EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [KINGCA Week 2014 (Korea International Gastric Cancer Week)]
[KINGCA Week 2014 (Korea International Gastric Cancer Week)]


5월 15일부터 17일까지 대전에서 KINGCA (Korean International Gastric Cancer Week) 2014가 진행중입니다. 위암학회에서 준비한 국제학회입니다. 총회에서 미션과 비전이 발표되었습니다.
![]() [2014-5-15] Robotic surgery에 대한 심포지엄
[2014-5-15] Robotic surgery에 대한 심포지엄
로봇과 관련된 합병증은 어느 정도일까요? 대부분의 연구 결과는 복강경 수술과 비슷하다고 합니다. 걱정하였던 로봇에 unique한 합병증은 거의 없다고 하네요. 현재 로봇과 복강경을 비교하는 연구가 진행되고 있으니 결과를 기다려야 할 것 같습니다 (NCT01309256). 그러나 이러한 연구가 과연 타당한가에 대한 comment가 많았습니다. 저는 아래와 같은 질문을 했습니다. 분위기를 깨는 듯한 질문이라 조금 뒷골이 따갑기는 했지만...
Except for the money issue, robot gastrectomy is promising and quite safe and may be interesting for doctors. We can see more and more medical evidence. However, most discussions seems to be surgeon-oriented. I am an endoscopist doing endoscopic submucosal dissection. Patients can understand the advantage of ESD very easily. I am not sure what's the advantage of robot gastrectomy for the patients. So, my silly question is why so many patients are choosing robot gastrectomy.
한 연자의 결론은 다음과 같았습니다. "Robot gastrectomy in gastric cancer is still controversial comparing to the conventional open and laparoscopic surgery. However, reported publications claim that this procedure is feasible and not inferior to conventional surgery. More strong evidence by clinical trials is required in the future."
그렇습니다. 현재까지 로봇과 복강경은 비슷한 결과를 보이고 있지만, 환자에게 특별한 잇점은 없어 보입니다. 이번 로봇 심포지엄을 다 듣고 난 소감을 정리하면 다음과 같습니다. "아직 변화는 없다. 복강경 수술이 가능하다면 복강경 수술이 최선이다."
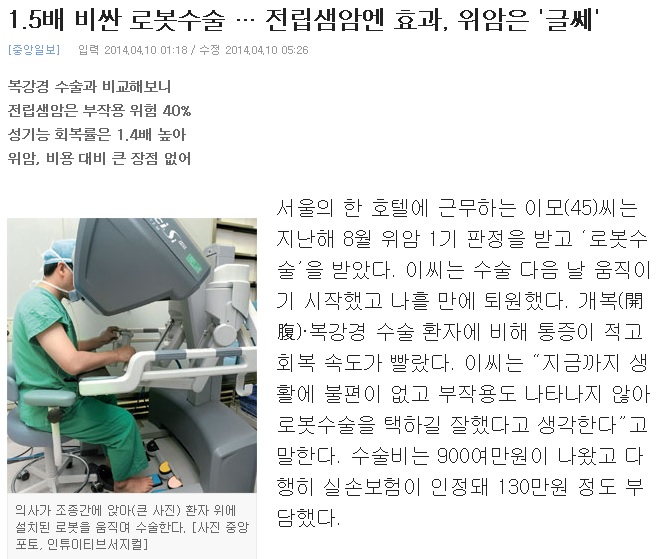
![]() [2014-5-16. 추가] 연구를 통하여 해결할 수 없는 문제도 있습니다. 로봇 위절제술과 복강경 수술을 비교한 여러 연구 결과는 impressive한 차이를 보여주지 못했습니다. NECA에서도 메타연구를 시행하여 비슷한 결과를 보였고, 여러 언론에서도 이 이슈를 다룬 바 있습니다 (아래 그림을 click해 주세요). 그러나 외과의사들이 느끼는 장점은 무엇일까요? 몇 분과 토론해 보았습니다.
[2014-5-16. 추가] 연구를 통하여 해결할 수 없는 문제도 있습니다. 로봇 위절제술과 복강경 수술을 비교한 여러 연구 결과는 impressive한 차이를 보여주지 못했습니다. NECA에서도 메타연구를 시행하여 비슷한 결과를 보였고, 여러 언론에서도 이 이슈를 다룬 바 있습니다 (아래 그림을 click해 주세요). 그러나 외과의사들이 느끼는 장점은 무엇일까요? 몇 분과 토론해 보았습니다.
여러분과 장시간 토론 끝에 제가 내린 결론은 "로봇 위절제술을 버릴 수는 없다"는 것입니다. 어떻게든 비용 문제를 해결하고 (독점구조를 깨야 합니다), 국민이나 정책 당국자를 설득할 수 있는 논리를 개발하여 불씨는 살려둘 필요가 있을 것 같습니다.
[2014-5-16. 애독자 (K대 소화기내과 교수) 의견] 보내주신 글 감사히 읽고 있습니다. 저는 로봇 수술에 대해 상당히 경계하는 의견을 가지고 있습니다. 외과 의사들이 이런 저런 장점을 나열하지만, 대부분의 장점들은 의사 위주의 장점입니다. 나이 먹어서도 수술을 할 수 있고, 보조자 없이도 수술할 수 있고, 등등... 하지만, 환자 위주의 장점들은 그렇게 뚜렷하지 않은 것 같습니다. 일부 해부학적으로 로봇 수술이 유리하다는 데에는 동의합니다. 따라서, 의사 위주의 장점들은 주로 시스템으로 해결을 하거나 수술 보조 전문 인력을 쓰거나 등등... 다른 방법으로 극복할 수 있다고 생각합니다. 문제는 적응증인 것 같습니다. 로봇 수술이 유리한 일부 수술도 있지만, 많은 병원에서 무분별하게 고가의 수술을 넓은 적응증으로 유행처럼 많은 환자들에게 적응하고 있는 것이 문제라고 생각합니다. 로봇수술이 더 적응이 되는 꼭 필요한 환자에게 시술한다면 가장 바람직할 것 같지만, 현실은 그렇지 않은 것 같아 조금 아쉽습니다.
[2014-5-16. 이준행 답변] 좋은 의견 감사합니다. 저도 비슷하게 생각합니다. 환자 입장의 장점은 약합니다. 일부 외과의사들이 의사입장에서 느끼는 장점을 말하고 있을 뿐입니다. 동의합니다. 그렇다고 그냥 몽땅 버리기는 아깝다는 것입니다. 잘만 쓰면 필요한 경우가 없는 것은 아니니까요. 가격만 낮아진다면 복강경과 공존할 수 있지 않을까요? 제가 너무 순진한가요? 여하튼 좋은 의견 감사합니다.
![]() 스승의 날입니다. 은사님을 찾아뵙지 못해 마음이 무겁습니다.
스승의 날입니다. 은사님을 찾아뵙지 못해 마음이 무겁습니다.
어제 오늘 사이에 꽃과 와인과 편지를 받았습니다. 정말 즐겁습니다. 편지를 소개합니다. 손편지는 늘 반갑습니다.
![]() 15일 목요일 오후 3시 20분. Education session에서 경북대 전성우 교수께서 ESD전반에 대한 강의를 하셨습니다. 저는 아래와 같이 comment했습니다. 그렇습니다. ESD하다가 환자가 죽을 수 있습니다. 우리는 이 점을 잊지 말아야 합니다.
15일 목요일 오후 3시 20분. Education session에서 경북대 전성우 교수께서 ESD전반에 대한 강의를 하셨습니다. 저는 아래와 같이 comment했습니다. 그렇습니다. ESD하다가 환자가 죽을 수 있습니다. 우리는 이 점을 잊지 말아야 합니다.
I agree that there is no published report on ESD-related mortality. Physicians usually don't report their failures. But there are some ESD-related mortalities in the real clinical practice. I saw an abstract in a conference about ESD-related death, and there must be some more hidden cases. We need to collect data on ESD-related severe complications. ESD is not a mortality-free procedure.

