйАэ ЧеДЯДй. ЦЏШї LA-A.
2017Гт ЙпЧЅЕШ Update of the Porto consensusПЁМ acid exposure timeРЧ БтСиРЛ 6%ЗЮ СІНУЧб АЭПЁ ДыЧЯПЉ ПЉЗЏ МБЛ§ДдРЧ commentАЁ РжОњНРДЯДй. АњАХПЁДТ 4%ИІ БтСиРИЗЮ ЦЧСЄЧЯПДДТЕЅ АЉРкБт 6%ЗЮ ПУЖѓАЌБт ЖЇЙЎРдДЯДй. ЕЮ АГ СЄЕЕРЧ БЙГЛ ПЌБИПЁМ 4.0-4.5%АЁ СІНУЕШ Йй РжНРДЯДй. СжРЧЧиМ ЦЧСЄЧиОп Чв АЭ ААНРДЯДй.
Update of the Porto consensus (Neurogastroenterol Motil 2017)
KEY RESULTS: Reflux testing should be performed after cessation of acid suppressive medication in patients with a low likelihood of GERD. In this setting, testing can be either catheter-based or wireless pH-monitoring or pH-impedance monitoring. In patients with a high probability of GERD (esophagitis grade C and D, histology proven Barrett's mucosa >1 cm, peptic stricture, previous positive pH monitoring) and persistent symptoms, pH-impedance monitoring should be performed on treatment. Recommendations are provided for data acquisition and analysis. Esophageal acid exposure is considered as pathological if acid exposure time (AET) is greater than 6% on pH testing. Number of reflux episodes and baseline impedance are exploratory metrics that may complement AET. Positive symptom reflux association is defined as symptom index (SI) >50% or symptom association probability (SAP) >95%. A positive symptom-reflux association in the absence of pathological AET defines hypersensitivity to reflux.
(ЙкЙЋРЮ БГМіДд comment) Conventional pH monitoringРЧ false negativeДТ 20-30% СЄЕЕРдДЯДй. ИХПь РЧНЩЕЧИщ ЙнКЙ АЫЛчАЁ ЧЪПфЧв Мі РжНРДЯДй. Brovo pH ДТ 48НУАЃ АЫЛчАЁ АЁДЩЧЯЙЧЗЮ ЛъПЊЗљРЧ КѓЕЕАЁ ЖГОюСіДТ ЛчЖїПЁМ sensitivityАЁ ГєРЛ Мі РжНРДЯДй.
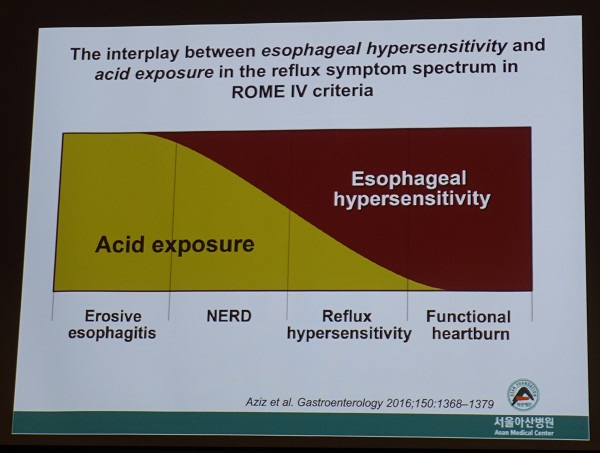
Rome IVПЁ ДыЧб ОрАЃРЧ ГэРЧАЁ РжОњНРДЯДй. Reflux hypersensitivityАЁ ОюДР СЄЕЕРЧ РЧЙЬИІ АЁСіДТ categoryРЮАЁПЁ ДыЧб РЧЙЎРЬ РжБт ЖЇЙЎРдДЯДй. ИХПь trickyЧеДЯДй. Hypersensitive esophagusАЁ ЦїЧдЕЧОю РжБт ЖЇЙЎРдДЯДй. АЫЛч ЕЕСп ШЏРкАЁ ЙіЦАРЛ ДЉИЃИщ reflux hypersensitivity (= positive symptom association)ЗЮ, ЙіЦАРЛ ДЉИЃСі ОЪРИИщ functional heartburn (= negative symptom association)РИЗЮ БИКаЕЫДЯДй.
