EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Heterotopic gastric mucosa of the esophagus. 식도 이소성 위점막. inlet patch] - 終
[Heterotopic gastric mucosa of the esophagus. 식도 이소성 위점막. inlet patch] - 終

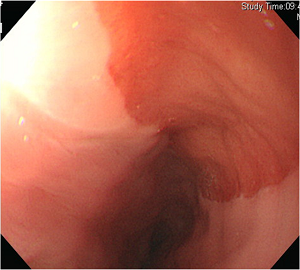
위 환자 inlet patch 조직검사에서 columnar epithelium이 확인됨.
고령환자의 상부식도에서 발견된 병변으로 조직검사에서 heterotopic gastric mucosa가 확인됨. 고령 환자에서 이 정도의 병소는 조직검사를 하지 않아도 좋을 것 같습니다.
![]() 1. Introduction
1. Introduction
Heterotopic gastric mucosa에 대하여 생각해 봅니다. 대부분의 내용이 2004년 American Journal of Gastroenterology의 리뷰에 잘 정리되어 있습니다. 요점은 리뷰의 introduction에 있습니다. 아래에 그대로 옮깁니다.
Heterotopic gastric mucosa (HGM) is frequent in the cervical esophagus, but most carriers are asymptomatic. Nevertheless it can be responsible for local morphologic alterations (e.g., webs, strictures, ulcers, fistula) causing local symptoms (especially pain and dysphagia). Furthermore, in exceedingly rare cases, HGM can be the origin of malignant progression to cervical esophageal adenocarcinoma.
HGM is not exclusively found in the esophagus as it has also been described in other localizations throughout the gastrointestinal tract, like the tongue, the duodenum, the jejunum, the gall bladder, and the rectum.
The extent of HGM can vary from tiny microscopic foci to macroscopically visible area of red or salmon-colored velvety patches. Predominant localization of esophageal HGM is the region immediately below the upper esophageal sphincter. Such patches of macroscopically visible HGM are also called "inlet patches."
관련하여 몇 가지를 말씀드리고 싶습니다.
1) 먼저 용어입니다. Heterotopic gastric mucosa 중 상부식도에 위치하고 macroscopic한 병변을 inlet patches라고 합니다. 그러니까 내시경에서 상부식도에서 보이는 것은 inlet patch라고 부르는 것은 타당한 일입니다.
2) Inlet patch는 증상을 일으킬 수 있습니다. 물론 궤양이나 암도 포함됩니다. 그러나 어디까지나 가능성 수준입니다. 리뷰 저자도 can 혹은 in exceedingly rare cases 라는 표현을 사용하고 있습니다.
3) 육안적으로 특별한 점이 없는 inlet patch에서 조직검사까지 할 필요는 없을 것 같습니다. 물론 inlet patch에서도 암이 발생할 수 있습니다. 저는 30년 내시경 의사로 살면서 딱 한 명 보았습니다. 그것도 제가 진단한 것이 아니고 집담회에서 본 것이었습니다. 그만큼 흔치 않습니다.
4) 위암 검진이 주 목적인 내시경 검사에서 우연히 발견된 inlet patch를 결과지에 쓸 필요가 있을지 고민입니다. 각자 판단에 따라 적절히 하시면 되겠습니다. 저는 보통 쓰지 않고 있습니다.
![]() 2. Velvet-like surface. 용어의 역사
2. Velvet-like surface. 용어의 역사
정확한 이해를 위해서는 역사를 알아야 합니다. 저는 오래된 책을 찾아보는 것을 좋아합니다. 이번에도 우리나라 최초의 내시경책(번역서임)을 참고해 보았습니다.
속편한 내과의 조성락 선생님께서 성분도병원 내과과장으로 계실 때 번역한 '소화관 내시경 진단 TEXT (1)' 32쪽입니다. 제가 내시경을 처음 배운 책입니다. 민영일 교수님 책(orange book이라고도 부릅니다)이 나오기 전에는 유일한 내시경 참고서였습니다.
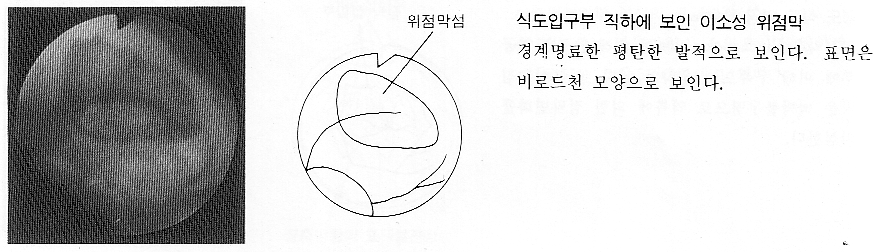
"식도입구부 직하에 보인 이소성 위점막. 경계명료한 평탄한 발적으로 보인다. 표면은 비로드천 모양으로 보인다"라는 설명이 붙어 있었습니다. 비로드가 무엇일까요? 비로드의 어원은 포르투갈어 Velludo라고 합니다. 영어로는 Velvet입니다. 결국 "식도 상부에 경계가 명료한 발적부가 있는데 그 표면은 벨벳같다" 정도의 의미입니다.
비로드와 비슷한 말로 '골덴'이 있습니다. 이는 골이 가는 면 비로드를 말합니다. 골덴은 영어로 Corded velveteen 또는 Corduroy입니다. 골덴은 일본에서 만든 합성어입니다. Corded 또는 Corduroy의 머리말인 콜(cor)에 天(하늘 천)을 합한 것인데 天의 일본 발음이 덴이라고 합니다. 왜 갑자기 天이 나왔냐고요? 비로드는 한문으로 천아융(天鵝絨)입니다. 요약하면 아래와 같습니다.
골덴 = Corded velveteen = Cor + 天 = 가는 면 비로드 = 가는 면 벨벳
![]() 3. Prevalence
3. Prevalence
Inlet patch가 얼마나 흔할까요? 앞서 소개한 리뷰 (Am J Gastroenterol 2004)에는 이런 말이 있습니다.
In endoscopic studies, HGM patches are found in 0.1-10% of the cases, but frequency tends to be clinically underestimated...... The region is quickly passed protruding the endoscopoe over the sphincter's resistance and only by gently withdrawing the instrument can an inlet patch be detected.
내시경의사의 입장에 따라 inlet patch의 진단율은 크게 달라집니다. 이 점에서 레바논의 한 연구(J Clin Gastroenterol. 2007)는 흥미롭습니다. Inlet patch에 관심이 많은 의사가 내시경을 하면 2.6%정도 발견되는데 (inlet patch에 특별한 관심이 없는) 보통 의사들이 내시경을 하면 그 빈도가 0.4%밖에 되지 않았습니다. 그렇습니다. 관심있으면 보이고 그렇지 않으면 보이지 않습니다.
학회나 세미나의 어떤 강의 후에 갑자기 prevalence가 증가하는 병이 있습니다. 역류성 식도염이나 바렛식도 같은 것이 그렇습니다. EndoTODAY 때문에 갑자기 inlet patch의 진단이 많아질까 걱정입니다. 별로 중요하지도 않은데...