![]() [5월 16일 금요일 오전 7시 30분 Meet the professor session]
[5월 16일 금요일 오전 7시 30분 Meet the professor session]

아산병원 정훈용 선생님께서 How to reduce selection bias in ESD에 대하여 흥미로운 강의 후 동영상을 보여 주셨습니다. 7명이 모여 열띤 토론을 한 즐겁고 유익한 시간이었습니다. 아래는 정훈용 교수님의 key slide 내용을 옮긴 것입니다.
1) Meaing of selection bias
2) Causes of selection bias? Pre-ESD
3) Causes of selection bias? Post-ESD
4) Regarding endoscopists' skill
5) 정훈용 선생님의 comment
![]() [5월 16일 금요일 오전 8시 30분 ESD 심포지엄]
[5월 16일 금요일 오전 8시 30분 ESD 심포지엄]
1) Treatment outcomes of high grade dysplasia in Korea. 연세대학교 김지현
저는 아래와 같은 질문을 했습니다. "13%of HGD was actually a caner in the ESD specimen. How many of them required surgery? By the experience in my institution SMC, surgery rate for this group of patients (HGD in biopsy and cancer in ESD specimen) was 12.9%."
정훈용 교수님께서는 chromoendoscopy 후 오히려 병변을 underestimation하여 lateral margin에 tumor involvement가 있을 수 있다는 코맨트를 하셨습니다. 아산병원에서 HGD로 ESD한 환자 315명 중 53%인 166명이 암으로 최종진단되었다고 합니다. 아산병원 53%, 연세대병원 44.6%, 삼성서울병원 34.1%인 셈입니다. 병원간에 약간의 차이는 있지만 아주 크지는 않았습니다.
2) Pathologic interpretation of difficult ESD specimen. 을지대학교 병리과 강동욱
이 질문을 하고 싶었는데 시간이 없어서 못 했습니다. 안타깝습니다. "You classified mucinous adenocarcinoma as undifferentiated type. Then mucinous adenocarcinoma cannot be a candidate for ESD. However, there is a report that mucinous adenocarcinoma can be classified into high grade and low grade. In this scheme, low grade mucinous adenocarcinoma can be classified into differentiated type, and ESD can be done for this low grade mucinous adenocarcinoma."
3) Current issues in ESD. 울산대학교 정훈용
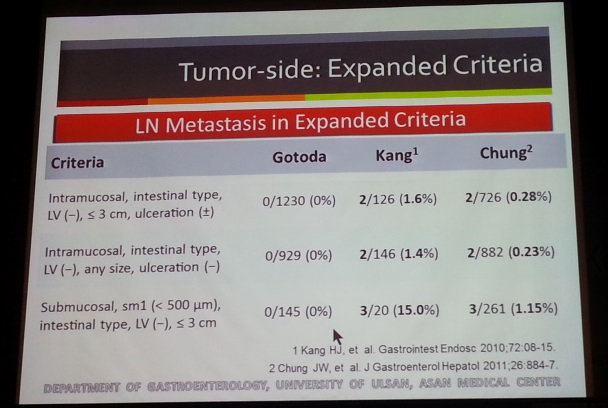
Expanded indication에서 림프절 전이가 없다는 일본 데이타와 달리 우리나라 데이타에서는 적지만 일부에서는 분명히 림프절 전이가 있습니다. 실제로 SM1으로 ESD후 간전이가 발생한 환자가 있습니다.
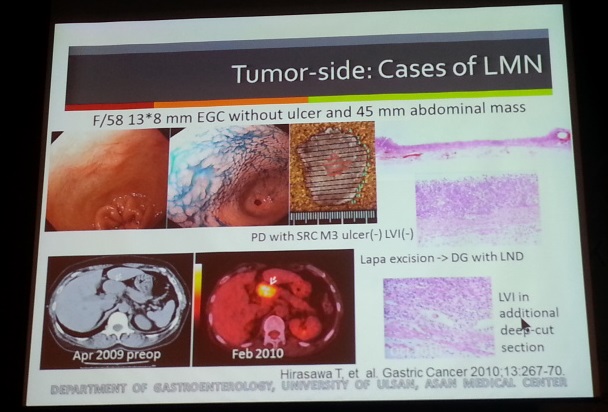
일본에서 Suzuki 등은 Endoscopy 2013:45;93-97에 submucosal cancer로 ESD 후 사망한 환자 4명을 보고했습니다. 모두 non-curative resection이었습니다. 이 중 lymphatic invasion이 있던 2명은 수술을 했는데도 사망하였습니다. 역시 lymphatic invasion은 매우 중요한 risk factor입니다.