РЬПЭ АќЗУЕШ ГЛПыРЛ АњАХ РЬЧѕ БГМіДд АРЧПЁМ ПХБщДЯДй.
Rome IIПЁМДТ NERDАЁ ОЦДб АЭРК И№ЕЮ functional heartburnРЬЖѓ КвЗЖАэ РЬ Сп Чб БзЗьРЬ reflux-related hypersensitive esophagusПДНРДЯДй.
Rome IIIПЁМ hypersensitive esophagusАЁ functional heartburnАњ КаИЎЕЧОњСіИИ, NERDПЭРЧ АќАшАЁ ИэШЎЧЯСі ОЪОвНРДЯДй.
Rome IVПЁМ functional heartburnРК reflux hypersensitivity Йз NERDПЭ БИКаЕЧДТ КААГРЧ ЛѓШВРИЗЮ ГЊДЉОюСГНРДЯДй.
PPIИІ ЛчПыЧдПЁЕЕ КвБИЧЯАэ СіМгРћРИЗЮ heartburnРЛ ШЃМвЧЯДТ ШЏРкРЧ РЯКЮАЁ functional heartburnРдДЯДй.
![]() 1-2. ЙЮОчПј БГМіДд ЙпЧЅРкЗс
1-2. ЙЮОчПј БГМіДд ЙпЧЅРкЗс
ЙЮОчПј БГМіДдВВ КЮХЙЧЯПЉ GERD academy ЙпЧЅРкЗс(СѕЗЪ СІПм)ИІ ЙоОвНРДЯДй. МвАГЧеДЯДй.
PPT PDF 2.0M
ЙЮОчПј БГМіДдРК ШЧИЂЧб speakerРдДЯДй. РЬЙј АРЧЕЕ ИХПь ССОвНРДЯДй. СІАЁ Ию РхРЧ ННЖѓРЬЕхПЁ оя№ыРЛ КйПЉКОДЯДй.
GERDРЧ РгЛѓСјДмРИЗЮ PPIИІ ЛчПыЧб ШЏРк Сп ЛѓДчМіПЁМ residual symptomРЬ РжНРДЯДй. AchalasiaУГЗГ СјДмРЬ ЦВИА АцПьЕЕ РжАкАэ, ЛъКаКёОяСІАЁ УцКаЧЯСі ОЪРК АцПьЕЕ РжРИИч, НФЕЕ АњЙЮМКЕЕ АЁДЩЧеДЯДй. РћР§Чб ЦђАЁИІ ХыЧЯПЉ КИДй ШЎНЧЧб СѕЛѓ АГМБ ЙцЙ§РЛ УЃОЦКИДТ АЭРК ССРК РЯРдДЯДй. БзЗЏГЊ, РќЧќРћРЮ GERDРЬ PPI responseАЁ ОЦСж ССРК ЛчЖїЕЕ АЃШЄ residual symptomРЛ АцЧшЧЯАя ЧеДЯДй. 'ОрРЬГЊ ЙКАЁРЧ ФЁЗсЗЮ 100% ПЯКЎЧЯАд И№Еч СѕЛѓРЬ ССОЦСњ АЭРЬДй'ДТ ШЏЛѓРЛ Бњ СжДТ АЭРЬ СпПфЧб АцПьЕЕ РжНРДЯДй. БтДы МіСиРЛ ГЗУчСжДТ АЭ ИЛРдДЯДй. ЛѓДчШї ССОЦСГРИИщ Бз МіСиПЁМ ИИСЗЧЯАэ ОрАЃРК ТќАэ СіГЛДТ АЭЕЕ ЧіНЧРћРЮ ЙцЙ§РдДЯДй. 100%РЛ БтДыЧЯИщ ГЪЙЋ ИЙРК АЫЛч, ГЪЙЋ ИЙРК ХѕОр, ГЪЙЋ ИЙРК ЧъЙпСњРЛ ЧЯБт ИЖЗУРЬДЯБюПф.