![]() 4. Helicobacter
4. Helicobacter
Inlet patch에는 헬리코박터가 살 수도 있습니다. 터키의 어떤 연구자가 그 빈도를 잰 적도 있군요 (Int J Clin Pract. 2009). Dysphagia와 관련이 있다는 것인데... 간혹 PPI를 쓰고 dysphagia가 좋아졌다는 환자가 있는데 약간 관련되었을지도 모르겠습니다. 큰 inlet patch를 가진 환자에서는 한번 고려해 볼 수 있을까요?
Inlet patch의 헬리코박터 colonization은 위에 헬리코박터가 있는 경우에만 발견된다고 합니다 (Dig Dis Sci 1993).
![]() 5. Pathogenesis
5. Pathogenesis
Inlet patch는 보통 congenital이라고 생각됩니다. 간혹 acquired라는 주장도 있지만 (Dig Dis. 2000) 소수의견인 것 같습니다.
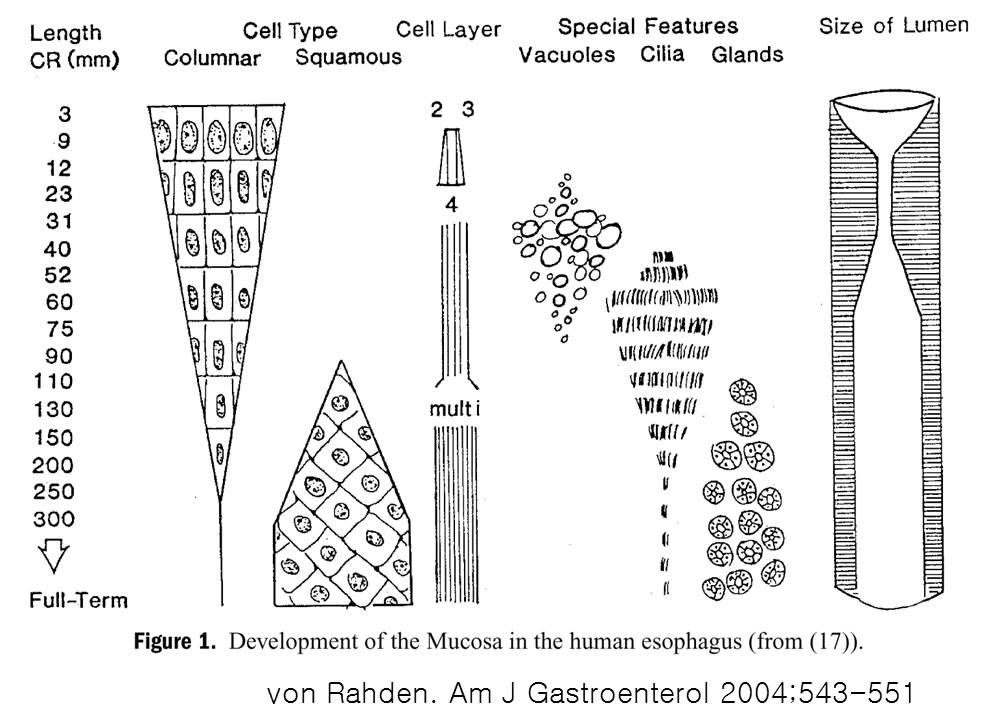
발생학적으로 columnar epithelium으로 덮혀있던 식도가 squamous epithelium으로 바뀌면서 일부 남은 부분이 inlet patch라는 설이 지배적입니다. 2004년 American Journal of Gastroenterology의 리뷰에서 옮깁니다.
The columnar epithelium of the embry's esophagus is generally replaced by squamous cell epithelium. This process starts in the midesophagus and extents vertically in both directions with the cervical esopahgus being the last region to get stratified. If the squamous epithelization remains incomplete, the persisting columnar-lined area differentiates to HGM.
![]() 6. Acid is the Evil Agent
6. Acid is the Evil Agent
Inlet patch는 web이나 stricture를 일으킬 수 있습니다. Plummer Vinson 증후군의 esophageal web도 inlet patch에 의한 것이라는 주장도 있습니다 (Dig Dis Sci 1979). Pain이나 odynophagia도 가능합니다. Laryngopharyngeal reflux symptoms 과 관련되었다는 주장도 있습니다 (Eur Arch Otorhinolaryngol 2010).
이와 같은 inlet patch에 의한 합병증은 위산과 관련된 것 같습니다. 앞서 소개한 리뷰 (Am J Gastroenterol 2004)에는 이런 말이 있습니다. The clinical importance of HGM is limited to symptomatic cases. Symptoms, signs, and complications are acid-related. 흥미롭게도 이와 같은 내용이 담긴 문단의 제목이 'Acid is the Evil Agent'였습니다.
제가 보는 임상적 의미는 이렇습니다. Web이나 stricture는 가능하다고 생각합니다. 그러나 laryngopharyngeal reflux (LPR)는 다를 수 있습니다. LPR symptoms으로 PPI를 사용한 후 증상이 호전되었다면, 이는 위산역류가 줄었기 때문일 수도 있고 inlet patch에서 산분비가 줄었기 때문일 수도 있습니다. 둘을 정확히 구분하는 것은 불가능한 일입니다. 다만 inlet patch의 산분비 감소가 중요하다면 PPI 투약 후 상부식도증상이 즉시 좋아져야 할 것입니다. 사실은 그렇지 않습니다. 그렇다면 이것이 뜻하는 것은 무엇일까요?
제 주장과 달리 2009년 Gastroenterology에는 Argon plasma coagulation of cervical heterotopic gastric mucosa as an alternative treatment for globus sensations라는 흥미로운 논문이 발표된 바 있습니다. 저도 어떻게 의미를 부여해야 할지 잘 모르겠습니다. 추시가 필요한 부분입니다.
![]() 7. Inlet patch and upper esophageal adenocarcinoma
7. Inlet patch and upper esophageal adenocarcinoma
2011년 6월 12일 EndoTODAY에서 inlet patch가 암이 될 수 있는지 잘 모르겠다고 말씀드린 바 있습니다. 당시까지만 해도 한 증례도 경험한 적이 없었기 때문입니다. 어쩔 수 없이 문헌(Am J Gastroenterol 2004)만 소개드렸습니다.
The low frequency of malignant transformation of HGM in the cervical esophagus as compared to Barrett's esophagus in the distal esophagus suggests that it may not be regarded as a premalignant lesion. Malignant procression of HGM is - compared to its high prevalence - an exceedingly rare and sporadic event.