![]() [2014-5-16. ESD session에서의 이준행 강의]
[2014-5-16. ESD session에서의 이준행 강의]
2014년 5월 16일 오늘 오전 첫 세션에 제가 Differences between pre-ESD and post-ESD diagnosis라는 제목으로 강의할 예정입니다. 일부 내용을 소개합니다. 우리나라에서 우리나라 사람을 대상으로 영어로 강의하려니 무척 힘듭니다. 허울 좋은 국제학회라는 시스템을 빨리 없애야 할 것 같습니다. 저는 우리나라 사람끼리 우리말로 토론하고 싶습니다. 무슨 식민지도 아니고 왠~~~
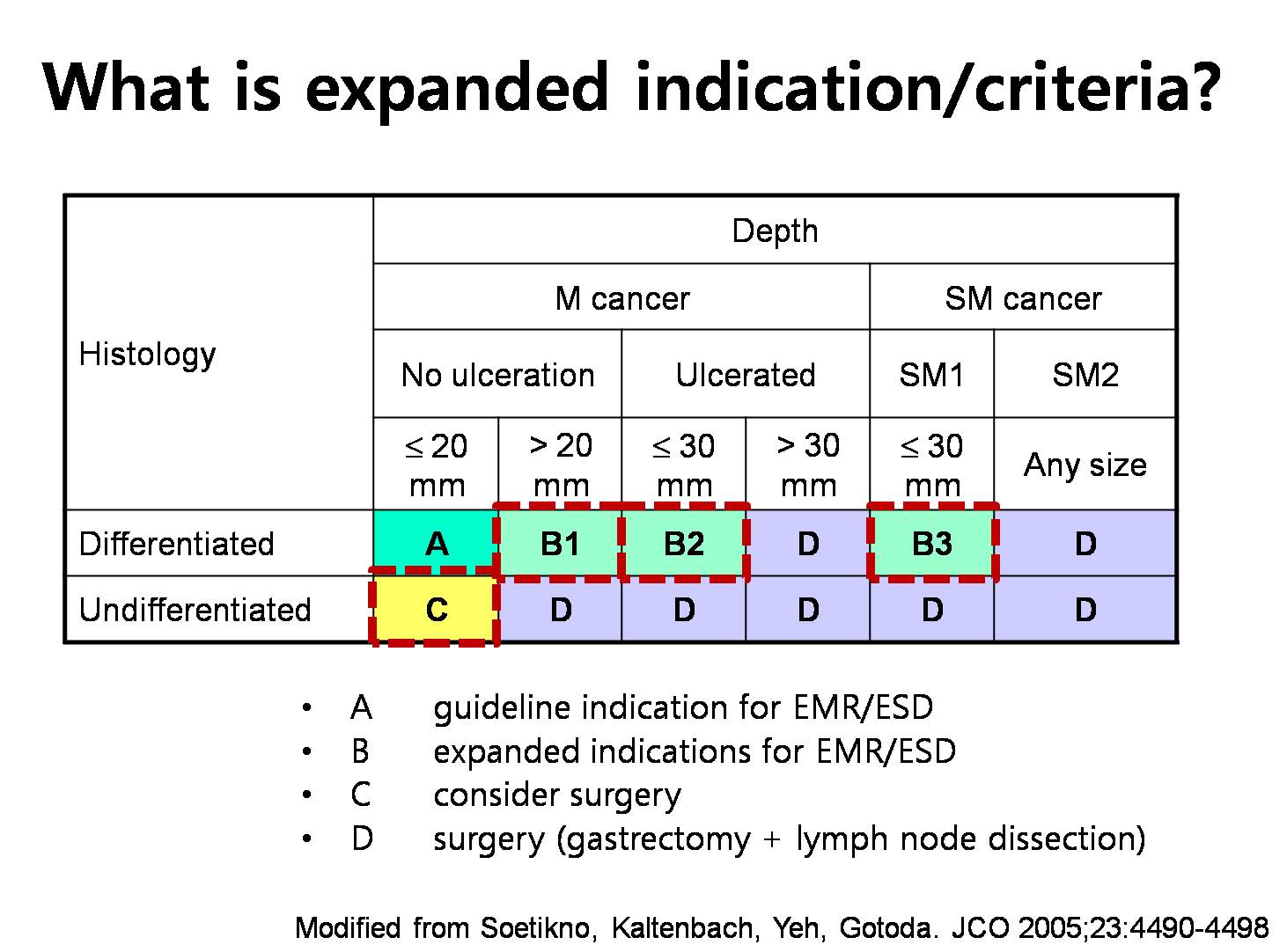
This is a very famous table for expanded indication. Three boxes in group B are expanded indications for ESD. However, the yellow box, group C, is considered to be an expanded indication by some endoscopists. So, there are two different definitions for expanded indications of ESD. Only B versus B and C. We need to be very careful when we read literatures on expanded indications.
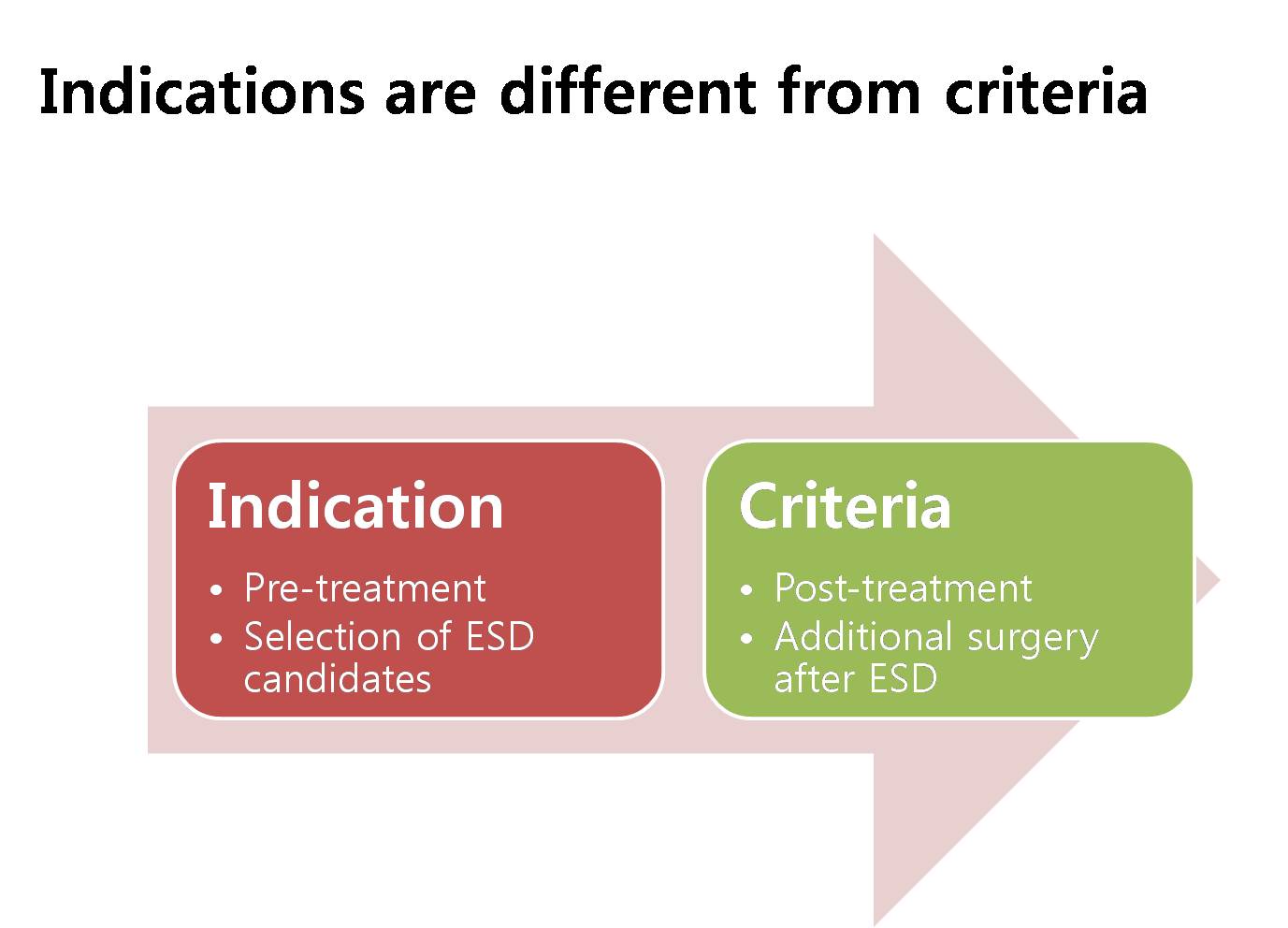
There is an important thing that we sometimes forget. Indications are different from criteria. Indication is something that we consider before the treatment. Criteria is something we consider after the treatment. In this regard, selection of patients for ESD can be different from selection of patients for additional surgery after ESD.
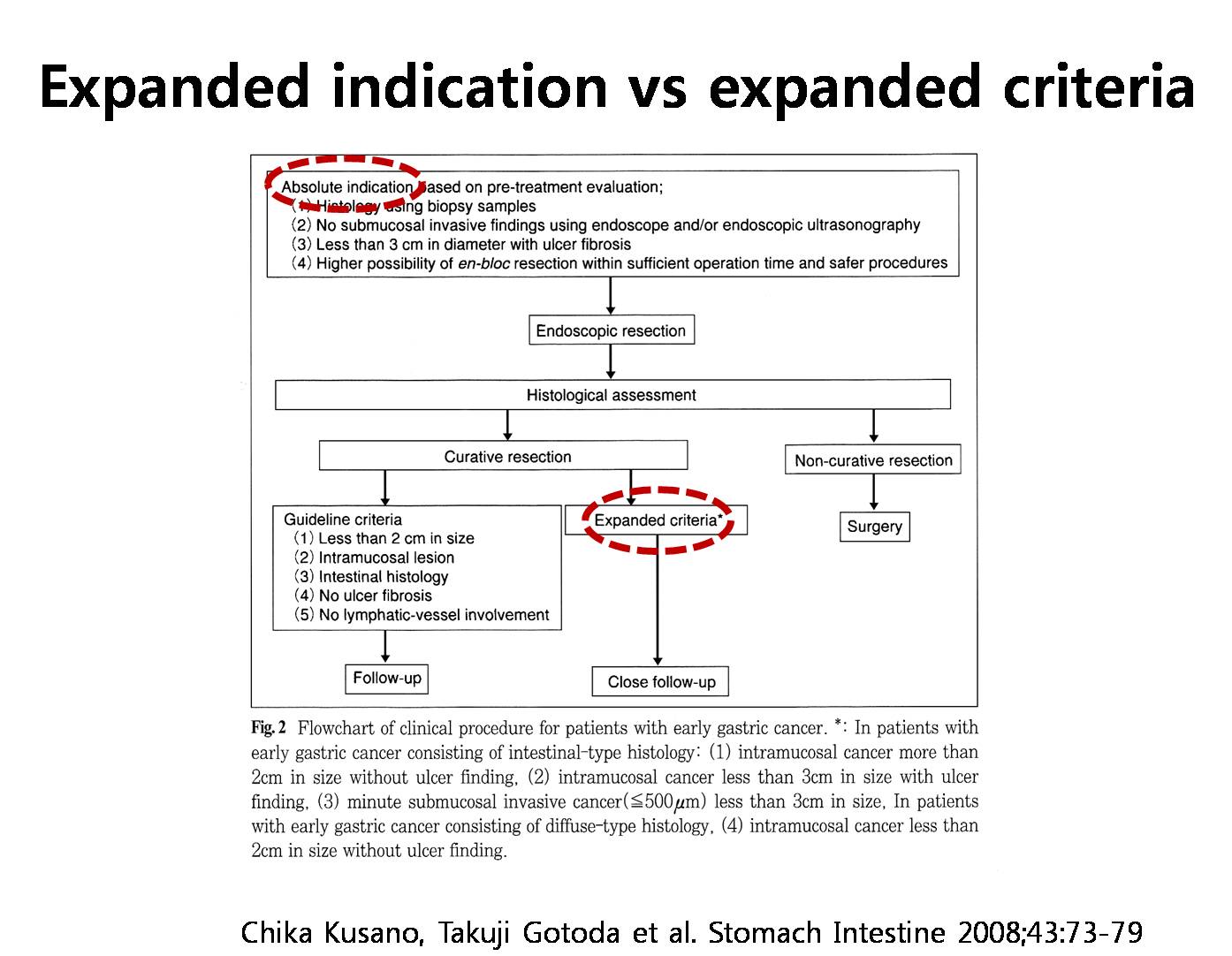
This is an algorithm from a Japanese literature. ESD candidates are selected by the absolute indications. Expanded indications are not considered for ESD in this flowchart. After ESD and histological assessment, you can see the concept of expanded criteria. When the lesion is slightly over the standard guideline criteria, you can choose close follow-up rather than additional surgery. So this group of patients was originally considered as an absolute indication, but after ESD they were changed into expanded criteria. So, indication and criteria is different in terms of the timing. Indication is before ESD, criteria is after ESD. We should not confuse them. But until now, the two terminologies are used interchangeably. I don’t like it.