ДУ КИДТ ННЖѓРЬЕхСіИИ РњДТ ОрАЃ ДйИЅ РЧАпРЛ АЁСіАэ РжНРДЯДй. ComplianceПЭ adherenceАЁ ЙЎСІРЮ АцПьИІ АХРЧ АцЧшЧб РћРЬ ОјНРДЯДй. ОЦЧСИщ ОрРЛ Дѕ Рп ИдБт ИЖЗУРдДЯДй. ОрРЛ ОШ ИдАэ РЧЛчПЁАд ШПАњЕЕ ОјАэ АшМг ОЦЧСДйАэ РЬОпБтЧЯДТ ЛчЖїРК АХРЧ ОјНРДЯДй. РћОюЕЕ СІАЁ БйЙЋЧЯДТ МПяРЧ 3Тї КДПјПЁМДТ БзЗБ ШЏРк ОјНРДЯДй. ОрРЛ Рп ИдОњДТЕЅЕЕ ОЦЧСДЯБю ОЦЧСДйАэ ЧЯДТ АЭРдДЯДй. ОрИдДТ НУАЃРЛ НФШФПЁМ НФРќРИЗЮ ЙйВлДйАэ ССОЦСіДТ АцПьЕЕ АХРЧ КЛ РћРЬ ОјНРДЯДй. ЛчНЧ СіГ 20Гт АЃ Дм Чб ИэЕЕ КЛ РћРЬ ОјНРДЯДй. ЧЯЗч РЬЦВРК НФШФПЁ ОрРЛ ИдОюМ СѕЛѓ СЖР§РЬ КЮСЗЧв Мі РжРЛ АЭРдДЯДй. БзЗЏГЊ ИХРЯ НФШФПЁ ИдРИИщ РЬ ЖЧЧб Рп ЕшНРДЯДй. РњДТ ПРШїЗС PPIИІ ХѕОрЧЯИщМ prokineticsИІ ЧдВВ УГЙцЧЯДТ АќЗЪ ЖЇЙЎПЁ АэЛ§ЧЯДТ ШЏРкИІ ИЙРЬ КИОвНРДЯДй. ProkineticsДТ ЛѓДчШї КЮРлПыРЬ ИЙРК ОрРдДЯДй. PPIИІ НсМ РЇЛъКаКёОяСІАЁ Рп ЕЧОю ЛъПЊЗљ СѕММДТ ССОЦСГДТЕЅ, ЕПНУПЁ УГЙцЙоРК prokineticsРЧ КЮРлПы ЖЇЙЎПЁ АњАХПЁ ОјДј ЖЧ ДйИЅ СѕЛѓРЬ ЙпЛ§ЧЯДТ ЛчЗЪАЁ ИЙНРДЯДй. GERD ШЏРкРЧ УЪФЁЗсПЁМДТ PPI ДмЕЖ УГЙц, БзЗЏДЯБю ЧЯЗч Еќ Чб ОЫ УГЙцЧЯДТ АЭРЬ АЁРх ССНРДЯДй.
PPI 4Сж УГЙцРИЗЮ СѕЛѓСЖР§РЬ УцКаФЁ ОЪРИИщ pH АЫЛчИІ Чв Мі РжДйДТЕЅ ЕПРЧЧеДЯДй. БзЗЏГЊ РњДТ pH АЫЛч Рќ УГРН ОрРЛ 2Йш ПыЗЎРИЗЮ ДУИЎАХГЊ, ОрРЛ Дѕ АЧб АЭРИЗЮ ЙйВуКОДЯДй. БзЗЏИщ pH АЫЛчАЁ ЧЪПфЧб АцПьИІ ЛѓДчШї СйРЯ Мі РжНРДЯДй.
Porto consensusДТ ГюЖѓПю АГГфРЧ КЏШРдДЯДй. Reflux esophagitis LA-AПЭ LA-BИІ GERDЗЮ СјДмЧЯДТ СѕАХЗЮ КЮСЗЧЯДйДТ Л§АЂРЬДЯБюПф. СѕЛѓЕЕ ОјДТЕЅ ДмСі АЫСј ГЛНУАцПЁМ АцСѕ ПЊЗљМК НФЕЕПАРЬЖѓДТ РЬРЏЗЮ КвЧЪПфЧЯАд PPIИІ КЙПыЧЯДТ ШЏРкАЁ ОѓИЖГЊ ИЙНРДЯБю. ДйИИ, acid exposure time БтСи 6%ДТ СіГЊФЁАд strict ЧЯДйАэ Л§АЂЧеДЯДй.