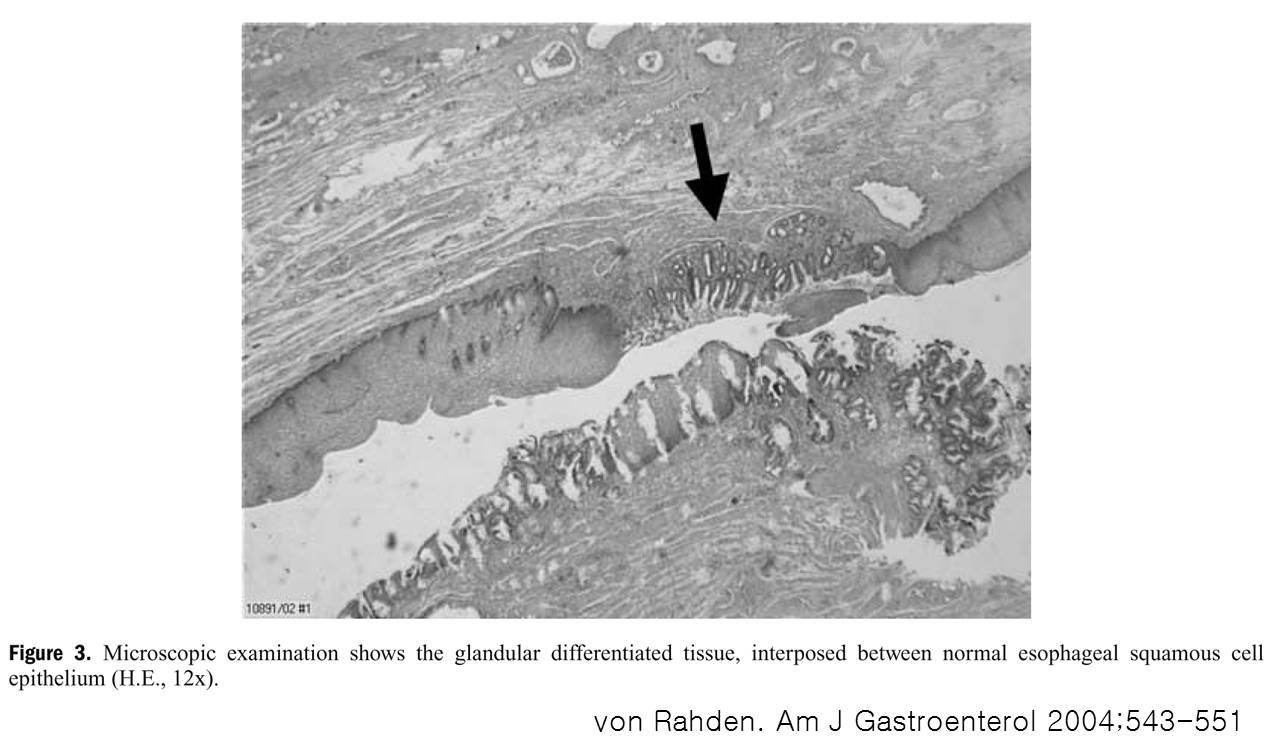
이후 몇 증례를 경험하였습니다. 상부식도선암 주변에 정상적인 inlet patch 부분이 있었으므로 inlet patch에서 시작한 상부식도선암으로 추정하였던 증례들입니다. 물론 보다 진행된 상부식도선암도 inlet patch에서 시작했을 것으로 생각되지만, 정상 inlet patch가 보이지 않으면 직접적인 관련성을 말씀드리기 어려울 것 같습니다.
Inlet patch에서 시작된 상부식도선암. 수술을 시행하였음.
Tubular adenocarcinoma, moderately differentiated, arising in heterotopic gastric mucosa within esophageal diverticulum:
1) tumor size: 1.6x0.9 cm
2) extension to proper muscle layer
3) endolymphatic tumor emboli: not identified
4) perineural invasion: not identified
5) resection margins: free from carcinoma