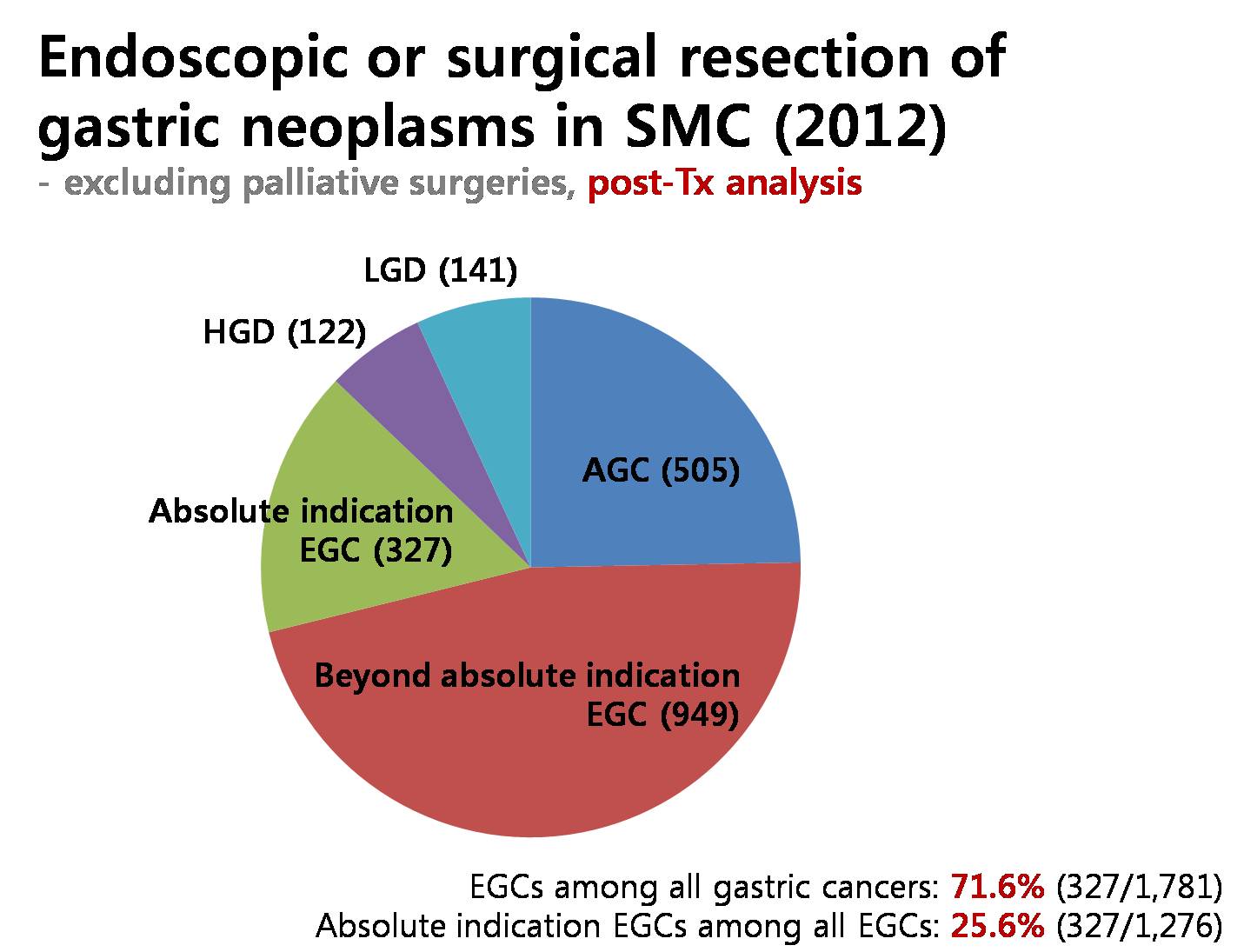
For the last 10 years, we did almost two thousand endoscopic resections for gastric cancers. In the technical aspects, the complete resection rate was 97% for cancers in the absolute indication, and it is 89% for beyond absolute indication cases. This is an example of data analysis based on post-ESD diagnostic groups.

In this flowchart, there was no case of recurrence in expanded indication group. Then, ESD for expanded indications is really safe? Stop. Take a moment. We need to be careful. Actually, most cases were considered as absolute indications, so the exact terminology is expanded criteria group rather than expanded indication group. I think expanded criteria group is safe after ESD, but expanded indication group before ESD may be different.
So I can say again that expanded criteria group after ESD is safe. But expanded indication group before ESD, we don’t know yet.