ЧіНЧРћРИЗЮ СЄЙаЧЯАд УјСЄЧЯБт ОюЗСПю СіЧЅЕщРдДЯДй. РњДТ АХРЧ, ОЦДЯ РќЧє ОШ КОДЯДй.
GERDЗЮ УпСЄЧЯАэ PPIИІ ЕхЗШРИГЊ СѕЛѓРЬ ЧіРњШї ССОЦСіСі ОЪРИИщ achalasiaИІ РЧНЩЧи КИДТ АЭРЬ ССНРДЯДй. EsophagographyИІ ЧЯИщ ЕЫДЯДй. БзЗЏГЊ, esophagographyИІ УГЙцЧЯБт Рќ ГЛНУАц ЛчСјРЛ ДйНУ ЛьЦьКИИщ ССНРДЯДй. Esophagogastric junctionПЁ ЖбЗЧЧб hiatal hernia ШЄРК short segment hiatal herniaАЁ РжРИИщ achalasiaДТ АХРЧ ОЦДЯЖѓАэ Л§АЂЧиЕЕ ССНРДЯДй. EG junctionРЬ ОрАЃ tight Чб ДРГІРЬ ЕщИщ Бз ЖЇПЁДТ ЧбЙјТы achalasiaИІ РЧНЩЧЯНУБт ЙйЖјДЯДй.
![]() 2. Manometry
2. Manometry
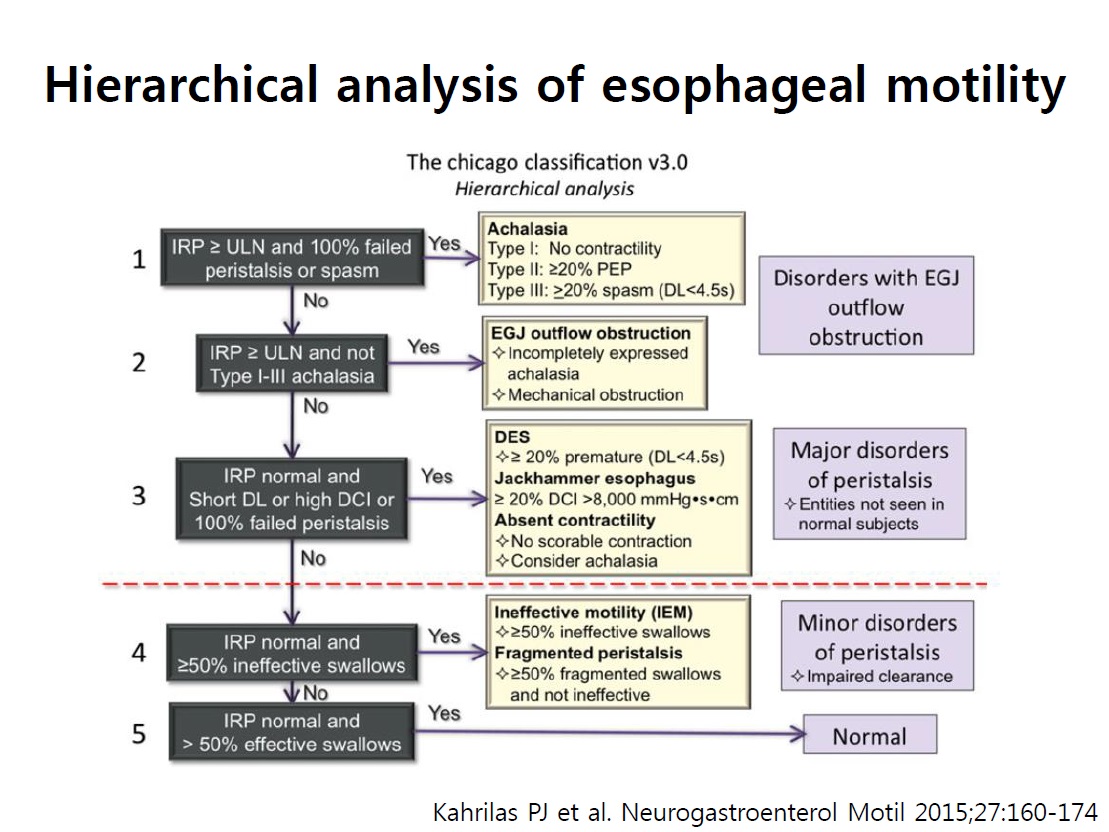
High resolution manometry (HRM)РК ЧіРч Chicago version 3РИЗЮ ЦЧЕЖЧЯАэ РжНРДЯДй.