6) no metastasis in 33 regional lymph nodes
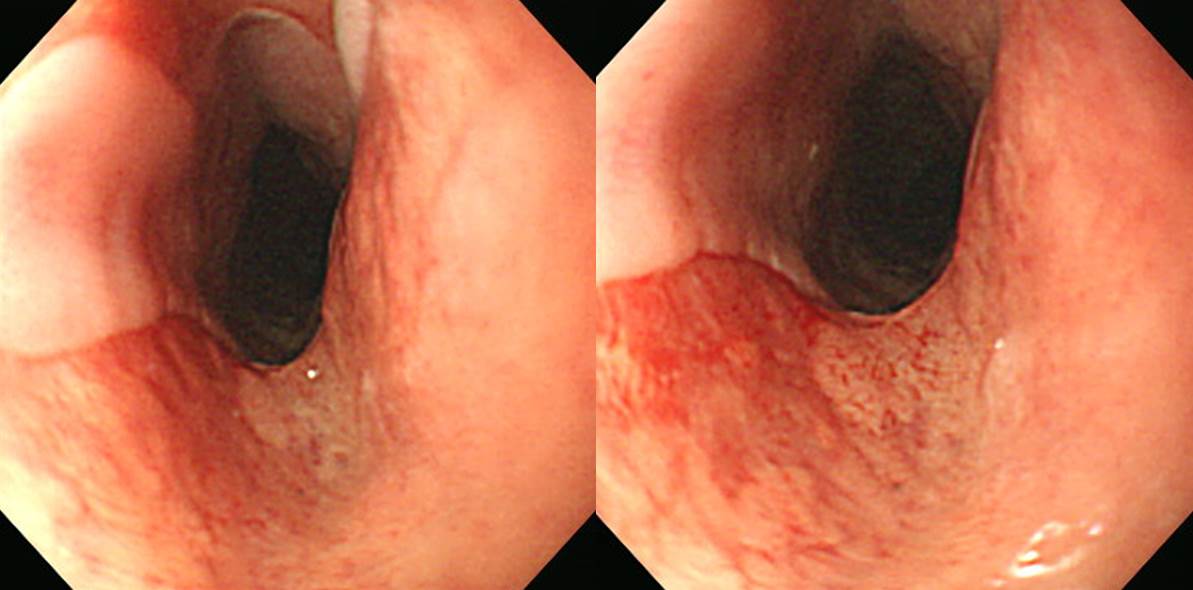
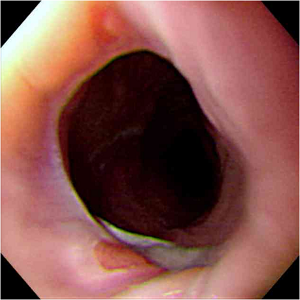
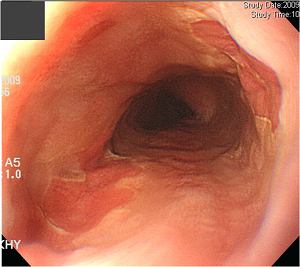
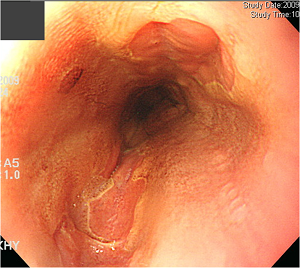
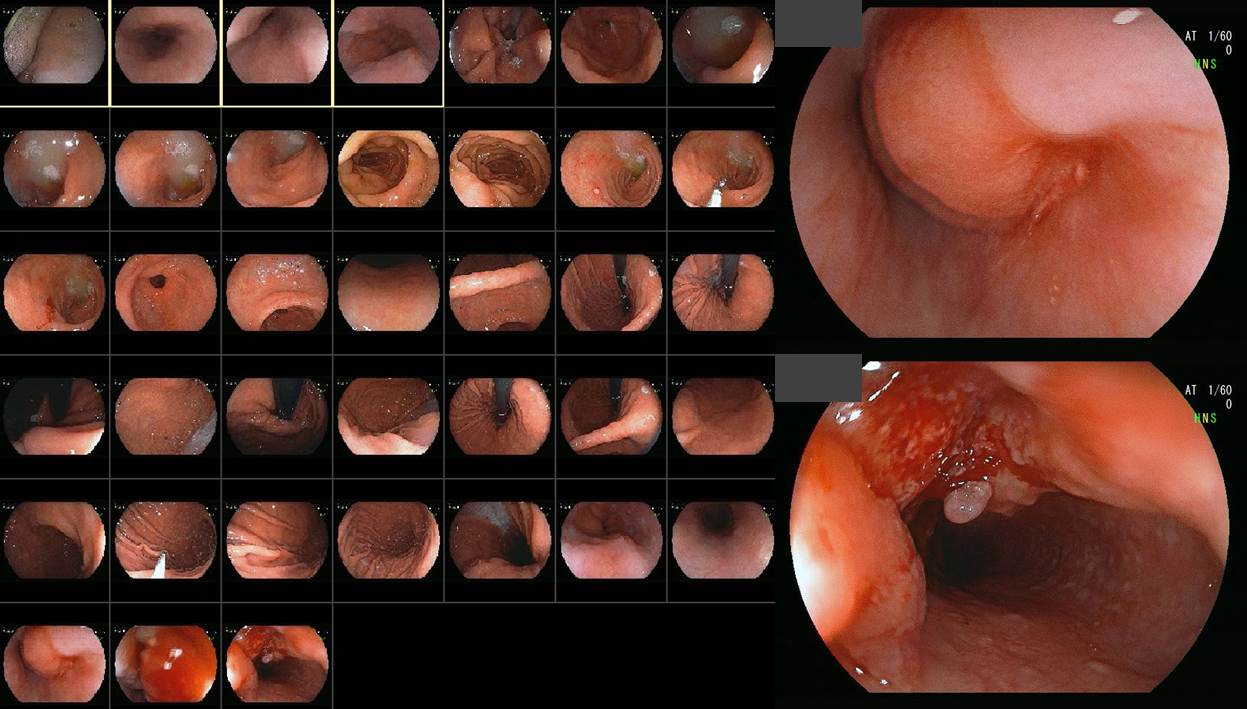
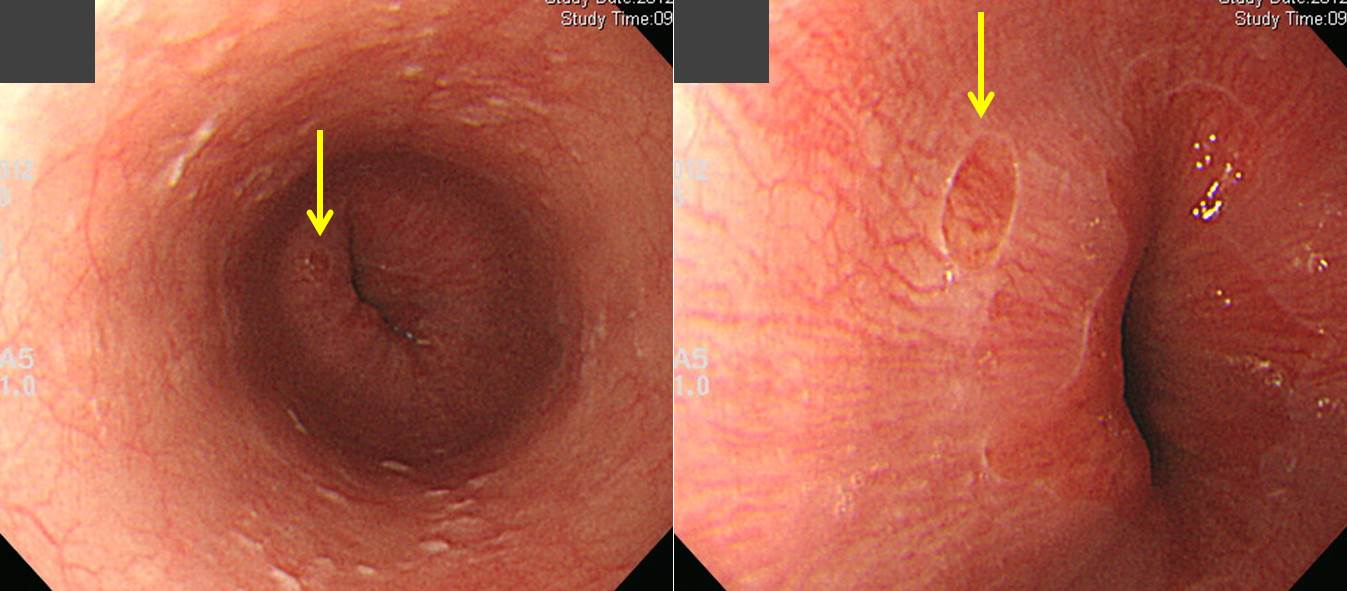
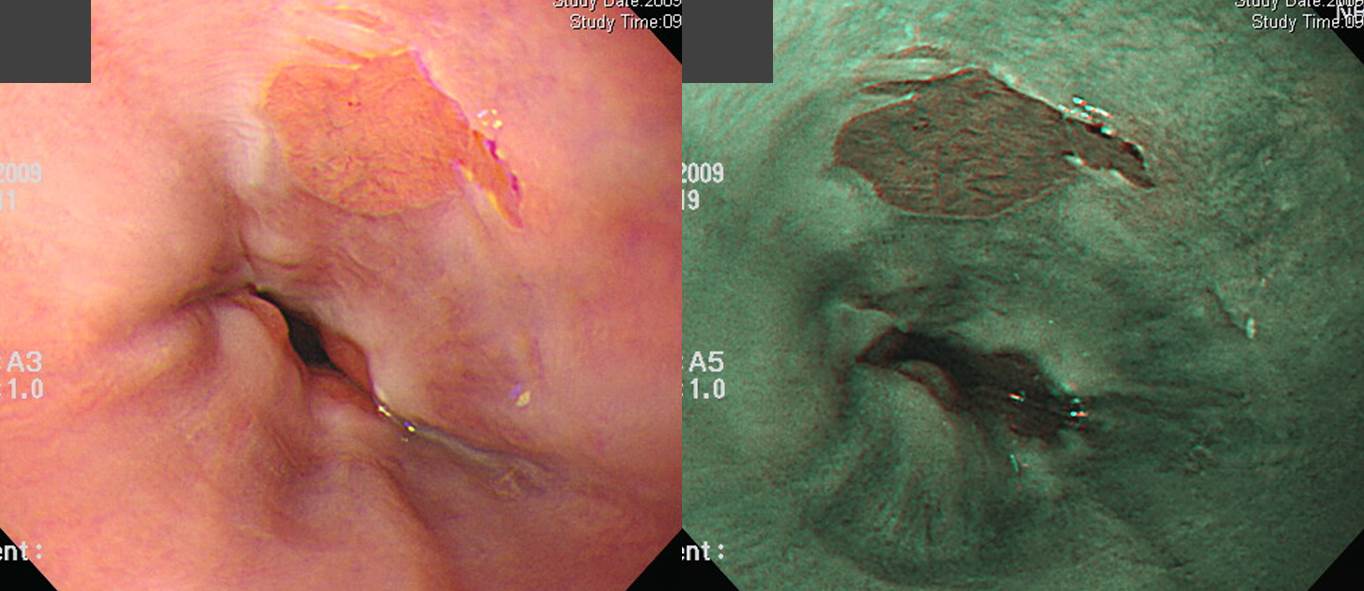
Neoadjuvant CCRT 후 병소가 소실되었고, 수술(3-field operation)을 시행하였는데 no residual tumor가 나왔습니다. 이 환자는 진단 측면에서 learning point가 있습니다. 처음 진단되었을 때의 내시경 사진(아래)을 잘 보시기 바랍니다. 내시경 삽입 과정에서는 암을 발견하지 못하였고, 내시경을 빼는 과정에서 암이 진단되었습니다. 상부식도는 매우 유명한 blind area입니다. 내시경을 천천히 제거하면서 자세히 관찰하지 않으면 상부식도 암은 놓치기 마렵니다. 내시경 천천히 뺍시다.