Before further discussion, I’d like to show you my conceptual framework of early gastric cancers. Some cases of EGC are absolute indications for ESD. Others are EGC beyond absolute indication. BAI. Considering expanded indications, some cases can be called EGC beyond expanded indication. BEI.
Before further discussion, I’d like to show you my conceptual framework of early gastric cancers. Some cases of EGC are absolute indications for ESD. Others are EGC beyond absolute indication. BAI. Considering expanded indications, some cases can be called EGC beyond expanded indication. BEI.
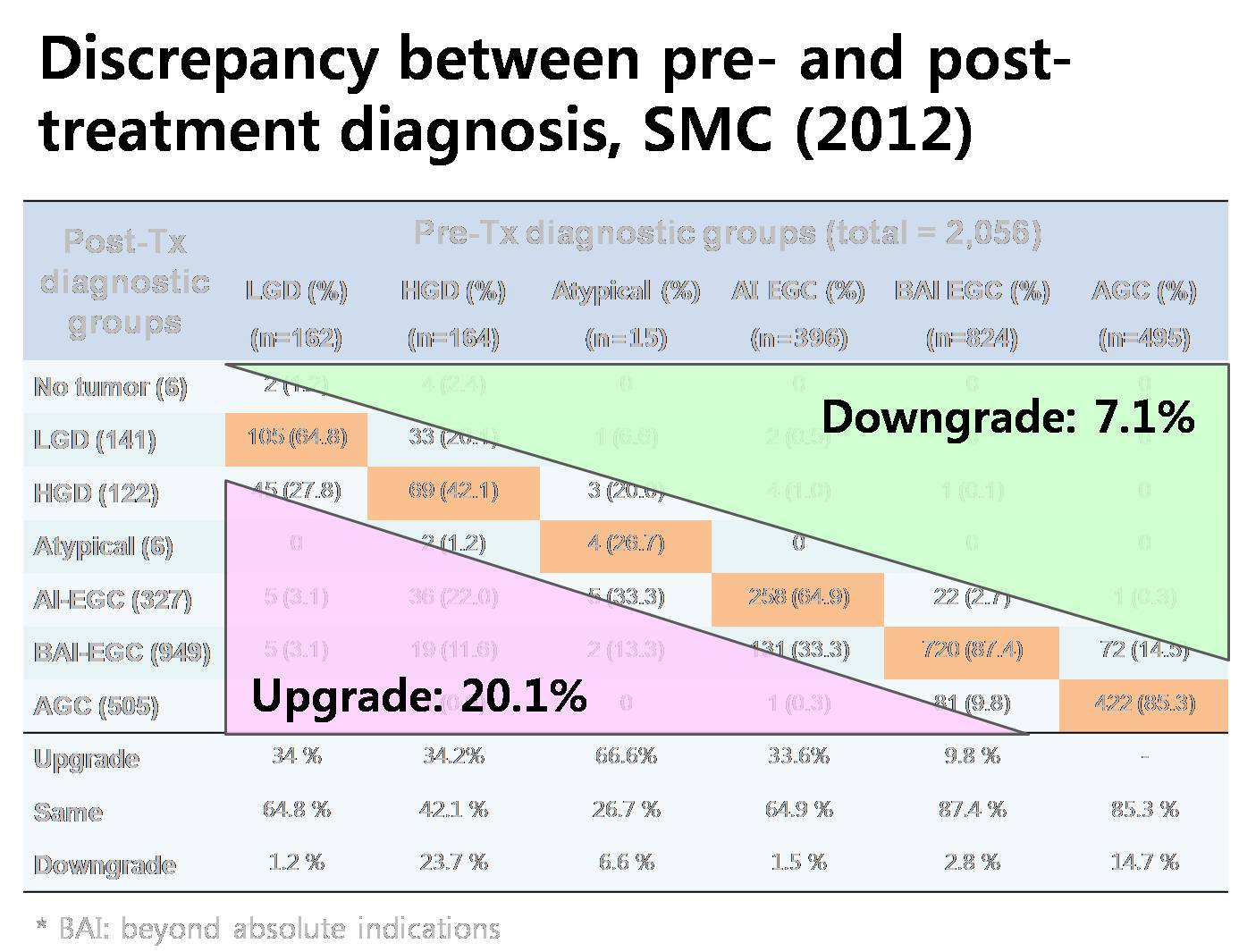
To put it simply, 7% were downgraded after the treatment, and 20% were upgraded after the treatment. It’s a huge difference.
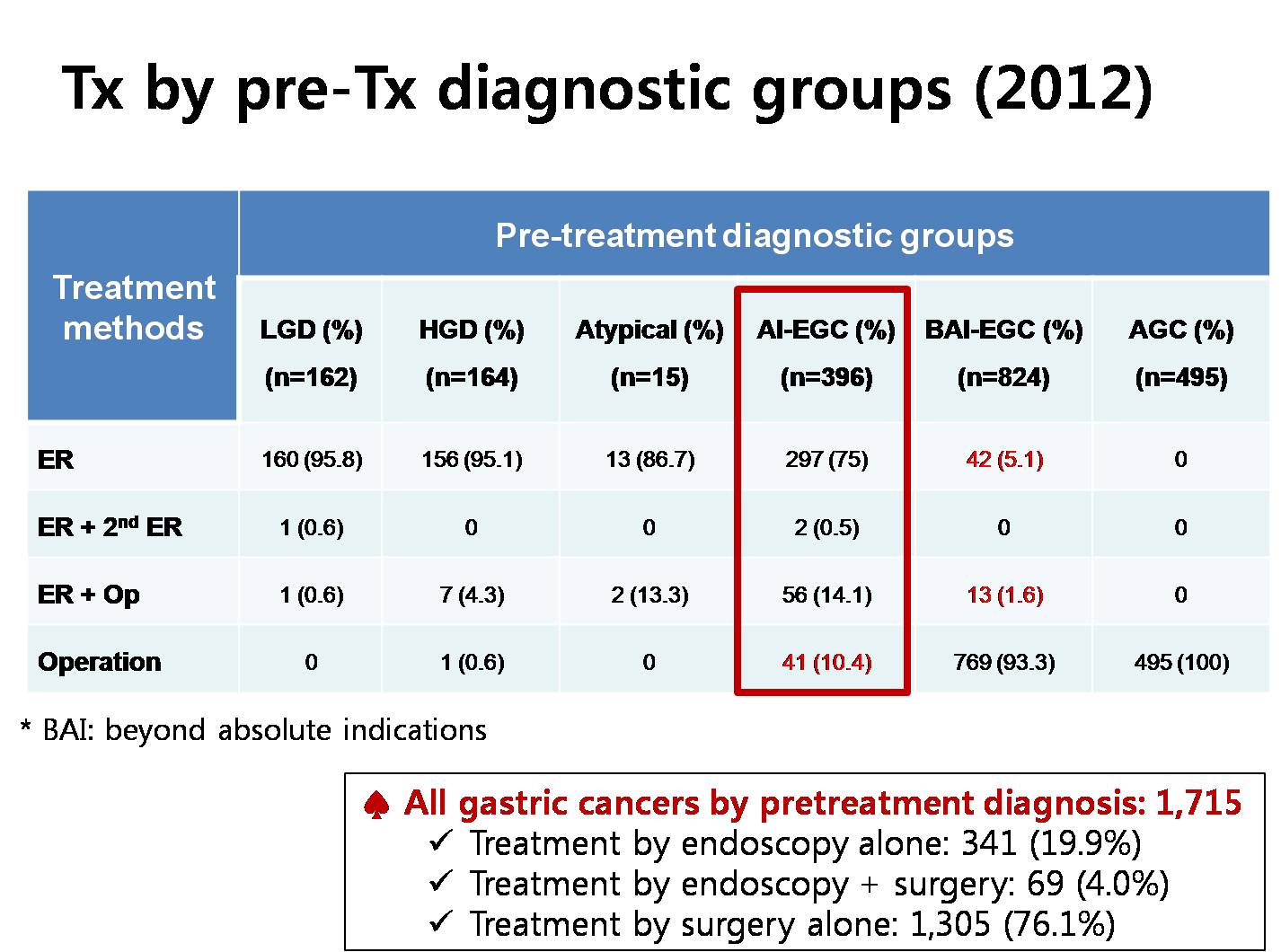
This is the treatment modalities for various gastric neoplasms by the pretreatment diagnostic groups. For early gastric cancers in the absolute indications, 90% were initially treated by ESD. Among them, additional surgeries were required in 16 percent. For early gastric cancers beyond absolute indications, 7 percent were initially treated by ESD. Among them, additional surgeries were required in 23%. In general, 20% of all gastric cancers were treated by endoscopy alone in our institution.
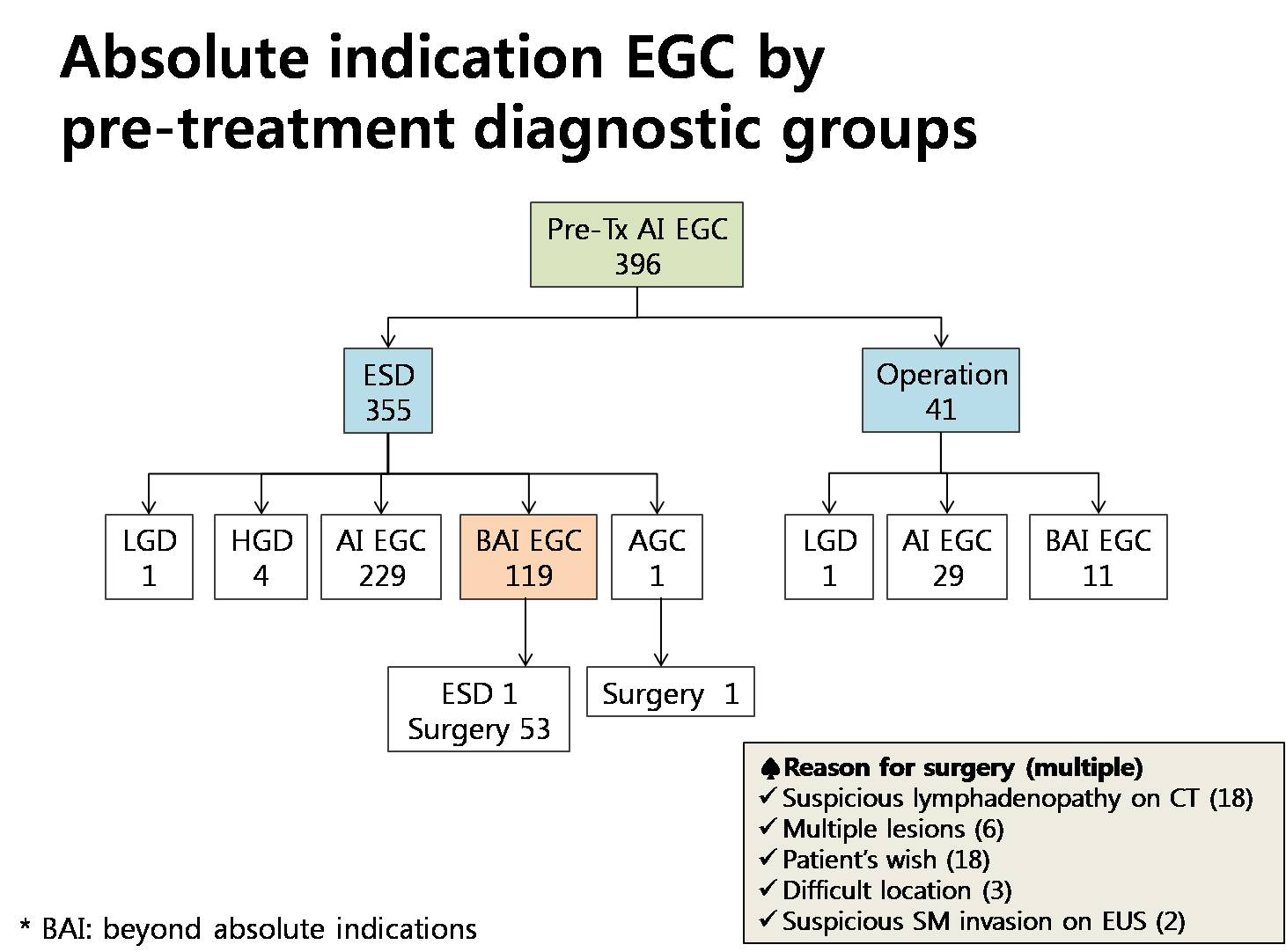
This flow diagram shows how we handled absolute indication early gastric cancers by the pretreatment diagnostic groups. Among 355 early gastric cancers initially treated by ESD, 119 cases, this is 34 percent, belonged to the beyond absolute indication group. Ten percent of patients in the absolute indication group were initially treated by surgery, and you can see the reason in the box at the corner. Suspicious lymphadenopathy was the most common reason for surgery.
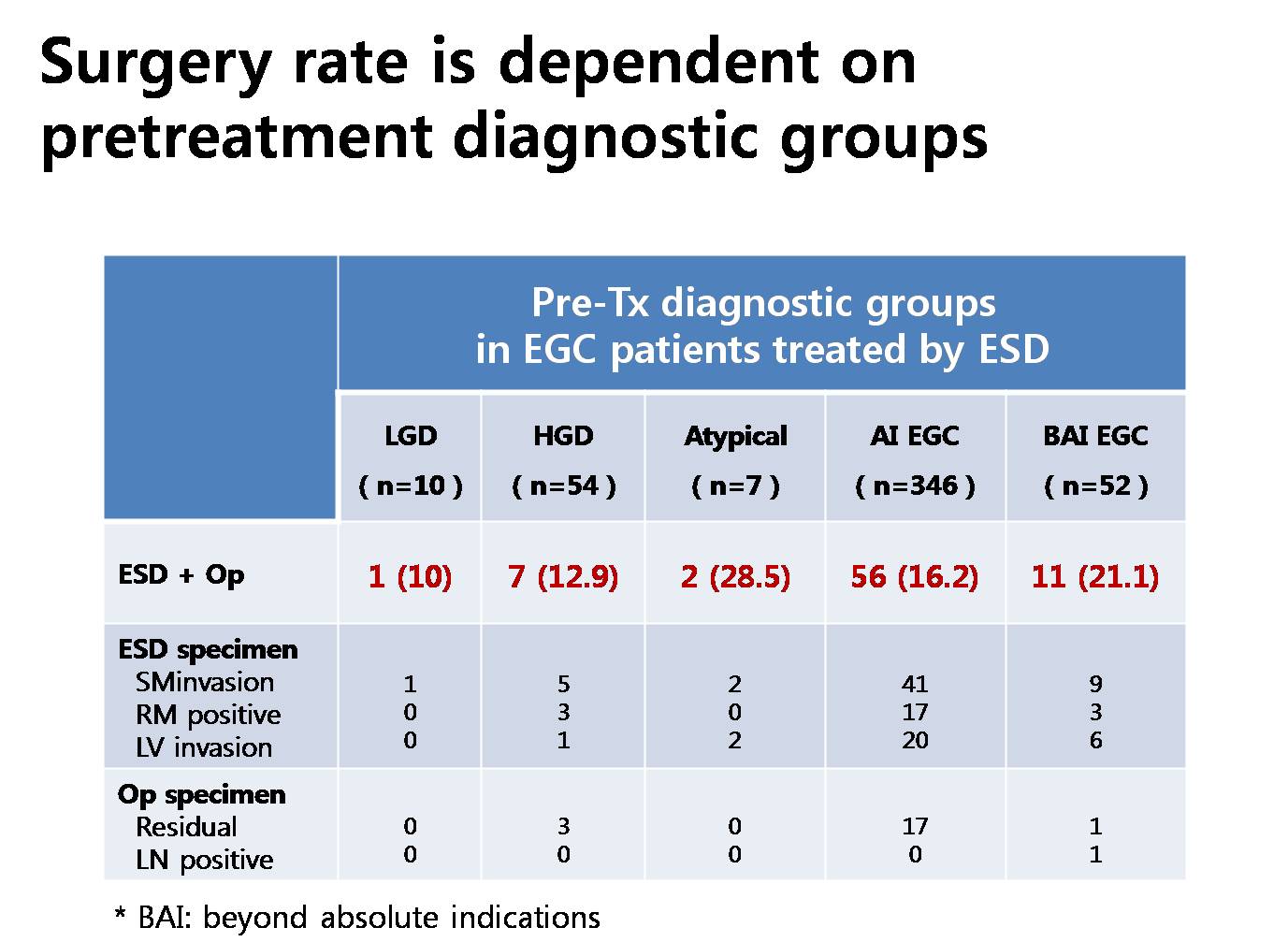
We also found that the rate of additional surgery was different by the pretreatment diagnostic groups. In groups of EGC of absolute indication before ESD, additional surgery rate was 16%, but it was 21% for patients in beyond absolute indication EGCs.