Hierachical approach by Chicago classification version 3
PDF 2.9M

IRP (integrated relaxation pressure): deglutitive inhibitionПЁ РЧЧЯПЉ 10УЪ Сп EGJ ОаЗТРЬ АЁРх ГЗРК 4УЪРЧ ЦђБе ОаЗТ (СЄЛѓ: <15)
CDP (contractile deceleration point): peristalsis БзЗЁЧСАЁ ВЊРЬДТ СіСЁ = МгЕЕАЁ ДРЗССіДТ СіСЁ
DL (distal latency) : CDPБюСі НУАЃ = БзЗЁЧСАЁ ВЊРЯЖЇБюСі НУАЃ. 4.5УЪ ЙЬИИРЬИщ premature contraction. (СЄЛѓ>4.5)
DCI (distal contractile integral) : peristalsisРЧ АЕЕ (СЄЛѓ: 450-8000)
GERDРЧ СјДмПЁМ HRMРЧ ПЊЧвРК ЙЬЙЬЧеДЯДй. GERD ШЏРкПЁМ mean wave amplitudeАЁ СЖБн ГЗАэ, basal LES pressureАЁ СЖБн ГЗАэ, EG junction type IIIАЁ СЖБн ИЙСіИИ РЬ МвАпИИРИЗЮ СјДмЕЧДТ АцПьАЁ ИЙНРДЯДй (NM 2015;27:963). InspirationЖЇ LESПЭ crural diaphragmРЧ separationРЬ ТќАэАЁ ЕЩ АЭ ААНРДЯДй (ОЦЗЁ БзИВ ТќСЖ). Refractory GERDПЁМДТ HRMИІ ХыЧЯПЉ achalasiaЗЮ СјДмЕЧДТ АцПьАЁ РжНРДЯДй.
Esophagogastric junction (EGJ) morphology subtypes. For each panel the instantaneous spatial pressure variation plot corresponding to the red line on the pressure topography plot is illustrated by the black line to the right. The two main EGJ components are the LES and CD, which cannot be independently quantified when they are superimposed as with a type I EGJ (Panel A). The respiratory inversion point (RIP), shown by the white horizontal dashed line, lies near the proximal margin of the EGJ. During inspiration (I) EGJ pressure increases, whereas it decreases during expiration (E). Type II EGJ pressure morphology is illustrated in Panel B. Note the 2 peaks on the instantaneous spatial pressure variation plot; the nadir pressure between the peaks is greater than the intra gastric pressure. The RIP is at the level of the CD. Panels C and D correspond to type III EGJ pressure morphology defined as the presence of 2 peaks of the instantaneous spatial pressure variation plot with the nadir pressure between the peaks equal to or less than intragastric pressure. The RIP is at the CD with type IIIa (Panel C) whereas it is at the level of the LES in IIIb (Panel D).
ЙкЙЋРЮ БГМіДдВВМДТ antireflux surgery РќПЁДТ ЙнЕхНУ HRMИІ НУЧрЧЯПЉ (1) achalasiaДТ ОЦДбСі (2) НФЕЕУМКЮРЧ peristalsisДТ СЄЛѓРЮСіИІ ШЎРЮЧв ЧЪПфАЁ РжДйДТ АЭРЛ АСЖЧЯМЬНРДЯДй.
Supragastric belchingРК diaphragmatic breathing (КЙНФШЃШэ)РЬ ЕЕПђРЬ ЕЫДЯДй. Speech therapyИІ ЧиКМ Мі РжНРДЯДй. BaclofenРЬ ЕЕПђРЬ ЕШДйСіИИ ШПАњДТ ГЗНРДЯДй.