![]() 8. Proposed clinicopathologic classification (2011-6-13)
8. Proposed clinicopathologic classification (2011-6-13)
앞서 소개한 리뷰 (Am J Gastroenterol 2004)에서 제안된 식도 HGM의 분류를 소개합니다.
HGM I - asymptomatic
HGM II - symptomatic without morphologic changes (dysphagia/odynophagia)
HGM III - symptomatic with morphologic changes (benigh complications: strictures, ulcers, webs, stenoses, fistula)
HGM IV - intraepithelial neoplasia (dysplasi)
HGM V - invasive adenocarcinoma
![]() 9. Inlet patch during screening endoscopy (2011-6-14)
9. Inlet patch during screening endoscopy (2011-6-14)
Screening endoscopy setting에서 inlet patch를 봐야 할까요? 상부식도증상이 있으면 모를까 별 증상이 없는 사람에서도 inlet patch를 꼭 봐야 할까요? 저는 이렇게 생각합니다. "그다지 중요하지 않은 것은 봐도 좋고 안 봐도 좋다. 다만 중요하지 않은 것을 보기 위하여 중요한 것을 안 보면 곤란하다. Screening endoscopy setting에서 inlet patch 여부를 찾는 것은 중요하지 않다. 다만 우연히 inlet patch를 보았을 때 그것이 무엇인지 알아야 하고 별로 중요하지 않다는 것을 간파할 수 있어야 한다."
봐도 그만 안 봐도 그만인 것을 무리해서 볼 필요는 없다고 생각합니다. 평범한 inlet patch를 보았을 때 보통 조직검사는 필요없습니다.
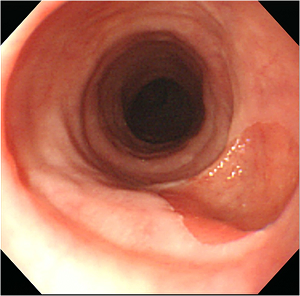