As I mentioned before, pretreatment expanded indication cases are different from post-treatment expanded indication cases in terms of the rate of complete resection and the rate of additional surgery. 80% of cases in post-treatment expanded indication cases were considered as absolute indication before ESD. 24% of pretreatment expanded indication cases are actually beyond expanded indication after ESD.
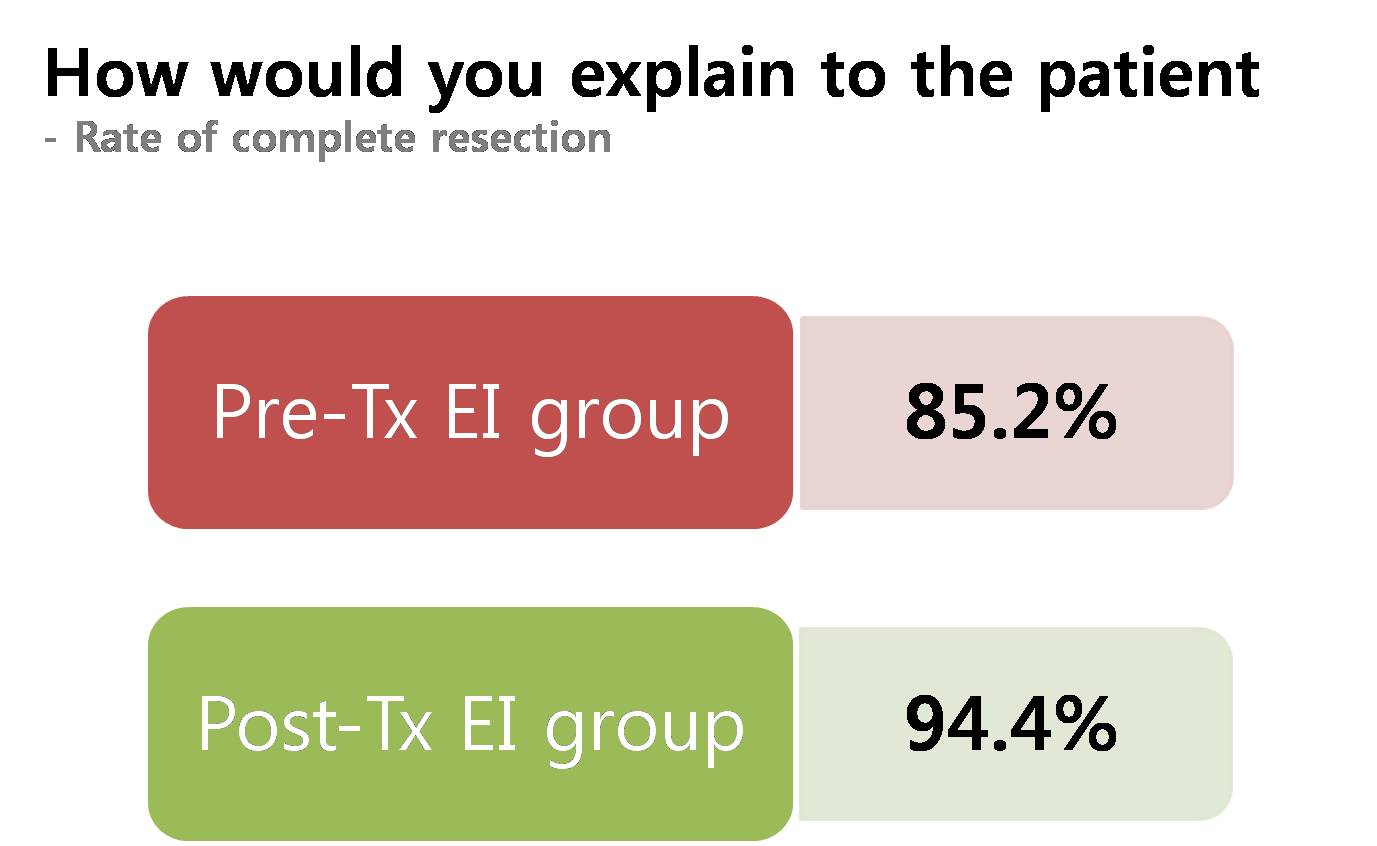
For patient with pretreatment expanded indication group, how would you explain the rate of complete resection or additional surgery after ESD? Complete resection rate will be 85 percent or 95% depending on your choice of data analysis. And I think data analysis based on pretreatment diagnostic groups is more relevant when we decide initial treatment options.
Ladies and gentlemen, I'd like to wrap up my short presentation. Selection of ESD candidates can be subjective. More effort for standardization is required. Indications are different from criteria. We need to be careful when reading the literatures. At least 20% of patients are upgraded after endoscopic or surgical resection of gastric neoplasms.