![]() [FAQ]
[FAQ]
[ПмАњ МБЛ§Дд СњЙЎ]
GERD ШЏРкРЧ МіМњ Рќ manometryИІ ВР ЧЯЖѓАэ ЧЯДТЕЅ, manometryИІ ЧЯСі ОЪАэ esophagographyИІ ХыЧЯПЉ achalasiaИІ ЙшСІЧЯИщ УцКаЧЯСі ОЪРЛБюПф?
[РЬХТШё БГМіДд ДфКЏ]
EsophagographyЗЮЕЕ ЛѓДчКЮКа achalasiaИІ ЙшСІЧв Мі РжНРДЯДй. ГЛНУАцПЁМ achalasiaИІ СјДмЧЯАХГЊ EG jucntion morphology СЄКИИІ ОђРЛ Мі РжСіИИ УцКаЧЯСі ОЪНРДЯДй. (ТќАэЗЮ ГЛНУАц АЫЛчПЁМДТ algironРЛ СжЛчЧЯАэ АЫЛчЧЯБт ЖЇЙЎПЁ body contractilityАЁ ГєОЦСј АЭРЛ ЙпАпЧЯСі ИјЧв Мі РжНРДЯДй.) БзЗЏГЊ РЯКЮ motility СњШЏРК manometryПЁМИИ ЙпАпЕЩ Мі РжНРДЯДй. МвМіРЧ СѕЗЪПЁМДТ manometryЗЮ СјДмРЬ ДоЖѓСіДТ АцПьЕЕ РжРЛ Мі РжНРДЯДй. МіМњРК ЧбЙј ЧЯИщ ЕЙРЬХАБт ОюЗЦДйДТ СЁРЛ АэЗСЧЯИщ, УжДыЧб РкММШї АЫЛчЧб ШФ МіМњЧЯДТ АЭРЬ ССАкНРДЯДй. ОЦСї МіМњПЙАЁ РћБт ЖЇЙЎПЁ ЧтШФ ШЏРкРЧ ФЁЗсИІ РЇЧб СЄКИИІ И№РКДйДТ УјИщ Йз ПЌБИ ИёРћРИЗЮЕЕ ЛѓММЧб СЄКИДТ РЧЙЬАЁ РжНРДЯДй.
[ПмАњ МБЛ§Дд СњЙЎ]
Subtotal gastrectomy 1-2До ШФ РННФРЛ ЕхНУИщ НФЕЕПЁ АЩЗСМ ГЪЙЋ КвЦэЧЯПЉ ХфЧЯАд ЕЧАэ 30Ка ШФ ДйНУ ИдОюКИИщ ОЦЙЋ ЙЎСІАЁ ОјДТ ШЏРкАЁ ИЙНРДЯДй. Ию ДоРЬ СіГЊИщ РЬЗБ СѕЛѓРЬ ОјОюСіБтЕЕ ЧЯДТЕЅПф... РЬРЏДТ ЙЋОљРЯБюПф?
[РЬХТШё БГМіДд ДфКЏ]
Post-surgical gastroparesisРЯ АЭ ААНРДЯДй. Post-surgical gastroparesisПЁМ НФЕЕЕЕ ПЕЧтРЛ ЙоРЛ Мі РжНРДЯДй. МіМњ СїШФПЁ GERDАЁ НЩЧиСіБтЕЕ ЧеДЯДй. МіМњ ШФ СЄМРћ ЙнРРЕЕ ПЕЧтРЛ Сй Мі РжНРДЯДй. НУАЃРЬ СіГЊИщ ШЏРкАЁ РћРРЧЯДТ ИщЕЕ РжСі ОЪРЛБю НЭНРДЯДй.
![]() [References]
[References]
1) EsoTODAY - Esophageal diseases
2) SmallTODAY - Small bowel diseases
3) ColonTODAY - Colorectal diseases
4) Dr. Sinn's LiverTODAY - Liver diseases
© РЯПјГЛНУАцБГНЧ ЙйИЅГЛНУАцПЌБИМв РЬСиЧр. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (2017-9-25)