상부식도의 이소성 위점막 (inlet patch, heterotopic gastric mucosa)은 보통 둥근 모양입니다. 그러나 semi-circular 혹은 circular한 경우가 있습니다. 조직검사는 acanthotic squamous epithelium and gastric mucosal showing chronic gastritis, active with intestinal metaplasia로 나왔습니다. 추적 관찰만 시행할 예정입니다.
![]() 10. 하부식도 heterotopic gastric mucosa
10. 하부식도 heterotopic gastric mucosa
[2017-5-10. 애독자 질문]
상부식도에 columnar mucosa가 velvet 처럼 보이면 inlet patch라고 부르는데요, 하부 식도에 비슷한 것이 보이면 outlet patch라고 부르는 것입니까?
[2017-5-10. 이준행 답변]
재미있는 아이디어입니다만, outlet patch라고 부르지는 않습니다. 그냥 하부식도 heterotopic gastric mucosa 혹은 하부식도 이소성 위점막 (ectopic gastric mucosa)이라고 부르는 것이 보통입니다.
발생학적으로 식도는 아주 초기에는 columnar epithelium인데, 점차 식도 중앙부터 상하로 squamous epithelium으로 대치된다고 합니다. 따라서 양쪽 끝인 상부식도와 하부식도에 약간 columnar epithelium이 남을 수 있는데 이를 heterotopic gastric mucosa라고 부르는 것입니다.
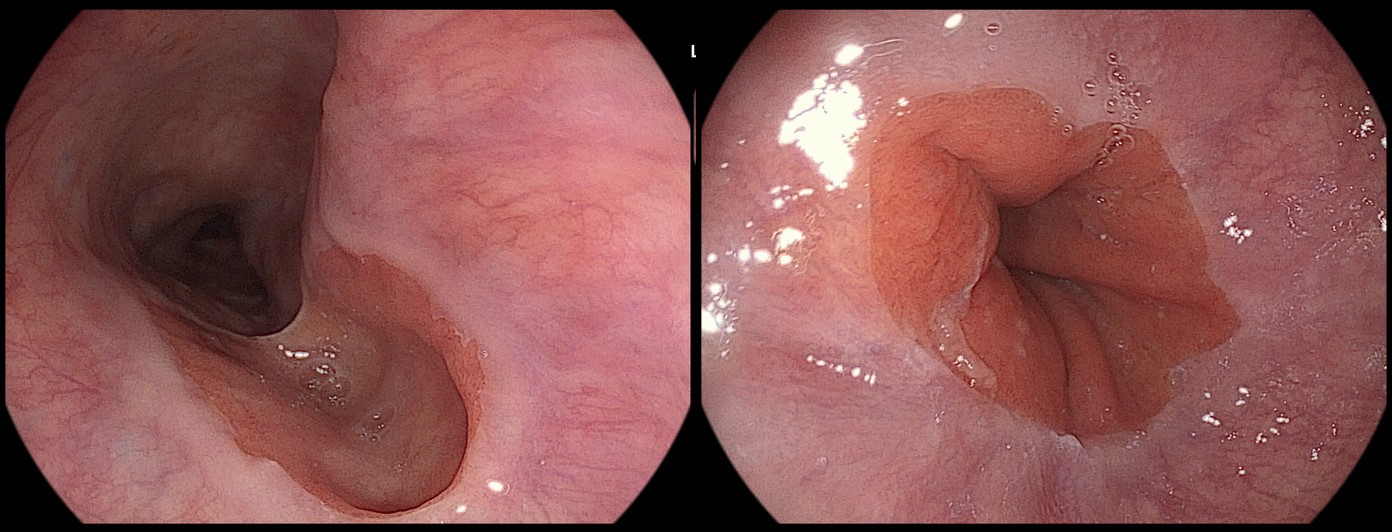
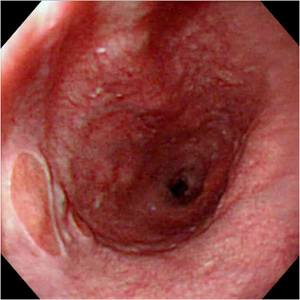
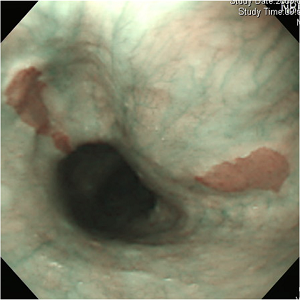
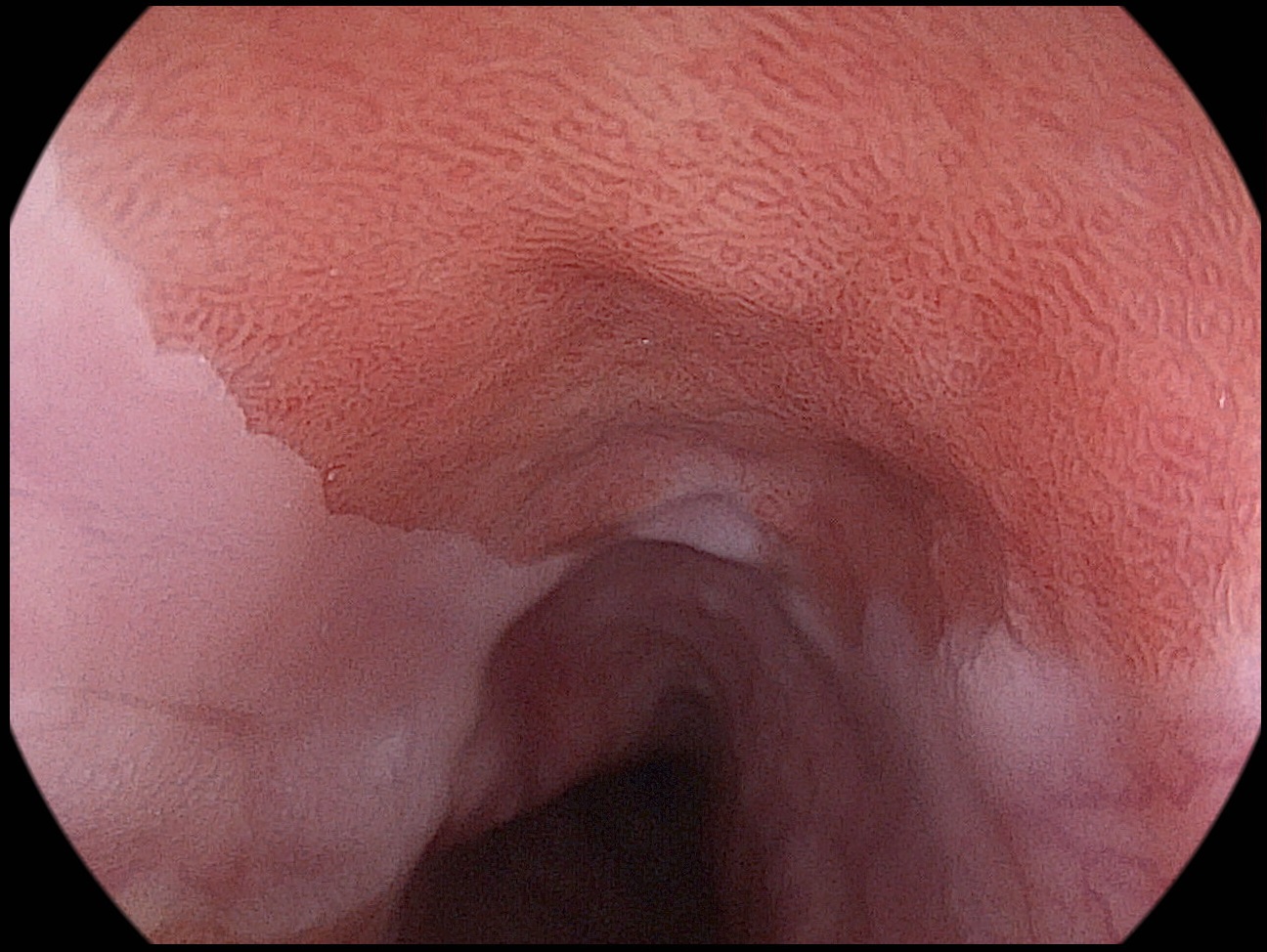
전형적인 내시경 소견은 아래와 같습니다. 하부식도에서 전형적인 heterotopic gastric mucosa가 보이면 좋은 사진 한 장 남겨놓고 조직검사는 하지 않아도 좋습니다. 걱정되면 1-2개 정도 해도 상관은 없습니다.
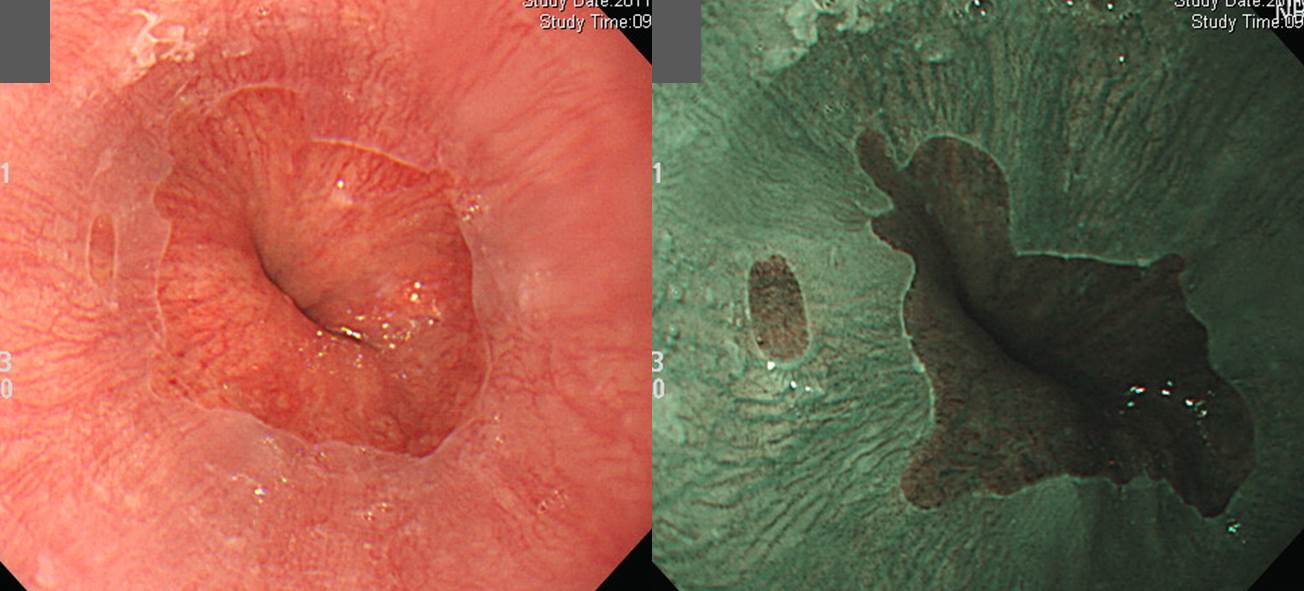
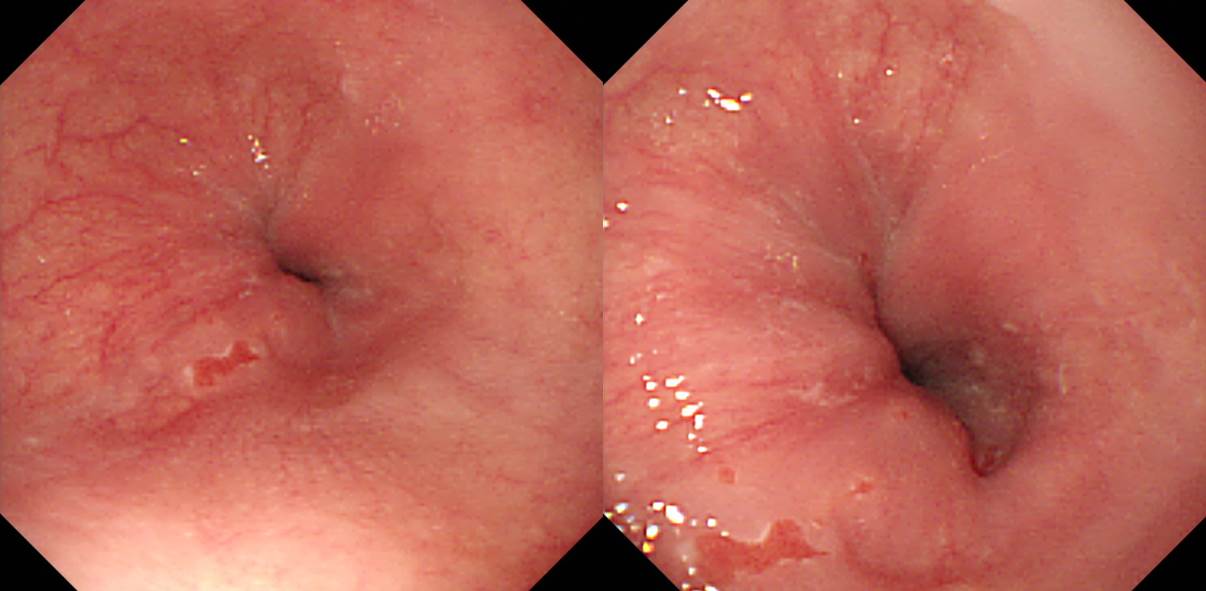
Heterotopic gastric mucosa로 부르고 넘어갈지 short tongue-like Barrett을 의심해야 할지 고민입니다. 저는 전자를 택했습니다. 10년 전에도 동일했습니다.