조직검사에서 poorly differentiated 혹은 signet ring cell carcinoma로 나왔는데 수술이나 ESD 후 well 또는 moderately differentiated로 나온 경우가 어느 정도인지 질문이 있었는데 정확히 답하지 못했습니다.
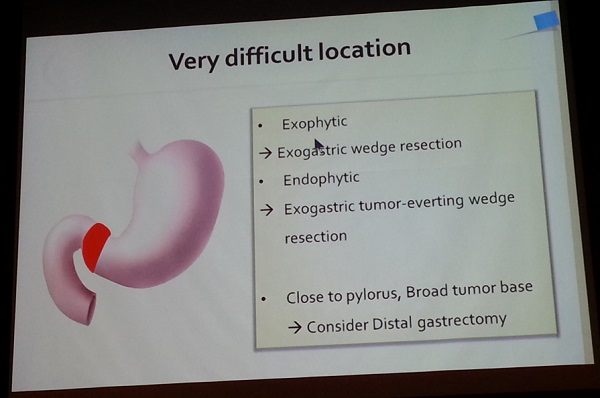
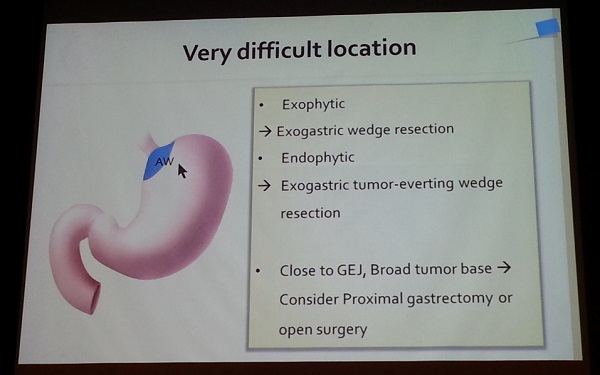
![]() [2014-5-16 오전 10시 30분. GIST 심포지엄]
[2014-5-16 오전 10시 30분. GIST 심포지엄]
1) Neoadjuvant imatinib for non-metastatic GISTs: indications and resuls. 서울대학교 임석안
증례가 흥미로웠습니다. 위체상부 전벽의 종괴인데 내시경 조직검사는 poorly cohesive adenocarcinoma라고 나왔으나 CT 소견을 바탕으로 GIST를 의심하고 병리 슬라이드를 재검하고 c-kit 염색을 다시하여 epithelioid type의 GIST로 진단하고 imatinib을 사용한 증례였습니다. Imatinib으로 질병이 거의 없어졌다가 setallite nodule이 발생하여 수술을 했다고 합니다. 병리결과만 보지 말고 CT 사진을 잘 들여다봐야 할 이유가 있습니다.
2) Role of PET-CT fir GISTs: preoperative risk evaluation and during chemotherapy. 원자력병원 임일한
Imatinib 사용 일주일 후 PET를 반복하면 response 여부를 일찍 알 수 있습니다. CT에서 크기가 줄어들기 전부터 PET의 signal이 약해지기 때문입니다. Early metabolic response라고 부르는 모양입니다.
3) Laparoscopic resection strategy for GISTs. 연세대학교 김종원
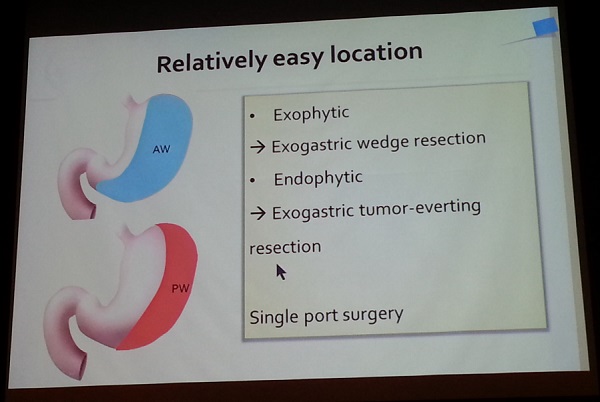
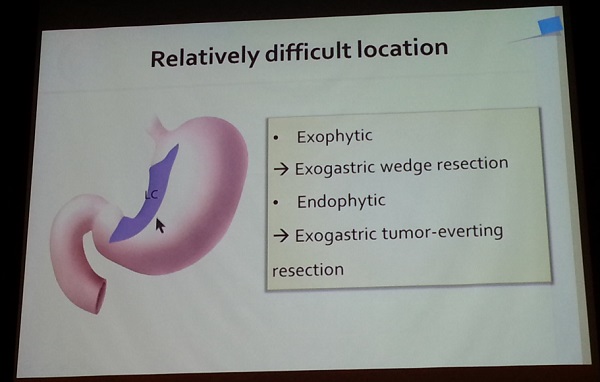
2010년 NCCN에서는 5cm 이하 GIST는 복강경으로 치료할 수 있다고 하였습니다 (may be라는 용어가 사용됨). 최근에는 5cm가 넘는 GIST에 대한 복강경치료가 많이 시행되고 있습니다. 2014년 NCCN에서는 크기에 대한 언급니 사라졌다고 합니다. 단지 위치에 대한 언급이 있다고 하네요 (in favorable anatomic location, greater curvature or anterior wall).

![]() [2014-5-16. Oral presentation (ESD)]
[2014-5-16. Oral presentation (ESD)]
연세대학교에서 'Is new criteria for mixed histology is necessary for endoscopic resection in EGC?'라는 제목의 발표를 하였습니다. 제가 흥미롭게 본 것은 Japanese classification입니다. 우리는 흔히 일본에서 말하는 differentiated cancer는 WHO 분류로 well-differentiated와 moderately-differentiated adenocarcinoma를 합한 것과 비슷하다고 생각합니다. 그런데 이번 발표를 보니 일본 분류에서 differentiated가 49.7%인 반면 well-differentiated와 moderately-differentiated adenocarcinoma의 합은 48%였습니다. 즉 2% 차이가 있습니다. 이 환자들은 어떤 조직학적 특징인 있는지 궁금할 뿐입니다. 일본 분류를 WHO 분류와 mapping하는 일은 무척 어려운 일입니다. 2 프로 부족합니다.