이소성 위점막은 far distal esophagus에 위치하는 것이 보통이지만, 간혹 좀 더 위쪽에서 발견되기도 합니다. 중부식도에서도 보이기도 합니다. 과거 어떤 선생님께 드린 답변을 소개합니다.

바렛식도이고 암이 되니 1-2개월 후 내시경 해보자고 듣고 겁에 질려 오신 환자로 바렛식도 아니므로 걱정하지 마시고 1년 후 내시경 하시도록 추천하였습니다.
![]() [FAQ]
[FAQ]
[2014-11-5. 애독자 질문]
얼마전에 소화불량을 주소로 검사한 60대 남성입니다. 상절치로부터 20cm에 heterotopic gastric mucosa로 생각되는 부위가 있었는데, 경한 요철이 동반되어 있어 생검을 했습니다. 조직 결과는 squamous cell carcinoma였습니다. Heterotopic gastric mucosa이면 adenocarcinoma일 것 같은데, base 병변이 이소성 위점막이 아닌 것인지, 아니면 동시에 존재하는 것인지 궁금합니다.

[2014-11-5. 이준행 답변]
좋은 질문 감사합니다. 그런데 사진만으로 자신있는 답변은 어렵다고 생각됩니다. 일견 heterotopic gastric mucosa의 전형적인 velvet같은 부드러운 부위는 없어 보입니다. 혹시 그냥 squamous cell carcinoma가 얕고 넓게 생긴 것은 아닐까요?
[2017-5-13. 애독자 질문]
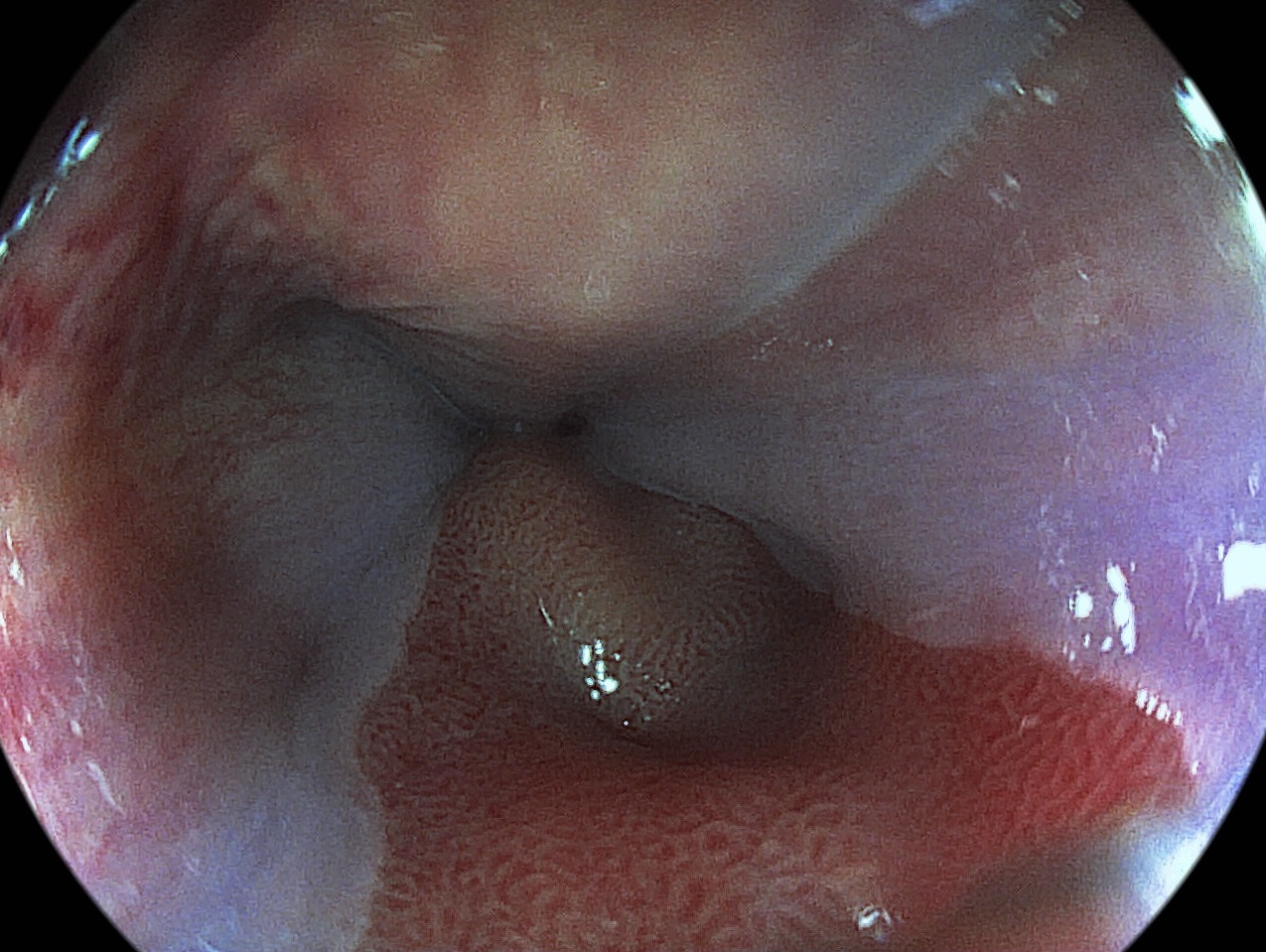
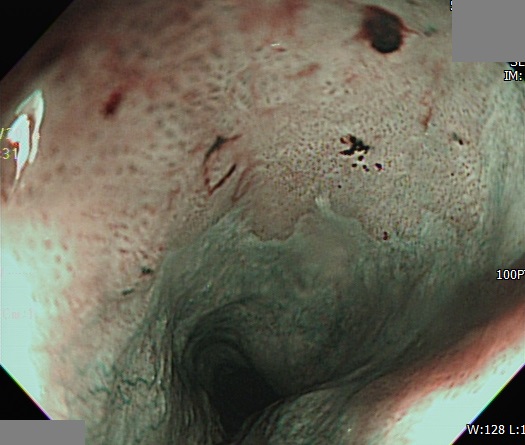
안녕하세요~ 교수님께 많은 도움 받고 있는 개원의입니다. 검진 내시경 GEJ 부위 사진입니다.

9시 부분에 위점막이 확장되어 보이는 부분을 어떻게 표현해야 할 지 애매합니다. 미란, 염증, 발적 소견이 없는 것으로 보아 바렛 병변은 아닌것 같은데 어떻게 report를 하는 것이 가장 적당할까요? (식도염 증상도 전혀 없는 분입니다.) 항상 저희같은 민초들의 고민도 함께해주셔서 감사드립니다!!
[2017-5-13. 이준행 답변]
한쪽 방향으로만 자라난 Ultra short segment 바렛식도라고 볼 수도 있으나 제 생각에는 ectopic gastric mucosa가 SC junction과 연결된 모양인 것 같습니다. 임상적 의의는 거의 없다고 보셔도 좋을 것 같습니다.
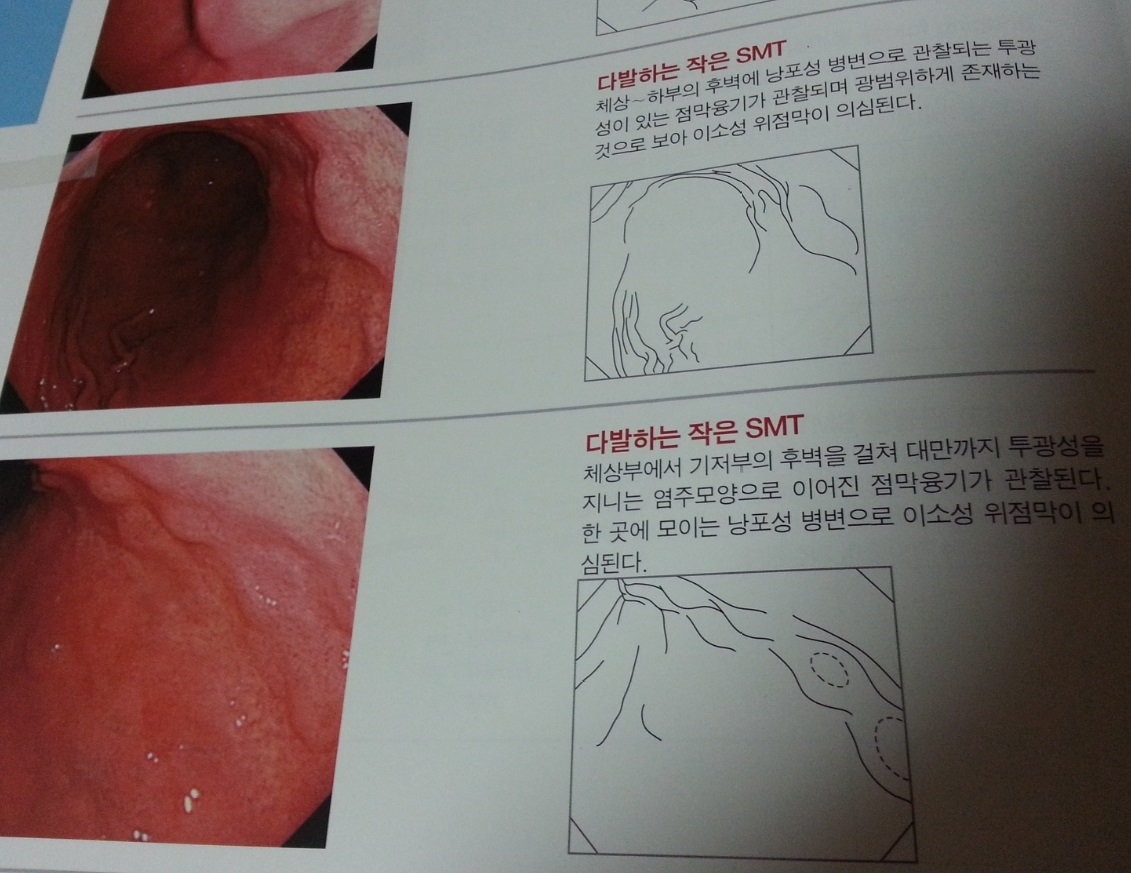
[2014-9-1. 애독자 질문] 내시경 책을 보다가 궁금점이 생겨서 문의드립니다. 첨부한 사진에도 나오지만 위내 점막하종양인데 이소성 위점막이라는 말을 할 수 있는 건가요? ^^;; 위외의 다른 장기에 있을때 이소성 위점막이라는 용어를 쓸것같은데... 폰으로 찍은 사진이라 화질이 나쁘네요. 죄송합니다.
[2014-9-2. 이준행 답변] 좋은 질문입니다. Heterotopic gastric mucosa in the esophagus 혹은 heterotopic gastric mucosa in the duodenum은 들어보셨을 것입니다. 그런데 heterotopic gastric mucosa in the stomach이라는 것도 있습니다. 위점막이 위점막하층에 위치하는 경우입니다. 당연히 점막하종양처럼 보입니다. 일전에 삼성서울병원에서 heterotopic gastric mucosa에서 시작한 위암 2예를 보고한 적도 있습니다. 그 증례보고의 discussion 부분을 옮깁니다.
Heterotopic gastric mucosa in the gastric submucosa is reported to occur in 3.0 to 20.1% of resected stomach specimens. Although the etiology of this disease is unknown, mucosal infoldings bulging in the submucosal tissue have been demonstrated, probably as a result of inflammation or ulceration. In addition, the histologic characteristics of heterotopic gastric mucosa with cystic expansion are very similar to gastritis cystic polyposa, but gastritis cystric polyposa is known to occur at anastromotic sites after gastrectomy. Heterotopic gastric mucosa is thought to occur due to infiltration of mucosa through muscularis mucosa cracks or defects by repeated erosion. While heterotopic gastric mucosa occurs due to movement of gastric mucosa to the submucosa through the muscularis mucosa of weak resistance, the muscularis mucosa of heterotopic gastric mucosa is connected with normally located muscularis mucosa, and such a characteristic suggests that it is a true mucosal diverticuli. Although it has not clearly been determined if heterotopic gastric mucosa is due to congenital or acquired causes, heterotopic gastric mucosa is found in 20.1% of gastric specimens from adults, but not in gastric specimens from children, thus it is thought to occur by acquired causes. Because heterotopic gastric mucosa is found primarily among adults in their 60s and is not found in autopsies of people <20 years of age, it is presumed to be due to repetitive inflammation.
![]() [References]
[References]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.