![]() 어제 보낸 위암 증례 28에서 제가 "필자는 평소 10개의 조기위암을 진단하는 것보다 1개의 보만 4형 진행성위암을 놓치지 않는 것이 더 중요하다고 강조하고 있습니다"라고 말한 부분에 대하여 한 애독자가 아래와 같은 의견을 보내주셨습니다. 이 또한 옳은 말씀입니다. 이 암 저 암 모두 놓치지 않는 것이 가장 좋습니다.
어제 보낸 위암 증례 28에서 제가 "필자는 평소 10개의 조기위암을 진단하는 것보다 1개의 보만 4형 진행성위암을 놓치지 않는 것이 더 중요하다고 강조하고 있습니다"라고 말한 부분에 대하여 한 애독자가 아래와 같은 의견을 보내주셨습니다. 이 또한 옳은 말씀입니다. 이 암 저 암 모두 놓치지 않는 것이 가장 좋습니다.
[2014-5-16. 애독자 comment] 저는 EGC 1개 진단하는 것이 AGC B-IV 10개 진단하는 것보다 중요하다고 생각합니다. 실제로 EGC 진단시에는 survival, QOL, treatment modality 등이 변하기 때문에 해당 환자의 인생을 좌우할 수 있지만, AGC B-IV는 거의 변하지 않기 때문입니다. 위암 검진의 방향이 일차예방(제균치료) + 이차예방(Correa 가설을 따르는 암의 조기진단)으로 좁혀지고 있는 것도 이 때문이라고 생각합니다. 전문가들이 pepsinogen+Hp Ab combination test로 놓칠 수 있는 위암(de novo carcinogenesis를 따르는 암)에 크게 의미를 두지 않는 것도 마찬가지 이유라고 생각합니다.
![]() 2014년 5월 17일 Bariatric surgery symposium
2014년 5월 17일 Bariatric surgery symposium
1. Setup & settling down metabolic & bariatric surgery. 순천향대학교 허경열
수술 이외에 Endobarrier라는 내시경치료가 소개되었습니다. 저는 경험이 없습니다. 우리나라에서 아직 아무도 경험이 없는 것 같습니다.
마지막 슬라이드제목은 Think outside the box: We have to change our strategy였습니다. 이런 내용이었습니다.
2. Surgical options for failed bariatric procedures. Keith C. Kim (Florida Hospital)
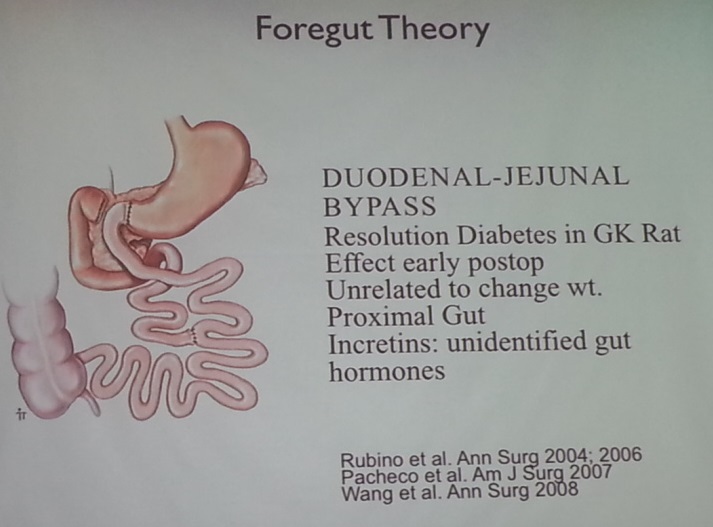

3. Recent results and issues ontype II DM between SG and RYGB. 고려대학교 박성수
최근 미국에서는 sleeve gastrectomy가 많이 시행되고 있습니다. 그러나 randomized trial에서는 sleeve gastrectomy의 remissin rate가 34%로 bypass surgery의 61%보다 낮았습니다. 비록 BMI에 따라 효과는 다르지만... Pure metabolic effect of sleeve gastrectomy may be lessened for BMI < 35.
@ 이준행 코맨트. 국민들이 운동하기 쉬운 환경을 만들고, 자동차를 적게 이용하고 대중교통을 이용하고 많이 걷도록 만들고, 좋은 음식을 적당히 먹도록 장려하고, 체중감소를 유도하고....... 이런 노력이 좀 더 필요할 것 같습니다. 요즘 당뇨 기준이 점차 강화되면서 이러다가는 전국민이 당뇨병 환자가 되지 않을까 걱정됩니다. 저는 외과의사들의 노력을 좀 더 지켜보려고 합니다. 부디 과잉치료가 되지 않기를 바랍니다. 마찬가지로 내과의사는 약을 너무 많이 주지 않기를 바랍니다. 지나침은 부족함보다 못한 법이니까요.
![]() 2014년 5월 17일 ESD symposium (Pros: 경희대학교 장재영, Cons: 단국대학교 지예섭)
2014년 5월 17일 ESD symposium (Pros: 경희대학교 장재영, Cons: 단국대학교 지예섭)
저는 아래와 같은 발언을 했습니다.
Not a question, but a comment. I am an endoscopist, but I am not with expanded indication. Indication and criteria is different. Expanded criteria may be OK, but expanded indication is too dangerous. The most important thing in this issue is that we doctors should provided best available treatment to the patients. After ESD for EGC, at least 10% of patients are indicated for surgery. In the real clinical practice, some of them refuse surgery. In some institution (maybe due to insufficient patient education), as much as 50% of patients refuse to be operated after ESD. That group of patients have high risk of recurrence, and most endoscopists already experienced sad stories of distant metastasis. In my opinion, the most important thing may be pre-ESD education. When surgery is required, surgery should be done. Without enough education and discussion, patients' choice cannot be an excuse for suboptimal treatment. Education is more important before ESD than before surgery.
Patient's preference가 중요하다는 floor의 comment가 있었습니다 (Y대학 교수). 동의합니다. 그러나 조건이 필요합니다. 아래와 같이 말하고 싶었으나 시간이 없었습니다.
전적으로 동의합니다. 저도 환자의 선택이 중요하다고 생각합니다. 자기 몸이므로 자기가 최종결정을 하는 것이 맞습니다. 당연합니다. 다만 저는 최종결정의 조건을 말하는 것입니다. 제가 논하고 싶은 것은 환자가 수술을 거부하기 전에, 즉 현재 기준으로 suboptimal treatment를 선택하기 전에 (1) 공정하고 충분한 정보를 제공 받았는가, (2) 결과가 나빴을 때 어떤 일이 가능한지 이해하고 있는가 (사실 많은 환자들이 재발하면 그 때 수술받지 뭐... 정도로 생각하고 있습니다. 수술할 수 없는 경우가 많다는 것을 모르는 것이지요. 죽을 수 있다는 것을 모르는 것이지요), (3) 의료진과 상의할 충분한 기회를 제공받았는가, (4) 지나치게 급하게 혹은 권위적인 분위기에서 결정된 것은 아닌가 등등입니다. 의사의 양심에 어긋나지 않는 충분하고도 자세한 교육과 편안한 분위기의 장시간 상담 등을 생략하고 그냥 환자의 선택이라는 이유로 suboptimal treatment를 용인하는 것은 반대합니다. 환자가 나쁜 선택을 하지 못하도록 노력하는 것도 의사의 중요한 역할입니다..

잠시 짬을 내서 동학사에 다녀왔습니다. 그 유명한 비구니 절.

세 스님

동학사 입구에 중증열성혈소판감소증후군의 원인인 작은소참진드기를 주의하라는 안내문이 있었습니다.

대전컨벤션센터 바로 건너편에 골프존에서 큰 건물을 짓고 있었습니다. 그런데 벽에 붙어있는 모토가 맘에 들었습니다. /기/본/이/혁/신/이/다/
![]() [References]
[References]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.